Embed Size (px)
Citation preview
PATHOLOGY OF CARDIOVASCULAR
AND RESPIRATORY SYSTEM
Institute of Pathological anatomy
FM CU BA
Atherosclerosis, myocardial infarction, ischemic heart disease, brown lung
induration, lung edema, chronic liver venostasis, embolism, endocarditis,
bronchopneumonia, pneumonia, SCLC, NSCLC
Disclaimer
Please note, that the following information is intended just
for educational purposes of the medical students at Faculty of Medicine,
Comenius University.
All copyrights belong to their owners and
are used here for educational purposes only.
CARIDOVASCULAR SYSTEM
CASE NO. 1
• At a periodic checkup a 60-year-old male patient complains of occasional chest pain with radiation into the left arm. Recently he noticed swelling on his legs, mainly around ankles, he wakes up during nights coughing and prefers to sleep with two extra pillows.
• Physical examination shows hepatosplenomegaly, jugular vein distention, leg edema.
• Diagnosis?
• Complications?

Disseminated myocardial fibrosis
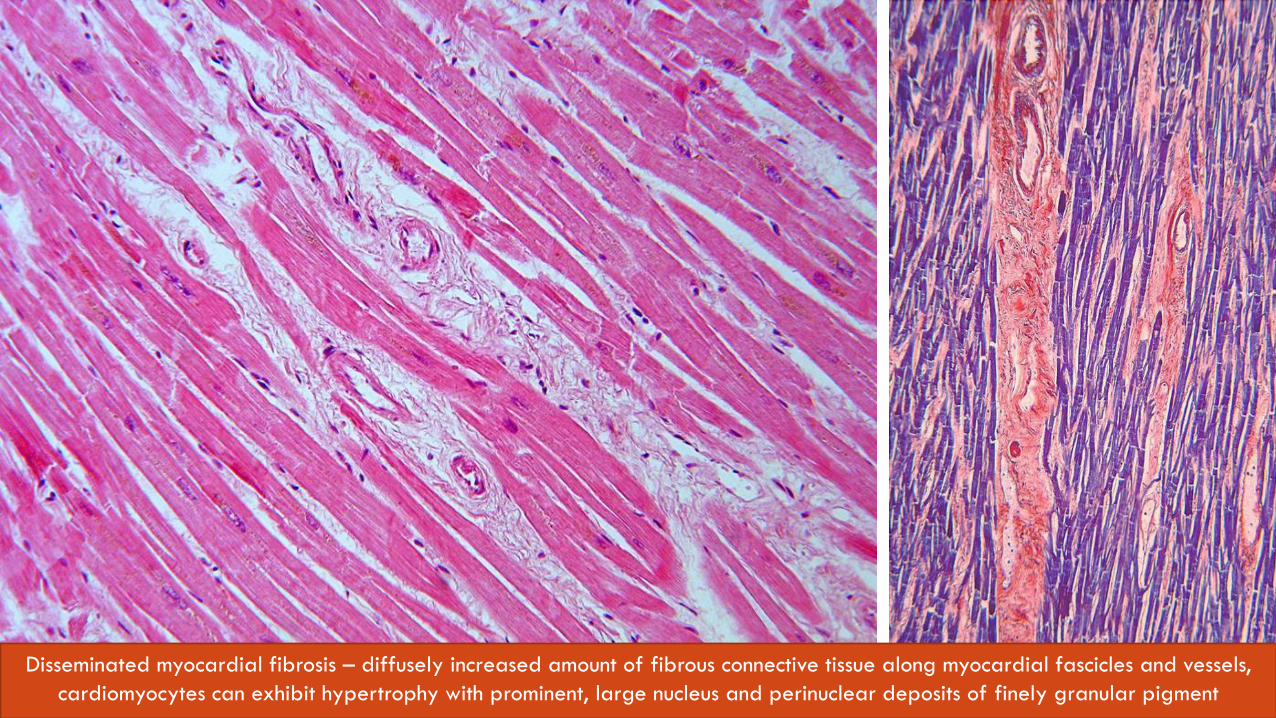
Disseminated myocardial fibrosis – diffusely increased amount of fibrous connective tissue along myocardial fascicles and vessels,
cardiomyocytes can exhibit hypertrophy with prominent, large nucleus and perinuclear deposits of finely granular pigment

Liver venostasis
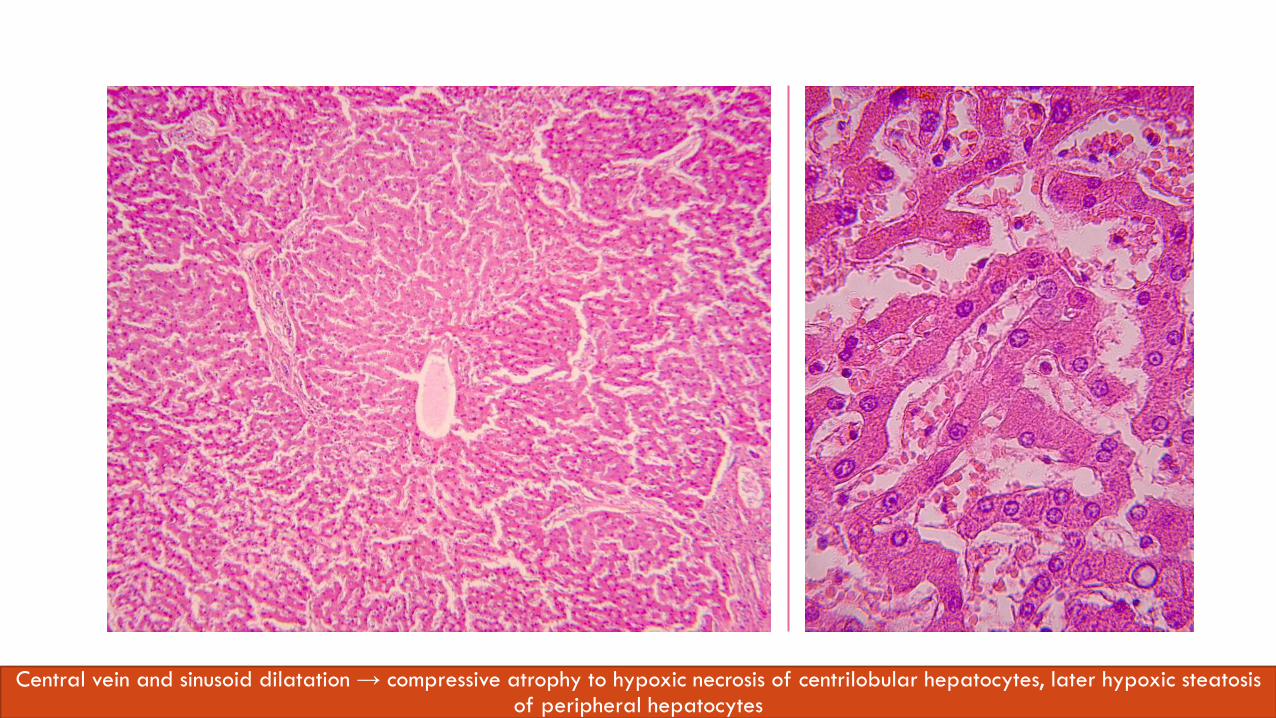
Central vein and sinusoid dilatation → compressive atrophy to hypoxic necrosis of centrilobular hepatocytes, later hypoxic steatosis of peripheral hepatocytes

Lung edema
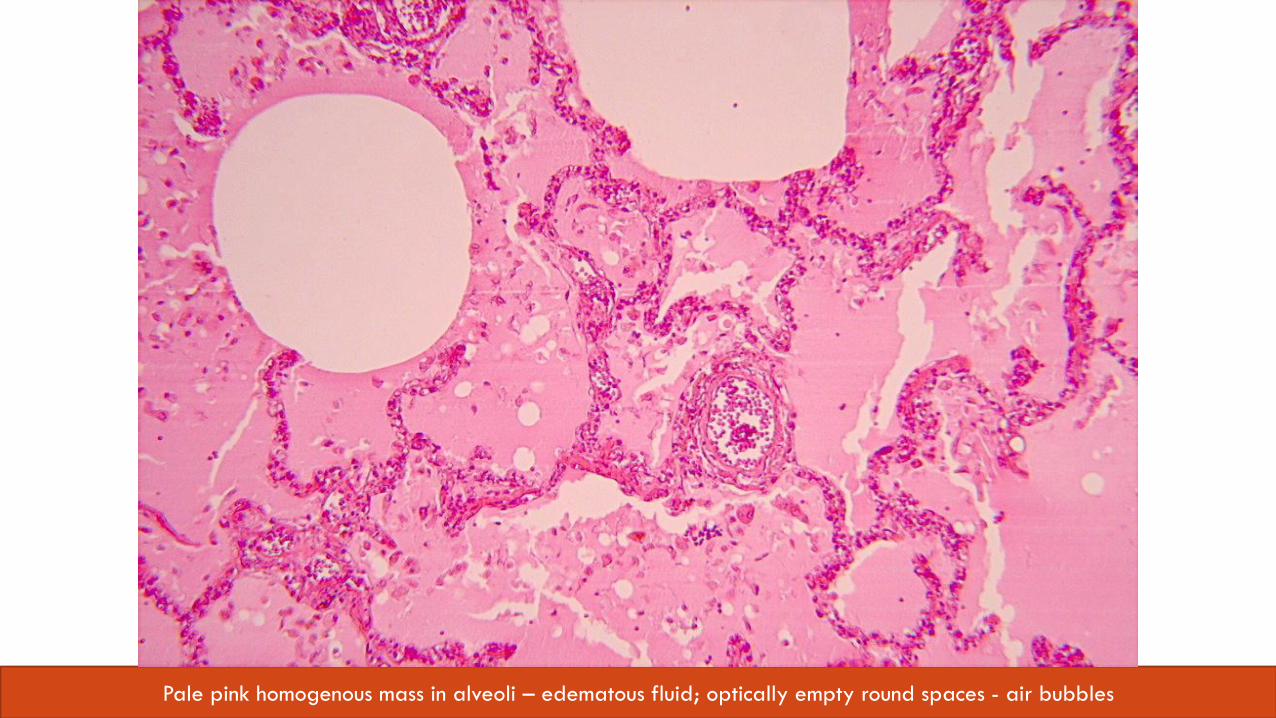
Pale pink homogenous mass in alveoli – edematous fluid; optically empty round spaces - air bubbles

Brown induration of lungs
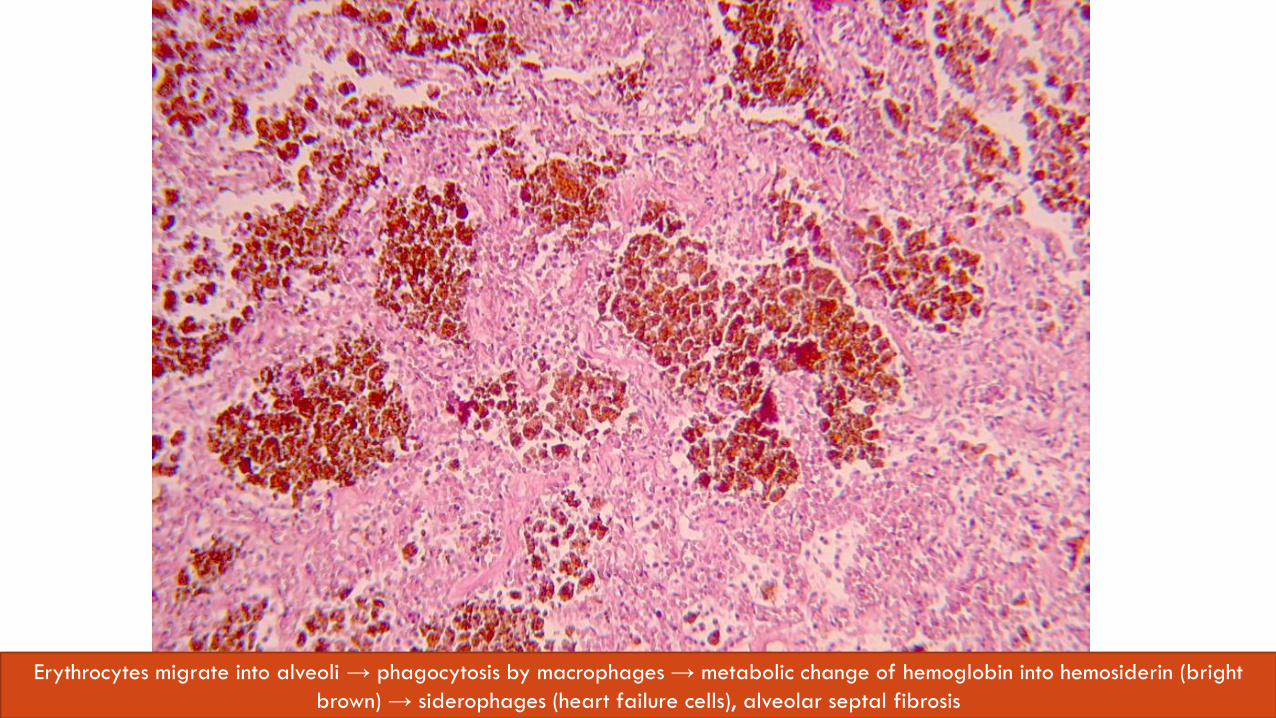
Erythrocytes migrate into alveoli → phagocytosis by macrophages → metabolic change of hemoglobin into hemosiderin (bright
brown) → siderophages (heart failure cells), alveolar septal fibrosis
CONGESTIVE HEART FAILURE
• right- and left-sided heart failure
• clinical diagnosis with symptoms and changes distinguishable on the level of pathological anatomy
• group of changes causing deterioration of cardiac output
• disseminated myocardial fibrosis – morphologic equivalent of chronic ischemic heart disease
• ischemic heart disease can be manifested as: angina pectoris, myocardial infarction, chronic ischemic heart disease, sudden cardiac death
Etiology:
Atherosclerosis, arterial hypertension, cardiac valve diseases, myocarditis, cardiomyopathy, lung hypertension (cor pulmonale)
CASE NO.2
• 82-year-old female was admitted to the emergency room with sudden severe dyspnea, she has had a tender right calf in the last few days
• she is bedridden due to stroke she surived 6 months ago
• laboratory results show severe hypoxia and increased value of D-dimer
• Diagnosis?
• Complications?

Pulmonary artery embolism Venous thrombosis of lower extremity
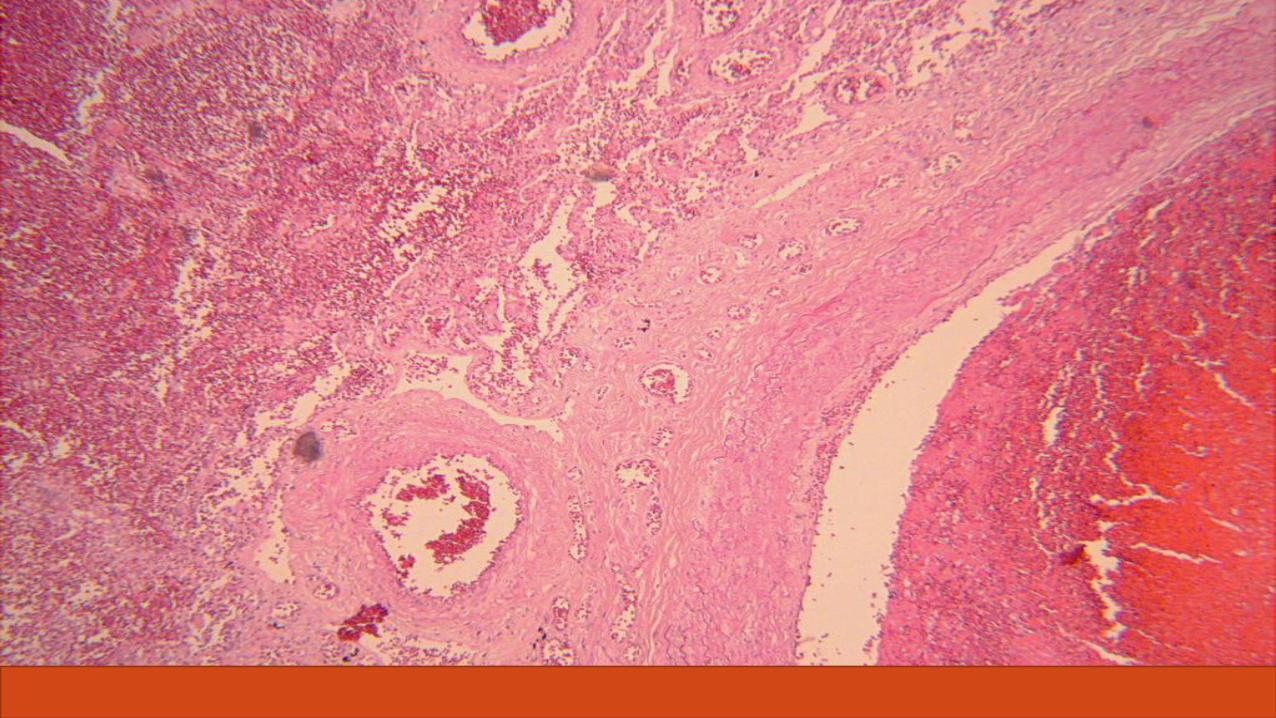
PULMONARY ARTERY EMBOLISM
• embolism – sudden blockage of bloodstream
• based on the type of embolism: solid, liquid, gas embolism
• pulmonary embolism is the third most common cause of death in hospitalised patients
• thromboembolus is the most common cause of embolism
• Virchow„s triad
• the result depends on the size of embolus
• Asymptomatic / mild dyspnea → lung hypertension with right sides heart failure
• Lung infarction
• Cardiovascular shock with sudden death
CASE NO. 3
• 60-year-old patient, long-term smoker, was admitted to the emergency department. He complains of chest pain with sudden onset after physical exercise, but persisting even when resting. During the examination he experiences sharp stabbing chest pain with radiation into the right hypochondrium, malaise, shortness of breath.
• Diagnosis?
• Complications?
• Which marker can be detected by laboratory examination?

Atherosclerosis
ATHEROSCLEROSIS • affects intima of large and medium-sized elastic and muscular arteries
• most commonly affected vessels are aorta, coronary and brain arteries
• multifactorial process
Risk factors
Main risk factors – modifiable – dyslipidaemia, hypertension, DM, smoking
– constitutional – age, gender, genetics, family and race predisposition Emerging risk factors – environmental influence, obesity, hormones, stress, inactivity, infections (CMV, HHV), high CRP
Complications
Ischemic changes of affected tissues and organs, aneurysm formation, aortic dissection, embolism
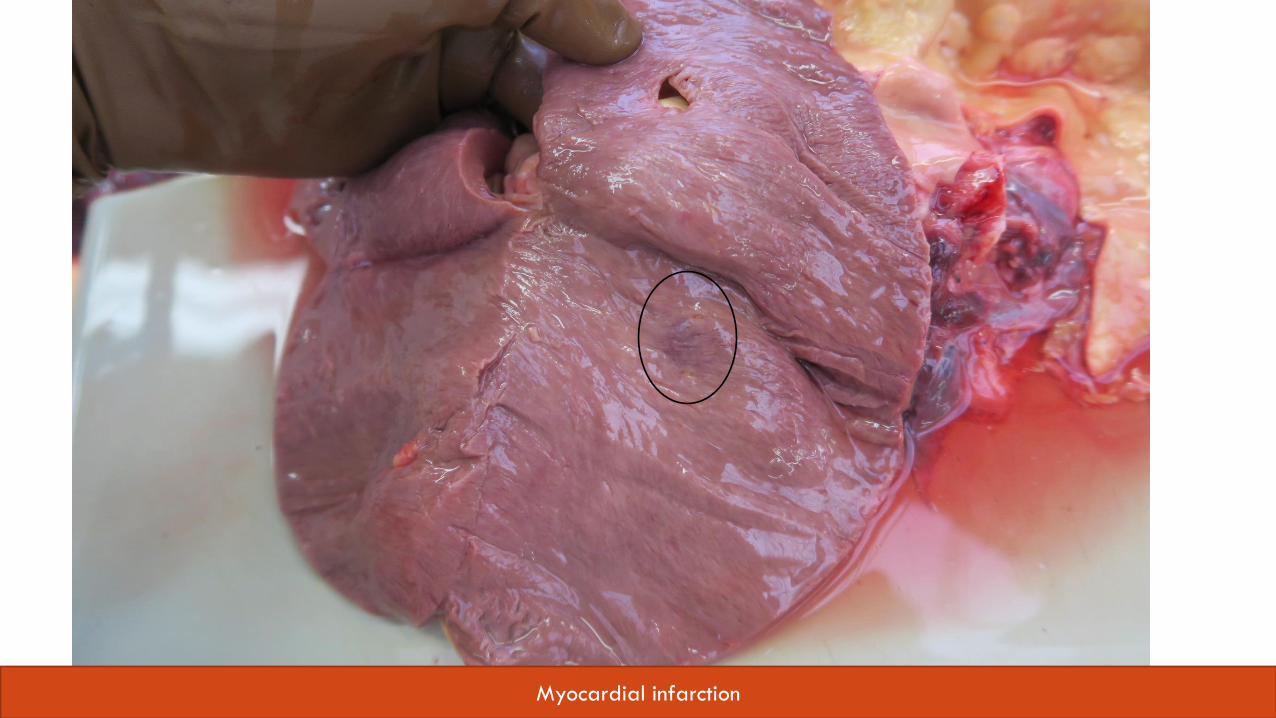
Myocardial infarction
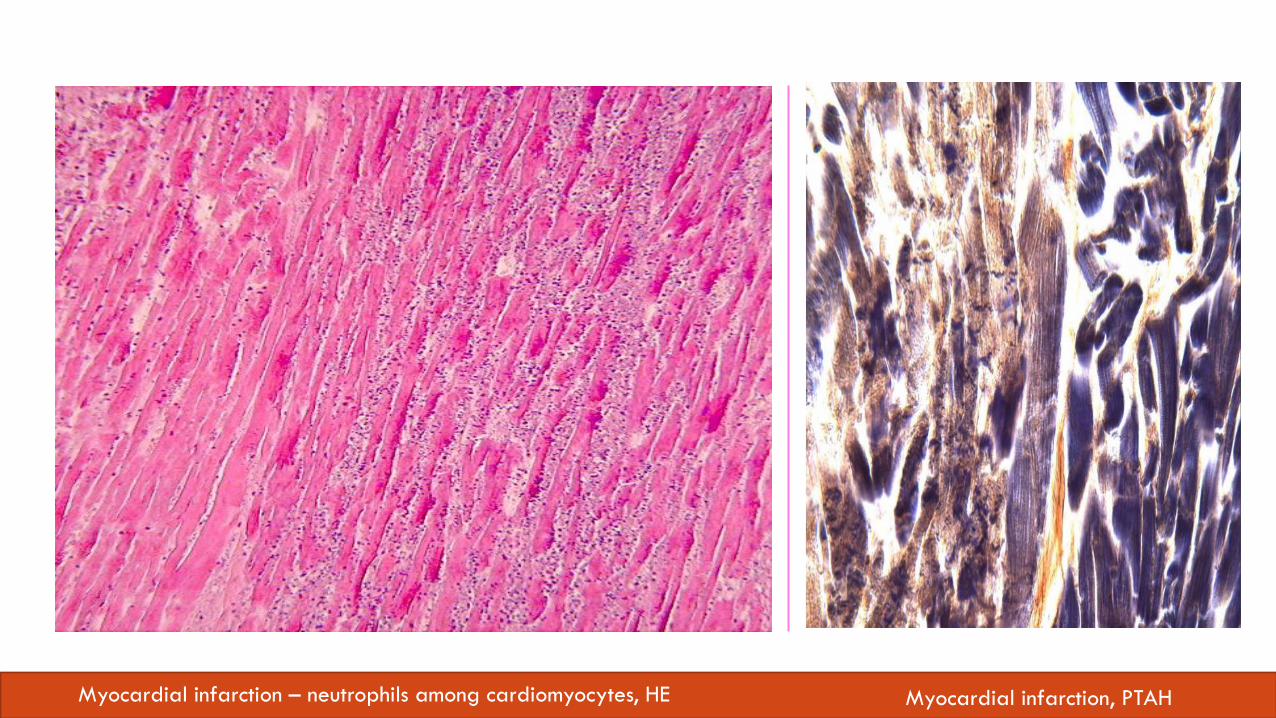
Myocardial infarction – neutrophils among cardiomyocytes, HE Myocardial infarction, PTAH
MYOCARDIAL INFARCTION
• acute necrosis of cardiomyocates due to long lasting ischemia
• blockage of coronary artery, rupture of atherosclerotic plaque, arteritis, spasm, cardiac arrhythmia with thrombosis
A classic example of coagulative necrosis which fully develops in a matter of several hours. The loss of the integrity of cytoplasmatic membrane of cardiomyocytes results into release of myocardial ensymes into blood, the levels of which are used as a biochemical diagnostic marker of MI – troponin.
CASE NO.4
• 30-year-old male was admitted to the emergency room for sudden onset of high fever with chills. On auscultation, a new murmur can be heard on the mitral valve. Physical examination revealed petechial hemorrhages under the nails, painful nodules on the tips of the fingers, erythematous rash on hands and feet and white plaques with hemorrhagic rim on the retinae.
• Diagnosis?
• Complications?
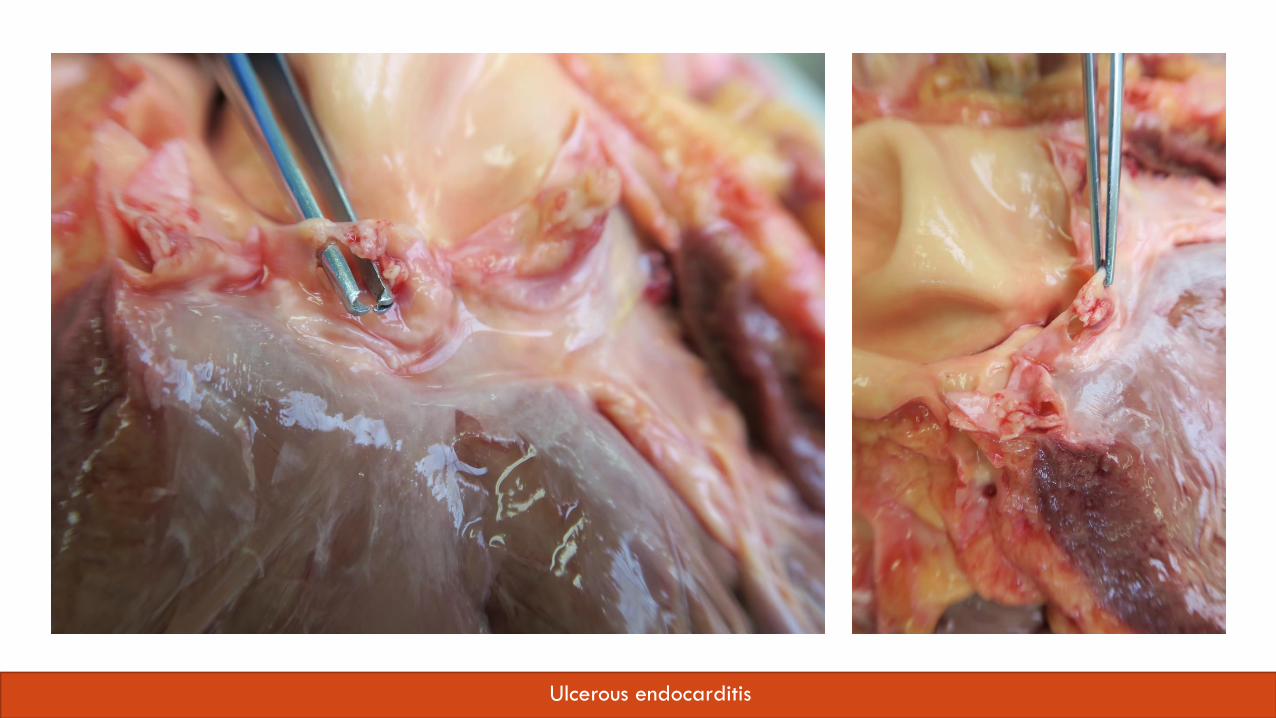
Ulcerous endocarditis
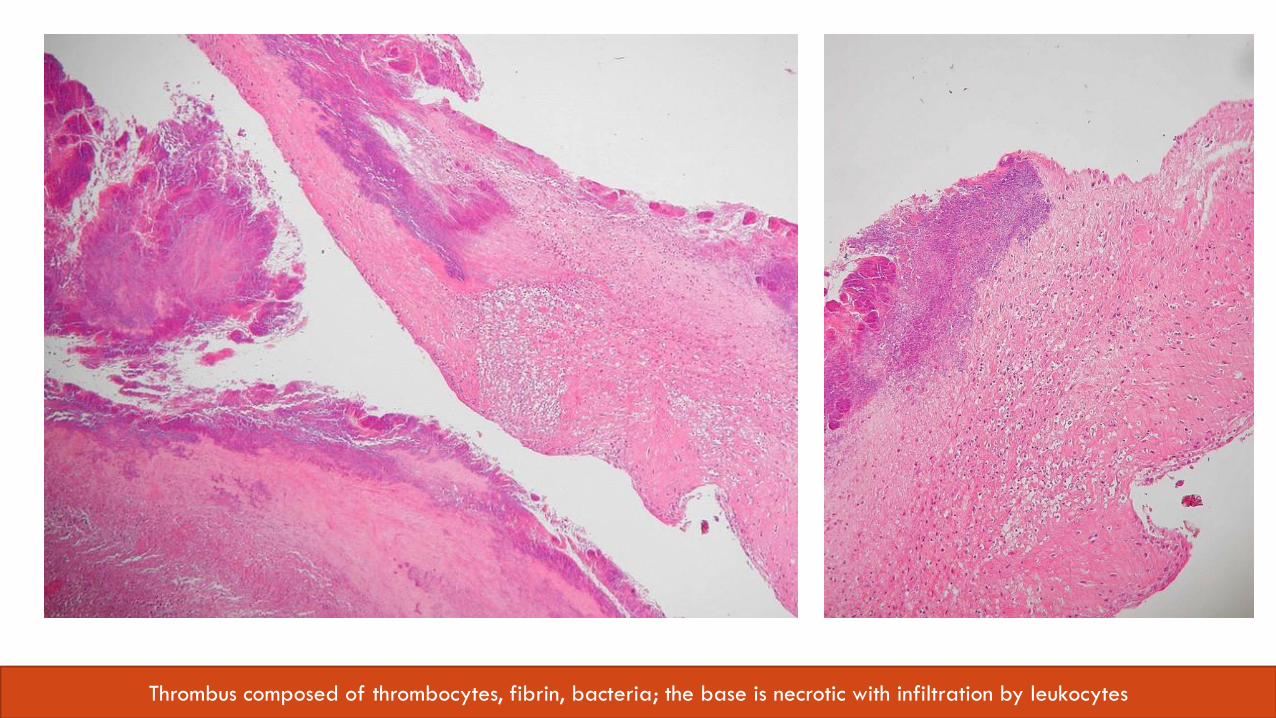
Thrombus composed of thrombocytes, fibrin, bacteria; the base is necrotic with infiltration by leukocytes
ENDOCARDITIS
1. Non-infectious endocarditis
• Atypical verrucous (Libman-Sacks) – in SLE
• Non-bacterial thrombotic (marantic, cachectic)
• Rheumatic endocarditis (rheumatic fever)
2. Infectious endocarditis
• Bacterial endocarditis
• other: mycotic, TBC, rickettsia, syphilitic, viral, ...
Typical lesion = vegetation (plateles, fibrin, inflammatory cells + microorganisms)
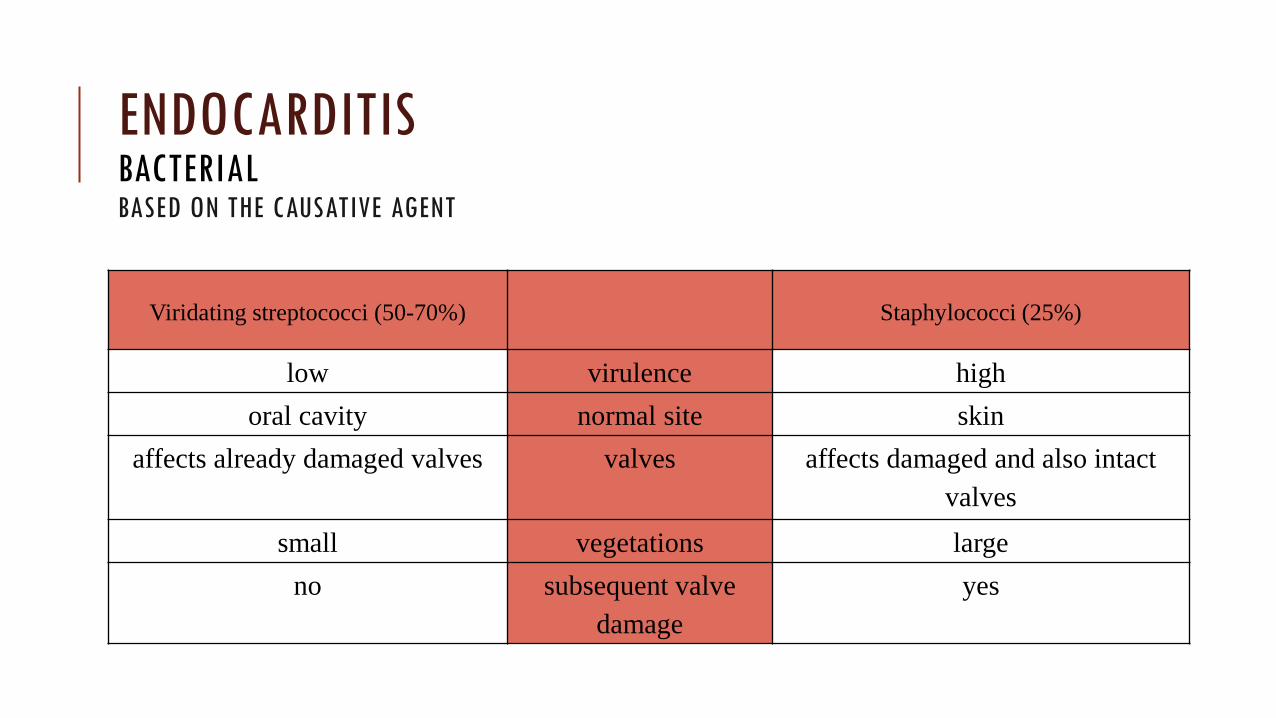
Viridating streptococci (50-70%)
Staphylococci (25%)
low virulence high
oral cavity normal site skin
affects already damaged valves valves affects damaged and also intact
valves
small vegetations large
no subsequent valve
damage
yes
ENDOCARDITIS BACTERIAL BASED ON THE CAUSATIVE AGENT
BASED ON MORPHOLOGY AND COURSE
1. Endocarditis maligna acuta (ulcerosa)
• infectious vegetation, necrosis and ulceration present
Vegetation – nodular, red, yellow to greenish, soft consistency, especially on the aortic and mitral valve
– tricuspid valve involvement - especially in intravenous addicts and with a long-term catheter inserted into the right heart
Necrosis and ulceration – “bitten out” free edge of the valve
– center of the valve - aneurysm to perforation of the valve
– ulcus cordis acutum on the wall endocardium
Healing – organisation of vegetation by granulation tissue, with subsequent fibrous change of the valve, often calcified
ENDOCARDITIS BACTERIAL
2. Endocarditis maligna lenta (polyposa)
• less prominent ulcerations
• vegetation formation with a polypoid shape
• most commonly affected are mitral and aortic valve
Complications
• cardiac - valve insufficiency, valve stenosis, valve rupture, myocardial abscess formation, heart failure, AV conduction disorders
• systemic - embolisation of parts of the vegetation, Löhlein nephritis, deposition of immunocomplexes with subsequent formation of fibrinoid vascular wall necrosis
• Diagnostics
• blood culture, echocardiography, physical examination
BASED ON MORPHOLOGY AND COURSE
ENDOCARDITIS BACTERIAL
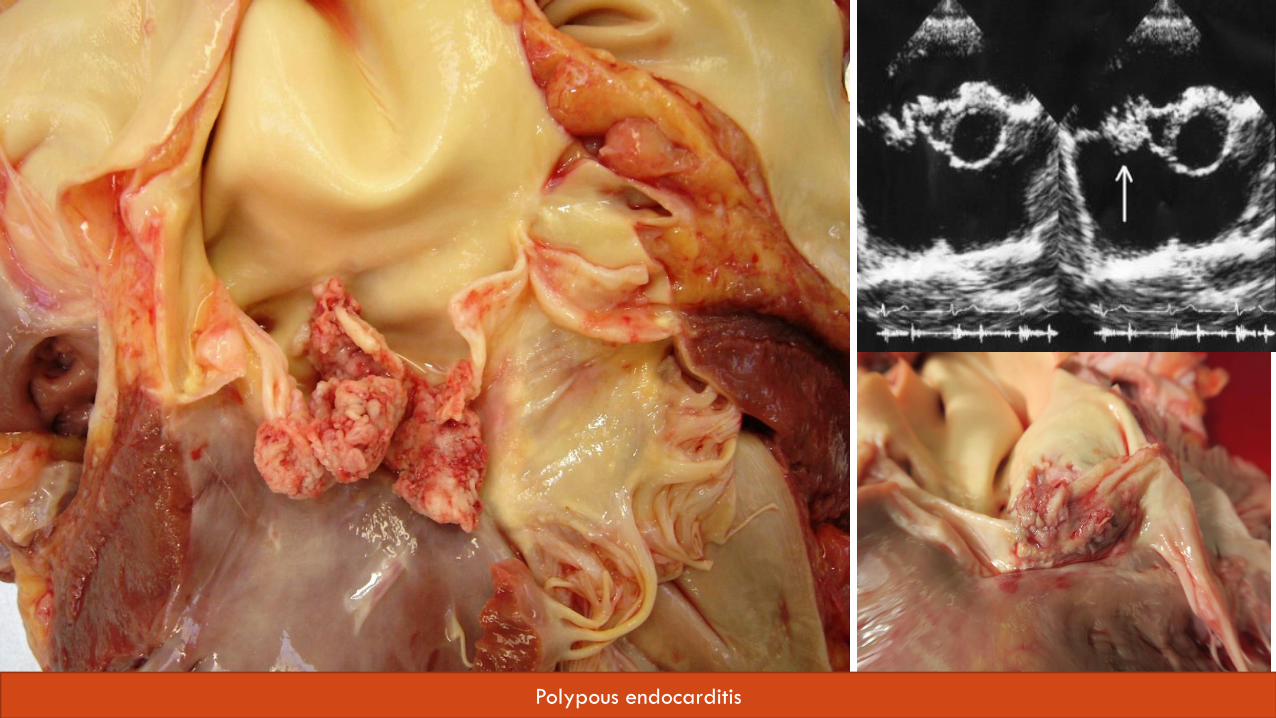
Polypous endocarditis
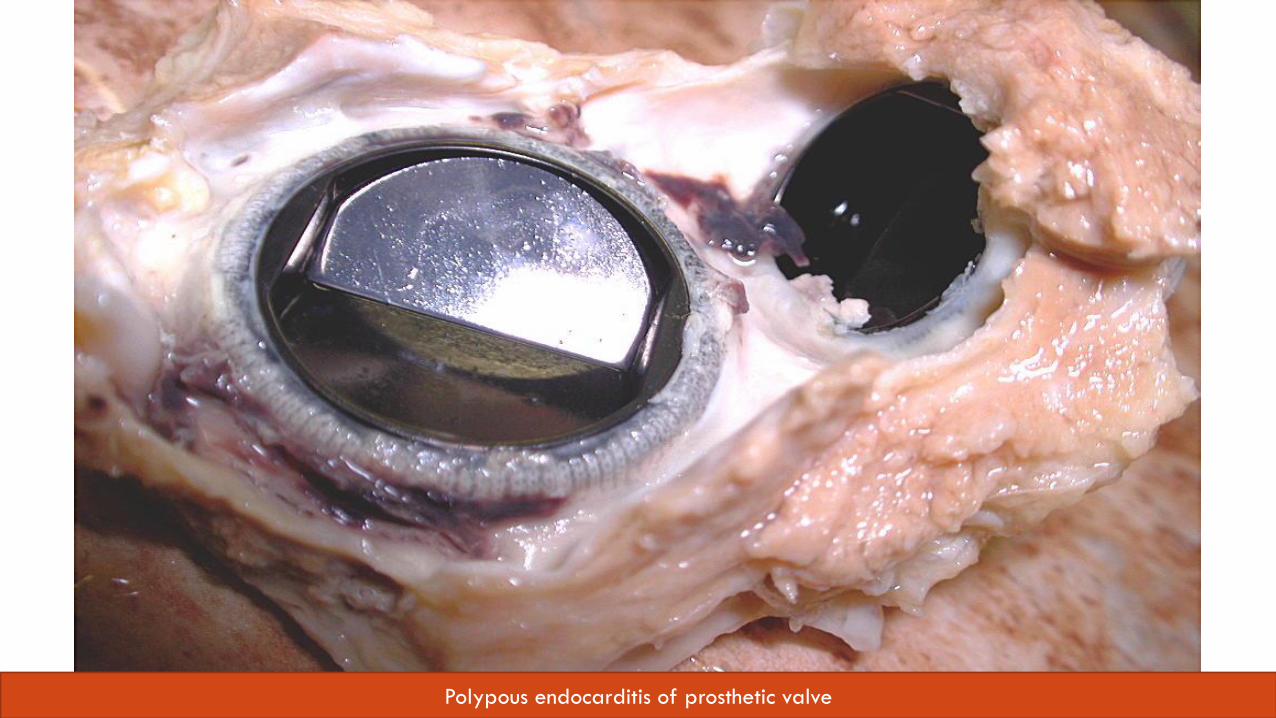
Polypous endocarditis of prosthetic valve
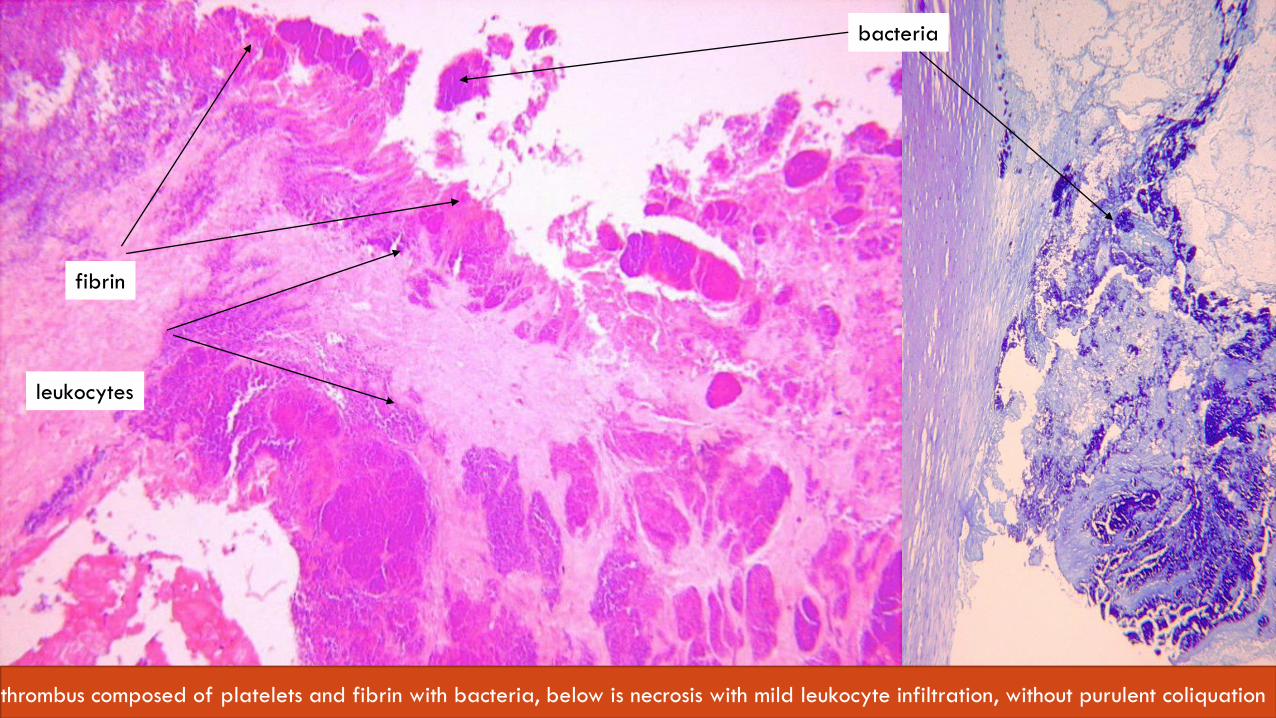
bacteria
fibrin
leukocytes
thrombus composed of platelets and fibrin with bacteria, below is necrosis with mild leukocyte infiltration, without purulent coliquation
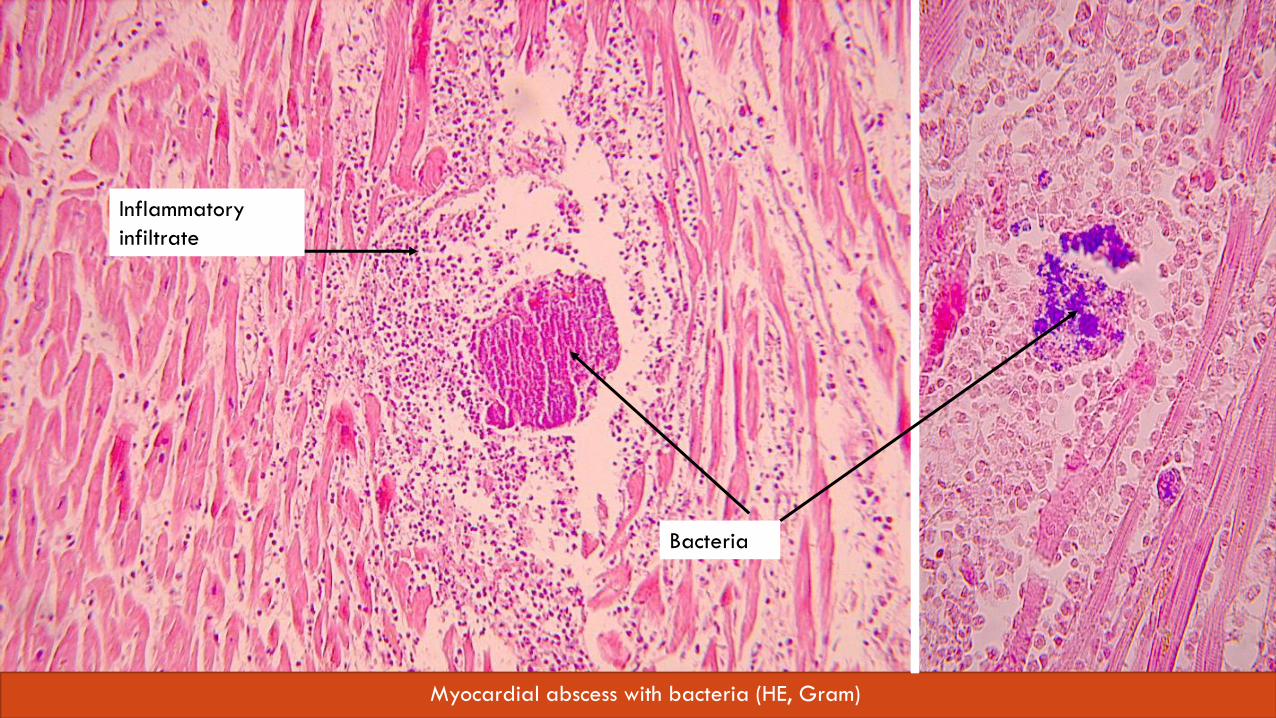
Inflammatory
infiltrate
Bacteria
Myocardial abscess with bacteria (HE, Gram)
ENDOCARDITIS RHEUMATIC ENDOCARDITIS
• systemic, non-purulent heart inflammation following previous upper respiratory tract infection with ß-hemolytic streptococcus
• 5.-15. year old patients
• 2-3 weeks after the resolution of infection - autoimmune reaction
(cross-reaction to the surface M-protein of streptococci, and myosin, actin, laminin, ...)
Diagnostics
• anamnesis, FV, CRP, sedimentation, ASLO, echocardiography
Complications
• cardiovascular: pancarditis, rheumatic verrucous endocarditis
• extracardiac: polyarthritis, subcutaneous nodules, arteritis, erythema marginatum, chorea minor
ENDOCARDITIS RHEUMATIC ENDOCARDITIS
Jones„ criteria
1. major criteria – carditis, chorea minor, erythema marginatum, subcutaneous nodules
2. minor criteria – fever, arthralgia, + history, CRP, FW, ECG changes
Microscopic findings
• focal inflammation of the connective tissue with the formation of Aschoff nodules
• Early stage - (after 4w), fibrinoid degeneration (dystrophy) due to mucopolisaccharide deposition
• Proliferation stage - (4-13w), nodule formation, infiltration by Lym, Ma – Anitschkow cells
• Healing stage - (12-16w), scarring of nodules, Anitschkow cells = spindle-shaped, with scarce cytoplasm and monochromatic nucleus with linear wavy condensation of chromatin
RESPIRATORY SYSTEM
CASE NO. 5
•75-year-old patient visited the general practitioner for 5-day long nausea, fever, irritating productive cough, fatigue, muscle aches, loss of appetite.
• on auscultation tubular breathing and a damped percussion above the right lower lobe of the lungs
• Diagnosis?
• Complications?

Bronchopneumonia
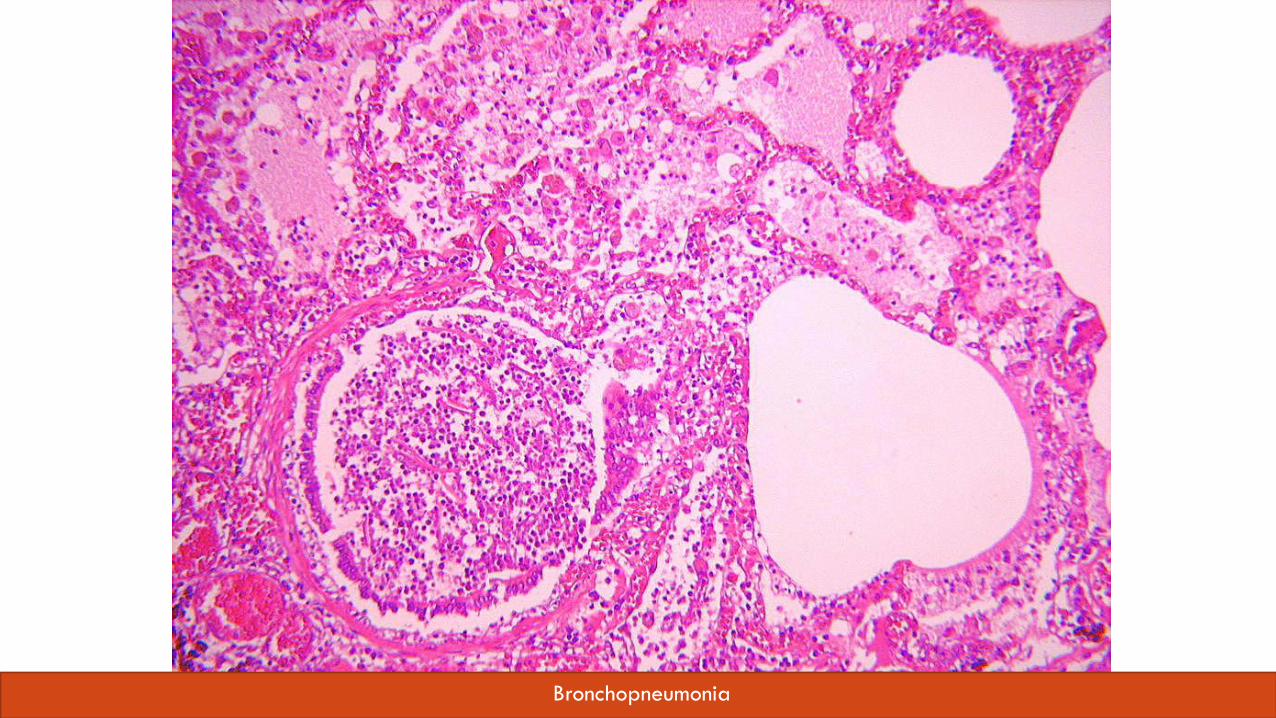
Bronchopneumonia
BRONCHOPNEUMONIA
• infection of terminal bronchioles with migration into surrounding alveoli
• common complication in bedridden patients
• complication of viral bronchitis
CASE NO. 6
• 68-year-old man admitted to the emergency room, he complains of shortness of breath, dry, irritating cough without sputum production, high fever, malaise and severe headaches. The auscultation above the entire lung lobe is hollow. The patient is being treated for type 2 DM , hypertension, suffers from exogenous obesity.
• Diagnosis?
• Complications?
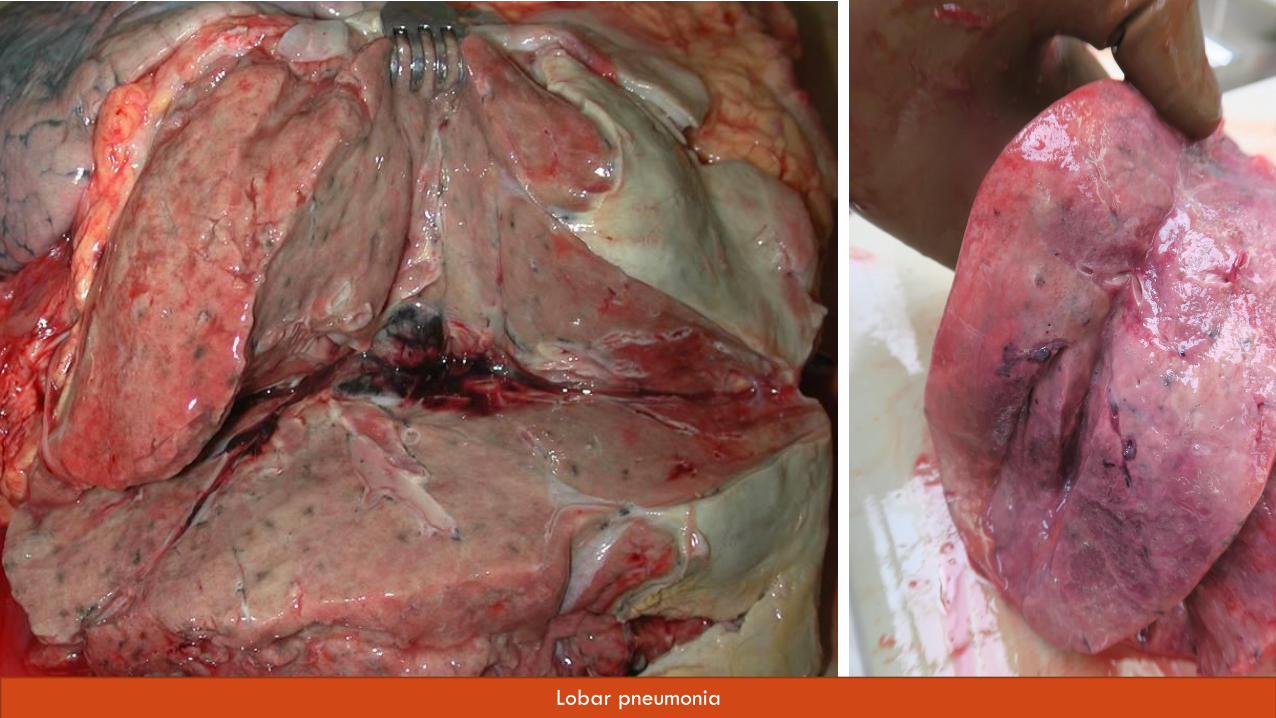
Lobar pneumonia
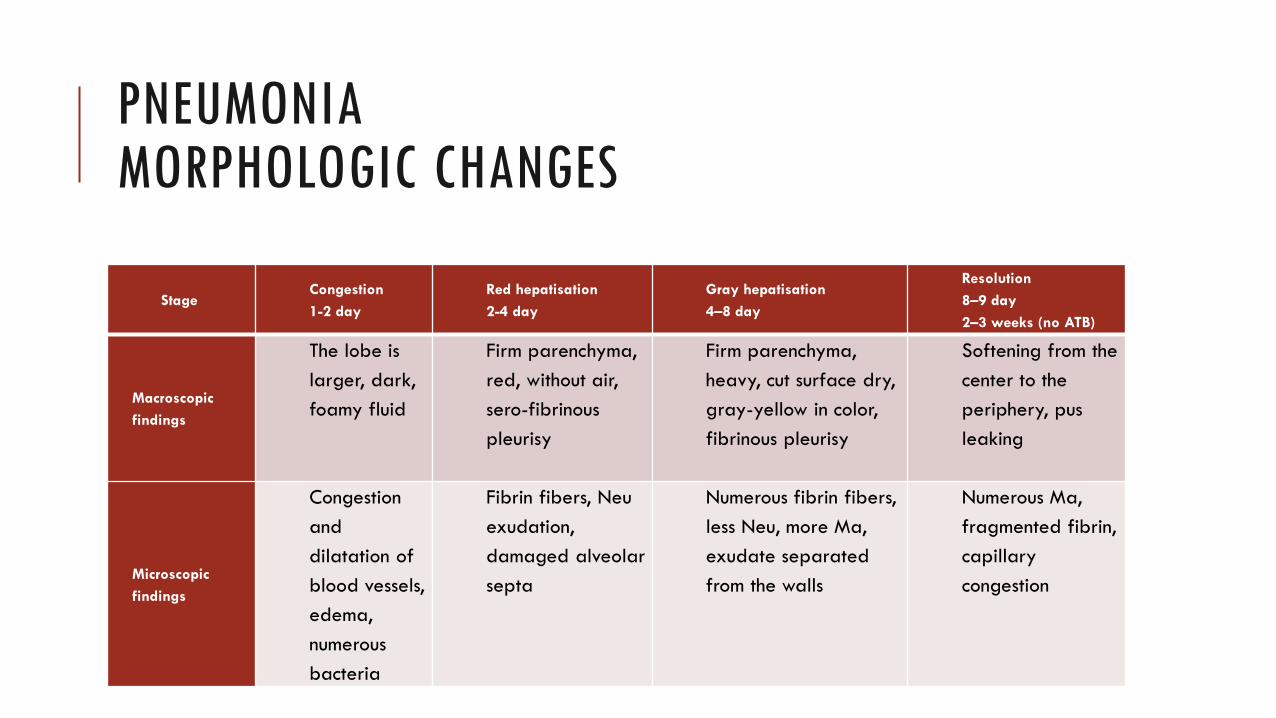
PNEUMONIA MORPHOLOGIC CHANGES
Stage Congestion
1-2 day
Red hepatisation
2-4 day
Gray hepatisation
4–8 day
Resolution
8–9 day
2–3 weeks (no ATB)
Macroscopic
findings
The lobe is
larger, dark,
foamy fluid
Firm parenchyma,
red, without air,
sero-fibrinous
pleurisy
Firm parenchyma,
heavy, cut surface dry,
gray-yellow in color,
fibrinous pleurisy
Softening from the
center to the
periphery, pus
leaking
Microscopic
findings
Congestion
and
dilatation of
blood vessels,
edema,
numerous
bacteria
Fibrin fibers, Neu
exudation,
damaged alveolar
septa
Numerous fibrin fibers,
less Neu, more Ma,
exudate separated
from the walls
Numerous Ma,
fragmented fibrin,
capillary
congestion
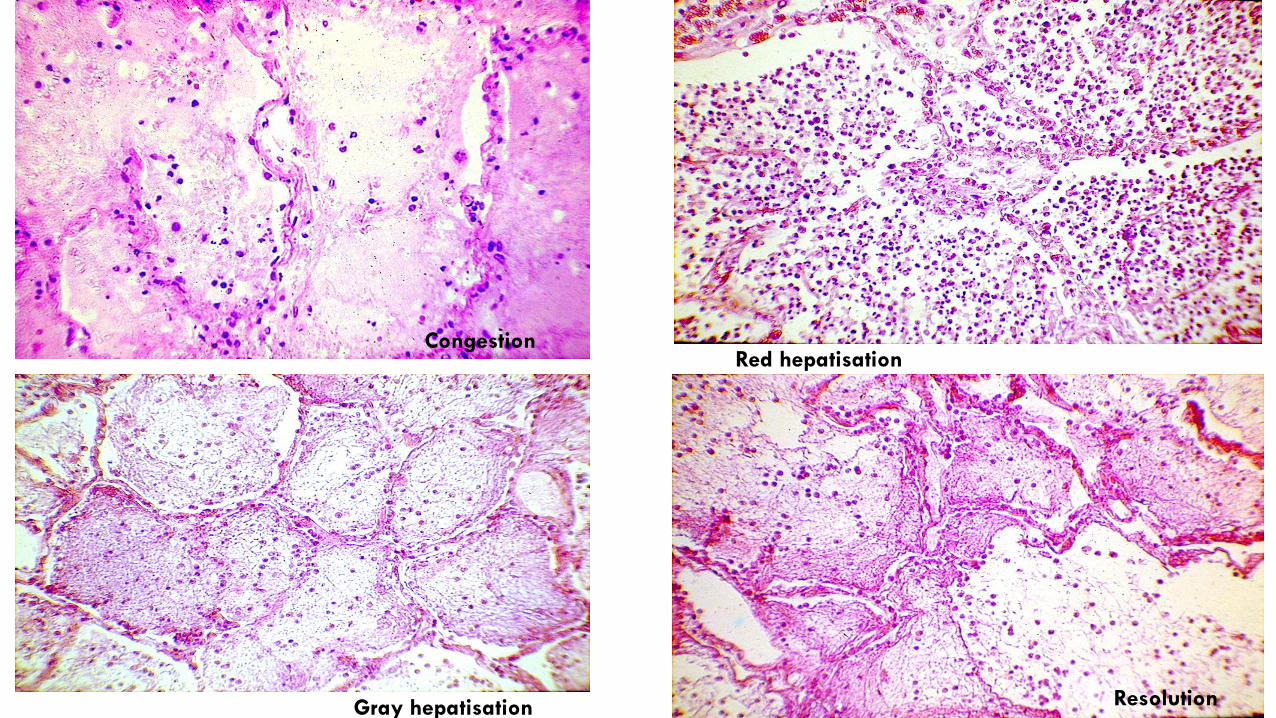
Congestion Red hepatisation
Gray hepatisation Resolution
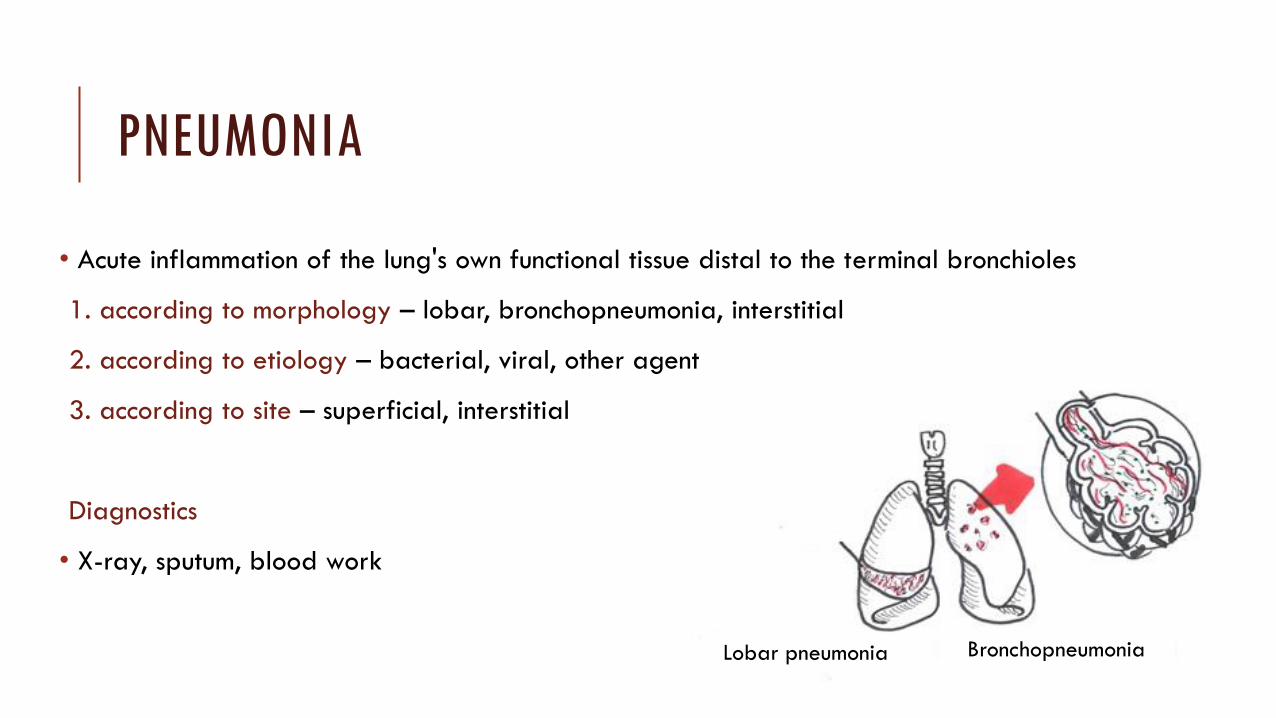
PNEUMONIA
• Acute inflammation of the lung's own functional tissue distal to the terminal bronchioles
1. according to morphology – lobar, bronchopneumonia, interstitial
2. according to etiology – bacterial, viral, other agent
3. according to site – superficial, interstitial
Diagnostics
• X-ray, sputum, blood work
Lobar pneumonia Bronchopneumonia
LOBAR PNEUMONIA
Etiology
• pneumococcal, staphylococcal, streptococcal, caused by G- bacteria
Complications
• organization of inflammation and fibrous change of lung tissue (carnification)
• pleural effusion with pleurisy (often ending in adhesions)
• empyema
• lung abscess
• metastatic infection
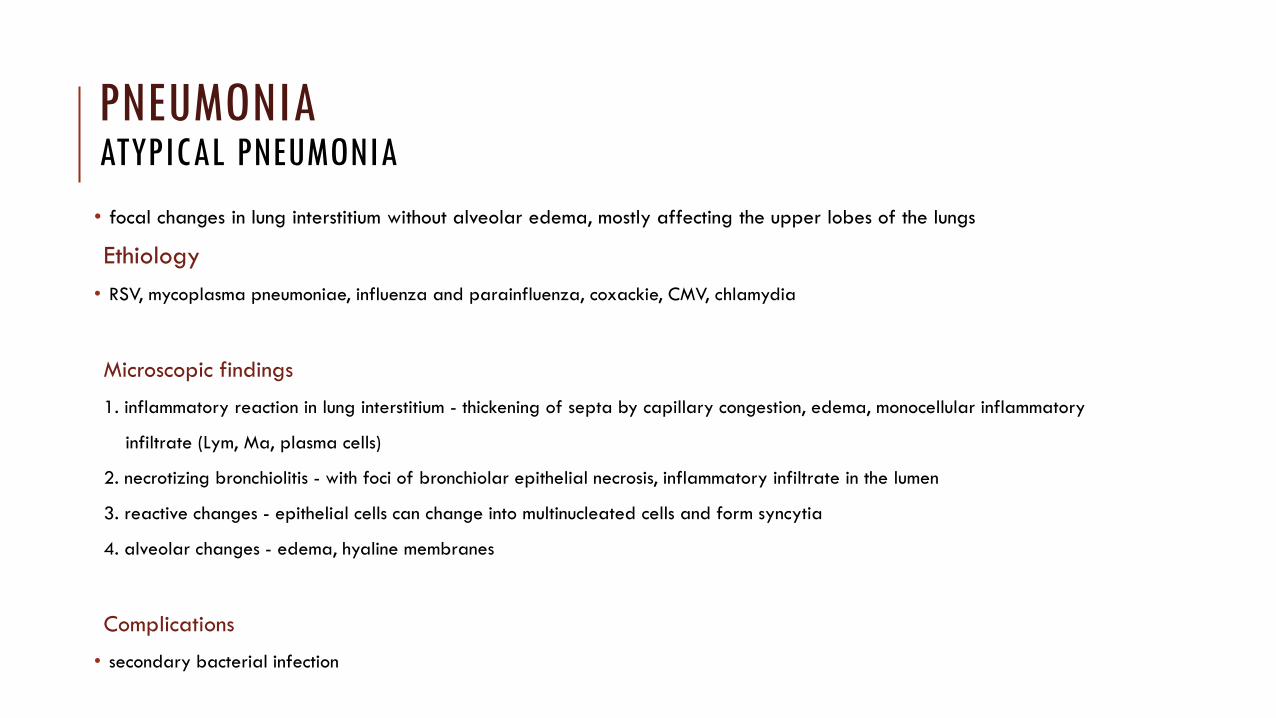
• focal changes in lung interstitium without alveolar edema, mostly affecting the upper lobes of the lungs
Ethiology
• RSV, mycoplasma pneumoniae, influenza and parainfluenza, coxackie, CMV, chlamydia
Microscopic findings
1. inflammatory reaction in lung interstitium - thickening of septa by capillary congestion, edema, monocellular inflammatory
infiltrate (Lym, Ma, plasma cells)
2. necrotizing bronchiolitis - with foci of bronchiolar epithelial necrosis, inflammatory infiltrate in the lumen
3. reactive changes - epithelial cells can change into multinucleated cells and form syncytia
4. alveolar changes - edema, hyaline membranes
Complications
• secondary bacterial infection
PNEUMONIA ATYPICAL PNEUMONIA
CASE NO. 7
• a 71-year-old woman felt a lump on her right breast, in addition to complaining of restless shortness of breath and weight loss (10 kg in half a year)
• breast mammography reveals a tumour lesion in the left breast as well
• core cut biopsy with the conclusion of "small blue cells"
• whole-body CT revealed nodular structures in the liver, heart and chest
• she stopped smoking cigarettes two months ago (until then 15 cigarettes a day, for 30 years)
• Diagnosis?
• Describe the method of material collection.
• Complications?

Small cell lung carcinoma with metastasis to the chest wall

Metastasis of small cell carcinoma to liver and pericardium
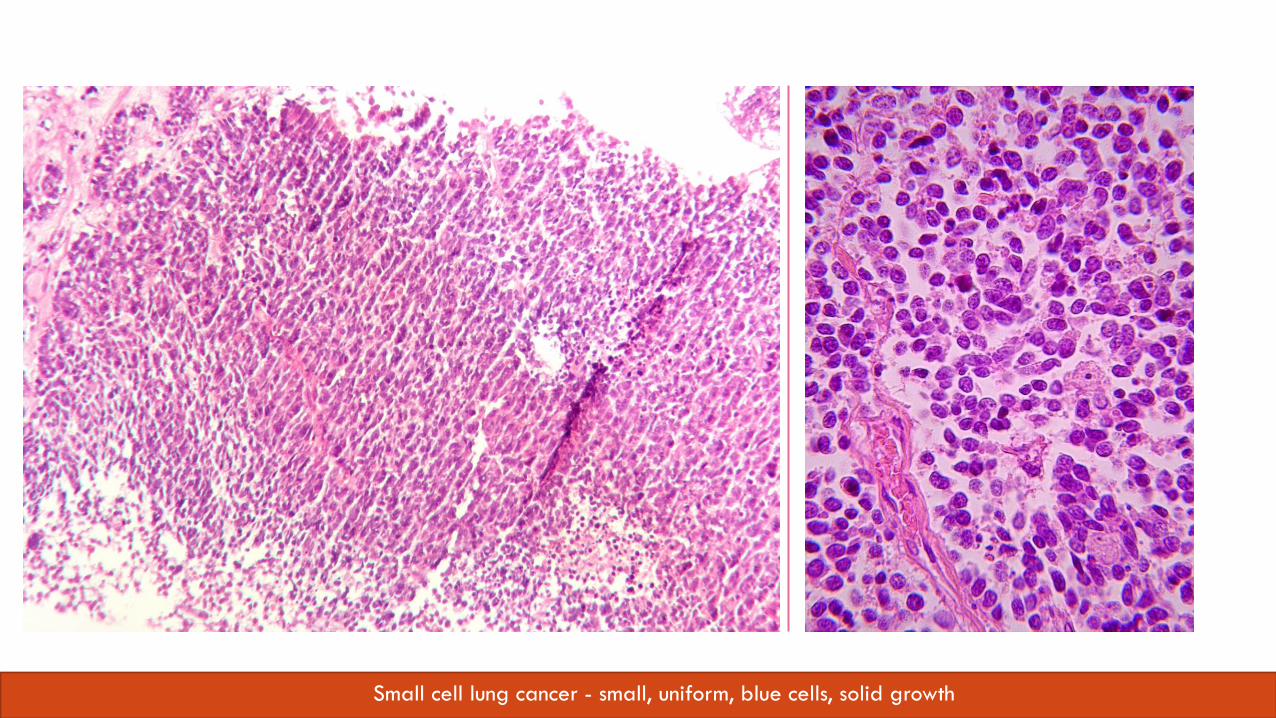
Small cell lung cancer - small, uniform, blue cells, solid growth
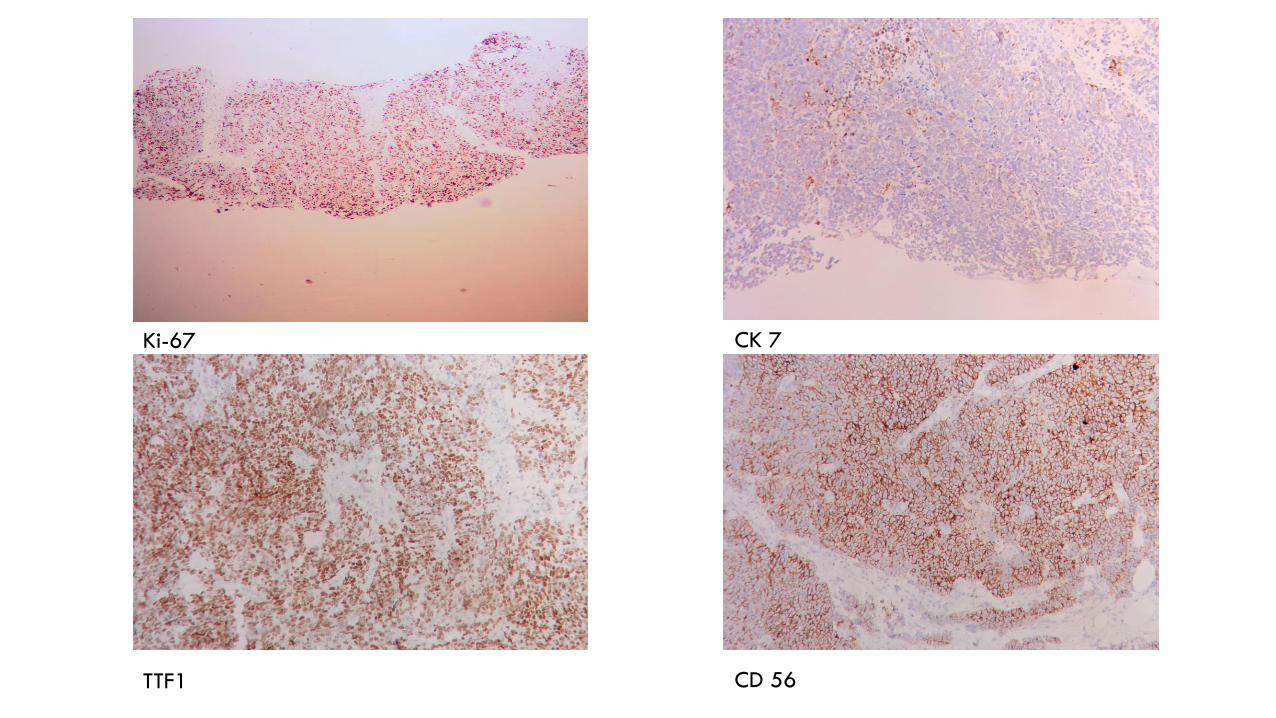
Ki-67
TTF1
CK 7
CD 56
SMALL CELL LUNG CARCINOMA SCLC 20 – 25%
• aggressive tumor
• central location
• strong association with smoking
• frequent paraneoplastic syndrome (hormone production)
• rapidly metastasizing tumor
• limited surgical treatment
• worse prognosis
PARANEOPLASTIC SYNDROME
• often accompanies small cell lung carcinoma
• nervous system dysfunction without direct tumor invasion, infections or vascular complications of nervous tissue
• cachexia is part of the manifestation
• ACTH - the source is SCLC, causes paraneoplastic Cushing's syndrome (central obesity, rounded face, stretch marks, hypertension, hyperglycemia, virilization and amenorrhea in women)
• SIADH
• Lambert–Eaton syndrome – myasthenia gravis due to defective acetylcholine secretion
CASE NO. 8
• 57-year-old patient was admitted to the internal medicine department on the recommendation of a general practitioner for an 8-week irritating cough that does not subside after ATB treatment
• yesterday he found blood in sputum, has fatigue, can not quantify the weight loss
• has been smoking continuously for 30 years
• Diagnosis?
• Proposed examinations?
• Complications?

Centrally growing lung cancer - squamous cell type
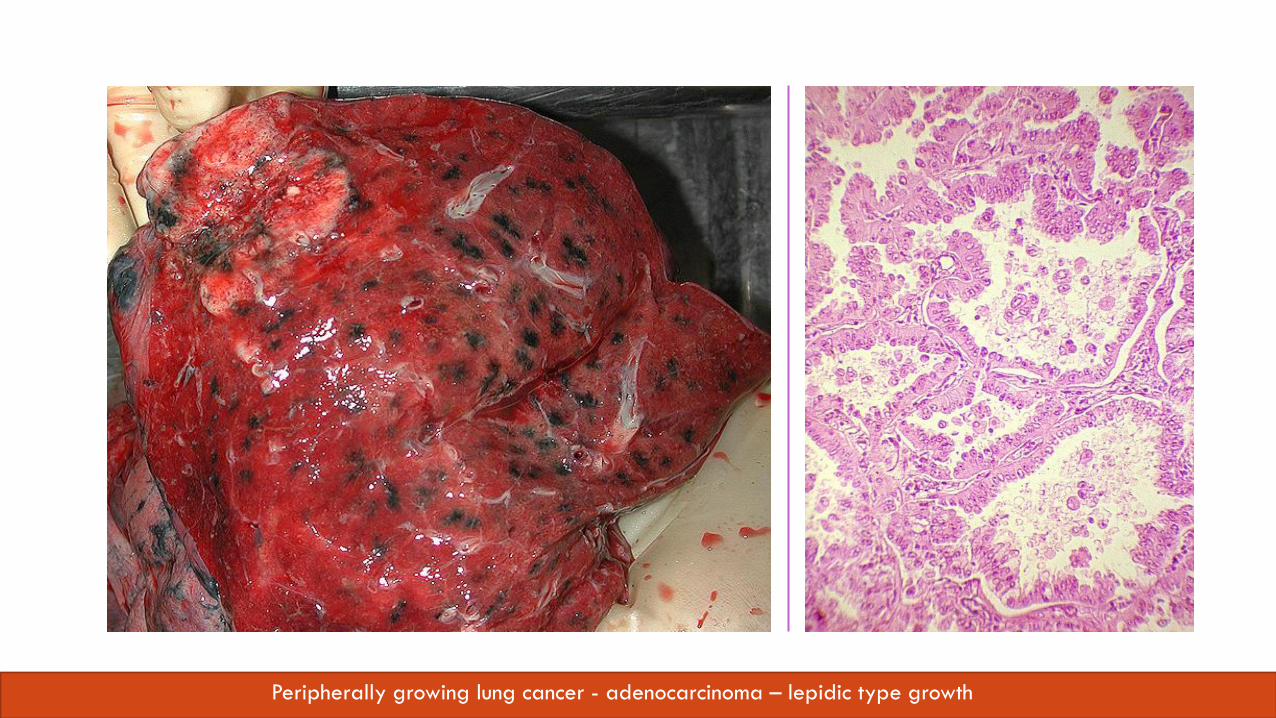
Peripherally growing lung cancer - adenocarcinoma – lepidic type growth
NON-SMALL CELL LUNG CANCER NSCLC CCA 75%
• a histologically diverse group of cancers
• lung adenocarcinoma grows predominantly peripherally
• squamous cell carcinoma grows predominantly centrally
• mostly slow growth
LUNG TUMORS
WHO classification 2015
I. Epithelial tumors • Benign
Papiloma
Adenoma
• Malignant
II. Connective tissue tumors
chondroma, myoepithelioma, ...
III. Lymphohistiocytic tumors
lymphomas, ...
IV. Tumors of ectopic origin
malignant melanoma, teratoma, ...
Secondary tumors
Historical clinical classification
1. Malignant epithelial lung tumors
• Small cell lung tumors (SCLC)
• Non-small cell lung tumors(NSCLC)
• adenocarcinoma • grows most often on the periphery - Pancoast tumor in the lung
apex
• Lepidic type – grows along surface of alveolar walls
• epidermoid carcinoma • grows mainly in the central part of the lungs
• neuroendocrine carcinoma
• large cell carcinoma
• adenosquamous carcinoma
• pleomorphic carcinoma
• spindle cell carcinoma
LUNG TUMORS
Etiology
• smoking, living in the city, profession, lifestyle,
chronic diseases, genetic predisposition, infections
Diagnostics
• X-ray
• Bronchoscopy - collection of material for histological examination using a brush for cytological examination, macroscopically it is possible to evaluate changes
• Video-assisted thoracoscopy (VATS) - biopsy / resection of a part of the lung parenchyma.
• Mediastinoscopy
• Transparietal biopsy – under X-ray / CT visualisation (mainly lesions on the periphery)
• Cryobiopsy
LUNG TUMORS MOLECULAR PATHOLOGY
• the exact morphological classification and evidence of specific genetic changes affect the patient's therapy and prognosis
• Genetic changes in tumors idnetify patients suitable for individual types of anti-tumor therapies
• used mainly in the group of non-small cell lung cancers (NSCLC)
• BRAF, EGFR, KRAS, RB, TP53.....
EGFR
• affects proliferation of cells
• inhibitors of tyrosin kinase receptors in therapy
• 10 – 15% of all NSCLC
EML4/ALK fusion gene
• 5% of all NSCLC
Summary
• Atherosclerosis and arterial hypertension contribute to heart failure
• In right-sided failure we observe venostasis in the liver and spleen
• In left-sided failure we observe edema and venostasis of the lungs
• Embolism is a life-threatening condition
• The most common cause of embolism is lower limb venous
thrombosis
• The most common cause of pneumonia is streptococcal infection
• Bronchopneumonia (inflammation on the level of smaller bronchi) is
a common complication in bedridden patients
• The most common lung tumors are adenocarcinoma, squamous cell
carcinoma and small cell carcinoma
• Morphological and molecular diagnosis of lung tumors is important
in terms of prognosis