Embed Size (px)
DESCRIPTION
In this paper, we attempt to bring out the current state of affairs in the healthcare delivery space in the northern region of India, recent trends in the sector and challenges in executing an effective healthcare agenda, with recommendations and actions for transforming healthcare in North India.
Citation preview
© Grant Thornton India LLP. All rights reserved.
Agenda for Transforming Healthcare Delivery in the Northern Region
Bridging the Divide - for a Healthy India

© Grant Thornton India LLP. All rights reserved.
03 | Foreword
04 | The Healthcare industry
09 | Healthcare delivery
17 | Healthcare infrastructure
23 | Investment Horizon
28 | Changing trends
32 | Outlook
37 | Appendices
48 | Contact us
Contents

© Grant Thornton India LLP. All rights reserved. 3
Foreword
In a populous nation like ours, with an ever increasing need for healthcare infrastructure and
services, the private sector has remained the lynchpin of growth, accounting for more than half of
the total healthcare spending in the country.
The healthcare delivery sector is characterised by wide regional disparities with rural India being
highly underserved. Further, the Southern region has been a change catalyst and far ahead of its
Northern counterpart in terms of access, technology, infrastructure and sometimes even, in the
quality of service.
Against a backdrop of changing demographics and socio economic mix in the Indian population, it
is imperative to raise the bar on quality of healthcare service delivery and ensure equitable and
affordable access across social strata. Achieving this requires several factors to come together, not
least the optimal utilization of existing healthcare resources and the role the government needs to
play in the holistic development of a regional healthcare system.
In this paper, we attempt to bring out the current state of affairs in the healthcare delivery space in
the northern region of India, recent trends in the sector and challenges in executing an effective
healthcare agenda, with recommendations and actions for transforming healthcare in North India.
Mahadevan Narayanamoni
Partner and Practice Leader
Healthcare and Life-sciences
Advisory
Grant Thornton India LLP
Harpal Singh
Conference Chairman &
Past Chairman
CII Northern Region
© Grant Thornton India LLP. All rights reserved. 4
The Healthcare industry Market size and segmentation
© Grant Thornton India LLP. All rights reserved. 5
Glaring statistics
our country ranks 112th on the World Health Organisation’s (WHO) ranking of the
world’s health systems.
doctor-to-patient ratio for rural India, as per the Health Ministry statistics, stands
at 1:30,000, well below the WHO’s recommended 1:1,000.
Overall healthcare spending (public and private) accounts for a mere 4% of India's
GDP, far below the average of 9.5% across Organisation for Economic Co-operation
and Development (OECD) countries. Private sector accounts for more than 70% of
this spend, while the public sector spend has been only 1.4%.
in terms of the total health expenditure per capita (in US$), India spends the least
on public healthcare among the BRICS nations.
for FY14, the Union Budget has allocated larger funds for the health sector, Rs
37,330 crore from the revised estimates of Rs 24,894 crore for FY13
merely 20% of India’s 1.2 billion population is covered by health insurance
of the 1.35 million hospital beds in the country, only 48% are functional
the private sector accounts for 65% of the total number of operational beds, and
over 70% of the spending on healthcare in India.
lack of healthcare facilities in the rural areas as well as among those at the
bottom of the pyramid is one of the big challenges in delivering scalable
healthcare options
© Grant Thornton India LLP. All rights reserved. 6
While the healthcare delivery sector in North
has been making progress with a number of
hospitals and healthcare centres gaining
accreditations from National Accreditation
Board for Hospitals & Healthcare Providers
(NABH), the region still lags behind many parts
of the country on several healthcare parameters.
The number of hospitals and inpatient beds
available relative to the total population of the
region is far lower than the national average.
The states (Delhi, Haryana, Himachal Pradesh,
Jammu & Kashmir, Punjab, Rajasthan,
Uttarakhand and Uttar Pradesh) continue to
battle high rates of infant mortality and
incidence of deaths due to dengue, cholera,
diarrhea and other ailments.
The lack of requisite infrastructure in the
semi-rural and rural areas of northern India is
one of the key barriers to the delivery of basic
healthcare services in the region.
Market size and segmentation
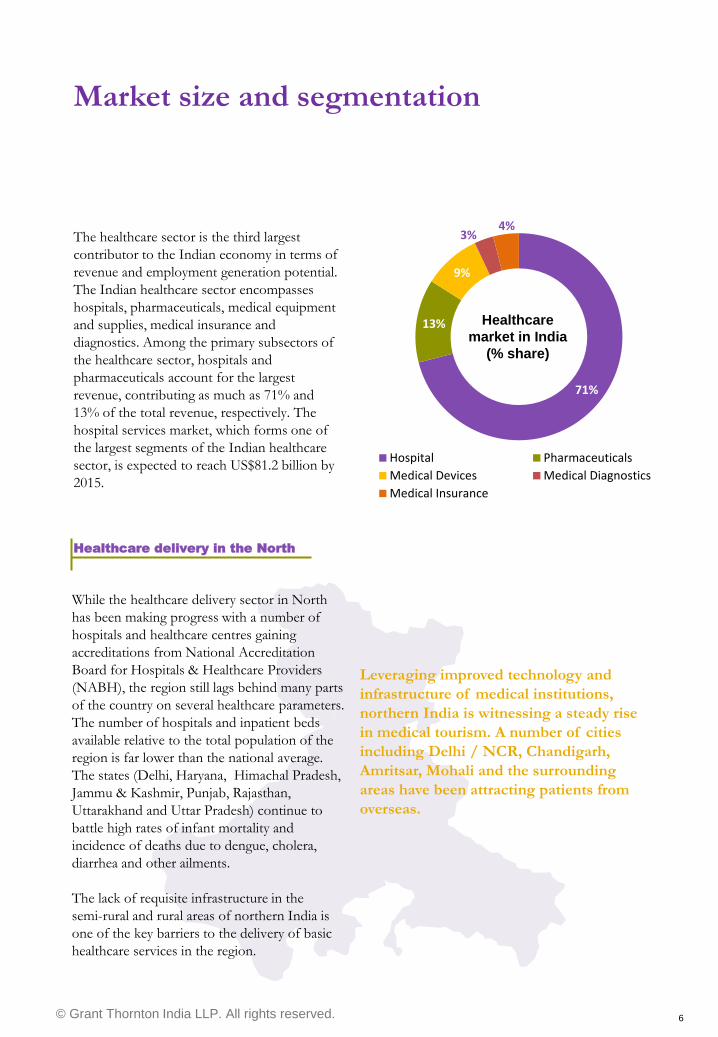
The healthcare sector is the third largest
contributor to the Indian economy in terms of
revenue and employment generation potential.
The Indian healthcare sector encompasses
hospitals, pharmaceuticals, medical equipment
and supplies, medical insurance and
diagnostics. Among the primary subsectors of
the healthcare sector, hospitals and
pharmaceuticals account for the largest
revenue, contributing as much as 71% and
13% of the total revenue, respectively. The
hospital services market, which forms one of
the largest segments of the Indian healthcare
sector, is expected to reach US$81.2 billion by
2015.
Leveraging improved technology and
infrastructure of medical institutions,
northern India is witnessing a steady rise
in medical tourism. A number of cities
including Delhi / NCR, Chandigarh,
Amritsar, Mohali and the surrounding
areas have been attracting patients from
overseas.
Healthcare delivery in the North
71%
13%
9%
3% 4%
Hospital Pharmaceuticals
Medical Devices Medical Diagnostics
Medical Insurance
Healthcare
market in India
(% share)
© Grant Thornton India LLP. All rights reserved. 7
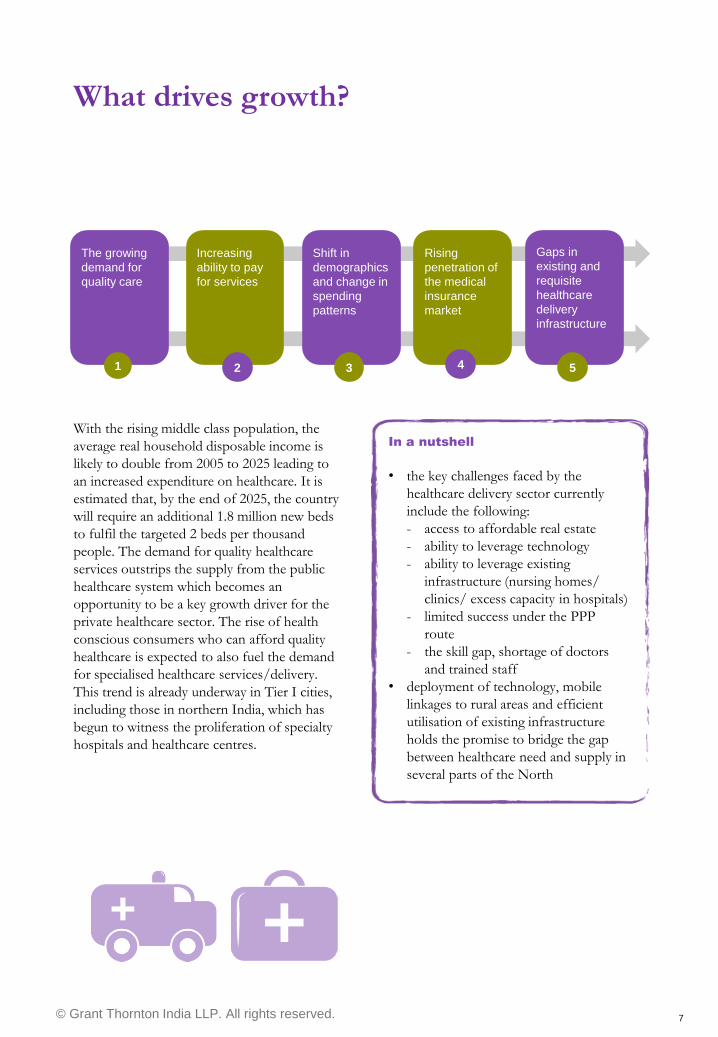
What drives growth?
With the rising middle class population, the
average real household disposable income is
likely to double from 2005 to 2025 leading to
an increased expenditure on healthcare. It is
estimated that, by the end of 2025, the country
will require an additional 1.8 million new beds
to fulfil the targeted 2 beds per thousand
people. The demand for quality healthcare
services outstrips the supply from the public
healthcare system which becomes an
opportunity to be a key growth driver for the
private healthcare sector. The rise of health
conscious consumers who can afford quality
healthcare is expected to also fuel the demand
for specialised healthcare services/delivery.
This trend is already underway in Tier I cities,
including those in northern India, which has
begun to witness the proliferation of specialty
hospitals and healthcare centres.
The growing
demand for
quality care
Shift in
demographics
and change in
spending
patterns
Increasing
ability to pay
for services
Rising
penetration of
the medical
insurance
market
Gaps in
existing and
requisite
healthcare
delivery
infrastructure
1
. 2 3 4 5
In a nutshell
• the key challenges faced by the
healthcare delivery sector currently
include the following:
- access to affordable real estate
- ability to leverage technology
- ability to leverage existing
infrastructure (nursing homes/
clinics/ excess capacity in hospitals)
- limited success under the PPP
route
- the skill gap, shortage of doctors
and trained staff
• deployment of technology, mobile
linkages to rural areas and efficient
utilisation of existing infrastructure
holds the promise to bridge the gap
between healthcare need and supply in
several parts of the North
© Grant Thornton India LLP. All rights reserved. 8
Recent policy initiatives
To increase access and utilisation of quality
health services by the rural population, the
Central Government launched the National
Rural Health Mission (NRHM) in April 2005.
NRHM has helped upgrade health
infrastructure, improve manpower availability
and skills of healthcare service providers and
improve accessibility of drugs and diagnostics
and service delivery in the rural areas. The
Centre is also planning to launch the National
Urban Health Mission (NUHM), which will
focus on slums and urban poor. NUHM will
cover all cities and towns with a population of
more than 50,000. The scheme will cover
over 779 Indian cities and towns, as well as
several Tier I cities.
As a part of NRHM, Government of India's
Ministry of Health and Family Welfare
(MoHFW) has instituted Accredited Social
Health Activists (ASHAs). The initiative
entails the provision of a trained female
community health activist in every village in
the country. The female community health
activist is a representative of the village and
works as an interface between the community
and the public health system.
To-do’s
• efficiently utilise current infrastructure, before allowing for more
• link ASHA‟s to the nearest facilities, provide infrastructure and financial support
• mobile healthcare units to form the link between the interiors and the nearest facility
• rural public infrastructure must remain at the forefront of healthcare policies
• preferential land allotment/ subsidies where there is infrastructure gap
• cutting down the risk of deaths in maternal and perinatal conditions
• increase public health spending
• streamline drug purchase stocking distribution arrangements
• low-cost day care surgery models at government hospitals
• continued focus on development of medical colleges and institutions

© Grant Thornton India LLP. All rights reserved. 9
Healthcare delivery Key players, operating models and recent trends
© Grant Thornton India LLP. All rights reserved. 10
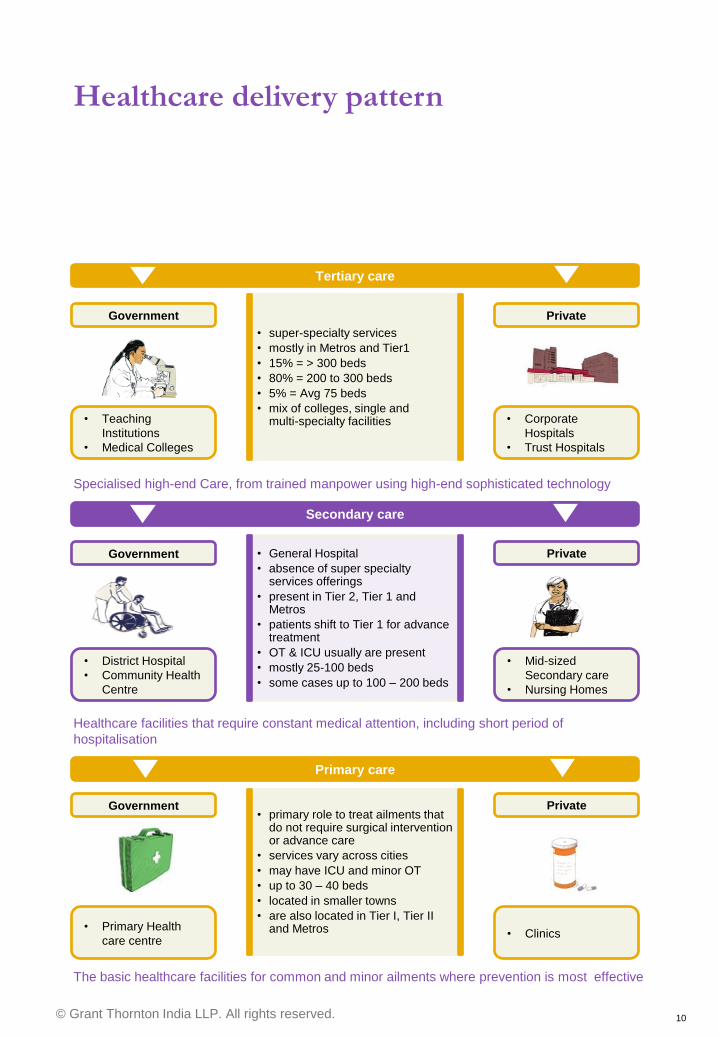
Healthcare delivery pattern
• General Hospital
• absence of super specialty services offerings
• present in Tier 2, Tier 1 and Metros
• patients shift to Tier 1 for advance treatment
• OT & ICU usually are present
• mostly 25-100 beds
• some cases up to 100 – 200 beds
Tertiary care
Government
• Teaching
Institutions
• Medical Colleges
Private
• Corporate
Hospitals
• Trust Hospitals
Specialised high-end Care, from trained manpower using high-end sophisticated technology
Secondary care
Government
• District Hospital
• Community Health
Centre
Private
• Mid-sized
Secondary care
• Nursing Homes
Healthcare facilities that require constant medical attention, including short period of
hospitalisation
The basic healthcare facilities for common and minor ailments where prevention is most effective
Primary care
Government
• Primary Health
care centre
Private
• Clinics
• super-specialty services
• mostly in Metros and Tier1
• 15% = > 300 beds
• 80% = 200 to 300 beds
• 5% = Avg 75 beds
• mix of colleges, single and multi-specialty facilities
• primary role to treat ailments that do not require surgical intervention or advance care
• services vary across cities
• may have ICU and minor OT
• up to 30 – 40 beds
• located in smaller towns
• are also located in Tier I, Tier II and Metros
© Grant Thornton India LLP. All rights reserved. 11
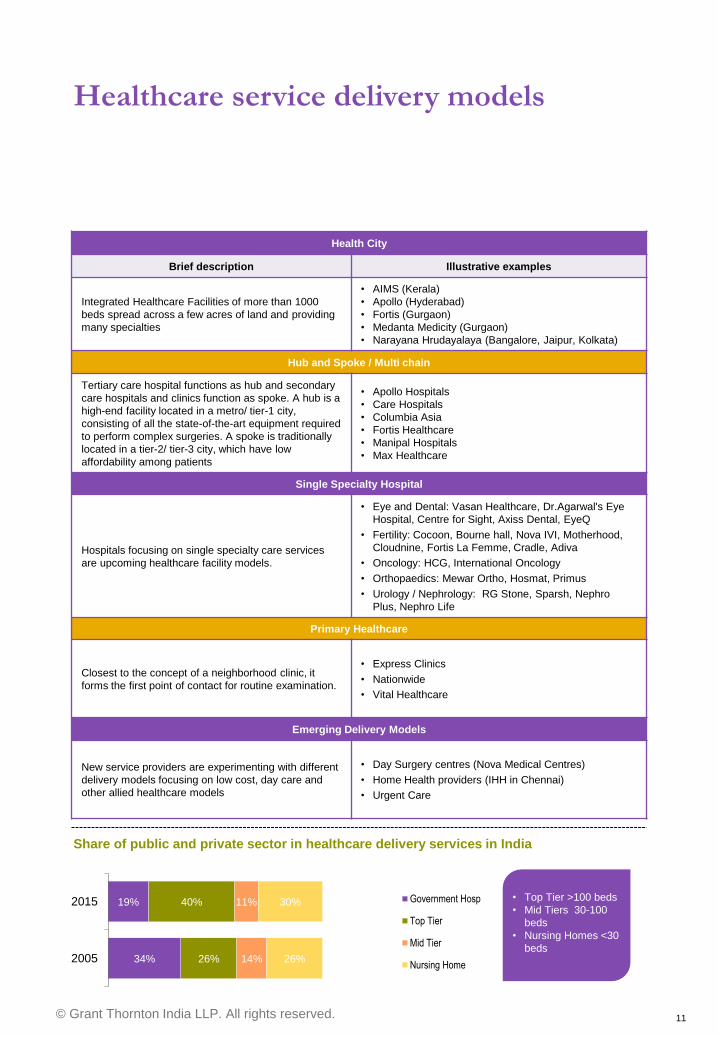
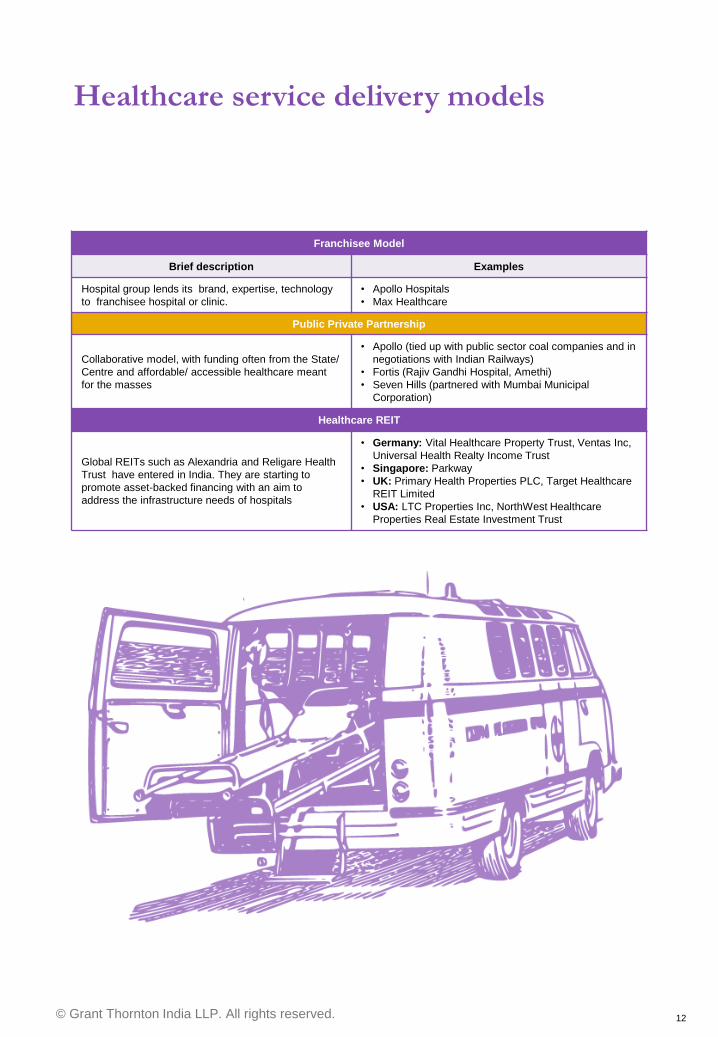
Healthcare service delivery models
Health City
Brief description Illustrative examples
Integrated Healthcare Facilities of more than 1000
beds spread across a few acres of land and providing
many specialties
• AIMS (Kerala)
• Apollo (Hyderabad)
• Fortis (Gurgaon)
• Medanta Medicity (Gurgaon)
• Narayana Hrudayalaya (Bangalore, Jaipur, Kolkata)
Hub and Spoke / Multi chain
Tertiary care hospital functions as hub and secondary
care hospitals and clinics function as spoke. A hub is a
high-end facility located in a metro/ tier-1 city,
consisting of all the state-of-the-art equipment required
to perform complex surgeries. A spoke is traditionally
located in a tier-2/ tier-3 city, which have low
affordability among patients
• Apollo Hospitals
• Care Hospitals
• Columbia Asia
• Fortis Healthcare
• Manipal Hospitals
• Max Healthcare
Single Specialty Hospital
Hospitals focusing on single specialty care services
are upcoming healthcare facility models.
• Eye and Dental: Vasan Healthcare, Dr.Agarwal's Eye
Hospital, Centre for Sight, Axiss Dental, EyeQ
• Fertility: Cocoon, Bourne hall, Nova IVI, Motherhood,
Cloudnine, Fortis La Femme, Cradle, Adiva
• Oncology: HCG, International Oncology
• Orthopaedics: Mewar Ortho, Hosmat, Primus
• Urology / Nephrology: RG Stone, Sparsh, Nephro
Plus, Nephro Life
Primary Healthcare
Closest to the concept of a neighborhood clinic, it
forms the first point of contact for routine examination.
• Express Clinics
• Nationwide
• Vital Healthcare
Emerging Delivery Models
New service providers are experimenting with different
delivery models focusing on low cost, day care and
other allied healthcare models
• Day Surgery centres (Nova Medical Centres)
• Home Health providers (IHH in Chennai)
• Urgent Care
34%
19%
26%
40%
14%
11%
26%
30%
2005
2015 Government Hosp
Top Tier
Mid Tier
Nursing Home
• Top Tier >100 beds
• Mid Tiers 30-100
beds
• Nursing Homes <30
beds
Share of public and private sector in healthcare delivery services in India
© Grant Thornton India LLP. All rights reserved. 12
Franchisee Model
Brief description Examples
Hospital group lends its brand, expertise, technology
to franchisee hospital or clinic.
• Apollo Hospitals
• Max Healthcare
Public Private Partnership
Collaborative model, with funding often from the State/
Centre and affordable/ accessible healthcare meant
for the masses
• Apollo (tied up with public sector coal companies and in
negotiations with Indian Railways)
• Fortis (Rajiv Gandhi Hospital, Amethi)
• Seven Hills (partnered with Mumbai Municipal
Corporation)
Healthcare REIT
Global REITs such as Alexandria and Religare Health
Trust have entered in India. They are starting to
promote asset-backed financing with an aim to
address the infrastructure needs of hospitals
• Germany: Vital Healthcare Property Trust, Ventas Inc,
Universal Health Realty Income Trust
• Singapore: Parkway
• UK: Primary Health Properties PLC, Target Healthcare
REIT Limited
• USA: LTC Properties Inc, NorthWest Healthcare
Properties Real Estate Investment Trust
Healthcare service delivery models
Top Tier >100 beds
Mid Tiers 30-100
beds
Nursing Homes <30
beds
Top Tier >100 beds
Mid Tiers 30-100
beds
Nursing Homes <30
beds
© Grant Thornton India LLP. All rights reserved. 13
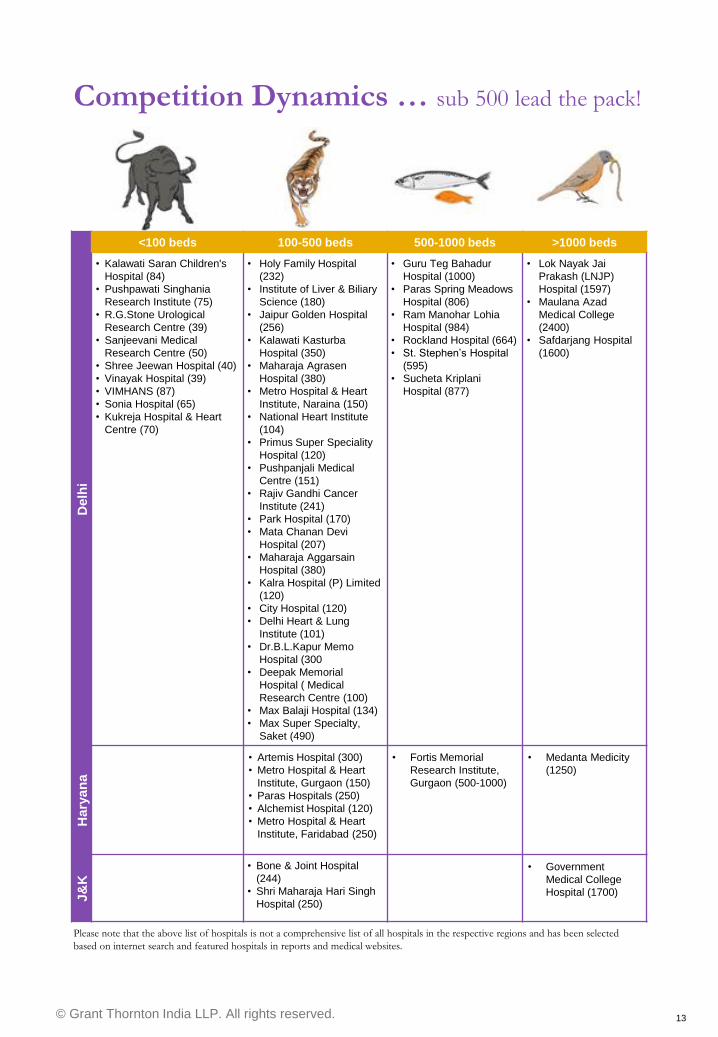
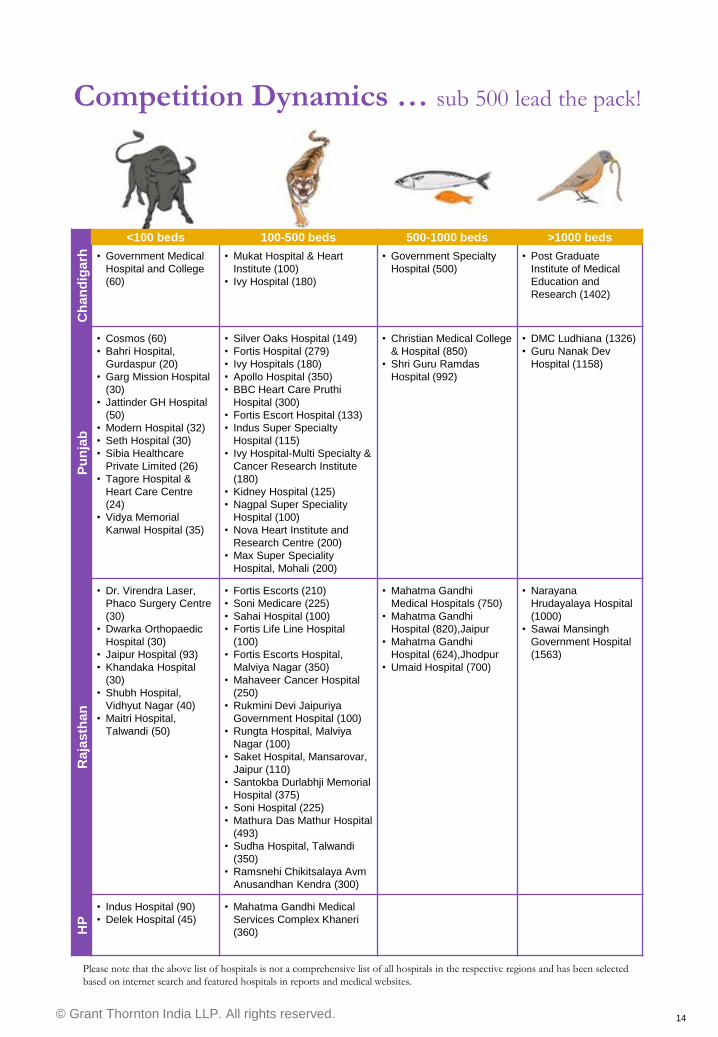
Competition Dynamics … sub 500 lead the pack!
<100 beds 100-500 beds 500-1000 beds >1000 beds
Delh
i
• Kalawati Saran Children's
Hospital (84)
• Pushpawati Singhania
Research Institute (75)
• R.G.Stone Urological
Research Centre (39)
• Sanjeevani Medical
Research Centre (50)
• Shree Jeewan Hospital (40)
• Vinayak Hospital (39)
• VIMHANS (87)
• Sonia Hospital (65)
• Kukreja Hospital & Heart
Centre (70)
• Holy Family Hospital
(232)
• Institute of Liver & Biliary
Science (180)
• Jaipur Golden Hospital
(256)
• Kalawati Kasturba
Hospital (350)
• Maharaja Agrasen
Hospital (380)
• Metro Hospital & Heart
Institute, Naraina (150)
• National Heart Institute
(104)
• Primus Super Speciality
Hospital (120)
• Pushpanjali Medical
Centre (151)
• Rajiv Gandhi Cancer
Institute (241)
• Park Hospital (170)
• Mata Chanan Devi
Hospital (207)
• Maharaja Aggarsain
Hospital (380)
• Kalra Hospital (P) Limited
(120)
• City Hospital (120)
• Delhi Heart & Lung
Institute (101)
• Dr.B.L.Kapur Memo
Hospital (300
• Deepak Memorial
Hospital ( Medical
Research Centre (100)
• Max Balaji Hospital (134)
• Max Super Specialty,
Saket (490)
• Guru Teg Bahadur
Hospital (1000)
• Paras Spring Meadows
Hospital (806)
• Ram Manohar Lohia
Hospital (984)
• Rockland Hospital (664)
• St. Stephen‟s Hospital
(595)
• Sucheta Kriplani
Hospital (877)
• Lok Nayak Jai
Prakash (LNJP)
Hospital (1597)
• Maulana Azad
Medical College
(2400)
• Safdarjang Hospital
(1600)
Hary
an
a
• Artemis Hospital (300)
• Metro Hospital & Heart
Institute, Gurgaon (150)
• Paras Hospitals (250)
• Alchemist Hospital (120)
• Metro Hospital & Heart
Institute, Faridabad (250)
• Fortis Memorial
Research Institute,
Gurgaon (500-1000)
• Medanta Medicity
(1250)
J&
K
• Bone & Joint Hospital
(244)
• Shri Maharaja Hari Singh
Hospital (250)
• Government
Medical College
Hospital (1700)
Please note that the above list of hospitals is not a comprehensive list of all hospitals in the respective regions and has been selected
based on internet search and featured hospitals in reports and medical websites.
© Grant Thornton India LLP. All rights reserved. 14
<100 beds 100-500 beds 500-1000 beds >1000 beds
Ch
an
dig
arh
• Government Medical
Hospital and College
(60)
• Mukat Hospital & Heart
Institute (100)
• Ivy Hospital (180)
• Government Specialty
Hospital (500)
• Post Graduate
Institute of Medical
Education and
Research (1402)
Pu
nja
b
• Cosmos (60)
• Bahri Hospital,
Gurdaspur (20)
• Garg Mission Hospital
(30)
• Jattinder GH Hospital
(50)
• Modern Hospital (32)
• Seth Hospital (30)
• Sibia Healthcare
Private Limited (26)
• Tagore Hospital &
Heart Care Centre
(24)
• Vidya Memorial
Kanwal Hospital (35)
• Silver Oaks Hospital (149)
• Fortis Hospital (279)
• Ivy Hospitals (180)
• Apollo Hospital (350)
• BBC Heart Care Pruthi
Hospital (300)
• Fortis Escort Hospital (133)
• Indus Super Specialty
Hospital (115)
• Ivy Hospital-Multi Specialty &
Cancer Research Institute
(180)
• Kidney Hospital (125)
• Nagpal Super Speciality
Hospital (100)
• Nova Heart Institute and
Research Centre (200)
• Max Super Speciality
Hospital, Mohali (200)
• Christian Medical College
& Hospital (850)
• Shri Guru Ramdas
Hospital (992)
• DMC Ludhiana (1326)
• Guru Nanak Dev
Hospital (1158)
Raja
sth
an
• Dr. Virendra Laser,
Phaco Surgery Centre
(30)
• Dwarka Orthopaedic
Hospital (30)
• Jaipur Hospital (93)
• Khandaka Hospital
(30)
• Shubh Hospital,
Vidhyut Nagar (40)
• Maitri Hospital,
Talwandi (50)
• Fortis Escorts (210)
• Soni Medicare (225)
• Sahai Hospital (100)
• Fortis Life Line Hospital
(100)
• Fortis Escorts Hospital,
Malviya Nagar (350)
• Mahaveer Cancer Hospital
(250)
• Rukmini Devi Jaipuriya
Government Hospital (100)
• Rungta Hospital, Malviya
Nagar (100)
• Saket Hospital, Mansarovar,
Jaipur (110)
• Santokba Durlabhji Memorial
Hospital (375)
• Soni Hospital (225)
• Mathura Das Mathur Hospital
(493)
• Sudha Hospital, Talwandi
(350)
• Ramsnehi Chikitsalaya Avm
Anusandhan Kendra (300)
• Mahatma Gandhi
Medical Hospitals (750)
• Mahatma Gandhi
Hospital (820),Jaipur
• Mahatma Gandhi
Hospital (624),Jhodpur
• Umaid Hospital (700)
• Narayana
Hrudayalaya Hospital
(1000)
• Sawai Mansingh
Government Hospital
(1563)
HP
• Indus Hospital (90)
• Delek Hospital (45)
• Mahatma Gandhi Medical
Services Complex Khaneri
(360)
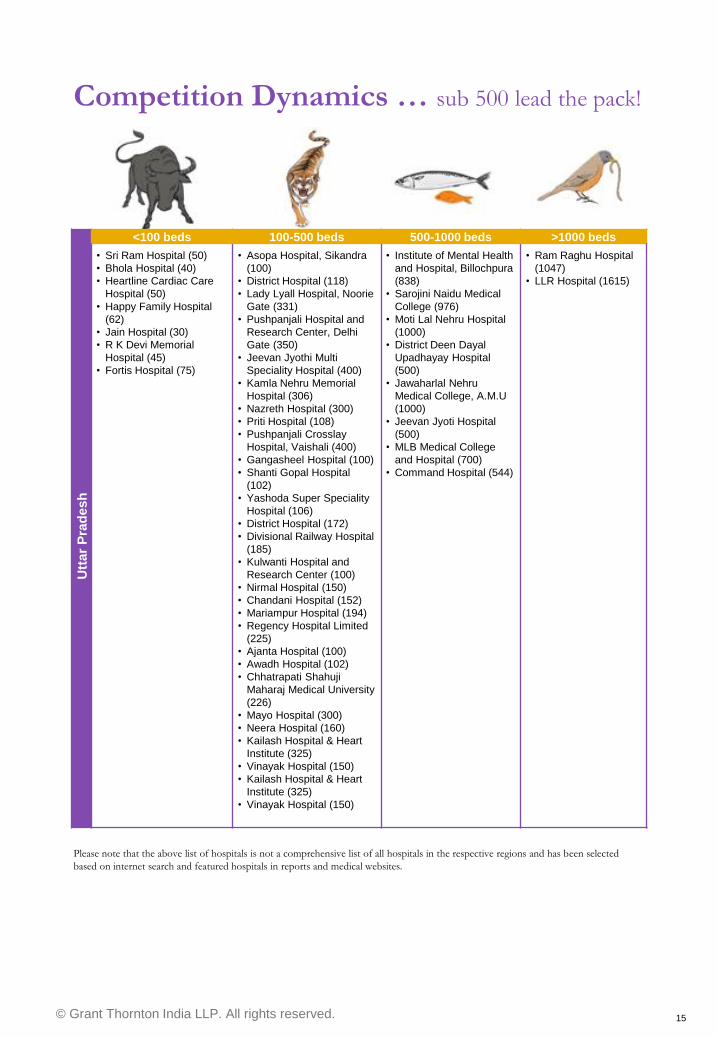
Competition Dynamics … sub 500 lead the pack!
Please note that the above list of hospitals is not a comprehensive list of all hospitals in the respective regions and has been selected
based on internet search and featured hospitals in reports and medical websites.
© Grant Thornton India LLP. All rights reserved. 15
<100 beds 100-500 beds 500-1000 beds >1000 beds
Utt
ar
Pra
desh
• Sri Ram Hospital (50)
• Bhola Hospital (40)
• Heartline Cardiac Care
Hospital (50)
• Happy Family Hospital
(62)
• Jain Hospital (30)
• R K Devi Memorial
Hospital (45)
• Fortis Hospital (75)
• Asopa Hospital, Sikandra
(100)
• District Hospital (118)
• Lady Lyall Hospital, Noorie
Gate (331)
• Pushpanjali Hospital and
Research Center, Delhi
Gate (350)
• Jeevan Jyothi Multi
Speciality Hospital (400)
• Kamla Nehru Memorial
Hospital (306)
• Nazreth Hospital (300)
• Priti Hospital (108)
• Pushpanjali Crosslay
Hospital, Vaishali (400)
• Gangasheel Hospital (100)
• Shanti Gopal Hospital
(102)
• Yashoda Super Speciality
Hospital (106)
• District Hospital (172)
• Divisional Railway Hospital
(185)
• Kulwanti Hospital and
Research Center (100)
• Nirmal Hospital (150)
• Chandani Hospital (152)
• Mariampur Hospital (194)
• Regency Hospital Limited
(225)
• Ajanta Hospital (100)
• Awadh Hospital (102)
• Chhatrapati Shahuji
Maharaj Medical University
(226)
• Mayo Hospital (300)
• Neera Hospital (160)
• Kailash Hospital & Heart
Institute (325)
• Vinayak Hospital (150)
• Kailash Hospital & Heart
Institute (325)
• Vinayak Hospital (150)
• Institute of Mental Health
and Hospital, Billochpura
(838)
• Sarojini Naidu Medical
College (976)
• Moti Lal Nehru Hospital
(1000)
• District Deen Dayal
Upadhayay Hospital
(500)
• Jawaharlal Nehru
Medical College, A.M.U
(1000)
• Jeevan Jyoti Hospital
(500)
• MLB Medical College
and Hospital (700)
• Command Hospital (544)
• Ram Raghu Hospital
(1047)
• LLR Hospital (1615)
Competition Dynamics … sub 500 lead the pack!
Please note that the above list of hospitals is not a comprehensive list of all hospitals in the respective regions and has been selected
based on internet search and featured hospitals in reports and medical websites.

© Grant Thornton India LLP. All rights reserved. 16
Industry speak
“We need to re-write the blueprint for
Health India…
All three segments (public health
systems, NGOs and private sector)
should be aligned to make a full chain
from ground up…
We have a mass enabler already – in
the form of ASHA - upgrade their
skills, provide access to technology,
clearly define the functionalities, use
mobile units for connectivity to B&C
cities and a national network will be
in place”
Dr Naresh Trehan
Medanta Medicity, envisioned as a
health city, has changed the face of
surgery in India across multiple
specialties.
Dr Amit Sachdeva
Axiss Dental is currently a North
India focused chain of dental
centres providing orthodontic and
implantology solutions. The
chain has recently secured
private equity funding from India
Equity Partners.
Dr Manish Chhaparwal
Mewar Ortho provides high quality,
fast turnaround care for patients in Tier
II cities, where there is a dearth of
orthopaedic and allied care facilities.
Mewar has recently completed its first
institutional round of equity funding
from Matrix Partners.
“We aim to keep our capital and
operating costs low and operate our
centres in an environment of patient
centricity –quality surgeries, quick
discharge, technology advancement
and safe infrastructure”
© Grant Thornton India LLP. All rights reserved. 17
Healthcare infrastructure Public health, disease profiles, mortality
rates
© Grant Thornton India LLP. All rights reserved. 18
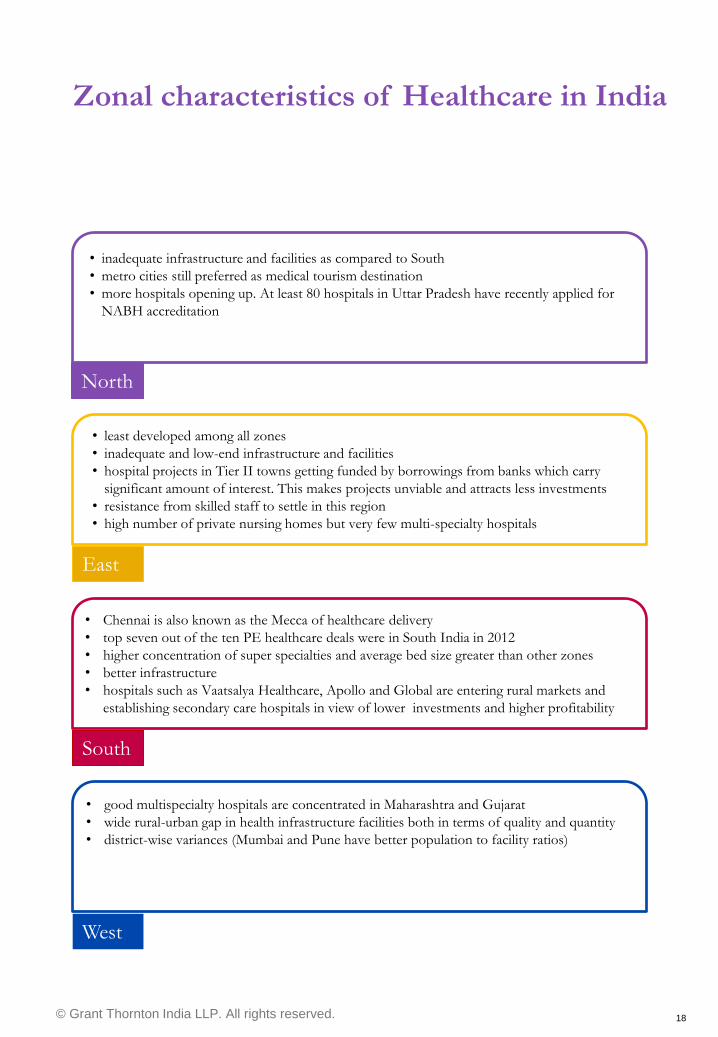
North
• inadequate infrastructure and facilities as compared to South
• metro cities still preferred as medical tourism destination
• more hospitals opening up. At least 80 hospitals in Uttar Pradesh have recently applied for
NABH accreditation
East
• least developed among all zones
• inadequate and low-end infrastructure and facilities
• hospital projects in Tier II towns getting funded by borrowings from banks which carry
significant amount of interest. This makes projects unviable and attracts less investments
• resistance from skilled staff to settle in this region
• high number of private nursing homes but very few multi-specialty hospitals
South
• Chennai is also known as the Mecca of healthcare delivery
• top seven out of the ten PE healthcare deals were in South India in 2012
• higher concentration of super specialties and average bed size greater than other zones
• better infrastructure
• hospitals such as Vaatsalya Healthcare, Apollo and Global are entering rural markets and
establishing secondary care hospitals in view of lower investments and higher profitability
West
• good multispecialty hospitals are concentrated in Maharashtra and Gujarat
• wide rural-urban gap in health infrastructure facilities both in terms of quality and quantity
• district-wise variances (Mumbai and Pune have better population to facility ratios)
Zonal characteristics of Healthcare in India
© Grant Thornton India LLP. All rights reserved. 19
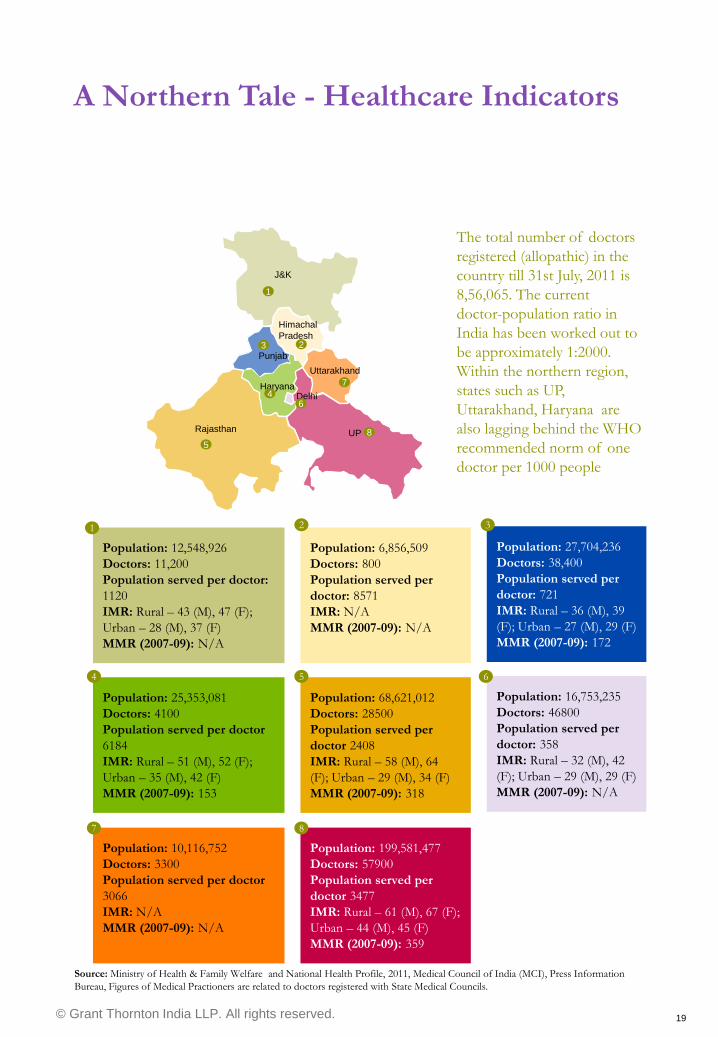
Population: 12,548,926
Doctors: 11,200
Population served per doctor:
1120
IMR: Rural – 43 (M), 47 (F);
Urban – 28 (M), 37 (F)
MMR (2007-09): N/A
Population: 6,856,509
Doctors: 800
Population served per
doctor: 8571
IMR: N/A
MMR (2007-09): N/A
Population: 27,704,236
Doctors: 38,400
Population served per
doctor: 721
IMR: Rural – 36 (M), 39
(F); Urban – 27 (M), 29 (F)
MMR (2007-09): 172
Population: 25,353,081
Doctors: 4100
Population served per doctor
6184
IMR: Rural – 51 (M), 52 (F);
Urban – 35 (M), 42 (F)
MMR (2007-09): 153
Population: 68,621,012
Doctors: 28500
Population served per
doctor 2408
IMR: Rural – 58 (M), 64
(F); Urban – 29 (M), 34 (F)
MMR (2007-09): 318
Population: 16,753,235
Doctors: 46800
Population served per
doctor: 358
IMR: Rural – 32 (M), 42
(F); Urban – 29 (M), 29 (F)
MMR (2007-09): N/A
Population: 10,116,752
Doctors: 3300
Population served per doctor
3066
IMR: N/A
MMR (2007-09): N/A
Population: 199,581,477
Doctors: 57900
Population served per
doctor 3477
IMR: Rural – 61 (M), 67 (F);
Urban – 44 (M), 45 (F)
MMR (2007-09): 359
1 2 3
4 5 6
7 8
Source: Ministry of Health & Family Welfare and National Health Profile, 2011, Medical Council of India (MCI), Press Information
Bureau, Figures of Medical Practioners are related to doctors registered with State Medical Councils.
J&K
Rajasthan UP
Himachal
Pradesh
Punjab
Haryana
Uttarakhand
Delhi
1
2 3
4
5
6
7
8
The total number of doctors
registered (allopathic) in the
country till 31st July, 2011 is
8,56,065. The current
doctor-population ratio in
India has been worked out to
be approximately 1:2000.
Within the northern region,
states such as UP,
Uttarakhand, Haryana are
also lagging behind the WHO
recommended norm of one
doctor per 1000 people
A Northern Tale - Healthcare Indicators
© Grant Thornton India LLP. All rights reserved. 20
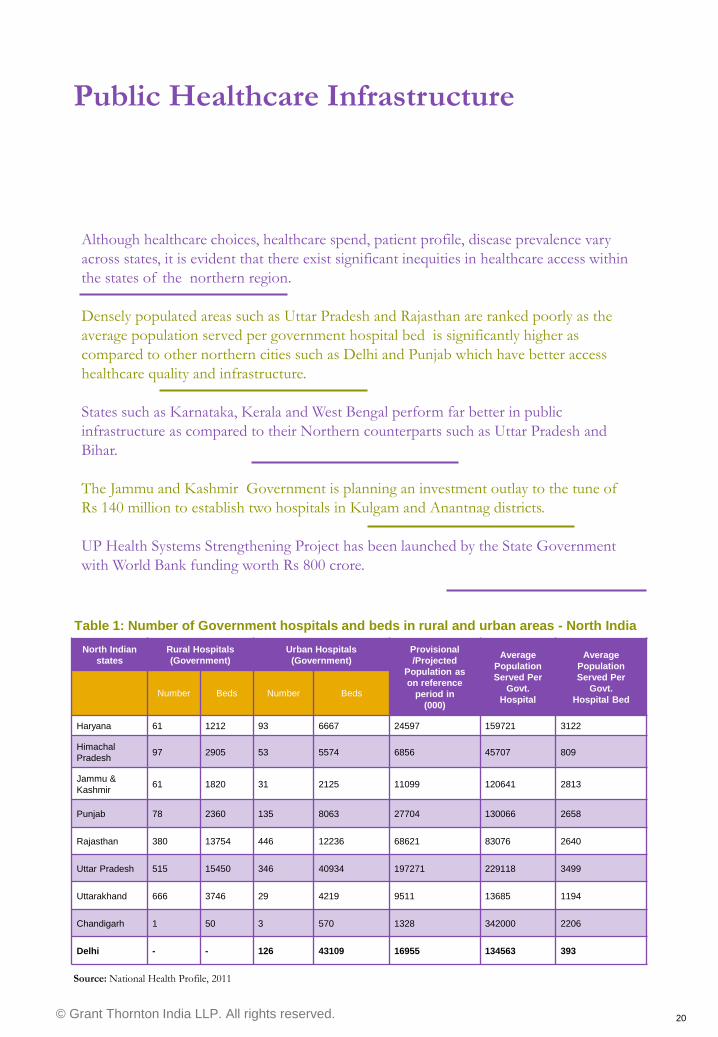
Table 1: Number of Government hospitals and beds in rural and urban areas - North India
North Indian
states
Rural Hospitals
(Government)
Urban Hospitals
(Government)
Provisional
/Projected
Population as
on reference
period in
(000)
Average
Population
Served Per
Govt.
Hospital
Average
Population
Served Per
Govt.
Hospital Bed Number Beds Number Beds
Haryana 61 1212 93 6667 24597 159721 3122
Himachal
Pradesh 97 2905 53 5574 6856 45707 809
Jammu &
Kashmir 61 1820 31 2125 11099 120641 2813
Punjab 78 2360 135 8063 27704 130066 2658
Rajasthan 380 13754 446 12236 68621 83076 2640
Uttar Pradesh 515 15450 346 40934 197271 229118 3499
Uttarakhand 666 3746 29 4219 9511 13685 1194
Chandigarh 1 50 3 570 1328 342000 2206
Delhi - - 126 43109 16955 134563 393
Source: National Health Profile, 2011
Although healthcare choices, healthcare spend, patient profile, disease prevalence vary
across states, it is evident that there exist significant inequities in healthcare access within
the states of the northern region.
Densely populated areas such as Uttar Pradesh and Rajasthan are ranked poorly as the
average population served per government hospital bed is significantly higher as
compared to other northern cities such as Delhi and Punjab which have better access
healthcare quality and infrastructure.
States such as Karnataka, Kerala and West Bengal perform far better in public
infrastructure as compared to their Northern counterparts such as Uttar Pradesh and
Bihar.
The Jammu and Kashmir Government is planning an investment outlay to the tune of
Rs 140 million to establish two hospitals in Kulgam and Anantnag districts.
UP Health Systems Strengthening Project has been launched by the State Government
with World Bank funding worth Rs 800 crore.
Public Healthcare Infrastructure
© Grant Thornton India LLP. All rights reserved. 21
Some recent activities in the healthcare
sector in the northern region
News bytes
© Grant Thornton India LLP. All rights reserved. 22
Fortis Healthcare (India)
plans to launch four
hospitals including one in
Himachal Pradesh to be
operational by 2013, as
part of its plans to
strengthen its nationwide
presence.
Immediate expansion plans
for Mewar Ortho include
setting up a 100–bed
centre of excellence in
Udaipur while also
increasing its footprint in
Central India with centres
in Sirohi, Mandsaur,
Chittorgarh and several
more.
ASG Eye Hospitals, a
Rajasthan based group of
super specialty eye
hospitals has recently
raised Rs 50 crore from
Sequoia Capital. The fund
will support the expansion
plan of the hospital
Metropolis Healthcare has
made investments of Rs
one crore each in Tier II
and Tier III cities such as
Lucknow, Bareilly, and
Jalandhar and has recently
acquired two brownfield
ventures in Chandigarh
and Jodhpur.
Apollo Hospitals Group
launched its first Apollo
Cosmetic Clinic in North
India.
As a part of its expansion
plans over the next couple
of years, Rockland Group
will open a multi-specialty
505 beds hospital in
Manesar, Haryana as well
as a 500 beds hospital in
Greater Noida (Uttar
Pradesh)
Rajasthan based group of
super specialty eye
hospitals, ASG Eye
Hospitals has raised Rs 50
crore from Sequoia Capital
to support expansion in
central and north Indian
states including Madhya
Pradesh, Uttar Pradesh,
Jharkhand, Chhattisgarh
and Bihar
Besides undertaking the
construction of a new 300-
bed hospital at its Medcity
campus, Moolchand
Healthcare has also
earmarked Rs 100 crore
for acquisitions in the
pathology and diagnostic
segment
News bytes
Some recent activities in the healthcare sector in the northern region
© Grant Thornton India LLP. All rights reserved. 23
Investment Horizon Deal trends, options – public and private route

© Grant Thornton India LLP. All rights reserved. 24
Private Funding Options
Establishing and growing a hospital business requires intensive planning and large capital outlay,
which makes it imperative for players to pursue new avenues to meet their capital needs.
2 Capital
Markets
Depends
entirely on
market
conditions,
not easy for
mid-cap
companies
Mezz/ Debt
High fixed
cost,
restrictions
on deal
structures
due to FDI
regulations,
limited
number of
providers
Private
Equity
Growth
Capital –
Most active
in today's
market
Overseas
Listing
Depends on
market
conditions
REIT
Limited
number of
operators,
restrictions
on deal
structures
due to FDI
regulations
1 3 4 5 Angel
Investors
For very
early stage
deals, there
is usually no
other option
6
© Grant Thornton India LLP. All rights reserved. 25
Deal Street
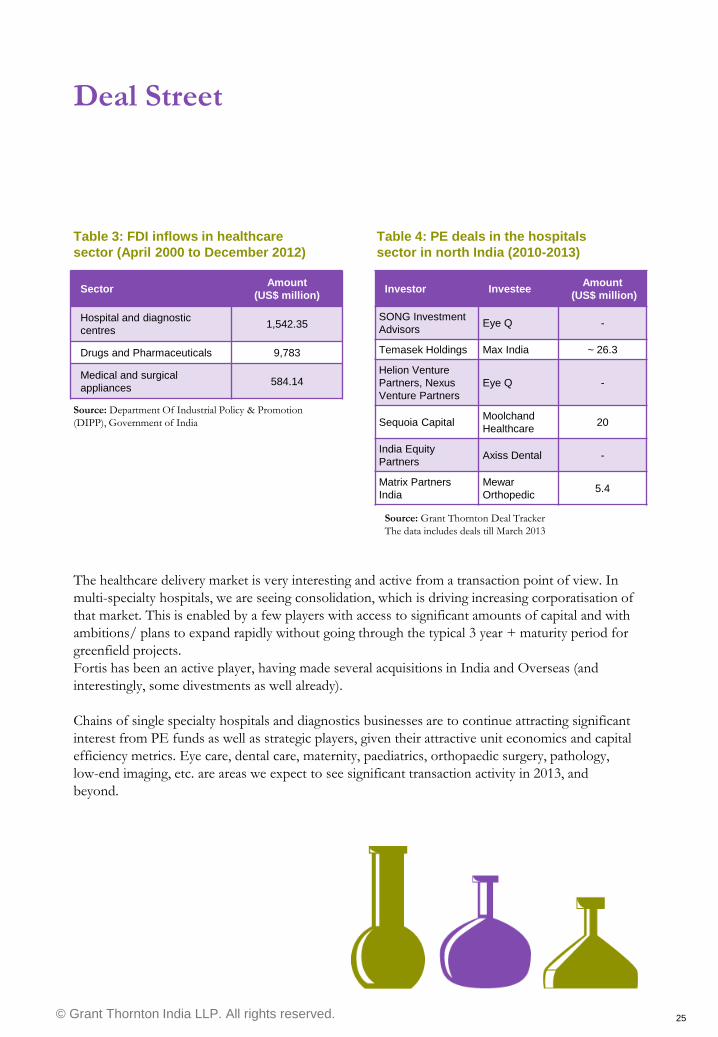
The healthcare delivery market is very interesting and active from a transaction point of view. In
multi-specialty hospitals, we are seeing consolidation, which is driving increasing corporatisation of
that market. This is enabled by a few players with access to significant amounts of capital and with
ambitions/ plans to expand rapidly without going through the typical 3 year + maturity period for
greenfield projects.
Fortis has been an active player, having made several acquisitions in India and Overseas (and
interestingly, some divestments as well already).
Chains of single specialty hospitals and diagnostics businesses are to continue attracting significant
interest from PE funds as well as strategic players, given their attractive unit economics and capital
efficiency metrics. Eye care, dental care, maternity, paediatrics, orthopaedic surgery, pathology,
low-end imaging, etc. are areas we expect to see significant transaction activity in 2013, and
beyond.
Investor Investee Amount
(US$ million)
SONG Investment
Advisors Eye Q -
Temasek Holdings Max India ~ 26.3
Helion Venture
Partners, Nexus
Venture Partners
Eye Q -
Sequoia Capital Moolchand
Healthcare 20
India Equity
Partners Axiss Dental -
Matrix Partners
India
Mewar
Orthopedic 5.4
Source: Grant Thornton Deal Tracker
The data includes deals till March 2013
Table 4: PE deals in the hospitals
sector in north India (2010-2013)
Sector Amount
(US$ million)
Hospital and diagnostic
centres 1,542.35
Drugs and Pharmaceuticals 9,783
Medical and surgical
appliances 584.14
Table 3: FDI inflows in healthcare
sector (April 2000 to December 2012)
Source: Department Of Industrial Policy & Promotion
(DIPP), Government of India
© Grant Thornton India LLP. All rights reserved. 26
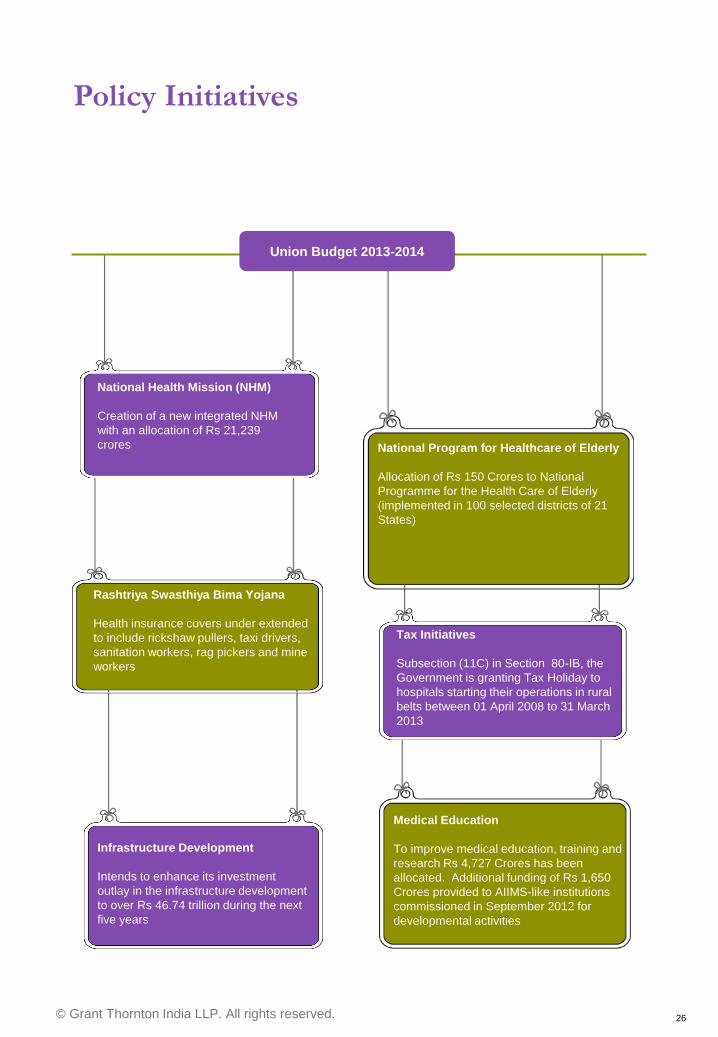
Policy Initiatives
National Health Mission (NHM)
Creation of a new integrated NHM
with an allocation of Rs 21,239
crores
National Program for Healthcare of Elderly
Allocation of Rs 150 Crores to National
Programme for the Health Care of Elderly
(implemented in 100 selected districts of 21
States)
Rashtriya Swasthiya Bima Yojana
Health insurance covers under extended
to include rickshaw pullers, taxi drivers,
sanitation workers, rag pickers and mine
workers
Infrastructure Development
Intends to enhance its investment
outlay in the infrastructure development
to over Rs 46.74 trillion during the next
five years
Medical Education
To improve medical education, training and
research Rs 4,727 Crores has been
allocated. Additional funding of Rs 1,650
Crores provided to AIIMS-like institutions
commissioned in September 2012 for
developmental activities
Tax Initiatives
Subsection (11C) in Section 80-IB, the
Government is granting Tax Holiday to
hospitals starting their operations in rural
belts between 01 April 2008 to 31 March
2013
Union Budget 2013-2014
© Grant Thornton India LLP. All rights reserved. 27
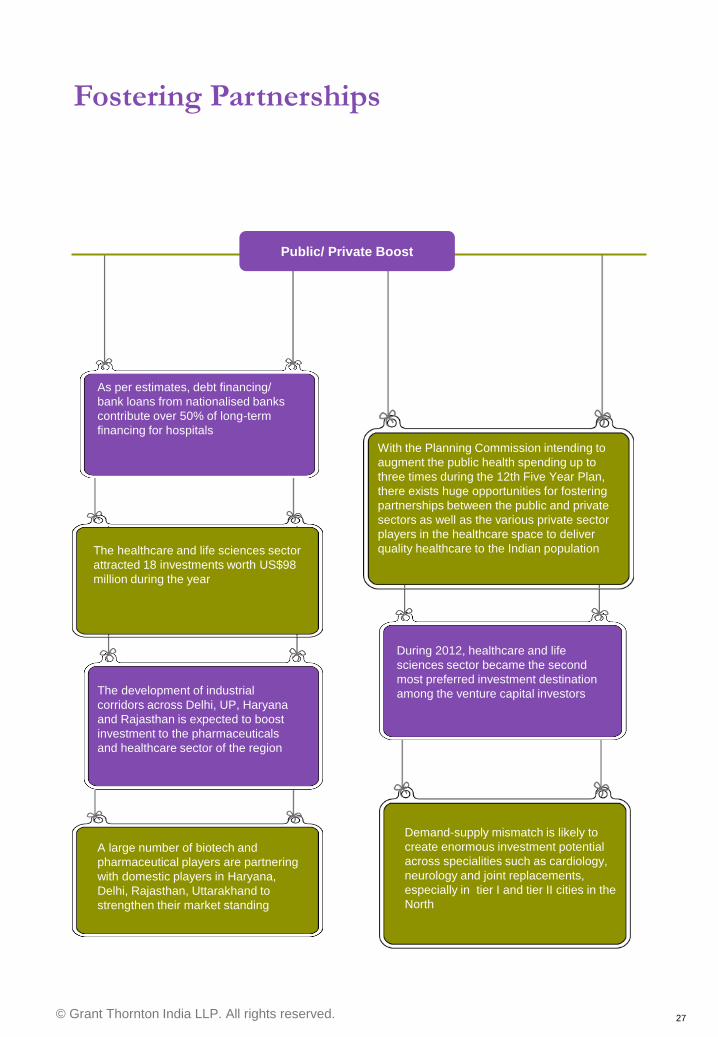
Fostering Partnerships
As per estimates, debt financing/
bank loans from nationalised banks
contribute over 50% of long-term
financing for hospitals
With the Planning Commission intending to
augment the public health spending up to
three times during the 12th Five Year Plan,
there exists huge opportunities for fostering
partnerships between the public and private
sectors as well as the various private sector
players in the healthcare space to deliver
quality healthcare to the Indian population
During 2012, healthcare and life
sciences sector became the second
most preferred investment destination
among the venture capital investors
The healthcare and life sciences sector
attracted 18 investments worth US$98
million during the year
The development of industrial
corridors across Delhi, UP, Haryana
and Rajasthan is expected to boost
investment to the pharmaceuticals
and healthcare sector of the region
A large number of biotech and
pharmaceutical players are partnering
with domestic players in Haryana,
Delhi, Rajasthan, Uttarakhand to
strengthen their market standing
Demand-supply mismatch is likely to
create enormous investment potential
across specialities such as cardiology,
neurology and joint replacements,
especially in tier I and tier II cities in the
North
Public/ Private Boost

© Grant Thornton India LLP. All rights reserved. 28
Changing trends Improving healthcare delivery
© Grant Thornton India LLP. All rights reserved. 29
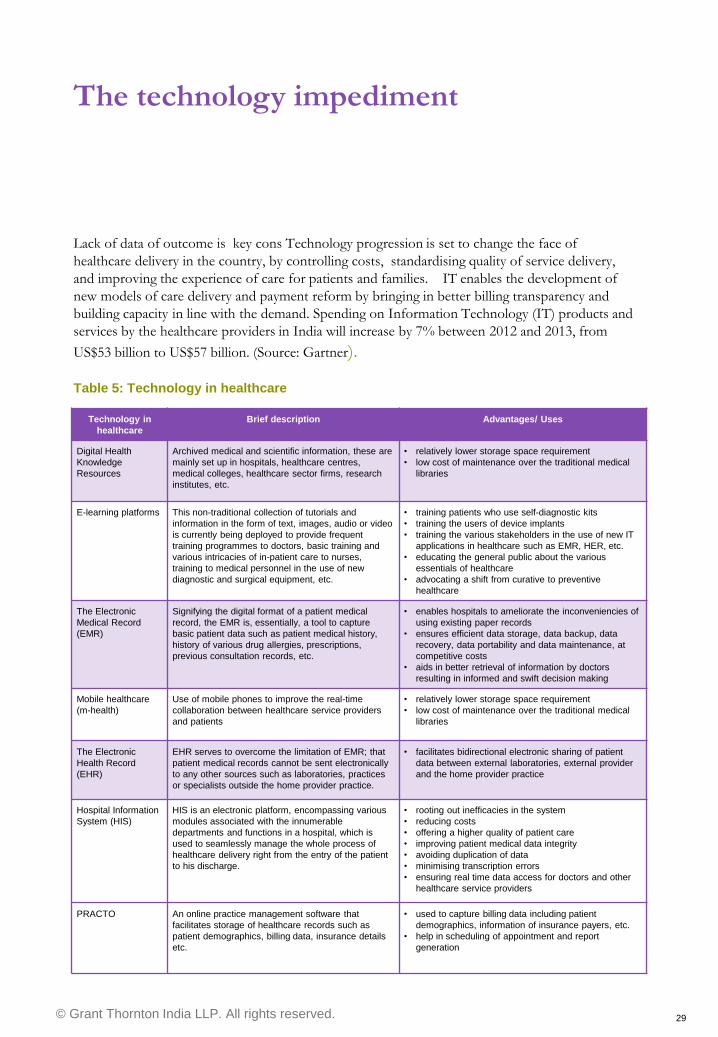
The technology impediment
Lack of data of outcome is key cons Technology progression is set to change the face of
healthcare delivery in the country, by controlling costs, standardising quality of service delivery,
and improving the experience of care for patients and families. IT enables the development of
new models of care delivery and payment reform by bringing in better billing transparency and
building capacity in line with the demand. Spending on Information Technology (IT) products and
services by the healthcare providers in India will increase by 7% between 2012 and 2013, from
US$53 billion to US$57 billion. (Source: Gartner).
Technology in
healthcare
Brief description Advantages/ Uses
Digital Health
Knowledge
Resources
Archived medical and scientific information, these are
mainly set up in hospitals, healthcare centres,
medical colleges, healthcare sector firms, research
institutes, etc.
• relatively lower storage space requirement
• low cost of maintenance over the traditional medical
libraries
E-learning platforms This non-traditional collection of tutorials and
information in the form of text, images, audio or video
is currently being deployed to provide frequent
training programmes to doctors, basic training and
various intricacies of in-patient care to nurses,
training to medical personnel in the use of new
diagnostic and surgical equipment, etc.
• training patients who use self-diagnostic kits
• training the users of device implants
• training the various stakeholders in the use of new IT
applications in healthcare such as EMR, HER, etc.
• educating the general public about the various
essentials of healthcare
• advocating a shift from curative to preventive
healthcare
The Electronic
Medical Record
(EMR)
Signifying the digital format of a patient medical
record, the EMR is, essentially, a tool to capture
basic patient data such as patient medical history,
history of various drug allergies, prescriptions,
previous consultation records, etc.
• enables hospitals to ameliorate the inconveniencies of
using existing paper records
• ensures efficient data storage, data backup, data
recovery, data portability and data maintenance, at
competitive costs
• aids in better retrieval of information by doctors
resulting in informed and swift decision making
Mobile healthcare
(m-health)
Use of mobile phones to improve the real-time
collaboration between healthcare service providers
and patients
• relatively lower storage space requirement
• low cost of maintenance over the traditional medical
libraries
The Electronic
Health Record
(EHR)
EHR serves to overcome the limitation of EMR; that
patient medical records cannot be sent electronically
to any other sources such as laboratories, practices
or specialists outside the home provider practice.
• facilitates bidirectional electronic sharing of patient
data between external laboratories, external provider
and the home provider practice
Hospital Information
System (HIS)
HIS is an electronic platform, encompassing various
modules associated with the innumerable
departments and functions in a hospital, which is
used to seamlessly manage the whole process of
healthcare delivery right from the entry of the patient
to his discharge.
• rooting out inefficacies in the system
• reducing costs
• offering a higher quality of patient care
• improving patient medical data integrity
• avoiding duplication of data
• minimising transcription errors
• ensuring real time data access for doctors and other
healthcare service providers
PRACTO An online practice management software that
facilitates storage of healthcare records such as
patient demographics, billing data, insurance details
etc.
• used to capture billing data including patient
demographics, information of insurance payers, etc.
• help in scheduling of appointment and report
generation
Table 5: Technology in healthcare

© Grant Thornton India LLP. All rights reserved. 30
Tele-docs and Tele-medicine
A novel idea implemented by
Haryana Jiva International, a
healthcare venture on the outskirts
of Delhi. It deploys a GPRS enabled
Java application to enhance the
reach of medical care to rural parts
of the region. The project, known as
the “Teledoc” project, has won
widespread acclaim globally,
including the World Summit Award
for eHealth.
Grameen Foundation has rolled
out an m-health service for AIDS
patients in India. The application
is used to send healthy living
tips, messages and reminders
regarding consultations and
medications to AIDS patients.
In a recent report for the 12th Five Year Plan, the steering committee on health has
recommended connecting all the district hospitals to tertiary care centres by telemedicine
using applications such as “Skype” which facilitate audio-visual interactions. The committee
also advocates adoption of mobile health solutions to enhance real-time collaboration
between patients and providers and between providers, improvement in the rate of
transmission of data and information between the various stakeholders and promotion for
the adoption of preventive healthcare across the various Indian states.
© Grant Thornton India LLP. All rights reserved. 31
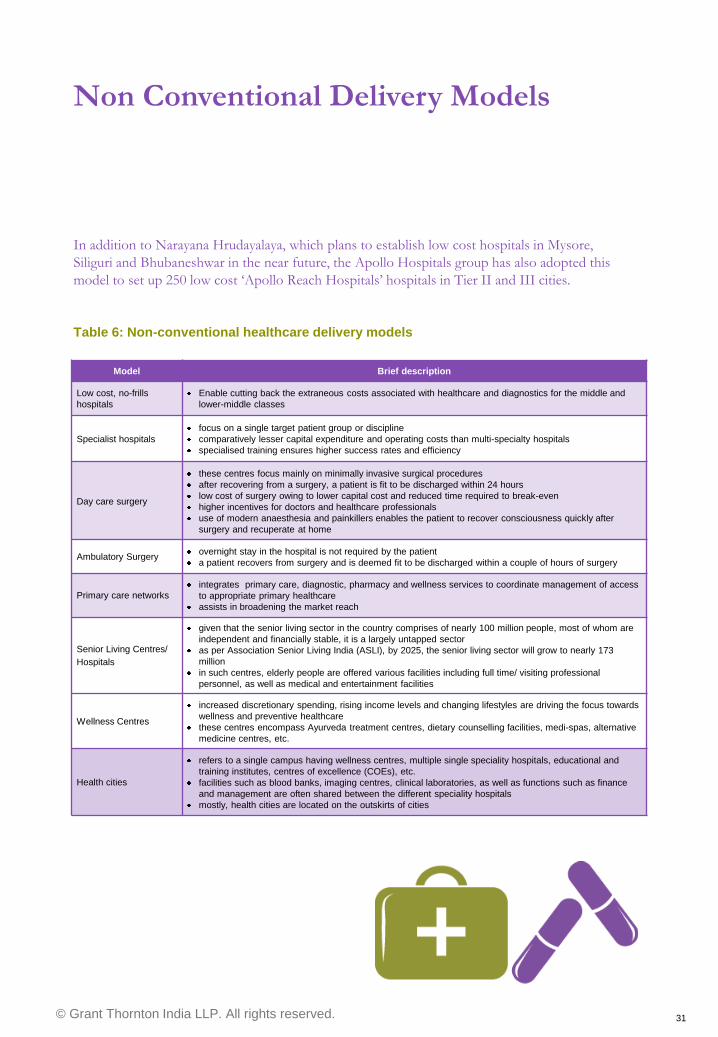
Non Conventional Delivery Models
In addition to Narayana Hrudayalaya, which plans to establish low cost hospitals in Mysore,
Siliguri and Bhubaneshwar in the near future, the Apollo Hospitals group has also adopted this
model to set up 250 low cost „Apollo Reach Hospitals‟ hospitals in Tier II and III cities.
Model Brief description
Low cost, no-frills
hospitals
Enable cutting back the extraneous costs associated with healthcare and diagnostics for the middle and
lower-middle classes
Specialist hospitals
focus on a single target patient group or discipline
comparatively lesser capital expenditure and operating costs than multi-specialty hospitals
specialised training ensures higher success rates and efficiency
Day care surgery
these centres focus mainly on minimally invasive surgical procedures
after recovering from a surgery, a patient is fit to be discharged within 24 hours
low cost of surgery owing to lower capital cost and reduced time required to break-even
higher incentives for doctors and healthcare professionals
use of modern anaesthesia and painkillers enables the patient to recover consciousness quickly after
surgery and recuperate at home
Ambulatory Surgery overnight stay in the hospital is not required by the patient
a patient recovers from surgery and is deemed fit to be discharged within a couple of hours of surgery
Primary care networks integrates primary care, diagnostic, pharmacy and wellness services to coordinate management of access
to appropriate primary healthcare
assists in broadening the market reach
Senior Living Centres/
Hospitals
given that the senior living sector in the country comprises of nearly 100 million people, most of whom are
independent and financially stable, it is a largely untapped sector
as per Association Senior Living India (ASLI), by 2025, the senior living sector will grow to nearly 173
million
in such centres, elderly people are offered various facilities including full time/ visiting professional
personnel, as well as medical and entertainment facilities
Wellness Centres
increased discretionary spending, rising income levels and changing lifestyles are driving the focus towards
wellness and preventive healthcare
these centres encompass Ayurveda treatment centres, dietary counselling facilities, medi-spas, alternative
medicine centres, etc.
Health cities
refers to a single campus having wellness centres, multiple single speciality hospitals, educational and
training institutes, centres of excellence (COEs), etc.
facilities such as blood banks, imaging centres, clinical laboratories, as well as functions such as finance
and management are often shared between the different speciality hospitals
mostly, health cities are located on the outskirts of cities
Table 6: Non-conventional healthcare delivery models
© Grant Thornton India LLP. All rights reserved. 32
Outlook Strategic recommendations
© Grant Thornton India LLP. All rights reserved. 33
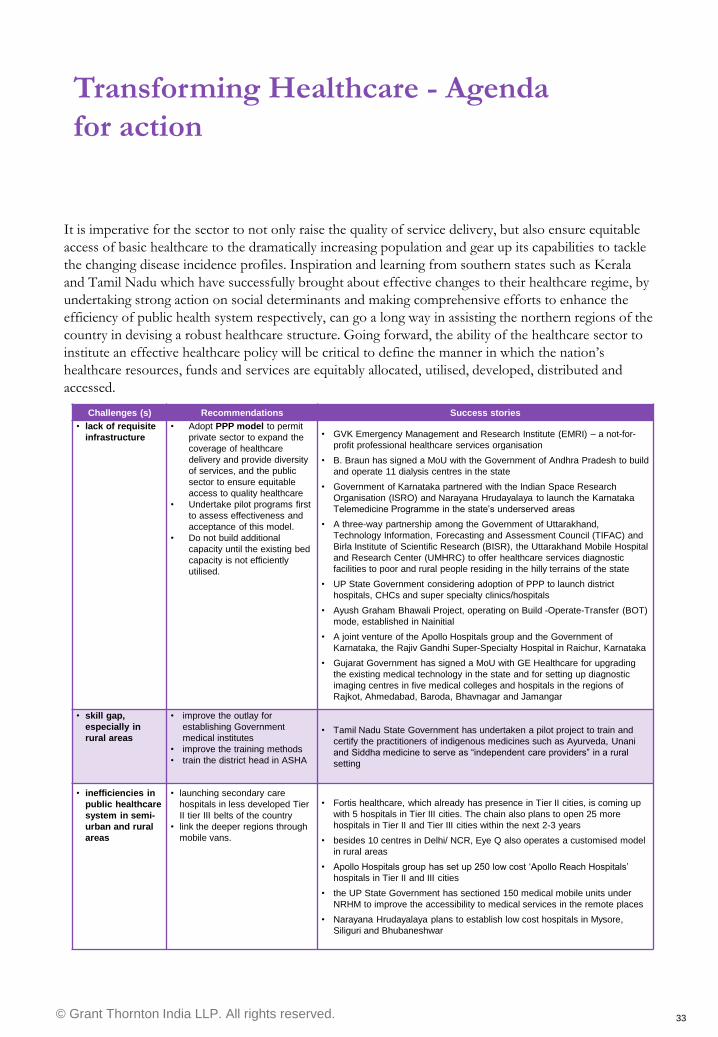
Transforming Healthcare - Agenda
for action
Challenges (s) Recommendations Success stories
• lack of requisite
infrastructure
• Adopt PPP model to permit
private sector to expand the
coverage of healthcare
delivery and provide diversity
of services, and the public
sector to ensure equitable
access to quality healthcare
• Undertake pilot programs first
to assess effectiveness and
acceptance of this model.
• Do not build additional
capacity until the existing bed
capacity is not efficiently
utilised.
• GVK Emergency Management and Research Institute (EMRI) – a not-for-
profit professional healthcare services organisation
• B. Braun has signed a MoU with the Government of Andhra Pradesh to build
and operate 11 dialysis centres in the state
• Government of Karnataka partnered with the Indian Space Research
Organisation (ISRO) and Narayana Hrudayalaya to launch the Karnataka
Telemedicine Programme in the state‟s underserved areas
• A three-way partnership among the Government of Uttarakhand,
Technology Information, Forecasting and Assessment Council (TIFAC) and
Birla Institute of Scientific Research (BISR), the Uttarakhand Mobile Hospital
and Research Center (UMHRC) to offer healthcare services diagnostic
facilities to poor and rural people residing in the hilly terrains of the state
• UP State Government considering adoption of PPP to launch district
hospitals, CHCs and super specialty clinics/hospitals
• Ayush Graham Bhawali Project, operating on Build -Operate-Transfer (BOT)
mode, established in Nainitial
• A joint venture of the Apollo Hospitals group and the Government of
Karnataka, the Rajiv Gandhi Super-Specialty Hospital in Raichur, Karnataka
• Gujarat Government has signed a MoU with GE Healthcare for upgrading
the existing medical technology in the state and for setting up diagnostic
imaging centres in five medical colleges and hospitals in the regions of
Rajkot, Ahmedabad, Baroda, Bhavnagar and Jamangar
• skill gap,
especially in
rural areas
• improve the outlay for
establishing Government
medical institutes
• improve the training methods
• train the district head in ASHA
• Tamil Nadu State Government has undertaken a pilot project to train and
certify the practitioners of indigenous medicines such as Ayurveda, Unani
and Siddha medicine to serve as “independent care providers” in a rural
setting
• inefficiencies in
public healthcare
system in semi-
urban and rural
areas
• launching secondary care
hospitals in less developed Tier
II tier III belts of the country
• link the deeper regions through
mobile vans.
• Fortis healthcare, which already has presence in Tier II cities, is coming up
with 5 hospitals in Tier III cities. The chain also plans to open 25 more
hospitals in Tier II and Tier III cities within the next 2-3 years
• besides 10 centres in Delhi/ NCR, Eye Q also operates a customised model
in rural areas
• Apollo Hospitals group has set up 250 low cost „Apollo Reach Hospitals‟
hospitals in Tier II and III cities
• the UP State Government has sectioned 150 medical mobile units under
NRHM to improve the accessibility to medical services in the remote places
• Narayana Hrudayalaya plans to establish low cost hospitals in Mysore,
Siliguri and Bhubaneshwar
It is imperative for the sector to not only raise the quality of service delivery, but also ensure equitable
access of basic healthcare to the dramatically increasing population and gear up its capabilities to tackle
the changing disease incidence profiles. Inspiration and learning from southern states such as Kerala
and Tamil Nadu which have successfully brought about effective changes to their healthcare regime, by
undertaking strong action on social determinants and making comprehensive efforts to enhance the
efficiency of public health system respectively, can go a long way in assisting the northern regions of the
country in devising a robust healthcare structure. Going forward, the ability of the healthcare sector to
institute an effective healthcare policy will be critical to define the manner in which the nation‟s
healthcare resources, funds and services are equitably allocated, utilised, developed, distributed and
accessed.
© Grant Thornton India LLP. All rights reserved. 34
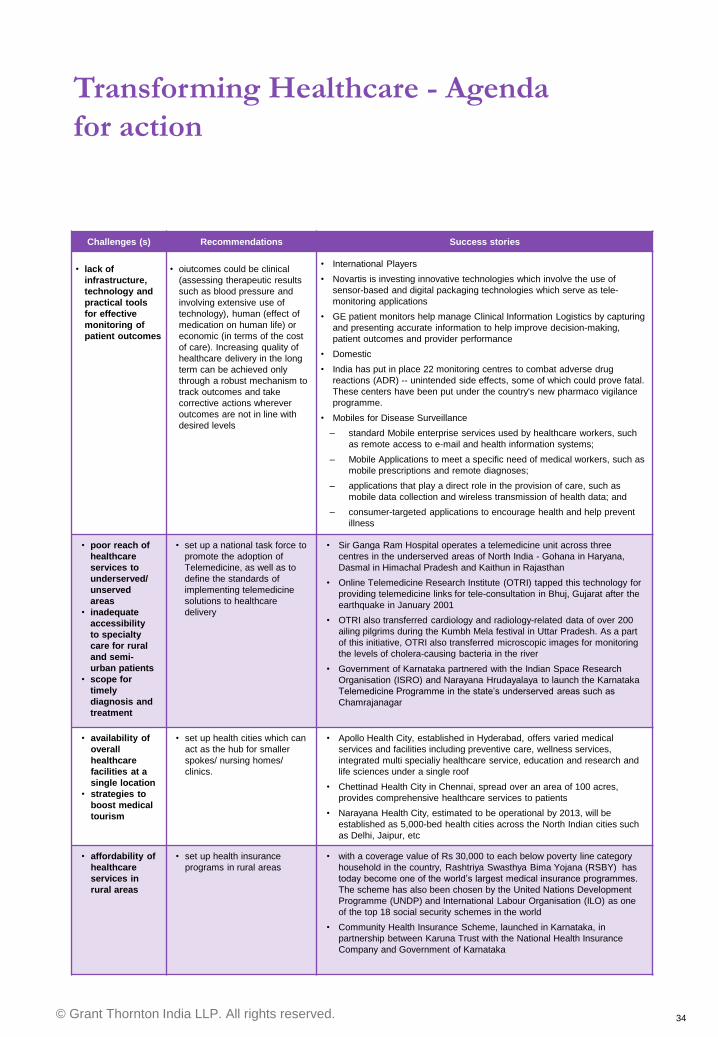
Challenges (s) Recommendations Success stories
• lack of
infrastructure,
technology and
practical tools
for effective
monitoring of
patient outcomes
• oiutcomes could be clinical
(assessing therapeutic results
such as blood pressure and
involving extensive use of
technology), human (effect of
medication on human life) or
economic (in terms of the cost
of care). Increasing quality of
healthcare delivery in the long
term can be achieved only
through a robust mechanism to
track outcomes and take
corrective actions wherever
outcomes are not in line with
desired levels
• International Players
• Novartis is investing innovative technologies which involve the use of
sensor-based and digital packaging technologies which serve as tele-
monitoring applications
• GE patient monitors help manage Clinical Information Logistics by capturing
and presenting accurate information to help improve decision-making,
patient outcomes and provider performance
• Domestic
• India has put in place 22 monitoring centres to combat adverse drug
reactions (ADR) -- unintended side effects, some of which could prove fatal.
These centers have been put under the country's new pharmaco vigilance
programme.
• Mobiles for Disease Surveillance
‒ standard Mobile enterprise services used by healthcare workers, such
as remote access to e-mail and health information systems;
‒ Mobile Applications to meet a specific need of medical workers, such as
mobile prescriptions and remote diagnoses;
‒ applications that play a direct role in the provision of care, such as
mobile data collection and wireless transmission of health data; and
‒ consumer-targeted applications to encourage health and help prevent
illness
• poor reach of
healthcare
services to
underserved/
unserved
areas
• inadequate
accessibility
to specialty
care for rural
and semi-
urban patients
• scope for
timely
diagnosis and
treatment
• set up a national task force to
promote the adoption of
Telemedicine, as well as to
define the standards of
implementing telemedicine
solutions to healthcare
delivery
• Sir Ganga Ram Hospital operates a telemedicine unit across three
centres in the underserved areas of North India - Gohana in Haryana,
Dasmal in Himachal Pradesh and Kaithun in Rajasthan
• Online Telemedicine Research Institute (OTRI) tapped this technology for
providing telemedicine links for tele-consultation in Bhuj, Gujarat after the
earthquake in January 2001
• OTRI also transferred cardiology and radiology-related data of over 200
ailing pilgrims during the Kumbh Mela festival in Uttar Pradesh. As a part
of this initiative, OTRI also transferred microscopic images for monitoring
the levels of cholera-causing bacteria in the river
• Government of Karnataka partnered with the Indian Space Research
Organisation (ISRO) and Narayana Hrudayalaya to launch the Karnataka
Telemedicine Programme in the state‟s underserved areas such as
Chamrajanagar
• availability of
overall
healthcare
facilities at a
single location
• strategies to
boost medical
tourism
• set up health cities which can
act as the hub for smaller
spokes/ nursing homes/
clinics.
• Apollo Health City, established in Hyderabad, offers varied medical
services and facilities including preventive care, wellness services,
integrated multi specialiy healthcare service, education and research and
life sciences under a single roof
• Chettinad Health City in Chennai, spread over an area of 100 acres,
provides comprehensive healthcare services to patients
• Narayana Health City, estimated to be operational by 2013, will be
established as 5,000-bed health cities across the North Indian cities such
as Delhi, Jaipur, etc
• affordability of
healthcare
services in
rural areas
• set up health insurance
programs in rural areas
• with a coverage value of Rs 30,000 to each below poverty line category
household in the country, Rashtriya Swasthya Bima Yojana (RSBY) has
today become one of the world‟s largest medical insurance programmes.
The scheme has also been chosen by the United Nations Development
Programme (UNDP) and International Labour Organisation (ILO) as one
of the top 18 social security schemes in the world
• Community Health Insurance Scheme, launched in Karnataka, in
partnership between Karuna Trust with the National Health Insurance
Company and Government of Karnataka
Transforming Healthcare - Agenda
for action
© Grant Thornton India LLP. All rights reserved. 35
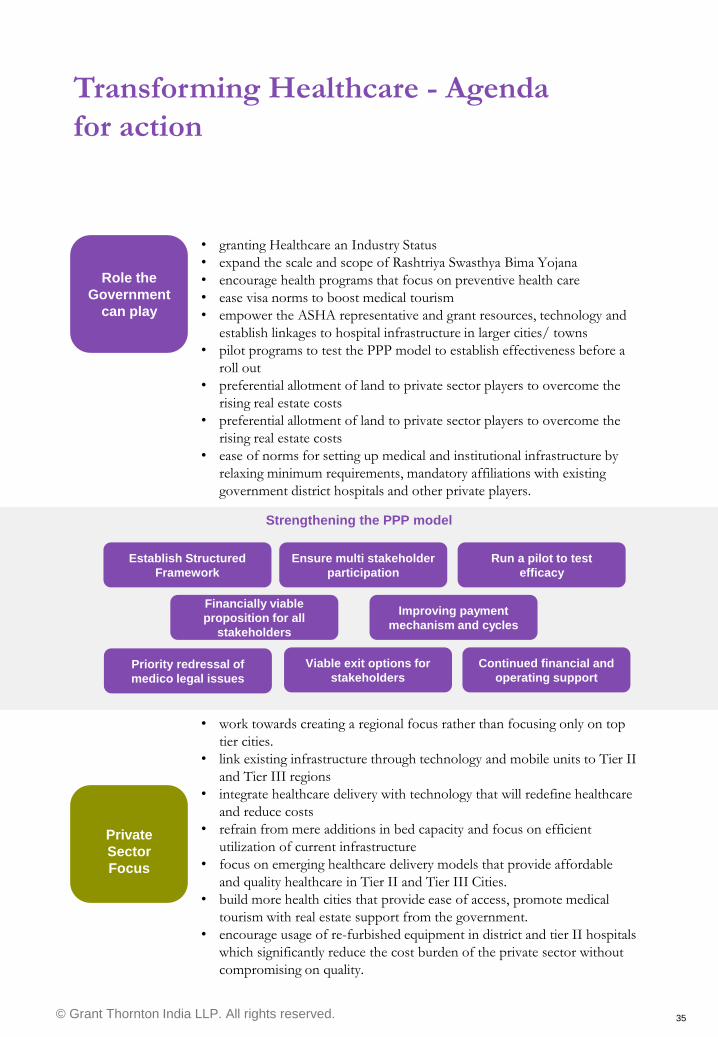
Transforming Healthcare - Agenda
for action
Role the
Government
can play
Private
Sector
Focus
Strengthening the PPP model
Establish Structured
Framework
Ensure multi stakeholder
participation
Run a pilot to test
efficacy
Financially viable
proposition for all
stakeholders
Improving payment
mechanism and cycles
Priority redressal of
medico legal issues
Viable exit options for
stakeholders
Continued financial and
operating support
• work towards creating a regional focus rather than focusing only on top
tier cities.
• link existing infrastructure through technology and mobile units to Tier II
and Tier III regions
• integrate healthcare delivery with technology that will redefine healthcare
and reduce costs
• refrain from mere additions in bed capacity and focus on efficient
utilization of current infrastructure
• focus on emerging healthcare delivery models that provide affordable
and quality healthcare in Tier II and Tier III Cities.
• build more health cities that provide ease of access, promote medical
tourism with real estate support from the government.
• encourage usage of re-furbished equipment in district and tier II hospitals
which significantly reduce the cost burden of the private sector without
compromising on quality.
• granting Healthcare an Industry Status
• expand the scale and scope of Rashtriya Swasthya Bima Yojana
• encourage health programs that focus on preventive health care
• ease visa norms to boost medical tourism
• empower the ASHA representative and grant resources, technology and
establish linkages to hospital infrastructure in larger cities/ towns
• pilot programs to test the PPP model to establish effectiveness before a
roll out
• preferential allotment of land to private sector players to overcome the
rising real estate costs
• preferential allotment of land to private sector players to overcome the
rising real estate costs
• ease of norms for setting up medical and institutional infrastructure by
relaxing minimum requirements, mandatory affiliations with existing
government district hospitals and other private players.

© Grant Thornton India LLP. All rights reserved. 36
A regional health strategy
A regional approach for developing sustainable health systems is the only means to address the
ballooning healthcare need of the Northern Region. Combined with innovative delivery models
and technological interface to bring regions together, Healthcare continues to remain one of the
most promising sectors for the Indian Economy for the coming decade and thereafter.
A regional focus can be maintained either through the current state wise institutional
framework or by channelizing the existing ecosystem of district/ civil hospitals, smaller
hospitals/ nursing care to larger hospitals in Tier I and Tier II cities. Spreading out
delivery models on the basis of the population profile of regions and doctor availability
will ensure equitable allocation of healthcare resources across all regions
Reach
Integration
Keeping the drivers in mind
Developing a clinical pathway
Skill enhancement
Integration of primary care and hospital based infrastructure to provide seamless,
uniform and pro-active care, keeping in mind the level of clinician support (doctor
availability and referral channels) that are available in and around such regions.
Ageing population profile, disease prevalence and general medical technology are key
drivers fueling the demand for healthcare in the Northern Region.
Depending on the need and complexity of surgical intervention, every doctor/
representative at the bottom of the clinical ecocystem shall decide on what activities can
be done at the primary centre level, what needs to be referred to relatively larger
hospitals/ nursing homes and finally acute needs which may need to be referred to
specialty hospitals with skilled professionals. A clear, well defined policy framework of
this clinical pathway is critical for the creation of a holistic and interlinked regional
healthcare system.
Overcome resistance of skilled medical professionals in moving to Tier II, Tier III cities
by creating a timetable of periodic mobility of professionals across deeper regions.
Develop adequate infrastructure and provide institutional support by regular and
continuous training of medical doctors and other skilled manpower to service the sector
Infrastructure support
Reducing the real estate burden and providing support for setting up infrastructure
across the entire spectrum of this regional ecosystem.
© Grant Thornton India LLP. All rights reserved. 37
Appendices Healthcare Indicators, Deal summary
© Grant Thornton India LLP. All rights reserved. 38
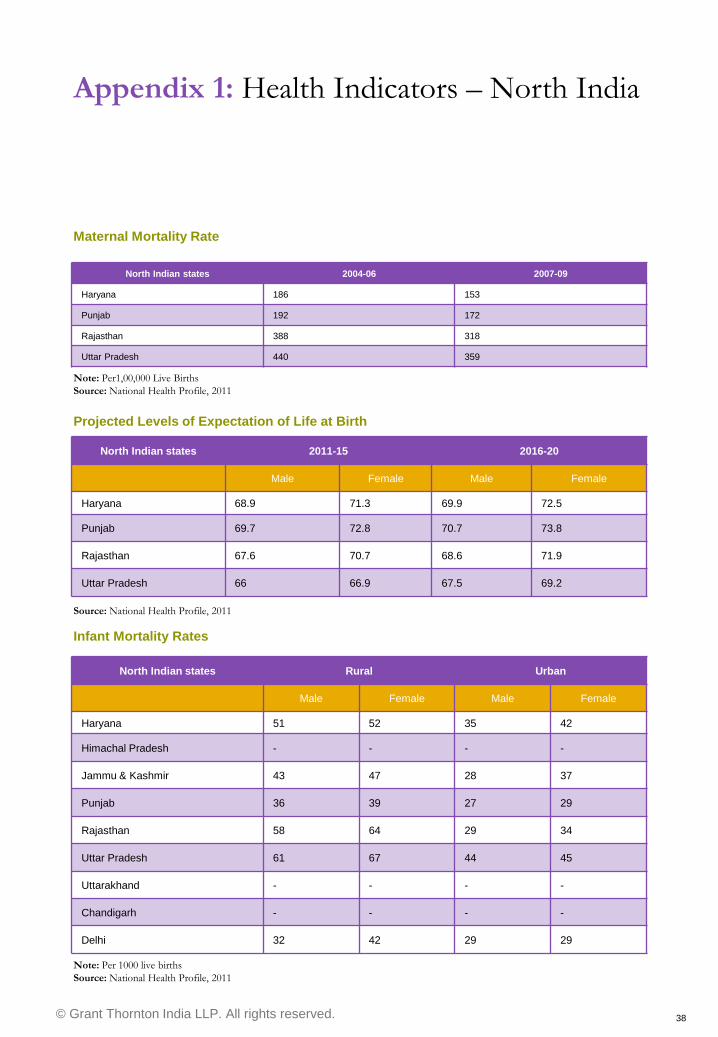
Maternal Mortality Rate
North Indian states 2004-06 2007-09
Haryana 186 153
Punjab 192 172
Rajasthan 388 318
Uttar Pradesh 440 359
Note: Per1,00,000 Live Births
Source: National Health Profile, 2011
Projected Levels of Expectation of Life at Birth
North Indian states 2011-15 2016-20
Male Female Male Female
Haryana 68.9 71.3 69.9 72.5
Punjab 69.7 72.8 70.7 73.8
Rajasthan 67.6 70.7 68.6 71.9
Uttar Pradesh 66 66.9 67.5 69.2
Source: National Health Profile, 2011
Infant Mortality Rates
North Indian states Rural Urban
Male Female Male Female
Haryana 51 52 35 42
Himachal Pradesh - - - -
Jammu & Kashmir 43 47 28 37
Punjab 36 39 27 29
Rajasthan 58 64 29 34
Uttar Pradesh 61 67 44 45
Uttarakhand - - - -
Chandigarh - - - -
Delhi 32 42 29 29
Note: Per 1000 live births
Source: National Health Profile, 2011
Appendix 1: Health Indicators – North India
© Grant Thornton India LLP. All rights reserved. 39
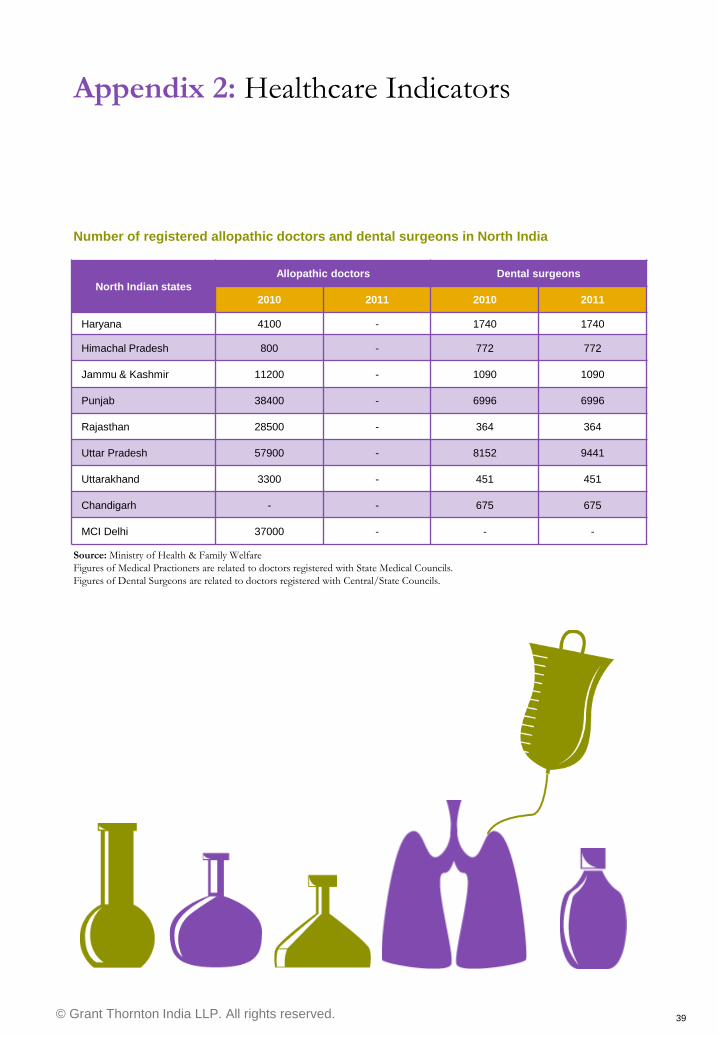
Number of registered allopathic doctors and dental surgeons in North India
Source: Ministry of Health & Family Welfare
Figures of Medical Practioners are related to doctors registered with State Medical Councils.
Figures of Dental Surgeons are related to doctors registered with Central/State Councils.
North Indian states
Allopathic doctors Dental surgeons
2010 2011 2010 2011
Haryana 4100 - 1740 1740
Himachal Pradesh 800 - 772 772
Jammu & Kashmir 11200 - 1090 1090
Punjab 38400 - 6996 6996
Rajasthan 28500 - 364 364
Uttar Pradesh 57900 - 8152 9441
Uttarakhand 3300 - 451 451
Chandigarh - - 675 675
MCI Delhi 37000 - - -
Appendix 2: Healthcare Indicators
© Grant Thornton India LLP. All rights reserved. 40
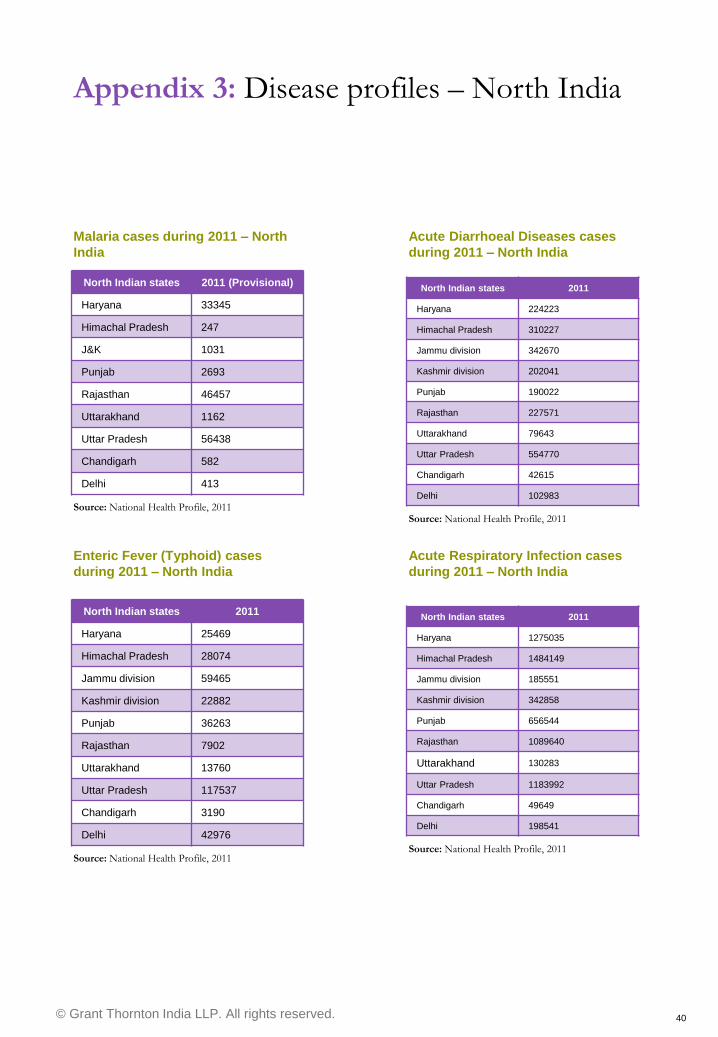
Malaria cases during 2011 – North
India
Source: National Health Profile, 2011
Appendix 3: Disease profiles – North India
North Indian states 2011 (Provisional)
Haryana 33345
Himachal Pradesh 247
J&K 1031
Punjab 2693
Rajasthan 46457
Uttarakhand 1162
Uttar Pradesh 56438
Chandigarh 582
Delhi 413
Acute Diarrhoeal Diseases cases
during 2011 – North India
North Indian states 2011
Haryana 224223
Himachal Pradesh 310227
Jammu division 342670
Kashmir division 202041
Punjab 190022
Rajasthan 227571
Uttarakhand 79643
Uttar Pradesh 554770
Chandigarh 42615
Delhi 102983
Source: National Health Profile, 2011
Enteric Fever (Typhoid) cases
during 2011 – North India
Source: National Health Profile, 2011
Acute Respiratory Infection cases
during 2011 – North India
North Indian states 2011
Haryana 1275035
Himachal Pradesh 1484149
Jammu division 185551
Kashmir division 342858
Punjab 656544
Rajasthan 1089640
Uttarakhand 130283
Uttar Pradesh 1183992
Chandigarh 49649
Delhi 198541
Source: National Health Profile, 2011
North Indian states 2011
Haryana 25469
Himachal Pradesh 28074
Jammu division 59465
Kashmir division 22882
Punjab 36263
Rajasthan 7902
Uttarakhand 13760
Uttar Pradesh 117537
Chandigarh 3190
Delhi 42976
© Grant Thornton India LLP. All rights reserved. 41
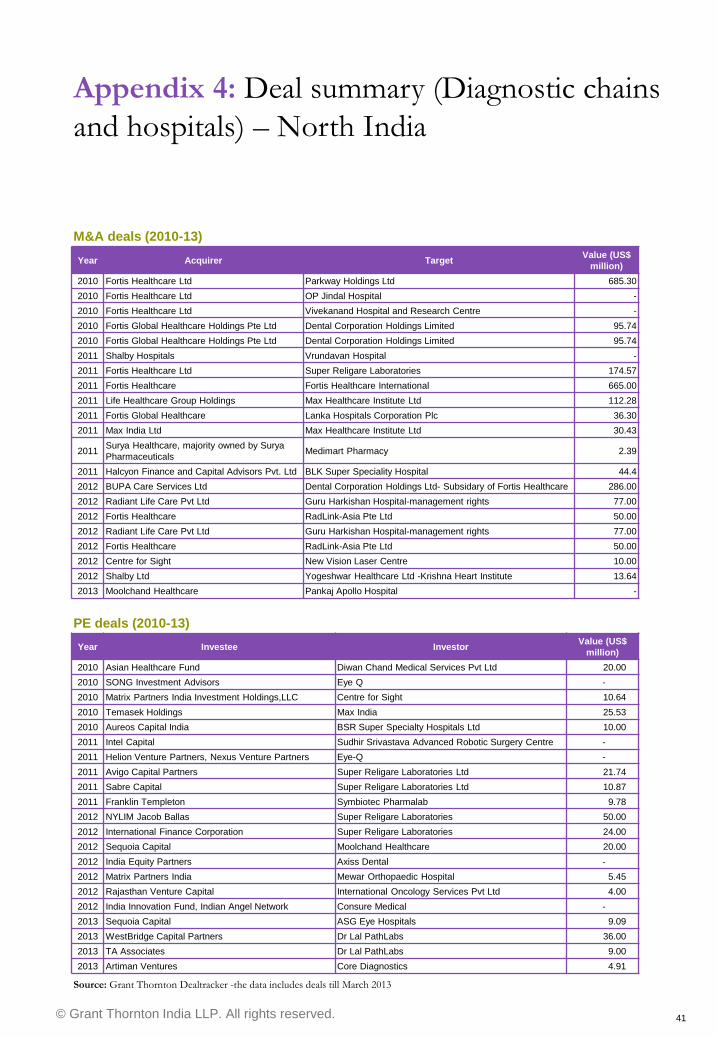
Appendix 4: Deal summary (Diagnostic chains
and hospitals) – North India
Year Acquirer Target Value (US$
million)
2010 Fortis Healthcare Ltd Parkway Holdings Ltd 685.30
2010 Fortis Healthcare Ltd OP Jindal Hospital -
2010 Fortis Healthcare Ltd Vivekanand Hospital and Research Centre -
2010 Fortis Global Healthcare Holdings Pte Ltd Dental Corporation Holdings Limited 95.74
2010 Fortis Global Healthcare Holdings Pte Ltd Dental Corporation Holdings Limited 95.74
2011 Shalby Hospitals Vrundavan Hospital -
2011 Fortis Healthcare Ltd Super Religare Laboratories 174.57
2011 Fortis Healthcare Fortis Healthcare International 665.00
2011 Life Healthcare Group Holdings Max Healthcare Institute Ltd 112.28
2011 Fortis Global Healthcare Lanka Hospitals Corporation Plc 36.30
2011 Max India Ltd Max Healthcare Institute Ltd 30.43
2011 Surya Healthcare, majority owned by Surya
Pharmaceuticals Medimart Pharmacy 2.39
2011 Halcyon Finance and Capital Advisors Pvt. Ltd BLK Super Speciality Hospital 44.4
2012 BUPA Care Services Ltd Dental Corporation Holdings Ltd- Subsidary of Fortis Healthcare 286.00
2012 Radiant Life Care Pvt Ltd Guru Harkishan Hospital-management rights 77.00
2012 Fortis Healthcare RadLink-Asia Pte Ltd 50.00
2012 Radiant Life Care Pvt Ltd Guru Harkishan Hospital-management rights 77.00
2012 Fortis Healthcare RadLink-Asia Pte Ltd 50.00
2012 Centre for Sight New Vision Laser Centre 10.00
2012 Shalby Ltd Yogeshwar Healthcare Ltd -Krishna Heart Institute 13.64
2013 Moolchand Healthcare Pankaj Apollo Hospital -
M&A deals (2010-13)
Source: Grant Thornton Dealtracker -the data includes deals till March 2013
Year Investee Investor Value (US$
million)
2010 Asian Healthcare Fund Diwan Chand Medical Services Pvt Ltd 20.00
2010 SONG Investment Advisors Eye Q -
2010 Matrix Partners India Investment Holdings,LLC Centre for Sight 10.64
2010 Temasek Holdings Max India 25.53
2010 Aureos Capital India BSR Super Specialty Hospitals Ltd 10.00
2011 Intel Capital Sudhir Srivastava Advanced Robotic Surgery Centre -
2011 Helion Venture Partners, Nexus Venture Partners Eye-Q -
2011 Avigo Capital Partners Super Religare Laboratories Ltd 21.74
2011 Sabre Capital Super Religare Laboratories Ltd 10.87
2011 Franklin Templeton Symbiotec Pharmalab 9.78
2012 NYLIM Jacob Ballas Super Religare Laboratories 50.00
2012 International Finance Corporation Super Religare Laboratories 24.00
2012 Sequoia Capital Moolchand Healthcare 20.00
2012 India Equity Partners Axiss Dental -
2012 Matrix Partners India Mewar Orthopaedic Hospital 5.45
2012 Rajasthan Venture Capital International Oncology Services Pvt Ltd 4.00
2012 India Innovation Fund, Indian Angel Network Consure Medical -
2013 Sequoia Capital ASG Eye Hospitals 9.09
2013 WestBridge Capital Partners Dr Lal PathLabs 36.00
2013 TA Associates Dr Lal PathLabs 9.00
2013 Artiman Ventures Core Diagnostics 4.91
PE deals (2010-13)
© Grant Thornton India LLP. All rights reserved. 42
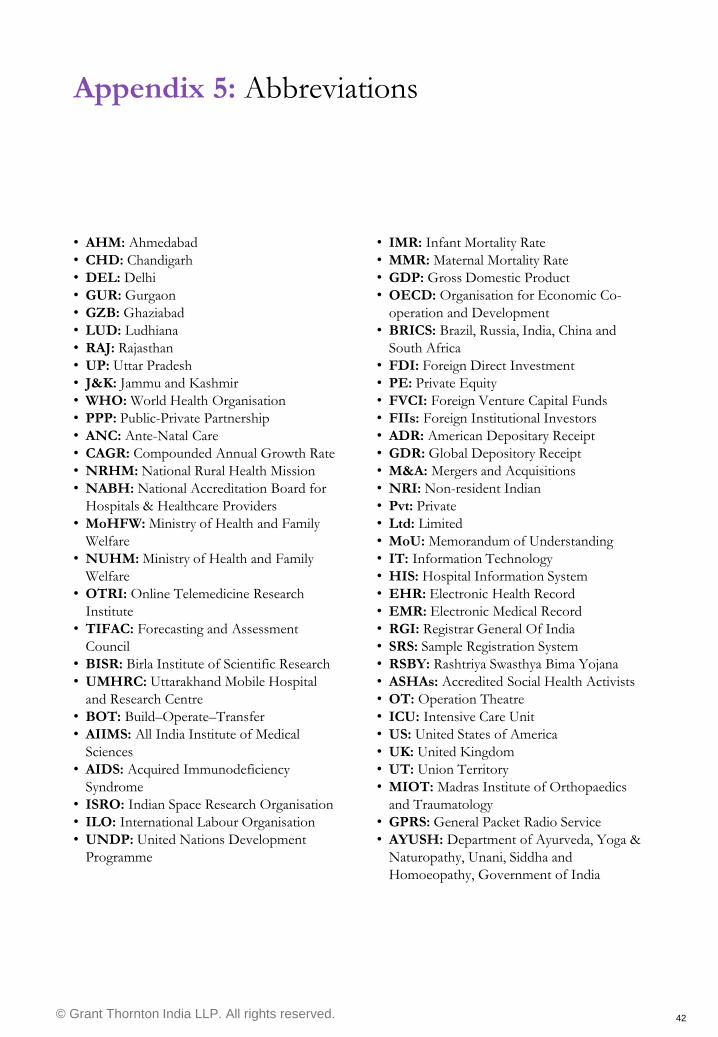
• IMR: Infant Mortality Rate
• MMR: Maternal Mortality Rate
• GDP: Gross Domestic Product
• OECD: Organisation for Economic Co-
operation and Development
• BRICS: Brazil, Russia, India, China and
South Africa
• FDI: Foreign Direct Investment
• PE: Private Equity
• FVCI: Foreign Venture Capital Funds
• FIIs: Foreign Institutional Investors
• ADR: American Depositary Receipt
• GDR: Global Depository Receipt
• M&A: Mergers and Acquisitions
• NRI: Non-resident Indian
• Pvt: Private
• Ltd: Limited
• MoU: Memorandum of Understanding
• IT: Information Technology
• HIS: Hospital Information System
• EHR: Electronic Health Record
• EMR: Electronic Medical Record
• RGI: Registrar General Of India
• SRS: Sample Registration System
• RSBY: Rashtriya Swasthya Bima Yojana
• ASHAs: Accredited Social Health Activists
• OT: Operation Theatre
• ICU: Intensive Care Unit
• US: United States of America
• UK: United Kingdom
• UT: Union Territory
• MIOT: Madras Institute of Orthopaedics
and Traumatology
• GPRS: General Packet Radio Service
• AYUSH: Department of Ayurveda, Yoga &
Naturopathy, Unani, Siddha and
Homoeopathy, Government of India
• AHM: Ahmedabad
• CHD: Chandigarh
• DEL: Delhi
• GUR: Gurgaon
• GZB: Ghaziabad
• LUD: Ludhiana
• RAJ: Rajasthan
• UP: Uttar Pradesh
• J&K: Jammu and Kashmir
• WHO: World Health Organisation
• PPP: Public-Private Partnership
• ANC: Ante-Natal Care
• CAGR: Compounded Annual Growth Rate
• NRHM: National Rural Health Mission
• NABH: National Accreditation Board for
Hospitals & Healthcare Providers
• MoHFW: Ministry of Health and Family
Welfare
• NUHM: Ministry of Health and Family
Welfare
• OTRI: Online Telemedicine Research
Institute
• TIFAC: Forecasting and Assessment
Council
• BISR: Birla Institute of Scientific Research
• UMHRC: Uttarakhand Mobile Hospital
and Research Centre
• BOT: Build–Operate–Transfer
• AIIMS: All India Institute of Medical
Sciences
• AIDS: Acquired Immunodeficiency
Syndrome
• ISRO: Indian Space Research Organisation
• ILO: International Labour Organisation
• UNDP: United Nations Development
Programme
Appendix 5: Abbreviations
© Grant Thornton India LLP. All rights reserved. 43
References
• http://www.gartner.com/newsroom/id/234
4215
• http://data.worldbank.org/indicator/SH.XP
D.PCAP/countries
• Health at a Glance 2011: OECD indicators
• http://www.business-
standard.com/article/economy-
policy/doing-less-with-more-india-s-health-
care-system-113033000209_1.html
• http://www.changemakers.com/changesho
p/primary-healthcare-rural-indian-
populations
• http://www.ncbi.nlm.nih.gov/pmc/articles/
PMC3283025/
• http://www.business-
standard.com/article/management/improvi
ng-the-picture-of-india-s-healthcare-
112061800066_1.html
• http://www.photius.com/rankings/healthra
nks.html
• http://www.ibef.org/download/Healthcare
50112.pdf
• http://ehealth.eletsonline.com/2013/02/he
alth-gets-over-28-hikes-in-budget/
• http://www.photius.com/rankings/world_h
ealth_systems.html
• Indian Healthcare sector report – MegStrat
Consulting
• http://www.indianmirror.com/indian-
industries/2012/health-2012.html
• http://www.business-
standard.com/article/companies/indian-
pharma-market-to-grow-at-15-cagr-by-fy14-
112060300047_1.html
• http://data.worldbank.org/indicator/NY.G
DP.PCAP.CD
• http://articles.timesofindia.indiatimes.com/
2012-11-01/jaipur/34856928_1_imr-infant-
mortality-rate-sample-registration-survey
• National Health Profile – 2011 and 2010
• http://www.businessinsider.com/inside-
indias-no-frills-hospitals-where-heart-
surgery-costs-just-800-2013-4
• http://www.livemint.com/Politics/D0gBg
wCn3huK72S06p8K5H/The-dark-
underbelly-of-Indias-clinical-trials-
business.html
• http://www.photius.com/rankings/world_
health_systems.html
• Grant Thornton Healthcare Sector Budget
report 2013-14
• Research on India – Hospital Market in
India (March 2012)
© Grant Thornton India LLP. All rights reserved. 44
About CII
The Confederation of Indian Industry (CII) works to create and sustain an environment conducive
to the development of India, partnering industry, Government, and civil society, through advisory
and consultative processes. CII is a non-government, not-for-profit, industry led and industry
managed organization, playing a proactive role in India's development process. Founded over 118
years ago, India's premier business association has over 7100 member organizations, from the private
as well as public sectors, including SMEs and MNCs, and an indirect membership of over 90,000
companies from around 257 national and regional sectoral associations.
CII charts change by working closely with Government on policy issues, interfacing with thought
leaders, and enhancing efficiency, competitiveness and business opportunities for industry through a
range of specialised services and global linkages. It also provides a platform for consensus-building
and networking on diverse issues. Extending its agenda beyond business, CII assists industry to
identify and execute corporate citizenship programmes. Partnerships with over 120 NGOs across the
country carry forward our initiatives for integrated and inclusive development, in affirmative action,
healthcare, education, livelihood, diversity management, skill development, empowerment of women,
and water, to name a few.
The CII Theme for 2013-14 is Accelerating Economic Growth through Innovation,
Transformation, Inclusion and Governance. Towards this, CII advocacy will accord top priority
to stepping up the growth trajectory of the nation, while retaining a strong focus on accountability,
transparency and measurement in both the corporate and social eco-system, building a knowledge
economy, and broad-basing development to help deliver the fruits of progress to many.
With 63 offices including 10 Centres of Excellence in India, and 7 overseas offices in Australia,
China, France, Singapore, South Africa, UK, and USA, as well as institutional partnerships with 224
counterpart organizations in 90 countries, CII serves as a reference point for Indian industry and the
international business community.
Confederation of Indian Industry
The Mantosh Sondhi Centre23, Institutional Area, Lodi Road, New Delhi – 110 003 (India)
T: 91 11 45771000 / 24629994-7 • F: 91 11 24626149
E: [email protected] • W: www.cii.in
Reach us via our Membership Helpline: 00-91-11-435 46244 / 00-91-99104 46244
CII Helpline Toll free No: 1800-103-1244
© Grant Thornton India LLP. All rights reserved. 45
Grant Thornton International
Grant Thornton International is one of the world‟s leading organisations of independently owned
and managed accounting and consulting firms. These firms provide assurance, tax and specialist
advisory services to privately held businesses and public interest entities.
Clients of member and correspondent firms can access the knowledge and experience of more
than 2500 partners in over 100 countries in order to consistently receive a distinctive, high quality
and personalised service wherever they choose to do business. Grant Thornton International
strives to speak out on issues that matter to business and which are in the wider public interest.
Its aim is to emerge as a bold and positive leader in its chosen markets and within the global
accounting profession.
About Grant Thornton India LLP
Grant Thornton in India is a member firm within Grant Thornton International Ltd. The firm
has today grown to be one of the largest accountancy and advisory firms in India with over 1,500
staff in New Delhi, Bangalore, Chandigarh, Chennai, Gurgaon, Hyderabad, Kolkata, Mumbai and
Pune, and affiliate arrangements in most of the major towns and cities across the country. The
firm specialises in providing assurance, tax and advisory services to growth-oriented,
entrepreneurial companies.
About Grant Thornton
© Grant Thornton India LLP. All rights reserved. 46
Our services: Unlocking the potential for growth in dynamic healthcare
organisations
Grant Thornton‟s assurance, tax and advisory professionals have extensive experience serving a
broad spectrum of growth-oriented organisations. The Firm seamlessly combines the
international reach, depth and expertise with personal attention and a relationship approach,
which has made us the leading firm in each of our chosen markets. With shorter decision making
chains, more senior personnel involvement and distinctive client services, we are able to take a
wider view and operate in a coordinated way that‟s as fast and agile as our clients.
We have a dedicated healthcare & lifesciences practice in India with extensive experience, having
worked across over 100 clients in the sector. Building successful organisations requires
management to work on many fronts simultaneously. Organic growth, capacity building, mergers
and acquisitions, joint ventures, managing business risk and putting in place the right capital
structure are all equally important in dynamic organisations looking to realise their full potential.
To help healthcare organisations unlock their potential for growth, we provide robust advice in
the areas below:
Healthcare &
Life sciences
Advisory
Tax and
Regulatory Business Risk &
Process
Improvement
Due Diligence
& Valuation
Strategic
Services
JV &
International
Expansion
Assurance
& Compliance
M&A and Capital
Raising
To know more about our solutions for healthcare businesses, please contact:
Mahadevan Narayanamoni
Partner
Healthcare and Life Sciences Advisory
+91 40 66308200
Vrinda Mathur
Associate Director
Healthcare and Life Sciences
+91 124 462 8000
About Grant Thornton
© Grant Thornton India LLP. All rights reserved. 47
Insights for healthcare in India
Grant Thornton India LLP strives to speak out on matters that relate to the success and
sustenance of your business. Through our publications, we seek to share our knowledge derived
from our expertise and experience. The firm publishes a variety of monthly and quarterly
publications designed to keep dynamic business leaders apprised of issues affecting their
companies.
Visit our Blog at www.grantthornton.in/insights to know more about our Thought Leadership
initiatives.
© Grant Thornton India LLP. All rights reserved. 48
Contact us
NEW DELHI National Office Outer Circle L 41 Connaught Circus New Delhi 110 001 T +91 11 4278 7070
CHENNAI Arihant Nitco Park, 6th floor No.90, Dr. Radhakrishnan Salai Mylapore Chennai 600 004 T +91 44 4294 0000
KOLKATA 10C Hungerford Street 5th floor Kolkata 700 017 T +91 33 4050 8000
CHANDIGARH SCO 17 2nd floor Sector 17 E Chandigarh 160 017 T +91 172 4338 000
GURGAON 21st floor, DLF Square Jacaranda Marg DLF Phase II Gurgaon 122 002 T +91 124 462 8000
HYDERABAD 7th floor, Block III White House Kundan Bagh, Begumpet Hyderabad 500 016 T +91 40 6630 8200
MUMBAI 16th floor, Tower II Indiabulls Finance Centre SB Marg, Elphinstone (W) Mumbai 400 013 T +91 22 6626 2600
PUNE 401 Century Arcade Narangi Baug Road Off Boat Club Road Pune 411 001 T +91 20 4105 7000
BENGALURU “Wings”, 1st floor 16/1 Cambridge Road Ulsoor Bengaluru 560 008 T +91 80 4243 0700
© Grant Thornton India LLP. All rights reserved.
Grant Thornton India LLP (formerly Grant Thornton India) is registered with limited liability with identity number AAA-
7677 and its registered office at L-41 Connaught Circus, New Delhi, 110001
Grant Thornton India LLP is a member firm within Grant Thornton International Ltd (Grant Thornton International).
Grant Thornton International and the member firms are not a worldwide partnership. Services are delivered by the
member firms independently.
For more information or for any queries, write to us at [email protected]
Disclaimer:
The information contained in this document has been compiled or arrived at from other sources believed to be reliable,
but no representation or warranty is made to its accuracy, completeness or correctness. The information contained in this
document is published for the knowledge of the recipient but is not to be relied upon as authoritative or taken in
substitution for the exercise of judgment by any recipient. This document is not intended to be a substitute for
professional, technical or legal advice or opinion and the contents in this document are subject to change without notice.
Whilst due care has been taken in the preparation of this report and information contained herein, Grant Thornton does
not take ownership of or endorse any findings or personal views expressed herein or accept any liability whatsoever, for
any direct or consequential loss howsoever arising from any use of this report or its contents or otherwise arising in
connection herewith.
www.grantthornton.in
Editorial team: Vrinda Mathur, Misbah Hussain, Sanjana Shankar
Design and production: Rakshit Dubey, Sushant Hivale
Abhishek Puri
Deputy Director
Confederation of Indian Industry
Northern Region Headquarters
Sector 31 – A
Chandigarh 160 030
T: +91 172 502 2522
F: +91 172 260 6259, 261 4974
Pankaj Jain
Executive
Confederation of Indian Industry
Northern Region Headquarters
Sector 31 – A
Chandigarh 160 030
T: +91 172 502 2522
F: +91 172 260 6259, 261 4974
Jasdeep Kaur
Executive
Confederation of Indian Industry I
Northern Region Headquarters
Sector 31 – A
Chandigarh 160 030
T: +91 172 502 2522
F: +91 172 260 6259, 261 4974