Embed Size (px)
Citation preview

Complications Of HDP
Dr. Shashwat Jani.M. S. ( Obs – Gyn )
Diploma in Advance Laparoscopy.
Consultant Assistant Professor,Smt. N.H.L. Municipal Medical College.
Sheth V. S. General Hospital , Ahmedabad.
Mobile : 99099 44160.E-mail : [email protected]

Introduction Giving birth should be a time for celebration,
but for more than half a million women each year—one every minute—pregnancy and childbirth end in death and mourning.
Six percent (approx. 1 in 16) of preeclamptic patients develop one or more major systemic complications .
Many maternal and fetal deaths or “near-misses” are associated with substandard care.
May 1, 2023 Dr Shashwat Jani. 9909944160. 2

HDP complicates 5 to 8% of all pregnancies.
This represents 8.5 million cases a year worldwide.
This pathology remains one of the three leading causes of maternal death.
The majority of these maternal deaths are related to cerebral hemorrhage that is secondary to poorly controlled hypertension.
May 1, 2023 Dr Shashwat Jani. 9909944160. 3

Objectives
Dr Shashwat Jani. 9909944160. 4
Understanding the complications of HDP Predictions and prevention of these
complications Early identification and appropriate
management Problem based learning .
May 1, 2023

Complications
Obstetric
Mother Fetus
May 1, 2023 Dr Shashwat Jani. 9909944160. 5

OVERVIEW
May 1, 2023 Dr Shashwat Jani. 9909944160. 6

Maternal
CNS• Seizures• Cerebral Edema• Cerebral Hemorrhage• Strokes (thrombosis)
Hepatic• Hepatic Failure• Hepatic Rupture• Subcapsular Hemorrhage
Heamatological• DIC• HELLP
Renal• Renal Failure• Oliguria• Proteinuria >> Hypoproteinemia (Glomerular
Injury)
Lungs• Pulmonary Edema
Fetal
Preterm Delivery
Stillbirth (IUFD)Intrapartum Fetal Distress
Placental Abruption
Uteroplacental Insufficency• Hypoxic Neurological Injury• IUGR• Oligohydraminos
May 1, 2023 Dr Shashwat Jani. 9909944160. 7

Obstetric
Increased risk for cesarean section
Placenta abruption
Premature labor
May 1, 2023 Dr Shashwat Jani. 9909944160. 8

COMPLICATIONS
Acute Future Pregnancy Late
Dynamics and incidence patterns of maternal complications in early-onset hypertension of pregnancy Ganzevoort W et al PETRA investigators. Obstet Gynecol. 2000 Jun;95(6 Pt 2):1017-9
May 1, 2023 Dr Shashwat Jani. 9909944160. 9

Acute Complications of HDP CNS Complications including eclampsia Acute Respiratory Failure HELLP Syndrome Uteroplacental Complications CVS Complications Acute Kidney Injury Hematological Complications Hepatic Complications
May 1, 2023 Dr Shashwat Jani. 9909944160. 10

CNS Complications
Dr Shashwat Jani. 9909944160. 11May 1, 2023

• Eclampsia is the most common, easily identifiable complication.
• Antepartum is the most common type (38-53%)intrapartum (18-36%)
postpartum (11-44%)• Atypical eclampsia
- < 20 weeks - Convulsions despite adequate MgSo4 . - 48 hours post partum (also called as late post
partum eclampsia)
May 1, 2023 Dr Shashwat Jani. 9909944160. 12

Intracranial hemorrhage Infarcts Cerebral edema PRES Blindness
SEIZURES
Focal neurological signs
Prolonged coma
Atypical or recurrent convulsions
Seizures even after delivery
May 1, 2023 Dr Shashwat Jani. 9909944160. 13

Posterior Reversible Encephalopathy Syndrome (PRES)
• A clinical neuroradiologic syndrome of heterogenous etiologies , that are grouped together because of similar findings on neuroimaging studies.
Dr Shashwat Jani. 9909944160. 14May 1, 2023

Pathophysiology
• Likely due to vasogenic edema secondary to an acute increase in arterial blood pressure, which overwhelms the autoregulatory capacity of the cerebral vasculature, causing arteriolar vasodilation and endothelial dysfunction, leading to extravasation of fluid (i.e preeclampsia) .
(Thackeray and Tielborg, 2007)
• OR an acute and significant episode of hypertension that causes cerebral vasoconstriction with subsequent ischemia and edema .
(Thackeray and Tielborg, 2007)
Dr Shashwat Jani. 9909944160. 15May 1, 2023

Autoregulatory failure
Normal autoregulation maintains constant cerebral blood flow over a range of systemic blood pressures .
When the upper limit is exceeded, the arterioles dilate, allowing breakdown of the blood-brain barrier, thus allowing extravasation of fluid and blood into the brain parenchyma.
Dr Shashwat Jani. 9909944160. 16May 1, 2023

PRES : Clinical manifestation and Etiopathogenesis• Postulations • Vasogenic cerebral oedema• ischaemia of brain tissue
• Posterior circulation – more susceptible – less sympathetic innervation
of the vertebro-basilar vasculature to protect the parenchyma from rapid increases in arterial blood pressure
Headache, nausea, vomiting Confusion, behavioral changes Changes of consciousness (from
somnolence to stupor) Vision disturbances (blurred vision,
hemianopia, cortical blindness) Epileptic manifestations (mostly
focal attacks with secondary generalization)
Mental functions are characterized with decreased activity and reactivity, confusion, loss of concentration and mild type of amnesia.
May 1, 2023 Dr Shashwat Jani. 9909944160. 17

Management Clinical symptoms and radiologic evidence
support the diagnosis . Should be recognized promptly so
treatment can be initiated In our patient population with
preeclampsia/eclampsia, this typically means delivery and treatment of Convulsions & Hypertension .
Dr Shashwat Jani. 9909944160. 18May 1, 2023

The immediate issues in caring for an eclamptic woman include …• Maintenance of maternal vital
functions, • Control of convulsions and blood
pressure, • Prevention of recurrent seizures, and
evaluation for delivery.
May 1, 2023 Dr Shashwat Jani. 9909944160. 19

Prognosis
Most cases of PRES are reversible in days to weeks with removal of the inciting factor and treatment of the blood pressure .
May 1, 2023 Dr Shashwat Jani. 9909944160. 20

ACUTE RESPIRATORY FAILURE / Pulmonary edema Pulmonary edema refers
to an excessive accumulation of fluid in the pulmonary interstitial and alveolar spaces.
It complicates around 0.05% of low-risk pregnancies but may develop in up to 2.9% of pregnancies complicated by preeclampsia.
May 1, 2023 Dr Shashwat Jani. 9909944160. 21

Only 30 % Antepartum
•Mainly,
- Post Partum,- Mulatiparity- Advance Maternal Age - Associated Medical Disorders
May 1, 2023 Dr Shashwat Jani. 9909944160. 22

DiagnosisDyspneaOrthopneaTachypneaAuditory crackles and ralesHypoxemia
ABGA, CHEST X RAY , ECG , CT SCAN , VQ SCAN May 1, 2023 Dr Shashwat Jani.
9909944160. 23

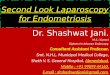
Pulmonary Edema ARDS Pleural Effusion
B/L Air bronchogramCentral bat wing patternRight side pleural effusion
Diffuse B/L Coalescent opacities
Left hemithoraxObliteration of right costophrenic angle.Mediastinal shift to right
May 1, 2023 Dr Shashwat Jani. 9909944160. 24

TreatmentOxygenPropped up positionI v lasixFluid restrictionInput – output chartingI v antibioticsIn refractory cases,Pulmonary artery catherisation and ventilation .May 1, 2023 Dr Shashwat Jani.
9909944160. 25

HELLP Syndrome• HELLP stands for: Hemolysis (abnormal smear), Elevated liver enzymes (serum SGOT >70 U/L
serum LDH >600 U/L, Low Platelets (< 100000)
6 % - one abnormalities 12 % - two abnormalities 10 % - three abnormalitiesMay 1, 2023 Dr Shashwat Jani.
9909944160. 26

Occurs in approximately 10% of pregnant women with pre-eclampsia or eclampsia.
One third of all cases of HELLP syndrome occur postpartum, and only 80% of such patients were diagnosed with preeclampsia before delivery.
May 1, 2023 Dr Shashwat Jani. 9909944160. 27

CAUSE :
It is thought to arise as a consequence of endothelial and microvascular injury, increased vascular tone and platelet aggregation.
May 1, 2023 Dr Shashwat Jani. 9909944160. 28

Spectrum of presentation Severity ranges from a mild and self-limited
course to a fulminant process leading to multiple organ failure.
In rare cases, occurs in normotensive pregnancy, only with epigastric pain and tenderness on palpation at the right hypochondrium as initial symptoms.
In most cases, resolves spontaneously within 48 hours of delivery.
Esan K, Moneim T, Page IJ. Postpartum HELLP syndrome after a normotensive pregnancy. Br J Gen Pract 1997;47:441−2.May 1, 2023 Dr Shashwat Jani.
9909944160. 29

HELLP post partum• Decreasing LDH and increasing PLT count
should be routinely observed on 4th postpartum day.
• Women not showing significant recovery should be suspected of TTP…- Normal coagulogram- Greatly elevated LDH 20,000 IU/L
- Neurological signs and symptoms
May 1, 2023 Dr Shashwat Jani. 9909944160. 30

Beware of Postpartum HELLP :
30% cases occur postpartum Majority within 48 hrs Risk of renal failure and pulmonary edema
is significantly increased compared to antenatal onset HELLP.
Clin Perinatol 2004,31:807-33Am J Obstet Gynecol 1993,168
May 1, 2023 Dr Shashwat Jani. 9909944160. 31

May 1, 2023 Dr Shashwat Jani. 9909944160. 32

Management Stabilization of pt. Rx of HTN Termination of pregnancy ( Depends on
Gest. Age & maternal condition ) Role of steroids ?????
With or without corticosteroids, the vast majority of women with HELLP syndrome will
recover within 96 hours of delivery. May 1, 2023 Dr Shashwat Jani.
9909944160. 33

FUTURE PREGNANCIES The reported risk of Recurrent HELLP
syndrome in a subsequent pregnancy ranges from 3% to 27%.
Future pregnancies are also at increased risk of other adverse events, including other manifestations of preeclampsia, preterm delivery, fetal growth restriction, placental abruption, and cesarean delivery.
The overall risk of such complications is 19–43%.
May 1, 2023 Dr Shashwat Jani. 9909944160. 34

Acute Kidney Injury AKI may occur in the context of severe
preeclampsia. In preeclampsia , due to the underlying
endothelial dysfunction the predominant abnormalities seen on renal histology are to the endothelium and glomeruli.
May 1, 2023 Dr Shashwat Jani. 9909944160. 35

Diagnostic Criteria : Creatinine clearance by measuring 24 hr urine creatinine remains the gold standard of GFR estimation in pregnancy.
Any Sustained Fall In Output < 0.5ml/Kg/Hr OR Rising Serum Creatinine Should Alert The Clinician Of Likelihood Of AKI.
May 1, 2023 Dr Shashwat Jani. 9909944160. 36

Management Supportive therapy includes blood
pressure control, positioning patients so as to improve renal blood flow, correcting fluid and electrolyte imbalance, and maintaining adequate nutrition.
If dialysis is required in pregnancy, hemodialysis is preferred over peritoneal dialysis.
May 1, 2023 Dr Shashwat Jani. 9909944160. 37

CVS COMPLICATIONSLow filling pressures and a hyperdynamic circulation• Cardiomyopathy Rare complication Treatment similar to other types of CCF HDP patient with pulmonary may wrongly labeled as a case of
peripartum cardiomyopathy. HTN CMP shows good recovery and regain cardiac function on follow up.
Acute MI Enhanced vascular reactivity to angiotensin II & norepinephrine
Endothelial dysfunction Decreased uterine perfusion leading to renin release Use of ergot alkaloids – Acute MI• Malignant Ventricular Arrhythmias 38

HEPATIC COMPLICATIONS Transaminases frequently elevated Epigastric/Subcostal pain (distension of liver
capsule by edema or subcapsular bleeding) Coagulopathy (high INR) Acute fatty liver Deficiency of the long chain 3-hydroxyacyl
coenzyme A dehydrogenase
Serum bilirubin - Important factor in predicting Maternal mortalityMay 1, 2023 Dr Shashwat Jani.
9909944160. 39

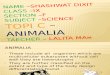
Jaundice High colored Urine
Liver Hematoma
Hepatic complications
May 1, 2023 Dr Shashwat Jani. 9909944160. 40

Liver Rupture / Hematoma• Mortality Is high.• First stabilize hemodynamically.• Then Exploratory Laparotomy with C.S.• Simple suturing is rarely effective because the entire
liver is edematous and friable and the hepatic parenchyma does not have the tensile strength to retain the sutures.
• Other surgical options include packing with gauze, topical coagulant agents or collagen fleeces coated with fibrin glue, incorporation of omental pedicles or surgical mesh into the liver, ligation of the hepatic artery, radiologic embolization of the hepatic artery, or hepatic lobectomy.
May 1, 2023 Dr Shashwat Jani. 9909944160. 41

Hematological Complications :
Hemolysis / Anemia
Bleeding as the incision is being closed & Incision site bleeding
Target cells, schistocytes & paucity of platelets
Associated with increased LDH
DIC
(In preeclampsia there is vasoconstriction which affects blood flow to the liver. Liver releases coagulation factors.)
May 1, 2023 Dr Shashwat Jani. 9909944160. 42

DIC• DIC is a hematologic disorder characterized
by a generalized increase in both fibrin formation and fibrinolysis, leading to excessive consumption of clotting factors, which presents clinically as a bleeding diathesis.
• The most common causes of DIC in pregnancy : are excessive blood loss with inadequate blood component replacement, placental abruption, amniotic fluid embolism, and severe preeclampsia / HELLP syndrome.
May 1, 2023 Dr Shashwat Jani. 9909944160. 43

Management Evidence of DIC in the setting of severe
preeclampsia / HELLP syndrome should prompt immediate delivery.
The decision of whether to proceed with induction of labor or cesarean delivery depends on such factors as gestational age, parity, cervical Bishop score, motivation of the patient, and the severity of DIC .
A rapidly falling platelet count may make cesarean delivery a more appropriate choice.
May 1, 2023 Dr Shashwat Jani. 9909944160. 44

Maintenance of intravascular volume and replacement of blood components and/or coagulation factors, as indicated by laboratory parameters.
May 1, 2023 Dr Shashwat Jani. 9909944160. 45

Ocular ManifestationsOcular involvement includes : Conjunctival vascular anomalies, Hypertensive retinopathy, Exudative retinal detachment, Vitreous and pre-retinal haemorrhages, Ischemic optic neuropathy , Hypertensive choroidopathy
May 1, 2023 Dr Shashwat Jani. 9909944160. 46

UTEROPLACENTAL COMPLICATIONSPLACENTAL ABRUPTION
BE ON GUARD
IUGR/ OLIGOHYDRAMNIOS
PRETERM DELIVERY (Iatrogenic)
May 1, 2023 Dr Shashwat Jani. 9909944160. 47

COMPLICATIONS DUE TO DRUGS Antihypertensive use : Maternal hypotension
& placental abruption Fluid overload and Betamimetics – pulmonary
edema Diuretics can cause pancreatitis especially in
patients with ARF Marcovici et al,Am J Perinatol 2002
Sublingual Nifedipine can lead to Sudden Hypotension & myocardial infarction and hence not to be used.
May 1, 2023 Dr Shashwat Jani. 9909944160. 48

Treatment :• Management of maternal hemodynamics &
prevention of eclampsia are key to a favorable outcome
• MgSO4 - Rx of choice for preeclampsia. • Goals
• Control BP• Prevent seizures• Deliver the fetus
May 1, 2023 Dr Shashwat Jani. 9909944160. 49

TAKE HOME MESSAGE Look for complications at Primary evaluation of
the patient. Ongoing risk assessment, continued surveillance
and interventions must be offered through comprehensive critical care.
Avoid Iatrogenic complications- drugs, fluids Tertiary care management and Multidisciplinary
Team approach.
May 1, 2023 Dr Shashwat Jani. 9909944160. 50

Thank you