Embed Size (px)
DESCRIPTION
Citation preview

Emergencies of Childbirth
Daniel J. Bartgen7.27.2010

Who its happened to…• Indiana Community ER: 2-3 per month• Christ ER: 4 last yr• Edwards Hospital: 1 in past 6 yrs• Colleen Crowe: 2 in first yr
• Chicago paramedic: 1-2 per shift• ER doc volunteered 1 yr in Guatemala: 40-50
Complications encountered by attendings…Shoulder dystocia, nuchal cords, breech, footling breech,
perimortumc-sections, preemies, twins, retained placentas, cord prolapse

Statistics
– Prolapsed Cord: 0.6%– Post-partum hemorrhage: 3%– Nuchal cord: 20% 1 loop; 5% 2 loops– Shoulder dystocia: 0.6 – 1.4%– Breech presentation:• Term: 1-3%• 32 wks: 7%• <28 wks: 22%

ToolsFOR MOM• OB KIT
– Scissors– Hemostats– Towels/Drapes– Sterile gloves– Alcohol– Bulb suction
FOR BABY• Pediatric Airway Box• Pediatric Code Cart• Key things for baby
– ETT tube: • 3.5 if term• 3 if preemie
– Laryngoscope: • 0 if term• 00 if preemie
– Neonatal suction: respiratory takes care of this.

Key Questions…
• Term/Preterm/Post-dates?• G’s and P’s?• Previous complications?• Size of fetus? Diabetes?

Case 1: 20 yo G2P1, with diabetes, 42 wks pregnant, and her first baby was 9 lbs. Now fully
dilated and pushing…• Head delivers, then retracts tightly against the
perineum = the dreaded “turtle sign”• NOW WHAT?
A. PanicB. HideC. Drop out & apply
for dermatologyD. Be a Hero

Be a Hero
• CALL FOR HELP!• Stop Pushing!• McRoberts• Suprapubic CPR• Episiotomy?• Maneuvers• Roll patient• Last ditch efforts– Clavicle Fracture– Symphysiotomy

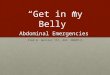
McRoberts&Suprapubic CPR

Episiotomy?• Provides extra hand
room for maneuvering.• Does not help with the
body impaction.

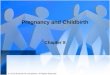
Maneuvers
1. Rubin II
2. Ruben II + Woods Corkscrew
3. Reverse Woods Corkscrew

Maneuvers
• Deliver Posterior Arm

Roll Patient
• Can increase outlet by 20mm.

Desperate Times Call for Desperate Measures(assuming no OB backup)
• Clavicle cracking time (just push on them)• Symphysiotomy– FOLEY– Betadine– Lido w/ epi– # 20 or 21 blade,
cut till it opens
• If OB backup, Zavanelli then OR

Questions on Case 1?

OB Blooper #1• Who was involved in the following conversation?– Doctor: So you are 30 wks pregnant?– Woman: No, my sister who is in the bathroom is 30 wks
pregnant, do I look pregnant?– Doctor: No, but this is awkward, so I’ll come back later.A: Dan Bartgen B: Jess Sinnot C: Vijay Menon D: Christian Badillo

Case Two – Cord Prolapse
• 22 yo female G1 at 34 wks, contractions q 5 min, and felt a gush of fluid immediately prior to arrival in ER.
• Cervix exam reveals 6cm dilation and a prolapsed umbilical cord.

Cord Prolapse - Who it happens to…
• Malpresenations• Prematurity• Abnormal fetus• Placenta previa
**THESE BABIES ARE SICKER****10-20% Perinatal mortality**

Cord Prolapse - What to do…• Relieve pressure• Gently place cord in vagina
- Cold air & rough handling causes spasms• Gently palpate cord for pulsations• Trendelenburg• Fill bladder• If pulsations, go to OR• No pulsations, deliver

Questions on Case 2
• ???????????????????????????????????????????????????????????????????????????????????????????????????????????????????????????????????????????????????????????????????????????????????????????????????????? ????????????????????????????????????????????????????????????????????????????????????????????????????????????????????????????????????????????????????????????????????????????????????????????????????????

OB Blooper # 2• Q: Which of the following residents attempted
to palpate the cervix though the rectum?A: Dan Bartgen B: JoEllenChannon C. Mark Hinton D: Big Party Riccardi

Last Case – Breech Delivery
• 24 yo female G1 at 32 wks, SROM, in labor.• Cervix is dilated to 7cm.• You palpate feet.
• What do you do?

Dangers
• Limb fractures• C-spine and brachial plexus injuries• Asphyxia
• Increased risk of cord prolapse prior to delivery• Delivery of head naturally compresses cord
**THESE BABIES ARE SICKER**

Go Slow• If not fully dilated, no pushing.• Once belly button shows, help
deliver legs– Hip flexion with external rotation– Keep slack on umbilical cord

Deliver Shoulders• Once scapulas show, help deliver arms– Sweep arms over chest– Rotating baby may help

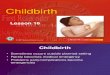
Delivering the Head• Deliver head (2-3 minute window)
– Mauriceau-Smellie-Veit maneuver– Suprapubicpresure

Decent Clip
• Pay attention to…• The good– Using a towel– Hooking the shoulders out– Hand position during head delivery
• The Bad– Didn’t use suprapubic pressure– Take your time, traction is bad
http://www.youtube.com/watch?v=DHF08AuLiUc

Questions on Case 3
?????

Take Home Points
• Expect the worst, be prepared.• Shoulder dystocia: Turtle sign. McRoberts and
suprapubic CPR is key. Lots of techniques, keep trying.
• Prolapsed cord: relieve pressure, check for pulsation, keep cord warm, get to OR.
• Breech delivery: relax, don’t pull. • The cervix is located in the vagina, not the
rectum.

Thanks

References
• Ouzounian JG, Korst LM, Ahn MO, et al. Shoulder dystocia and neonatal brain injury: significance of the head-shoulder interval. Am J ObstetGynecol 1998;178,S76
• Baskett, Thomas. Essential Management of Obstetric Emergencies. Clinical Press Limited, 2004.
• http://primary -surgery.org• Gabbe: Obstetrics: Normal and Problem Pregnancies, 5th
Ed.• Tintinelli, Judith. Emergency Medicine, A comprehensive
study guide. 6th Ed.