Embed Size (px)
Citation preview

Ranjita PallaviInternal Medicine, PGY-3
EM/IM/Surgery Conference

• Patient arrived to MICU on April 15,2014 at 0145.
• VS on arrival: BP 102/55 HR 109 RR 18 Sat 94% T 98.8 F FS 140.
• Started on maintenance IV fluids.
• Piperacillin/Tazobactam was continued based on prior urine culture and sensitivity report.
• Patient remained hemodynamically stable overnight.
MICU Course

• A Neck and Chest CT were done the subsequent morning for locating the site of the guidewire whether it was intra-luminal or in the soft tissue.
• Neck CT w/o contrast: Right-sided catheter within the lower neck, looped around the right internal jugular vein and common carotid artery, its tip abutting the anterior aspect of the right carotid artery.
• Chest CT w/o contrast: Pulmonary venous congestion, interstitial edema and moderate b/l pleural fluid collections.
MICU Course

• Hence as per the CT, the guidewire appeared to pierce the IJV coming out through the back wall and going around the carotid sheath but staying outside of the vessel wall.
• Thus, an IR attempt to retrieve the wire was not pursued and patient was taken to the OR on April 15 at 1448.
• He underwent right neck exploration and removal of the foreign body with right internal jugular repair.
• He was subsequently transferred to SICU for monitoring for 24 hours.
• Patient came back to MICU the following day.
MICU Course

• Venous duplex b/l lower extremity done in view of swelling noted over the LLE showed evidence of chronic DVT in left common femoral vein but acute DVT in the left popliteal vein.
• Chest CT ruled out acute pulmonary embolism.
• Owing to high risk of bleeding from recent neck exploration and low risk from left popliteal thrombosis, anticoagulation was withheld and plan for IVC filter placement was made.
• His course was further complicated with development of HCAP.
• Antibiotic was changed from Piperacillin/Tazobactam to Meropenem and Vancomycin.
• Both his complicated UTI and HCAP responded well to the above antibiotics.
MICU Course

• His sepsis and AKI resolved and he was subsequently transferred to the floors on 4/20 for further management after being in MICU for 5 days.
• He underwent IVC filter placement on 4/22 without complication.
• While on the medicine floors, he developed acute onset shortness of breath with flash pulmonary edema that responded to furosemide.
• Tests showed troponin elevation but without any interval EKG changes.
• CCU was consulted and patient was transferred to CCU.
MICU/CCU Course

He was treated for NSTEMI and started on ASA, Clopidogrel, Atorvastatin,
Metoprlol, Lisinopril and Furosemide.
Troponins trended down, EKG remained without interval changes.
Echo showed LVEF 50-55% with borderline hypokinesis basal-anteroseptal wall and
moderate pulmonary HTN (no wall motion abnormalities present on prior ECHO).
The plan was for nuclear stress test however patient was uncooperative.
CCU Course

He was continued on treatment for HCAP/UTI as per ID recommendations to
complete 14 days of meropenem and vancomycin (urine and blood cultures
were negative).
GU was following the patient due to BPH requiring chronic foley.
Psychiatry was consulted to evaluate frequent agitation, determined him not
to be capacitated with recommendation for risperidone 1 mg qhs.
The patient was deemed stable for transfer to the floor.
CCU Course

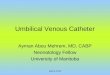
1. Schematic zones for catheter tip positioning can be categorized into three zones.
2. Zone A represents the lower SVC and upper RA.
3. In this zone CVCs placed from the left side are likely to lie parallel to the vessel walls.
4. This may represent a necessary compromise for left-sided CVCs to ensure that they lie parallel to the vessel wall.
5. Right-sided CVCs in this zone, however, should be pulled back to zone B.
6. Zone B represents the area around the junction of the left and right innominate veins and the upper SVC.
7. This is a suitable area for CVCs placed from the right side; however, left-sided CVCs will enter this area at a steep angle and are at risk of abutting the lateral wall of the SVC and should ideally be advanced into zone A.
8. Zone C represents the left innominate vein proximal to the SVC. CVCs in zone C are probably suitable for short-term fluid therapy and CVP monitoring, but not for inotrope infusions or long-term use. The safety of this site has been questioned.
Schematic zones for catheter tip positioning

Location Advantage Disadvantage
Internal Jugular
• Bleeding can be recognized and controlled• Malposition is rare• Less risk of pneumothorax
• Risk of carotid artery puncture• PTX possible
Femoral • Easy to find vein• No risk of pneumothorax• Preferred site for emergencies and CPR• Fewer bad complications
• Highest risk of infection• Risk of DVT• Not good for ambulatory patients
Subclavian • Most comfortable for conscious patients
• Highest risk of PTX, should not do on intubated pts•Vein is non-compressible

1. Most often premature atrial or ventricular contractions are reported during subclavian or IJ CVC insertion.
2. They are typically short lived, resulting from the guide wire touching the endocardium, and resolve when the tip is pulled out.
3. Most common cardiac conduction abnormalities are right bundle branch blocks, new left anterior and posterior fascicular blocks, and rarely asystole.
4. The cause of these conduction problems is also overzealous advancement of the guide wire.
5. The ease with which a right bundle branch block can be induced is probably related to the bundle branch's superficial position in the right ventricular endocardium, just inferior to the tricuspid valve.
6. Conduction abnormalities are usually transient and may go unnoticed.
7. However, in a patient with an underlying left bundle branch block, the induction of further conduction defects may lead to a life-threatening complete heart block requiring temporary pacing.
8. The mentioned arrhythmias and conduction problems are essentially avoidable during central venous catheterization since placement should not involve entry into the heart by the guide wire or by the subsequently placed catheter.
Cardiac dysrhythmias

Most common site of DVT for centrally placed catheters is the internal jugular vein.
For PICC catheters, the brachial, axillary, or subclavian veins may be involved.
Risk factors for thrombosis:
1. use of central vs peripherally inserted central catheters (PICCs-cancer, recent surgery, prior h/o DVT)
2. previous history of deep vein thrombosis
3. subclavian venipuncture insertion site
4. improper positioning of the catheter tip
5. Prothrombotic states
6. For a vein of similar size, thrombosis is more likely with a large-diameter, centrally-placed catheter (eg, plasmapheresis, dialysis, multilumen catheters) compared with a small-diameter catheter (eg, single lumen).
Catheter related thrombosis

Clinical prediction score
• Presence of a catheter or access device in a subclavian or jugular vein or a pacemaker (plus 1 point)
• Unilateral pitting edema (plus 1 point)
• Presence of localized pain in that extremity (plus 1 point)
• Another diagnosis at least as plausible (minus 1 point)
Total scores are rated as
• low probability (zero points or less, prevalence of upper extremity DVT 9 to 13 percent)
• intermediate probability (one point, prevalence 20 to 38 percent)
• high probability (2 to 3 points, prevalence 64 to 70 percent).
Catheter related thrombosis

• In patients with acute upper-extremity DVT (UEDVT) that involves the axillary or more proximal veins, acute treatment with parenteral anticoagulation (LMWH, fondaparinux, IV UFH, or SC UFH) over no such acute treatment is recommended.
• A minimum duration of anticoagulation of 3 months is suggested.
• The catheter should not be removed if it is functional and there is an ongoing need for it.
• In cases where the catheter is removed, 3 months of anticoagulation is recommended for both patients with cancer and with no cancer.
• In patients where the catheter is not removed, anticoagulation should be continued as long as the central venous catheter remains in patients with cancer and with no cancer.
Catheter related thrombosis

• Incidence of venous air embolism is 0.13% during the insertion and removal of central venous catheters despite using optimal positioning and techniques.
• Physiologic effects of venous air embolism are similar to that of pulmonary embolism (1) elevated pulmonary artery and right ventricular pressures; (2) increased ventilation/perfusion mismatch; (3) intrapulmonary shunting; and (4) increased alveolar dead space.
• The lethal dose for humans has been theorized to be 3-5 ml/kg.
• Furthermore, the rate of accumulation and patient position also contribute to the lethality.
• Air infusion rates of more than 1.5 ml/kg/min are associated with bradycardia and cardiovascular decompensation.
• Treatment may prove futile if the air bolus is larger than 50 ml.
Vascular air embolism

• If a patient is conscious during the event, chest pain, dyspnea, headache, and confusion can all be symptoms of air emboli.
• EKG changes include ST depression and right heart strain due to pulmonary artery obstruction.
• Furthermore, clinical signs of right heart failure and decreased cardiac filling can result in jugular venous distention and pulmonary edema.
• If the embolus is severe, cardiac ischemia, arrhythmias, hypotension, and cardiac arrest can ensue.
• If embolization occurs to the cerebral arteries patients can have symptoms of confusion, seizure, transient ischemic attack, and stroke.
• When air goes to left ventricle and the aorta, it can occlude any of the peripheral arteries and cause ischemia.
Vascular air embolism

• A “millwheel” murmur can be auscultated by a precordial or esophageal stethoscope.
• If a patient is intubated, an abrupt decrease in the end-tidal carbon dioxide levels, demonstrated by capnometry is concerning for a change in the relation between ventilation and perfusion due to the obstruction of the pulmonary arteries.
• A massive air embolus can be seen occasionally on CXR.
• Doppler ultrasonography is a sensitive and practical means of detecting intracardiac air.
• An even more sensitive and definitive method for detecting intracardiac gas is transesophageal echocardiography.
Vascular air embolism

• If a venous air embolism is suspected, treatment includes stopping air entry into the system, aspiration of the air from the right ventricle if a central catheter is being used and placing the patient in Trendelenburg and left lateral decubitus position also known as Durant's maneuver.
• This positioning allows the entrapped air in the heart to be stabilized within the apex of the ventricle.
• Previous studies have shown that left lateral decubitus positioning may be effective by allowing air to move toward the right ventricular apex, thereby relieving the obstruction of the pulmonary outflow tract.
Vascular air embolism

• Adequate oxygenation up to 100 percent oxygen should be used.
• Supplemental oxygen reduces the size of the gas embolus by increasing the gradient for the egress of nitrogen from the bubble.
• Rapid resuscitation with volume expansion is recommended to elevate venous pressure, thus preventing the continued entry of gas into the venous circulation.
• Aspiration via a central venous line accessing the heart may decrease the volume of gas in the right side of the heart, and minimize the amount traversing into the pulmonary circulation.
• Subsequent recovery of intracardiac and intrapulmonary air may require open surgical or angiographic techniques.
Vascular air embolism

Summary
After 3-4 tries, let someone else try
Get chest x-ray after unsuccessful attempt
If attempt at one site fails, try new site on same side to avoid bilateral complications
Halt positive pressure ventilation as the needle penetrates the chest wall in subclavian approach
If you meet resistance while inserting the guide wire, withdraw slightly and rotate the wire and re-advance
Align the bevel with the syringe markings
Use the vein on the same side as the pneumothorax
Withdraw slowly, you will often hit the vein on the way out.