Embed Size (px)
DESCRIPTION
Prepared by Marta R. Gerasymchuk, M.D., Ph.D., Associate Professor of PATHOPHYSIOLOGY DEPARTMENT, IFNMU
Citation preview


Plan of the lecture1. Organization of the circulatory system.2. Cardiac cycle.3. Conductive system of the heart.4. Mechanisms of compensation5. Arhytmias of the heart. Deffinition.
Classification. Pathogenesis.6. Ischaemic heart disease.7. Heart failure.8. Arterial hypertension.

Actuality of the lectureActuality of the lectureThe disorders of cardiac rhythm concern to complex manifestations of
pathology of heart. Its can arise in rather small damage of the conducting system, and in some cases in structural changes. More often arrythmia arise with infectious illnesses and intoxications as consequence of miocarditis or dystrophy processes in cardiac muscle, and also in heart ishemic disease, cardiosclerosis.
Arrythmia can be result in development of cardiac insufficiency.Arterial hypertension is a very common condition. Cerebral, coronary
and renal vessels are mainly affected by the deleterious effect of this condition, and both acute and chronic organ failure may ensue.
Exacerbation of underlying pathophysiologic conditions or new precipitating factors can lead to hypertensive crisis, either urgencies or emergencies.

FUNCTIONAL ORGANIZATIONOF THE CIRCULATORY SYSTEM
■ The circulatory system consists of the heartheart, which pumps blood; the arterial systemarterial system, which distributes oxygenated blood to the tissues; the venous systemvenous system, which collects deoxygenated blood from the tissues and returns it to the heart; and the capillariescapillaries, where exchange of gases, nutrients, and wastes occurs.
■ The circulatory system is divided into two parts: the low-pressure pulmonary low-pressure pulmonary circulationcirculation, linking the transport function of the circulation with the gas exchange function of the lungs; and the high-pressure high-pressure systemic circulationsystemic circulation, providing oxygen and nutrients to the tissues.
■ The circulation is a closed system, so the output of the right and left heart must be equal over time for effective functioning of the circulation.

Electrocardiogram (ECG)Electrocardiogram (ECG)


(Frank-) Starling Law(Frank-) Starling Law• Within limits, the greater the stretching of the
muscle fibers (preload), the greater the force of contraction.
• The extra force of contraction is necessary to pump the increased volume of blood from the ventricle.
• Cardiac output increases Neural reflexesNeural reflexes• Bainbridge reflex – increased heart rate due to
increased right atrial pressure• Increased pressure in arteries stimulates a
baroreceptor reflex that decreases heart rate.

Cardiac Conduction Cardiac Conduction SystemSystem

ARRHYTHMIAS OF HEARTARRHYTHMIAS OF HEART Violation of rhythm of heart Violation of rhythm of heart accompanies a accompanies a
number of diseases of the cardio-vascular system. number of diseases of the cardio-vascular system. Most often they are observed at coronary Most often they are observed at coronary insufficiency. insufficiency. Arrhythmia registered Arrhythmia registered in in the acute the acute period of heart attack of myocardium in 95-100 % period of heart attack of myocardium in 95-100 % patientspatients..
In most world countries In most world countries sudden cardiac death is sudden cardiac death is about 15 %about 15 % from all cases of «natural» death. The from all cases of «natural» death. The main reason of sudden death at cardiac pathology main reason of sudden death at cardiac pathology in 93 % is arrhythmias. in 93 % is arrhythmias.
Arrhytmias are violation of frequency, rhythm, Arrhytmias are violation of frequency, rhythm, co-ordination and sequence of heartbeatco-ordination and sequence of heartbeat..

Etiology of heart rhythm disorderEtiology of heart rhythm disorderThe rhythm violations arise under the influence of different The rhythm violations arise under the influence of different
pathological agents, which can be divided on such groups:pathological agents, which can be divided on such groups: Functional violationsFunctional violations and and influencesinfluences, for example: , for example: violation violation
of vegetative nerves systemof vegetative nerves system condition (sympathetic or condition (sympathetic or parasympathetic link hyperactivity), parasympathetic link hyperactivity), physical workphysical work, , physical physical overloadoverload, , body temperature changesbody temperature changes, , the increase of the increase of intracranium pressureintracranium pressure, , respirationrespiration (especially in children); (especially in children);
Organic injury of myocardiumOrganic injury of myocardium, for example: , for example: inflammation inflammation of myocardiumof myocardium (as the result of infection), the (as the result of infection), the myocardium myocardium dystrophydystrophy (in the result of hypoxia, ischemia or amiloidosis), (in the result of hypoxia, ischemia or amiloidosis), necrosis of myocardiumnecrosis of myocardium;;
Influences of toxic substances on the myocardiumInfluences of toxic substances on the myocardium (alcohol, drugs, big dose adrenalin and noradrenalin, (alcohol, drugs, big dose adrenalin and noradrenalin, glucocorticoids, bacterial toxins, phosphororganic substances);glucocorticoids, bacterial toxins, phosphororganic substances);
Hormone balance disorderHormone balance disorder (hyperthyroidism, (hyperthyroidism, hypothyroidism, hyperfunction of supranephral glands);hypothyroidism, hyperfunction of supranephral glands);
Violation of intracellular or extracellular ions balanceViolation of intracellular or extracellular ions balance (changes of sodium, potassium, calcium, magnesium and (changes of sodium, potassium, calcium, magnesium and chlorine concentration);chlorine concentration);
Mechanical influences on the heartMechanical influences on the heart (catheter using for the (catheter using for the diagnosis and treatment heart diseases, operation on the diagnosis and treatment heart diseases, operation on the heart, chest trauma).heart, chest trauma).

• Development of arrhythmias Development of arrhythmias can be related to can be related to violations of basic functions of the conducting violations of basic functions of the conducting system of heart: system of heart:
1) automatism1) automatism, , 2) 2) excitability excitability and and 3) 3) conductivity. conductivity. • Classification of arrhythmias:Classification of arrhythmias:I. Arrhythmias, related with violations of automatism.I. Arrhythmias, related with violations of automatism.II. Arrhythmias, related with violations of excitability.II. Arrhythmias, related with violations of excitability.III. Arrhythmias, related with violations of III. Arrhythmias, related with violations of
conductivity.conductivity.IV. Arrhythmias, related with violations of excitability IV. Arrhythmias, related with violations of excitability
and conductivity.and conductivity.

Normal Rhythms

Arrhythmias, related with Arrhythmias, related with violation ofviolation of automatism automatism of of
heartheart Distinguish two groups of arrhythmiasDistinguish two groups of arrhythmias, related with , related with
violation violation of automatism of heart.of automatism of heart.1) 1) Nomotopic arrhythmiasNomotopic arrhythmias - - the generation of impulsesthe generation of impulses, as , as
well as in a norm, well as in a norm, takes place by takes place by pacemaker cells (P-cells) pacemaker cells (P-cells) in in sinoatrial [sinus] node, [nodus sinuatrialis]sinoatrial [sinus] node, [nodus sinuatrialis]. To them . To them belong:belong:
a) a) sinus tachycardiasinus tachycardia is multiplying frequency of cardiac is multiplying frequency of cardiac reductions;reductions;
b) b) sinus bradycardiasinus bradycardia is diminishing of frequency of cardiac is diminishing of frequency of cardiac reductions;reductions;
c) c) sinus (respiratory) arrhythmiasinus (respiratory) arrhythmia is a change of frequency is a change of frequency of heartbeat in the different phases of respiratory cycle of heartbeat in the different phases of respiratory cycle (become more frequent at inhalation [breath] and (become more frequent at inhalation [breath] and diminishing is at exhalation [outward breath]).diminishing is at exhalation [outward breath]).

Arrhythmias, related with Arrhythmias, related with violation of automatismviolation of automatism

Heterotopic ArrhythmiasHeterotopic Arrhythmias2) 2) heterotopic arrhythmiasheterotopic arrhythmias are are a syndrome of a syndrome of weakness of sinus weakness of sinus
nodenode.. The generation of impulses appears into other structures of The generation of impulses appears into other structures of the conducting system. A syndrome develops as a result of the conducting system. A syndrome develops as a result of diminishing of activity or stopping of activity of sinus node at the diminishing of activity or stopping of activity of sinus node at the damage of it cells or primary functional violations. The followings damage of it cells or primary functional violations. The followings types of pathological rhythms of heart can develop:types of pathological rhythms of heart can develop:
a) a) atrium slow rhythmatrium slow rhythm - a driver of rhythm is in the structures of - a driver of rhythm is in the structures of left atrium, frequency of heartbeat lesser than 70 per 1 min;left atrium, frequency of heartbeat lesser than 70 per 1 min;
b) b) atrio-ventricular rhythmatrio-ventricular rhythm - the source of impulses are drivers of - the source of impulses are drivers of rhythm of the II order (overhead, middle or lower part of atrio-rhythm of the II order (overhead, middle or lower part of atrio-ventricular node), frequency of heartbeat in dependence on the ventricular node), frequency of heartbeat in dependence on the place of generation of impulses diminishes from 70 to 40 per place of generation of impulses diminishes from 70 to 40 per minute ;minute ;
c) c) idioventricular rhythmidioventricular rhythm - the generation of impulses appears in - the generation of impulses appears in the drivers of rhythm of the III order (His' bundle, atrioventricular the drivers of rhythm of the III order (His' bundle, atrioventricular fascicle, fasciculus atrioventricularis and pedunculi of it), fascicle, fasciculus atrioventricularis and pedunculi of it), frequency of heartbeat lesser than 40 per minute.frequency of heartbeat lesser than 40 per minute.

Reason and mechanisms of development of Reason and mechanisms of development of sinus tachy- and bradycardiasinus tachy- and bradycardia
Increase generating of impulsesIncrease generating of impulses.. Reasons: Reasons: a) at diminishing of level of maximal diastolic potential of cells of sinus a) at diminishing of level of maximal diastolic potential of cells of sinus
node node b) at approaching to it of maximum critical potential, b) at approaching to it of maximum critical potential, c) at multiplying speed of slow diastolic depolarization. c) at multiplying speed of slow diastolic depolarization.
Such phenomenon is observed: Such phenomenon is observed: a) under act of the promoted temperature of body a) under act of the promoted temperature of body b) stretching areas of sinus node, b) stretching areas of sinus node, c) under act of mediators of sympathetic system.c) under act of mediators of sympathetic system. Opposite, Opposite, a) diminishing of speed of slow diastolic depolarization, a) diminishing of speed of slow diastolic depolarization, b) hyperpolarization in a diastole and b) hyperpolarization in a diastole and c) the decreasing of critical maximum potential, as it is observed at c) the decreasing of critical maximum potential, as it is observed at
annoying a vagus nerve, are accompanied deceleration of generation annoying a vagus nerve, are accompanied deceleration of generation of impulses, and consequently - of impulses, and consequently -
The instability [fluctuation, variation] of tone of vagus nerve during The instability [fluctuation, variation] of tone of vagus nerve during the act of breathing predetermine respiratory arrhythmia (become the act of breathing predetermine respiratory arrhythmia (become more frequent palpitation at inhalation, deceleration - at exhalation). more frequent palpitation at inhalation, deceleration - at exhalation).
Children have respiratory arrhythmia in a normChildren have respiratory arrhythmia in a norm, sometimes it , sometimes it also observed for adults.also observed for adults.
Tachycardia developsTachycardia develops
Bradycardia developsBradycardia develops

Arrhythmias, related to violations of excitabilityArrhythmias, related to violations of excitability The main reason is appearance so-called ectopic hotbed of excitations which generate premature impulsespremature impulses.The most widespread arrhythmias of this group are:
a) extrasystole [beat] a) extrasystole [beat] and and b) paroxysmal [recurrent, reentrant] tachycardia.b) paroxysmal [recurrent, reentrant] tachycardia.
Extrasystole is a type of arrhythmias, which are stipulated violations of function of excitability which shows up the origin of premature contraction of heart or only ventricles. In dependence on localization of hotbed which an premature impulse goes out from, distinguish the followings types of extrasystole:
a) a) sinussinus (or nomotopic), (or nomotopic), b)b) atrial atrial, , c)c) atrio-ventricular atrio-ventricular and and d)d) ventricular [ventricular premature beats]. ventricular [ventricular premature beats].
As a wave of excitation, which arose up in an unusual place, spreads in the changed direction, it is reflected on the structure of the electric field of heart and finds a reflection on an electrocardiogram.

Sinus extrasystoleSinus extrasystole• Sinus extrasystole arises up
as a result of premature excitation part of cells of sinus node. On ECG: shortening interval TP. As a result shortening of diastole and diminishing of filling of ventricles a pulse wave is diminished too.

Atrial Atrial extrasystolesextrasystoles
• Atrial extrasystolesAtrial extrasystoles are observed at presence of hotbed of ectopic excitation in the different areas of atrium and are characterized: a) change the form P-waveform P-wave (reduced, two-phase, reduced, two-phase,
negativenegative); b) at the stored complex QRS and c) some lengthening of diastolic interval after extrasystole (an incomplete compensate pauseincomplete compensate pause).

Atrio-Atrio-ventricular ventricular extrasystolextrasystol
ee
• Atrio-ventricular extrasystole is observed in case of occurring of additional impulse in atrio-ventricular node.
• The wave of excitation, which goes out from overhead and middle parts of node, spreads in two directions:
a) into ventricles - as normal b) into atrium - retrograde direct. Thus: a) the negative negative P-waveP-wave can be present before or lay before or lay on complex QRSon complex QRS; b) diastole interval after a extrasystole is a little prolonged. A extrasystole can be accompanied simultaneous beat of atrium and
ventricles. • At a atrio-ventricular extrasystole which goes out from lower part of
node, there is a compensate pause, the same, as well as at a ventricular extrasystole and P-wave is negative and situated after complex QRS.

Ventricular extrasystoleVentricular extrasystole
• Ventricular extrasystoleVentricular extrasystole are characterized presence of a complete complete compensate pausecompensate pause after premature heartbeat and deformation complex QRS.
• Next beat of ventricles arises up only Next beat of ventricles arises up only after arrival to them of duty normal after arrival to them of duty normal impulseimpulse.. That is why duration of a compensate pause equals duration of two normal diastolic pauses. However if reductions of heart are so rare that to the moment of arrival of duty normal impulse ventricles have time to go out from the state of adiphoria, a compensate pause is absent. Premature heartbeat gets in an interval between two normal and in this case called the inserted extrasystole.

• 1) Atrial ectopic beatsAtrial ectopic beats appear as early (premature extrasystoles) and abnormal P-waves in the ECG; they are usually followed by normal QRS-complexes. Following the premature beat there is often a compensatory interval. A premature beat in the left ventricle is weak because of inadequate venous return, but after the long compensatory interval, the post-extrasystolic contraction (following a long venous return period) is strong due the Starling´s law of the heart. - Adrenergic b-blockers are sometimes necessary.
• 2) Ventricular ectopic beatsVentricular ectopic beats (extrasystoles) are recognized in the ECG by their wide QRS-complex (above 0.12 s), since they originate in the ventricular tissue and slowly spread throughout the two ventricles without passing the Purkinje system. The ventricular ectopic beat is recognized by a double R-wave. The classical tradition of simultaneous cardiac auscultation and radial artery pulse palpation eases the diagnosis. Now and then a pulsation is not felt, and an early frustraneous beat is heard together with a prolonged interval. A beat initiated in the vulnerable period may release lethal ventricular tachycardia, since the tissue is no longer refractory.

Paroxysmal tachycardiaParoxysmal tachycardia• Paroxysmal tachycardiaParoxysmal tachycardia is arrhythmia, which is stipulated
violations of function of excitability, which shows up the origin of group of extrasystoles which fully repress a physiology rhythm.
• At paroxysmal tachycardia the normal rhythm of heart is normal rhythm of heart is suddenly brokensuddenly broken by attack of beats with frequency from 140 to 250 shots per minute.
• Duration of attack can be different - from a few secondsfew seconds to a few minutesfew minutes. It is suddenly stopped and recommences normal rhythm.
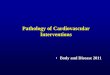
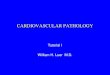
Paroxysmal supraventrical tachycardia
Paroxysmal supraventricular tachycardia: note accelerated rate and narrow QRS complexes.

Arrhythmias, related to violation of Arrhythmias, related to violation of conductivity of impulses conductivity of impulses
Select two groups of such arrhythmias: Select two groups of such arrhythmias: 1) Heart block. 1) Heart block. 2) Increased conducting of impulses – 2) Increased conducting of impulses – WPW-syndromeWPW-syndrome (Wolf-Parkinson- (Wolf-Parkinson-
White block) White block) Heart blocksHeart blocks are arrhythmias, conditioned are arrhythmias, conditioned deceleration or complete deceleration or complete
stopped conducting of impulsesstopped conducting of impulses on the conducting system. on the conducting system. ReasonsReasons: : a)a) the damage of conductive ways, the damage of conductive ways, b)b) worsening of other functional descriptions worsening of other functional descriptions, which is accompanied , which is accompanied
deceleration or complete stopped conducting of impulse.deceleration or complete stopped conducting of impulse. Violations of conductivity can Violations of conductivity can arise up: arise up: a)a) between a sinus node and atriums between a sinus node and atriums b)b) inwardly atriums, inwardly atriums, c)c) between atriums and ventricles and between atriums and ventricles and d)d) in one of legs of His' bundle. in one of legs of His' bundle. Followings types of blockades select: Followings types of blockades select: 1)1) intraatrial intraatrial; ; 2)2) atrio-ventricular; atrio-ventricular; 3)3) intraventricular intraventricular..

SA BLOCKSA BLOCK
Rate normal or bradycardia P wave those present are normal QRS normal Conduction normalRhythm basic rhythm is regular*

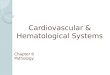
Atrio-Atrio-ventricular ventricular
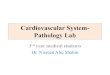
blockblock Four typesFour types of of
atrio-ventricular atrio-ventricular (AV)-block. From (AV)-block. From above above downwards: downwards:
First-degree AV-First-degree AV-block, block,
Second-degree Second-degree Mobitz I block Mobitz I block (Wenchebach), (Wenchebach),
Second-degree Second-degree Mobitz II block, Mobitz II block, andand
Complete AV-Complete AV-block.block.

Increase conducting Increase conducting of impulsesof impulses
• WPW-syndrome – characterized the speed-up conducting of impulses from atriums to the ventricles, as a result there is premature excitation of the last, tachycardia develops, the interval of PQ diminishes on an electrocardiogram.

Re-entry mechanismRe-entry mechanism Under normal conditions, an Under normal conditions, an
electrical impulse is conducted electrical impulse is conducted through the heart in an orderly, through the heart in an orderly, sequential manner. The sequential manner. The electrical electrical impulse then dies out and does not impulse then dies out and does not reenter adjacent tissuereenter adjacent tissue because because that that tissue has already been depolarized tissue has already been depolarized and is refractory to immediate and is refractory to immediate stimulationstimulation. However, under certain . However, under certain abnormal conditions, an impulse can abnormal conditions, an impulse can reenter an area of myocardium that reenter an area of myocardium that was previously depolarized and was previously depolarized and depolarize it again. There three depolarize it again. There three conditions are the necessary for this conditions are the necessary for this mechanism beginning: mechanism beginning:
1 – two conductive ways are the 1 – two conductive ways are the functionally or anatomically functionally or anatomically disconnected; disconnected;
2 – some conductive way is 2 – some conductive way is blocked;blocked;
3 – the antegrade conductive way 3 – the antegrade conductive way is blocked, but the retrograde one is blocked, but the retrograde one is preserved.is preserved.
So, in that condition impulse (or So, in that condition impulse (or impulses) travels numerous through impulses) travels numerous through some area of conductive system and some area of conductive system and returns through another pathway to returns through another pathway to the reactivated myocardiocytes.the reactivated myocardiocytes.

Arrhythmias with violation of functions Arrhythmias with violation of functions of excitability and conductivityof excitability and conductivity
1) 1) atrial flutteratrial flutter (frequency of (frequency of atrium beats - atrium beats - 250-400250-400 / / min).min).
2) 2) Atrial fibrillationAtrial fibrillation (frequency (frequency of impulses which arise up of impulses which arise up in atrium is in atrium is 400-600400-600 / min). / min).
► Atrial flutterAtrial flutter and and fibrillation have identical fibrillation have identical reasons of development reasons of development and can pass one to and can pass one to another. So, these two another. So, these two types of violation of types of violation of rhythm of heart combine rhythm of heart combine into one and called is into one and called is fibrillationfibrillation..
3) 3) ventricle flutterventricle flutter (frequency (frequency of ventricle beat is of ventricle beat is 150-150-300300/m)./m).
4) 4) FibrillationFibrillation of ventriclesof ventricles (frequency of impulses in (frequency of impulses in ventricles is ventricles is 300-500 300-500 / / min).min).
► Arrhythmias Arrhythmias which arise up as a result of simultaneous violation of functions which arise up as a result of simultaneous violation of functions of of excitability excitability and and conductivityconductivity. . To them belong:To them belong:

Even when the stimulus formation in the sinus
node is normal, abnormal ectopic
excitations can start from a focus in an
atrium (atrial), the AV node (nodal), or a
ventricle (ventricular).


Coronary Heart Disease The term coronary heart disease
(CHD) describes heart disease caused by impaired coronary blood flow.
In most cases, CHD is caused by atherosclerosis.
Diseases of the coronary arteries can cause angina, myocardial infarction or heart attack, cardiac dysrhythmias, conduction defects, heart failure, and sudden death.
Heart attack is the largest killer of American men and women, claiming more than 218,000 lives annually. Each year, 1.5 million Americans have new or recurrent heart attacks, and one third of those die within the first hour, usually as the result of cardiac arrest resulting from ventricular fibrillation.

Pathogenesis of Coronary Pathogenesis of Coronary Heart DiseaseHeart Disease
• HDL (good)HDL (good) cholesterol removes cholesterol removes excess cholesterol in excess cholesterol in the blood stream.the blood stream.
• LDL (bad)LDL (bad) cholesterol cholesterol enters the arterial enters the arterial wall andwall and is taken up is taken up by our body’s by our body’s scavenger cells.scavenger cells.
• Subsequently, they Subsequently, they will turn into fatty will turn into fatty streaks which streaks which progress into progress into atheromatous atheromatous plaques.plaques.
• Hence, LDL Hence, LDL cholesterol is said to cholesterol is said to promote promote atherosclerosis.atherosclerosis.

Cholesterol readings includes:Cholesterol readings includes:Total cholesterol Total cholesterol
DesirableDesirable : < 5.2 mmol/L: < 5.2 mmol/LBorderline HighBorderline High : 5.2 : 5.2 –– 6.2 6.2 mmol/Lmmol/LHighHigh : ≥ 6.2 mmol/L: ≥ 6.2 mmol/L
LDL cholesterolLDL cholesterolDesirableDesirable : < 3.3 mmol/L: < 3.3 mmol/LBorderline HighBorderline High : 3.3 : 3.3 –– 4.1 4.1 mmol/Lmmol/LHighHigh : ≥ 4.1 mmol/L: ≥ 4.1 mmol/L
Well-Balanced Cholesterol Levels :Well-Balanced Cholesterol Levels :
Healthy LifestyleHealthy Lifestyle


Types of chronic ischemic heart disease Types of chronic ischemic heart disease and acute coronary syndromesand acute coronary syndromes
Coronary heart diseaseCoronary heart disease
Chronic ischemic heart disease Acute coronary syndrome
StableStableanginaangina
Silent myocardialischemia
Variantangina
No ST-segmentelevation
Q-waveAMI
Unstableangina
Non-ST-segmentelevation AMI
ST-segmentelevation

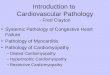
Atherosclerosis: A Progressive Process
Disease progression
PHASE I: Initiation PHASE II: Progression PHASE III: Complication
NormalFatty
StreakFibrousPlaque
Occlusive Atherosclerotic
Plaque
PlaqueRupture/Fissure &
Thrombosis
MI
Stroke
Critical Leg Ischemia
Coronary Death
UnstableAngina
Libby P. Circulation. 2001;104:365-372.
Ischemia
Thrombus formation
Coronary vasospasm

1) FATTY STREAK (non-palpable, but a visible YELLOW streak)
2) ATHEROMA (plaque) (palpable)
3) THROMBUS (non-functional, symptomatic)

ANGINA PECTORIS• Paroxysmal (sudden)• Recurrent• 15 sec.15 min.• Reduced perfusion, but NO infarction• THREE TYPES
• STABLE:STABLE: relieved by rest or nitroglycerin• PRINZMETAL:PRINZMETAL: SPASM is main feature, responds to
nitro, S-T elevation• UNSTABLEUNSTABLE (crescendo, PRE-infarction, Q-wave
angina): perhaps some thrombosis, perhaps some non transmural necrosis, perhaps some embolization, but DISRUPTION of PLAQUE is universally agreed upon

Chest PainChest Pain First symptom of those suffering myocardial First symptom of those suffering myocardial
ischemia.ischemia. Called angina pectoris (angina – “pain”)Called angina pectoris (angina – “pain”) Feeling of heaviness, pressureFeeling of heaviness, pressure Moderate to severeModerate to severe In substernal areaIn substernal area Often mistaken for indigestionOften mistaken for indigestion May radiate to neck, jaw, left arm/ shoulderMay radiate to neck, jaw, left arm/ shoulderDue to :Due to :
Accumulation of lactic acid in Accumulation of lactic acid in myocytes or stretching of myocytesmyocytes or stretching of myocytes

Stable angina pectoris Caused by chronic coronary obstruction Recurrent predictable chest pain Gradual narrowing and hardening of
vessels so that they cannot dilate in response to increased demand of physical exertion or emotional stress
Lasts approx. 3-5 minutes Relieved by rest and nitrates
Stress testStress testshowsshows
ST segment ST segment depression depression
> 1mm> 1mm

Prinzmetal angina pectorisPrinzmetal angina pectoris(Variant angina)(Variant angina)
Caused by abnormal vasospasm of normal vessels (15%) or Caused by abnormal vasospasm of normal vessels (15%) or near atherosclerotic narrowing (85%)near atherosclerotic narrowing (85%)
Occurs unpredictably and almost exclusively at rest.Occurs unpredictably and almost exclusively at rest. Often occurs at night during REM sleepOften occurs at night during REM sleep (rapid eye movement) (rapid eye movement) May result from hyperactivity of sympathetic nervous system, May result from hyperactivity of sympathetic nervous system,
increased calcium flux in muscle or impaired production of increased calcium flux in muscle or impaired production of prostaglandinprostaglandin
Vasoconstriction is due to platelet thromboxane AVasoconstriction is due to platelet thromboxane A22 or an or an increase in endothelin increase in endothelin
This causes a pattern of ST elevationST elevation that is very similar to acute STEMI — i.e. localised ST elevation with reciprocal ST depression occurring during episodes of chest pain. However, unlike acute STEMI the ECG changes are transient, reversible with vasodilators and not usually associated with myocardial necrosis. They may be impossible to differentiate on the ECG. ST elevation myocardial infarction (STEMI)

Silent IschemiaSilent Ischemia
•Totally asymptomaticTotally asymptomatic•May be due abnormality May be due abnormality in innervationin innervation
•Or due to lower level of Or due to lower level of inflammatory cytokinesinflammatory cytokines


Unstable Angina pectorisUnstable Angina pectoris
Lasts more than 20 minutes at rest, Lasts more than 20 minutes at rest, or rapid worsening of a pre-existing or rapid worsening of a pre-existing anginaanginaMay indicate a progression to M.I.May indicate a progression to M.I.
Pathogenesis:Pathogenesis:Severe, fixed, multivessel Severe, fixed, multivessel atherosclerotic diseaseatherosclerotic diseaseDisrupted plaques with or without Disrupted plaques with or without platelet nonocclusive thrombiplatelet nonocclusive thrombi

Sudden cardiac deatSudden cardiac death h (SC(SCDD)) 1. Inexpected death within 1 hour after the onset of 1. Inexpected death within 1 hour after the onset of
symptomssymptoms2. Risk factors2. Risk factors a. Obesitya. Obesity b. b. GGlucoslucosee intolerance intolerance c. Hypertensionc. Hypertension d. Recent non-Q wave myocardial infarctiod. Recent non-Q wave myocardial infarctionn e. Smokinge. Smoking3. Occurs more frequently in the morning hours when 3. Occurs more frequently in the morning hours when
hypercoagiilability is ahypercoagiilability is att its peaits peackck4. Pathogenesis4. Pathogenesis a. Severe aa. Severe attheroseleroheroselerottic coronary artery ic coronary artery didiseasesease b. Disrupted b. Disrupted filimnsfilimns plaques plaques c. Absence of occlusive vessel thrombus (>80%; of cases)c. Absence of occlusive vessel thrombus (>80%; of cases) d. Cause of death is ventricular fibrillation.d. Cause of death is ventricular fibrillation. 5. Diagnosis of exclusion after the following causes are 5. Diagnosis of exclusion after the following causes are
ruled outruled out a. Mitral valve prolapse (MVP)a. Mitral valve prolapse (MVP) b. Hypertrophic cardiomyopathyb. Hypertrophic cardiomyopathy c. Calcific aortic stenosisc. Calcific aortic stenosis d. Conduction system abnormalid. Conduction system abnormalitietiess e. Cocaine abusee. Cocaine abuse

Acute myocardial infarction (Acute myocardial infarction (AMIAMI))
1. 1. EEpidemiologypidemiology a. Most common cause of a. Most common cause of
deatdeath h in adults in the in adults in the United States.United States.
b. Prominent in males b. Prominent in males between 40 and 65 years between 40 and 65 years oldold
c. Nc. Noo predominant sex predominant sex predilection after 65 years predilection after 65 years oldold
d. At least 25% of AMIs are d. At least 25% of AMIs are clinically unrecognized.clinically unrecognized.

Myocardial IschemiaMyocardial Ischemia Myocardial cell metabolic demands not metMyocardial cell metabolic demands not met Time frame of coronary blockage:Time frame of coronary blockage:
10 seconds following coronary block10 seconds following coronary block Decreased strength of contractionsDecreased strength of contractions Abnormal hemodynamics Abnormal hemodynamics
See a shift in metabolism, so within minutes: See a shift in metabolism, so within minutes: Anaerobic metabolism takes overAnaerobic metabolism takes over Get build-up of lactic acid, which is toxic within Get build-up of lactic acid, which is toxic within
the cellthe cell Electrolyte imbalancesElectrolyte imbalances Loss of contractibilityLoss of contractibility

20 minutes after blockage20 minutes after blockageMyocytes are still viable, soMyocytes are still viable, soIf blood flow is restored, and If blood flow is restored, and
increased aerobic metabolism, and increased aerobic metabolism, and cell repair,cell repair,
→→Increased contractilityIncreased contractilityAbout 30-45 minutes after blockage, if About 30-45 minutes after blockage, if
no reliefno reliefCardiac infarct & cell death Cardiac infarct & cell death

Myocardial infarctionMyocardial infarction Necrosis of cardiac myocytesNecrosis of cardiac myocytes
• IrreversibleIrreversible• Commonly affects left ventricleCommonly affects left ventricle• Follows after more than 20 minutes of Follows after more than 20 minutes of
ischemiaischemia

PathogenesisPathogenesisa. Sequencea. Sequence 1) Sudden1) Sudden disnipti disniptioonn of an atheromatous of an atheromatous
plaque plaque 2) Su2) Subbendothelial endothelial colcoliaiagengen andand thrombogenic thrombogenic
necrotic material are exposed.necrotic material are exposed. 3) Platelets adhere to the exposed material 3) Platelets adhere to the exposed material
and eventually form an occlusiveand eventually form an occlusive platelet platelet tthhrombus.rombus.
b. Role of thromboxane Ab. Role of thromboxane A22 1) Contributes to 1) Contributes to fformation oformation of the platelet the platelet
thrombusthrombus 2) Causes vasospasm of2) Causes vasospasm of the artery to reduce the artery to reduce
blood flowblood flow

PATHOPHYSIOLOGYPATHOPHYSIOLOGYCoronary artery cannot supply enough blood to the Coronary artery cannot supply enough blood to the
heart in response to the demand due to CADheart in response to the demand due to CAD
Within 10 seconds myocardial cells experience ischemia Within 10 seconds myocardial cells experience ischemia
Ischemic cells cannot get enough oxygen or glucoseIschemic cells cannot get enough oxygen or glucose
Ischemic myocardial cells may have decreased Ischemic myocardial cells may have decreased electrical & muscular functionelectrical & muscular function
Cells convert to anaerobic metabolism.Cells convert to anaerobic metabolism.
Cells produce lactic acid as wasteCells produce lactic acid as waste
Pain develops from lactic acid accumulationPain develops from lactic acid accumulation
Pt feels anginal symptoms until receiving demand Pt feels anginal symptoms until receiving demand increase Oincrease O22 requirements of myocardial cells requirements of myocardial cells
Myo
card
ium
Infa
rctio
n

PROGRESSION OF PROGRESSION OF NECROSISNECROSIS
0-1/2 hr reversible injury

Reperfusion injuryReperfusion injurya. Follows throma. Follows thrombbolytic (fibrinolytic) therapyolytic (fibrinolytic) therapyb. Early reperfusion salvages some injured but b. Early reperfusion salvages some injured but viable myocytes but destroys myocytesviable myocytes but destroys myocytes that are that are irreversibly damaged.irreversibly damaged.
1) Removal of irreversibly damaged myocytes 1) Removal of irreversibly damaged myocytes improves short- and long-termimproves short- and long-term function and function and survival.survival.
2) Prevents any further damage to myocardial cells2) Prevents any further damage to myocardial cells3) Limits the size of3) Limits the size of the infarctionthe infarction
c. Reperfusion histologically alters irreversibly c. Reperfusion histologically alters irreversibly damaged cells.damaged cells.
1) Produces contraction band necrosis1) Produces contraction band necrosis2) Caused by 2) Caused by hyphypoorcontractionrcontraction of myofibrils in dying of myofibrils in dying
cellscells• • Due to the influx of Ca-Due to the influx of Ca-++++ into the cytosol into the cytosol

Types of myocardial infarction
a. Transmural infarction (Qwave infarction)• 1) Involves the full thickness of the
myocardium• 2) New Q waves develop in an
electrocardiogram (ECG).b. Subendocardial infarction (non-Q wave
infarction)• 1) Involves the inner third of the myocardium• 2) Q waves are absent.

Clinical ManifestationsClinical Manifestations May hear May hear
extra, rapid extra, rapid heart soundsheart sounds
ECG ECG changes: changes: T wave T wave
inversioninversion ST ST
segment segment depressiondepression

Structural, functional changesStructural, functional changes Decreased contractilityDecreased contractility Decreased LV complianceDecreased LV compliance Decreased stroke volumeDecreased stroke volume DysrhythmiasDysrhythmias Inflammatory response is severeInflammatory response is severe Scarring results –Scarring results –
Strong, but stiff; can’t contract like Strong, but stiff; can’t contract like healthy cellshealthy cells

Sign and Symptom Classic symptom of heart attack
are chest pain radiating to neck, jaws, back of shoulder, or left arm
The pain can be felt like: Squeezing or heavy pressure A tight band on the chest An elephant sitting on the chest

Cont Other symptoms include:• Shortness of breath
(SOB)• Weakness and
tiredness• Anxiety• Lightheadedness• Dizziness• Nausea vomiting• Sweating, which may
be profuse

Determinants of Blood Pressure
• Components of B/P– Pressure of blood against the walls
of the arteries– The elasticity of the artery walls– The volume and thickness of the
blood

Regulative systemsRegulative systems Sympathetic Nervous Sympathetic Nervous SystemSystem BaroreceptorsBaroreceptors
– Nerve cells in carotid artery & aortic Nerve cells in carotid artery & aortic archarch
– Maintain BP during normal activitiesMaintain BP during normal activities– React to increases & decreases in BPReact to increases & decreases in BP
BP – impulse to brain to inhibit SNS; BP – impulse to brain to inhibit SNS; HR & force of contraction; vasodilation of HR & force of contraction; vasodilation of arteriolesarterioles
BP – activates SNS; vasoconstriction of BP – activates SNS; vasoconstriction of arterioles; HR & heart contractilityarterioles; HR & heart contractility
1. Barroreceptors of aorta arch and sinus caroticus

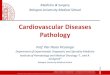
Increase BPIncrease BP
Renin
Angiotensin II
AldosteroneAldosteroneVasoconstrictionVasoconstrictionon systemic andon systemic and
renal vasselsrenal vassels
Left ventricularLeft ventricularhypertrophy hypertrophy
andandmyocardialmyocardialischemiaischemia
Increase leftIncrease leftventricular ventricular
wallwalltensiontension
Alteration of renalAlteration of renalarterial and arterial and
capillarycapillaryvessels’ wallvessels’ wall
Glomeruar ischemia,Glomeruar ischemia,parenchymal damage,parenchymal damage,proteinuria, end-stageproteinuria, end-stage
renal failurerenal failure
ADHADH
Sodium andSodium andwater renalwater renalretentionretention
HHypervolemiaypervolemia
Effect of renin-angiotensin system Effect of renin-angiotensin system on cardiovascular homeostasison cardiovascular homeostasis
2. 2. ReninRenin––angiotensinangiotensin systemsystem

Mechanism of Action of AldosteroneMechanism of Action of Aldosterone
Increases CO by increasing blood volume.

Healthy LifestyleHealthy LifestyleMaintain a Healthy Blood Pressure:
Blood Pressure Blood Pressure ClassificationClassification
Systolic BP Systolic BP (mm Hg)(mm Hg)
Diastolic BP Diastolic BP (mm Hg)(mm Hg)
NormalNormal < 120< 120 < 80< 80PrehypertensionPrehypertension 120 – 139120 – 139 80 – 8980 – 89Stage 1 HypertensionStage 1 Hypertension 140 – 159140 – 159 90 – 9990 – 99
Stage 2 HypertensionStage 2 Hypertension 160 – 179160 – 179 100 – 109100 – 109
Stage 3 HypertensionStage 3 Hypertension(Hypertensive crisis)(Hypertensive crisis)
≥ ≥ 180180 ≥ ≥ 110 110
Source: Clinical Practice Guidelines Management of Hypertension, 3rd Ed. 2008 February;MOH/P/PAK/156.08(GU)

Hypertension: Hypertension: DefinitionDefinition
Persistent elevation of Persistent elevation of Systolic bloodSystolic blood pressurepressure ≥140 mm Hg≥140 mm Hg
oror Diastolic blood pressureDiastolic blood pressure ≥90 mm Hg ≥90 mm Hg
Worldwide an estimated Worldwide an estimated 1 billion1 billion people people have hypertension; about 1 in 3 have hypertension; about 1 in 3 Americans affectedAmericans affected
Direct relationship between hypertension Direct relationship between hypertension and cardiovascular disease (CVD)and cardiovascular disease (CVD)


ClassificationClassification
Arterial hypotensionArterial hypotension
Arterial hypertensionArterial hypertension
AcuteAcuteChronicChronic
SecondarySecondary
AP above 139/89 mm HgAP above 139/89 mm Hg
PrimaryPrimary
AP less than 100/60 mm HgAP less than 100/60 mm Hg

Primary HypertensionPrimary Hypertension Etiological TheoriesEtiological Theories Inability of kidneys to excrete sodiumInability of kidneys to excrete sodium Overactive renin/angiotensin systemOveractive renin/angiotensin system Overactive sympathetic nervous Overactive sympathetic nervous
systemsystem Decreased vasodilatory reactionDecreased vasodilatory reaction Resistance to insulin actionResistance to insulin action Genetic Inheritance (polygenic)Genetic Inheritance (polygenic)

Risk Factors R/T Primary Risk Factors R/T Primary HypertensionHypertension
Age/HeredityAge/HereditySexSexRaceRaceObesityObesityStimulantsStimulantsSodiumSodiumAlcoholAlcoholStressStressHyperlipidemiaHyperlipidemiaDiabetesDiabetesSocioeconomic Socioeconomic StatusStatus

Primary HypertensionPrimary Hypertension
Water and sodium retentionWater and sodium retention• AA high sodium intake may result in high sodium intake may result in
water retentionwater retention• Some people are Na sensitive Some people are Na sensitive
(about 20%) ; not everyone with (about 20%) ; not everyone with high salt diet develops hypertensionhigh salt diet develops hypertension

Pathophysiology of Pathophysiology of Primary HypertensionPrimary Hypertension
• Stress and increased SNS activityStress and increased SNS activity– Produces increased Produces increased
vasoconstrictionvasoconstriction– ↑ ↑ HRHR– ↑ ↑ Renin releaseRenin release– Angiotensin II causes direct Angiotensin II causes direct
arteriolar constriction, promotes arteriolar constriction, promotes vascular hypertrophy and induces vascular hypertrophy and induces aldosterone secretionaldosterone secretion

HypertensionHypertensionClinical ManifestationsClinical Manifestations
often secondary to target organ disease Can include: – Fatigue, reduced
activity tolerance– Dizziness– Palpitations, angina– Dyspnea

Target Organ DamageTarget Organ Damage Caused by damage to the body’s blood Caused by damage to the body’s blood
vessels which particularly affect the vessels which particularly affect the following organs:following organs:
Blood Vessels Blood Vessels HeartHeart
KidneysKidneys BrainBrain EyesEyes

Accelerated-malignant Accelerated-malignant HTHT
Fundoscopic changesFundoscopic changes Retinal hemorrhagesRetinal hemorrhages Exudates Exudates PapilledemaPapilledema

Secondary HypertensionSecondary Hypertension ►It is caused by another disease It is caused by another disease
process such as:process such as:
►Renal FailureRenal Failure►Diabetes MellitusDiabetes Mellitus►Cushing’s SyndromeCushing’s Syndrome►Primary AldosteronismPrimary Aldosteronism►Coarctation of the AortaCoarctation of the Aorta►PheochromocytomaPheochromocytoma►Sleep ApneaSleep Apnea

Hypertensive crisisHypertensive crisis DefinitionDefinition
Severe elevation in BP ( >220/120 mmHg)Severe elevation in BP ( >220/120 mmHg) Sub classified into emergency and urgencySub classified into emergency and urgency
Hypertensive emergencyHypertensive emergency Require an immediate reduction in BP ( 1 hr ) Require an immediate reduction in BP ( 1 hr ) Rx IV therapy and in ICURx IV therapy and in ICU
Hypertensive urgencyHypertensive urgency No evidence of progressive end-organ injuryNo evidence of progressive end-organ injury Require only gradual reduction in BP in 24-48 hr Require only gradual reduction in BP in 24-48 hr

Collaborative CareCollaborative CareLifestyle ModificationsLifestyle Modifications
Physical activity: Physical activity: – Regular physical (aerobic) activity, Regular physical (aerobic) activity, – At least 30 min, most days of weekAt least 30 min, most days of week
Avoidance of tobacco productsAvoidance of tobacco products
Stress managementStress management


ExperimentalExperimental models of arterial models of arterial hypertensionhypertension..
Models confirming a role of the nervous factor in Models confirming a role of the nervous factor in increase of arterial pressure:increase of arterial pressure:
1. 1. Arterial hypertension owing to an irritation of Arterial hypertension owing to an irritation of hypothalamus nucleuseshypothalamus nucleuses. The irritation of a back . The irritation of a back nucleus frequently results nucleus frequently results toto hypertension, connected hypertension, connected with increase of cardiac output. The irritation of a with increase of cardiac output. The irritation of a central nucleus causes hyperension central nucleus causes hyperension due todue to of of peripheral resistance increase. Electricity stimulation peripheral resistance increase. Electricity stimulation ventro-medial nucleus gives hypertension, which ventro-medial nucleus gives hypertension, which depends from simultaneousdepends from simultaneouslyly increase of cardiac increase of cardiac output and peripheral resistance.output and peripheral resistance.
2. 2. Arterial hypertension from double-side damage Arterial hypertension from double-side damage nucleus tractus solitarii to nucleus tractus solitarii to medullamedulla oblong oblongataata of rats, of rats, where are located primary synapsis of sinuaorticus where are located primary synapsis of sinuaorticus baroreceptors. Arterial pressure is increased baroreceptors. Arterial pressure is increased immediately without change of frequency of cardiac immediately without change of frequency of cardiac rrateate. The reason of hypertension is the sharp increase . The reason of hypertension is the sharp increase of peripheral resistance of peripheral resistance
3. 3. Reflexogenic hypertensionReflexogenic hypertension, , inin dogs and rabbits dogs and rabbits aaffterffter section depressor nerve Ludvig-Cion or sinus section depressor nerve Ludvig-Cion or sinus nerves Hering nerves Hering ..

LiteratureLiterature Robbins and Cotran Pathologic Basis of Disease Robbins and Cotran Pathologic Basis of Disease 99thth edition./ Kumar, Abbas, edition./ Kumar, Abbas,
FautoFauto. –. – 20 201313.. Essentials of Pathophysiology: Concepts of Altered Health States (Lippincott Essentials of Pathophysiology: Concepts of Altered Health States (Lippincott
Williams & Wilkins), Trade paperback (2003) Williams & Wilkins), Trade paperback (2003) / / Carol Mattson Porth, Kathryn J. Carol Mattson Porth, Kathryn J. Gaspard Gaspard
J.B.Walter I.C.Talbot General pathology. Seventh edition. – 1996.J.B.Walter I.C.Talbot General pathology. Seventh edition. – 1996. Stephen J. McPhee, William F. Ganong. Pathophysiology of Disease, 5Stephen J. McPhee, William F. Ganong. Pathophysiology of Disease, 5thth
edition. – 2006.edition. – 2006. Pathophysiology, Concepts of Altered Health States, Carol Mattson Porth, Pathophysiology, Concepts of Altered Health States, Carol Mattson Porth,
Glenn Matfin. – New York, Milwaukee. – 2009. Glenn Matfin. – New York, Milwaukee. – 2009. General and clinical pathophysiology / Edited by Anatoliy V. Kubyshkin – General and clinical pathophysiology / Edited by Anatoliy V. Kubyshkin –
Vinnytsia: Nova Knuha Publishers – 2011. Vinnytsia: Nova Knuha Publishers – 2011. Symeonova N.K. Pathophysiology / N.K. Symeonova // Kyiv, AUS medicine Symeonova N.K. Pathophysiology / N.K. Symeonova // Kyiv, AUS medicine
Publishing. – 2010. Publishing. – 2010. Handbook of general and Clinical Pathophysiology / Edited by Handbook of general and Clinical Pathophysiology / Edited by
prof.A.V.Kubyshkin. – CSMU. – 2005. prof.A.V.Kubyshkin. – CSMU. – 2005. Pathophysiology / Edited by prof. Zaporozan. – OSMU. – 2005.Pathophysiology / Edited by prof. Zaporozan. – OSMU. – 2005.