Embed Size (px)
Citation preview

Pits & fissures caries in early stage, brown-discoloration in the pits or in the fissures
Probe
Mirror
Radiograph
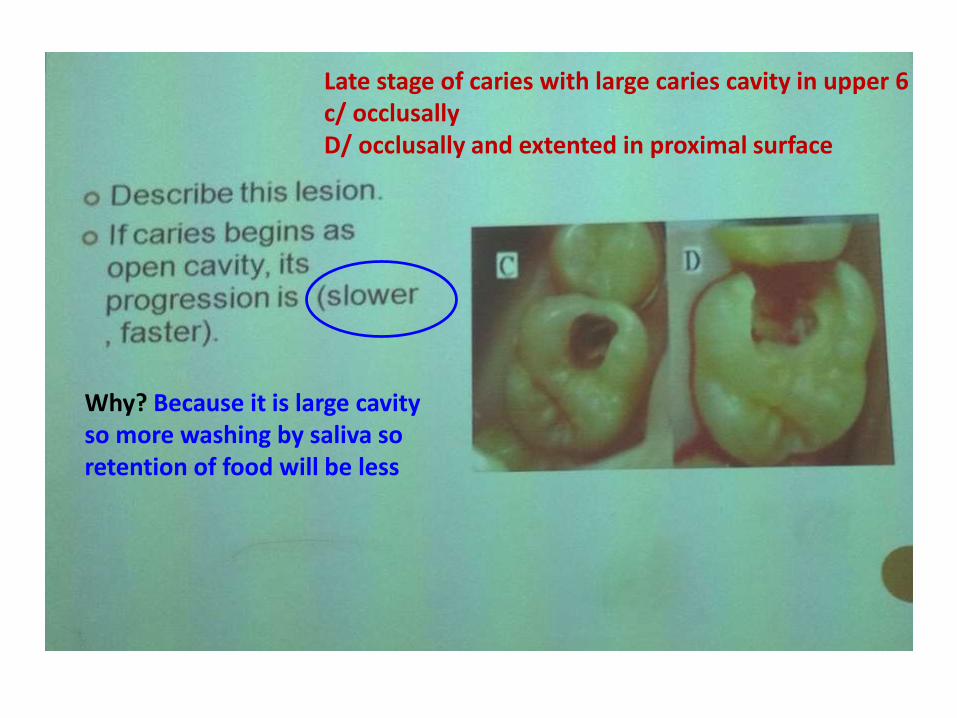
Late stage of caries with large caries cavity in upper 6c/ occlusallyD/ occlusally and extented in proximal surface
Why? Because it is large cavity so more washing by saliva so retention of food will be less

SmoothProximal
Dental plaque
1-Caries in anterior tooth in smooth surface ( gingival third ), cavity with uniform out line
2- Caries in anterior teeth in proximal surface, bluish discoloration around the cavity

Patient having multiple caries lesion in gingival third , incisal, and occlusal surfaces.
Due to gingival recession exposing the root surfaces and they have also reduce salivary flow

Decalcified section in dentine in early stage showing beading in dentinal tubules
Transverse clefts
When caries spread along the lateral (transverse) branching in dentinal tubules.

Patient presented with bad restoration resulted as bluish discoloration around the restoration due to recurrence of caries
Inadequate extension leading to retention of food
Poor adaptation of filling
All caries is not removed

Decalcified section in pulp tissue showing dilated B.Vs & extravasated RBCs
Hyperemia of the pulp

Decalcifies section in pulp tissue showing pathological cavity rich of debris (contain pus )
Pulp abscess

1-
2-
1- Patient having red mass protruding in the caries cavity in lower 6
2- decalcified section showing tooth with large cavity of pulp tissue into pulp cavity , this pulp tissue contain granulation tissue covered by thin layer of epithelium
Diagnosis : Pulp polyp

Swelling of sort tissue related to upper 4
Decalcified section showing cavity debrisSurrounded by dense bundles of collages fibers.
Diagnosis : Periapical abscess

Radiolucency related to apex of lower 6

Periapical radiolucency in lateral tooth, and the patient have proximal caries

Periapical granuloma with proliferated epithelium
Cholesterol clefts

Patient have protruded whitish lesion (sequestrum)
Decalcified section showing bone marrow infiltrated by acute inflammatory cells
Acute Osteomyelitis
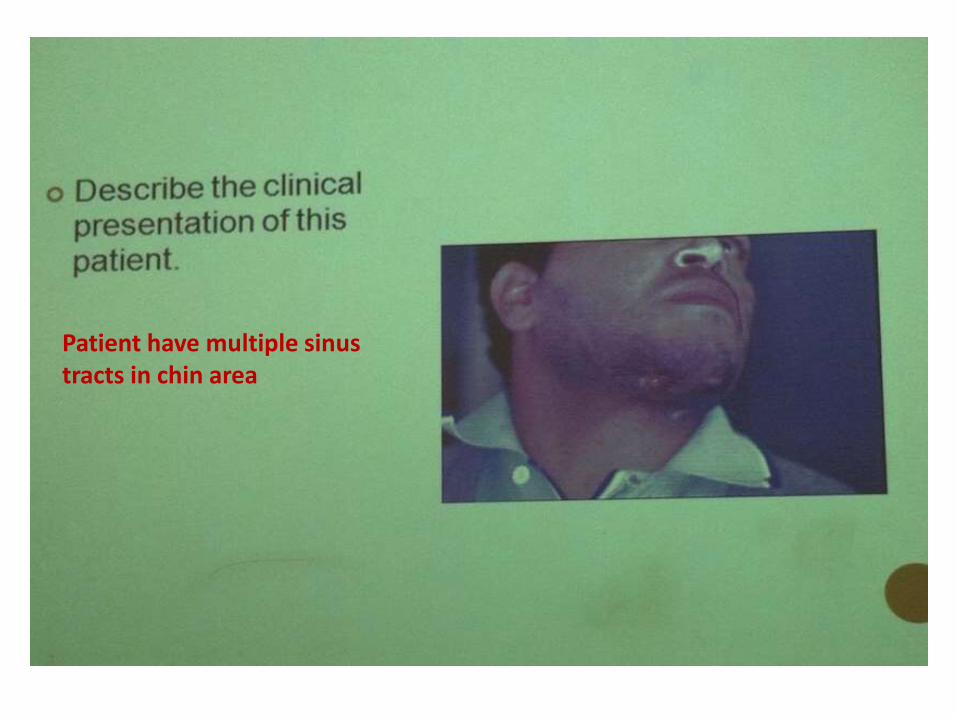
Patient have multiple sinus tracts in chin area
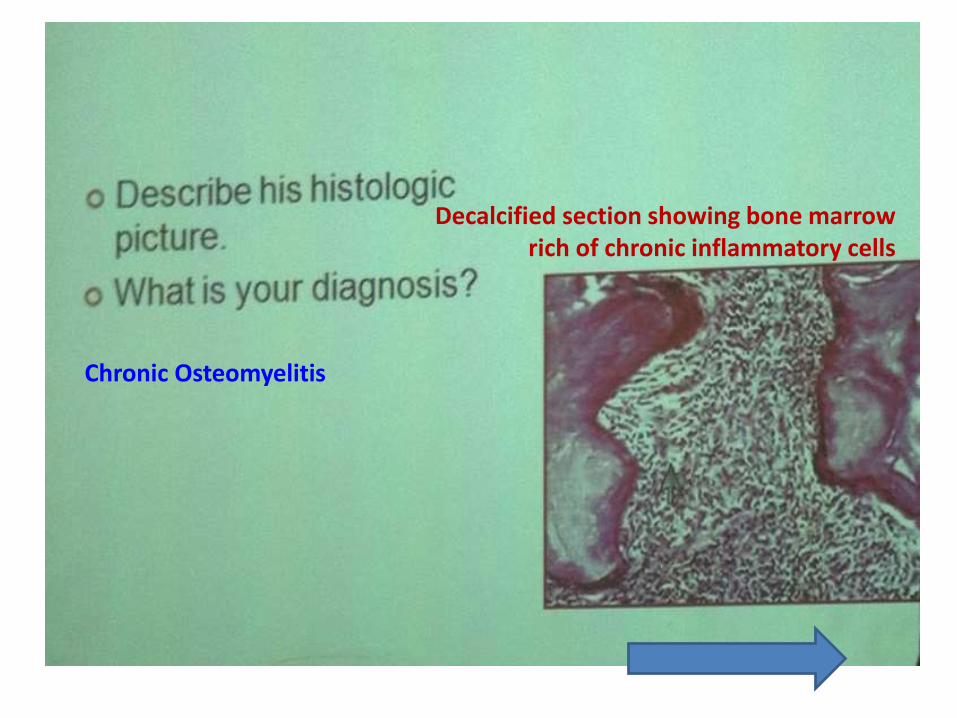
Decalcified section showing bone marrow rich of chronic inflammatory cells
Chronic Osteomyelitis

Radiopaque area surrounding the apex of lower 6

Dense masses of bone trabeculae contain osteocytes and rim of osteoblasts
Chronic focal sclerosing osteomyelitis

Patient have swelling in the part of the mandibleposterior

Occlusal film showing deposition of bone into layers of buccal aresaresult as enlargement of mandible showing periosteal ( outer cortical plate ) duplication or onion skin appearance
Garre’s osteomyelitis ( condensing periotitis), (Chronic osteomyelitis with proliferative periostitis)


Periapical lesion associated with extracted molar teeth
Cyst cavity lined by non-keratinized S.S.E and under line C.T
Unilocular radiolucency well defined with radiopaque margin in association with periapical part of non vital tooth Radicular Cyst

A/ well defined unilocular radiolucent lesion in association with vital teeth
C/ Large multilocular radiolucent lesion in association with root of posterior teeth
C/ Odotogenic Keratocyst , Aneuresmal bone cyst , AmeloblastomaA/ periapical cemental dysplasia

1- Diagnosis : Thyoglossal cyst2- Describe the clinical picture: Swelling at the midline of the neck3- Describe the histological picture : Cyst cavity in the posterior part lined by S.S.E & C.T and thyroid follicles in the upper part of slide

1
23
* Diagnosis : Nevoid basal cell carcinoma ( Gorlin Syndrome )* Describe : 1- Multiple basal cell carcinoma
2- well defined radiolucency3- The histology of odontogenic keratocyst

Extracted canine in association with cystic lesion, the cyst attached to the tooth at CEJ
Unilocular well defined periapical lesion in association with unerupted tooth
Cyst cavity lined by non-keratinized epithelium
Dentigenous cyst

Cyst associated with erupted upper maxillary
Histology of eruption cyst ( cyst cavity lined by non-keratinized epithelium & C.T

1- Extracted tooth associated with cystic lesion
2- Odontogenic Keratocyst
3- Radiolucent lesion in the posterior part of mandible ( associated with vital tooth ) , it may be : * Central intraosseuos tumor , * Metastatic tumor, *Odontogenic tumor , *Odontogenic keratocyst.

Gingival lesion showing nodular mass of the mandibular facial gingiva
Cyst cavity lined by epithelium contain : stellate reticulum ( ameloblast like cells ), Ghost cells, calcification area . - C.T rich of inflammatory cells
Well defined radiolucent lesion in associated with unerupted tooth
D.D : Gingival fibromas, Gingival cyst, periapical giant cell granulomas
Diagnosis : Gorlin cyst


1- huge swelling of the jaw
2- multilocular radiolucency, bone destruction is replaced by small well defined radiolucent areas giving rise to the honeycomb or soap-bubble appearance.
3- long anastomosing cords of epithelium cells bounded by columnar/ cuboidal cells, cells within cords are stellatereticulum like cells.
4- plexiform type of ameloblastoma


1- * pindborg tumor
* AOT ( Adenomatoiod odontogenic tumor )
* Gorlin cyst
* Ameloblastic fibroma
2- round area of concentric calcification deposits ( liesegang rings ) seen in amyloid material.
3- pindborg tumor


1-* folliacular type of ameloblastoma.
* plexiform type of ameloblastoma.
* Ameloblastic fibroma
2- it is formed of islands of epithelial follicles with microcyst or multi cyst, the individual follicles show central mass of stellate reticulum like cells surrounded by single peripheral layer of ameloblast- like cells, the nuclei of the peripheral cells have reversed polarity.
3- folliacular type of ameloblastoma.
![Revisiting Structure Graphs: Applications to CBC-MAC and …PRF analysis of truncated CBC [15]. Any revision in the FCPpf 2;‘ bound [3] will also necessitate revision of bound in](https://img.pdfslide.net/doc/110x75/6026c1842c95b234ac73b7b0/revisiting-structure-graphs-applications-to-cbc-mac-and-prf-analysis-of-truncated.jpg)









![NAME SYNOPSIS −AdDeflLnNOpqRStuUvxX ][esj/cnt4504/reading/tcpdump.1.pdf · TCPDUMP(8) TCPDUMP(8) Algorithms may bedes-cbc, 3des-cbc, blowfish-cbc, rc3-cbc, cast128-cbc,ornone.The](https://img.pdfslide.net/doc/110x75/604e8bc7dec7c8115c72cbfe/name-synopsis-aaddeilnnopqrstuuvxx-esjcnt4504readingtcpdump1pdf-tcpdump8.jpg)

















