Embed Size (px)
Citation preview

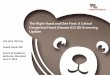
Embryology of upper limb
A bulge or limb bud on the ventrolateral wall of the embryo on day 26 (4-mm crown-to-rump length).
Also known as Wolff crest and lies opposite the 5 lower cervical and 2 upper thoracic segments

A thickening develops on the ventromedial border of the limb bud: the apical ectodermal ridge (AER) and is vital in axis orientation, outgrowth, and digitation
It covers a layer of undifferentiated,
proliferating mesenchymal cells 5-15 cells thick, known as the progress zone (PZ), essential in limb outgrowth.
The AER and PZ work as a functional unit responsible for the outgrowth of the limb along the proximodistal axis

The limb bud continues to grow outward from the ventral wall, and at day 32 it develops a somewhat flattened, paddle-shaped hand plate (8-mm crown-to-rump length).
During the fifth week, differentiating mesenchymal cells condense in a proximal-to-distal fashion to form blastemas, which eventually develop into cartilaginous models of, ultimately, the bones of the upper extremity.
At this time, nerve ingrowth from the rami of the spinal cord also occurs proximally. During the sixth week, hyaline cartilage models of the proximal bones of the extremity are formed.
Vessels : 3+1, br-med-uln-int-rad

In the seventh week, the upper extremity continues outgrowth and rotates 90° so that the elbows project posteriorly and the developing hands lie on the anterior thorax.
Cartilaginous models of the proximal bones are undergoing ossification
Mesenchymal cells derived from the dermomyotome condense within connective tissue (mesenchymal) scaffolds to form 2 common muscle masses. They are immediately penetrated by the spinal nerves. These dorsal and ventral common muscle masses split later to form the muscles of the extensor and flexor compartments, respectively.

Anatomically, the fetal period is signified by vascular penetration of the humerus
Most of the morphologic differentiation of the limb occurs during the embryonic period; the most critical period for the development of anomalies is from 24-36 days.

a brief timetable of hand development (modified from Tickle) Onset of development of arm bud - 27
days Well-developed arm bud - 28-30 days Elongation of arm bud - 34-36 days Formation of hand paddle - 34-38 days Onset of finger separation - 38-40 days Full separation of fingers - 50-52 days

Few out of so many…………..
Camptodactyly, syndactyly, and polydactyly are the most common abnormalities.
Assoc with 40, 38 and unkn no. of sydromes too.

Something about anomalies When 3 or more minor anomalies
exist in a single patient, the chance of the presence of a major anomaly is 90%
Developmentalists have designated the following 3 types of sequences: Malformation sequence Deformation sequence Disruption sequence

Only 5% of congenital hand anomalies occur as part of a recognized syndrome. Examples include the following:
Holt-Oram syndrome - Cardiac defects (atrial septal defect or ventriculoseptal defect) plus upper limb defects
VATER syndrome - Vertebral (defects), (imperforate) anus, tracheoesophageal (fistula), radial and renal (dysplasia)
Fanconi syndrome - Pancytopenia, preaxial limb defects, renal abnormalities, hyperpigmentation, short stature, microcephaly, or mental retardation
Nager syndrome - Preaxial aplasia associated with mandibulofacial dysostosis (Treacher Collins syndrome)
Roberts syndrome - Four deficient limbs plus cleft lip and palate

Classification: ASSH
Type I – Failure of formation: Transverse arrest Longitudinal arrest
Type II - Failure of differentiation Soft tissue - Syndactyly, trigger thumb, Poland
syndrome, camptodactyly Skeletal - Various synostoses and carpal coalitions Tumorous conditions - Include all vascular and
neurologic malformations Type III – Duplication: May apply to
whole limb, mirror hand, polydactyly

Type IV – Overgrowth: Includes conditions such as hemihypertrophy and macrodactyly
Type V – Undergrowth: Most commonly, radial hypoplasia, brachysyndactyly, or brachydactyly
Type VI - Constriction band syndromes: Streeter hypoplasia - Occurs with or without lymphedema; invs amputation at any level
Type VII - Generalized anomalies and syndromes
Unclassified [email protected]

Syndactyly : disorder of separation Defn : variable fusion of soft tissue/or
skeletal elements of adjacent fingers
Due to : failure of normal processes of digital separation and web space formation

Syndactyly is classified according to
completeness (complete, incomplete) presence of bony union (simple,
complex, complex-complicated).

Presentation
As Isolated Syndromic
Associated syndromes: poland (brachiocephalic -subclav
disruption) apert (FGFR2 acrocephalosyndactyly) Acrosyn(CRS)
Considerations for examination [email protected]

Management
Surgery Indications Contraindications
Principles of separation: from incision to splintage

Timing Order of release Commissure reconstruction Separation of digit Resurfacing of digit Paronychial fold

Early surgery is defined as that performed within the first 2 years of life
Advantages
Disadvantages

Polydactyly : disorder of duplication They are
Radial Ulnar Central Mirror hand, etc
Old classification Preaxial/ postaxial Balanced/ unbalanced

Radial polydactyly
Difference in black and other populations
Classification : Iowa : 6+1, along a longitudinal level German : 10 levels of longitudinal axis and
also transverse axis Wassel :7 types Buck –Gramcko universal
Etiology Imbalance between AER and mesoderm Cell division and apoptosis

classification of Stelling (1963) and Turek (1967) Type I - Soft tissue attachment Type II - Bony articulation Type III - Ray duplication
When it occurs in isolation, postaxial polydactyly has a strong inheritance pattern (AD)
Preaxial polydactyly most often presents as triphalangeal thumb.

Presentation
No two thumbs are alike Examine as per
Radial or ulnar partner Each digit : nail, soft tissue, joint, MC
head, its collateral ligaments, web space configuration, CMC joint, carpals

Other types
Central Ulnar Mirror hand Triphalangeal thumb Are less common than radial
polydactyly.

Treatment
Primarily surgical The principle of surgical treatment is to ablate
the most useless digit and to reconstruct it. Correction of type III deformities involves a
ray resection. Complex central reduplications require
individualized treatment. Conversion to a 3-finger hand may be the
best option in some patients.

Failure of differentiation Types
Congenital / Non-Congenital Sporadic / AD familial
Flexion extension imbalance is caused by Abnormal intrinsic muscle
anatomy:lumbrical insertion Other contributing factors

Presentation & Diagnosis
Age Deformity Order of frequency of occurrence Range of contractures Diagnosis-clinical/radiological D/D: DC, absent ext tendon,trigger

CRS
Type of transverse deficiency Digit absent and proximal support str
are present to some degree Various eponyms used Incidence: 1:3000 to 1:15000 Depends on environ / genetic factors

Associated malformations in 40 to 80% 2 types:
Am Def Adh Mut complex : wuth craniofacial
Am band disrup complex: only limbs Caused due to
Defective germ plasm Early rupture of amnion Intrauterine trauma

Classification Patterson’s
Presentation : Time As rings, grooves,multiple extr As congenital amputation /
acrosyndactyly D/D: cong amput , symbrachy, ADAM

Treatment
Timing : In utero/Neonatal/When child
walks/Complex procedures/Before School age
Principles of correction: Scar, digital length and jnt mobility,
growth, stump, web-space

Classification depends on Deviation of hand Thumb , phalanges and metacarpal size Radial carpals Ist web space Ulnar and median innervated muscles Pollex abductus

Classification
Type I : mild Type II : moderate Type III : severe, A,B,C Type IV : floating thumb(pouce flottant) Type V : absent(with and without
radius) Others :
Central defic CRS Five fingered hand Radial polydactyly Sydromic short skeletal thumb ray

Treatment
Timing : early vs late Principles
CMC jt MP jt stability 2/3 jt mobility Web space Motors for MP & IP jt Opposition

Management as per severity of situation
Consists of Z-plasties, local and distant flaps , tendon transfers, reconstruction of pulleys and eventually pollicisation

Pollicisation
Principles Racquet shaped incision Dissection of intrinsics & A1 pulley
decompression Skeletal shortening with metacarpal
osteotomy Tendon and intrinsic muscle rebalancing
& final positioning of thumb Broad web reconstruction and closure Diligent post-op regime

Some terms to know better…. Symbrachydactyly or atypical cleft
hand Symphalangism Brachysymphalangism Polysyndactyly or central polydactyly Wind blown hand Macrodactyly or gigantism