Embed Size (px)
Citation preview
Developmental Dysplasia of the Hip
Dr. Arshad Shaikh
• Developmental dysplasia of the hip (DDH) is a spectrum of disorders:
Laxity of the hip capsule, with failure to maintain the femoral head within the acetabulum
Instability of the hip, such that the femoral head can be displaced partially (subluxated) or fully (dislocated) from the acetabulum
• Dislocation : is defined as complete displacement of a joint, with no contact between the original articular surfaces.
• Subluxation : is defined as displacement of a joint with some contact remaining between the articular surfaces.
• Dysplasia: is a radiographic finding of increased obliquity and loss of concavity of the acetabulum, with an intact Shenton's line
• Teratologic dislocation of the hip is a distinct form of hip dislocation that usually occurs with other disorders.
These hips are dislocated before birth, have limited range of motion, and are not reducible on examination
• Adolph Lorenz:
Traveled extensively and demonstrated his vigorous techniques of closed reduction of the hip. Because his reductions were so forceful, he has been called the “father of avascular necrosis”
Ortolani
• He saw a 5-month-old child whose mother had noted a “click” every time she washed the baby's bottom. The woman showed Ortolani how to reproduce it, and he found that the child had a dislocated hip when he took a radiograph. He published this experience in 1937 in an article entitled “A Very Little Known Sign and Its Importance in the Early Diagnosis of Congenital Hip Redislocation.”
Etiology
• Ligamentous laxity (often inherited) • Prenatal Positioning (especially footling)• Postnatal positioning (hips swaddled in
extension)• Primary acetabular dysplasia (unlikely)
Ligamentous laxity
• Newborn's response to maternal relaxin hormones may explain the higher incidence of DDH in girls
• These hormones, which produce ligamentous laxity necessary for expansion of the maternal pelvis, cross the placenta and induce laxity in the infant. This effect is much stronger in female than in male offspring
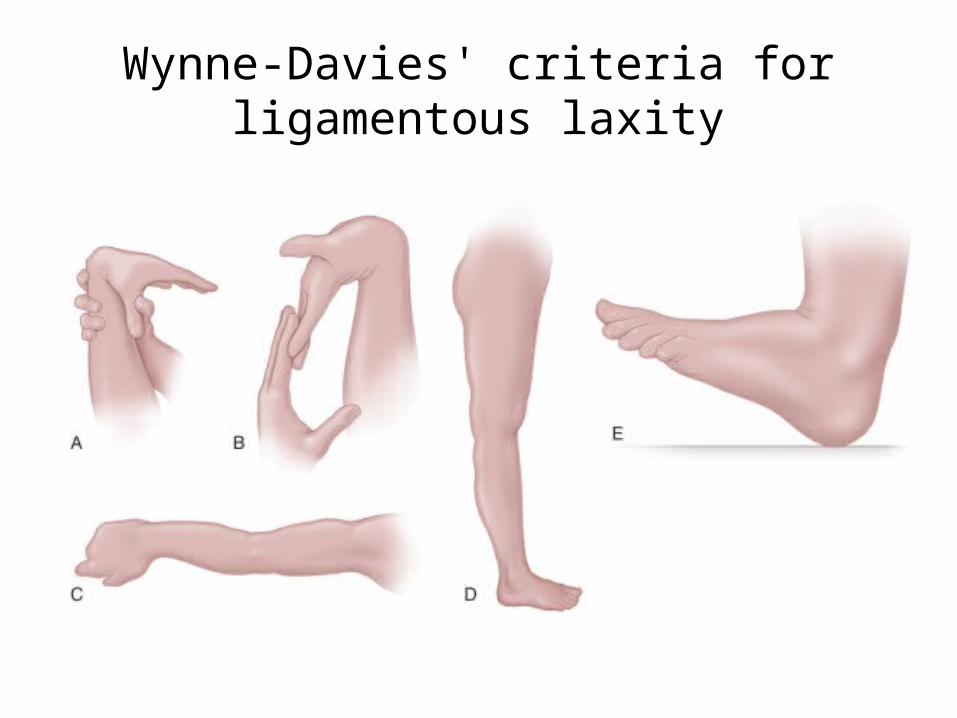
Wynne-Davies' criteria for ligamentous laxity
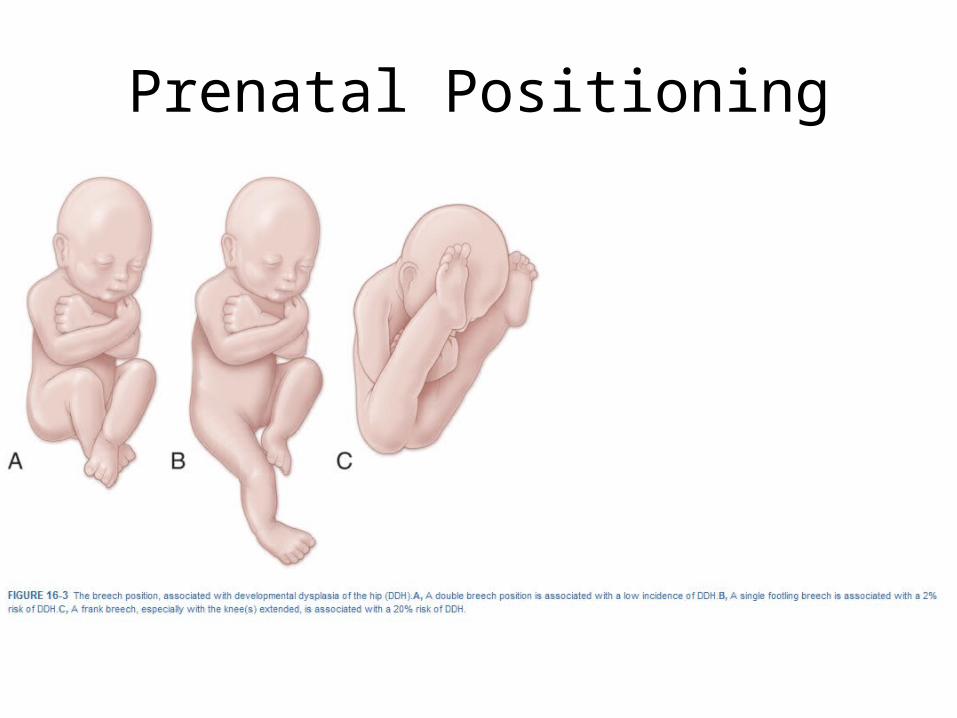
Prenatal Positioning
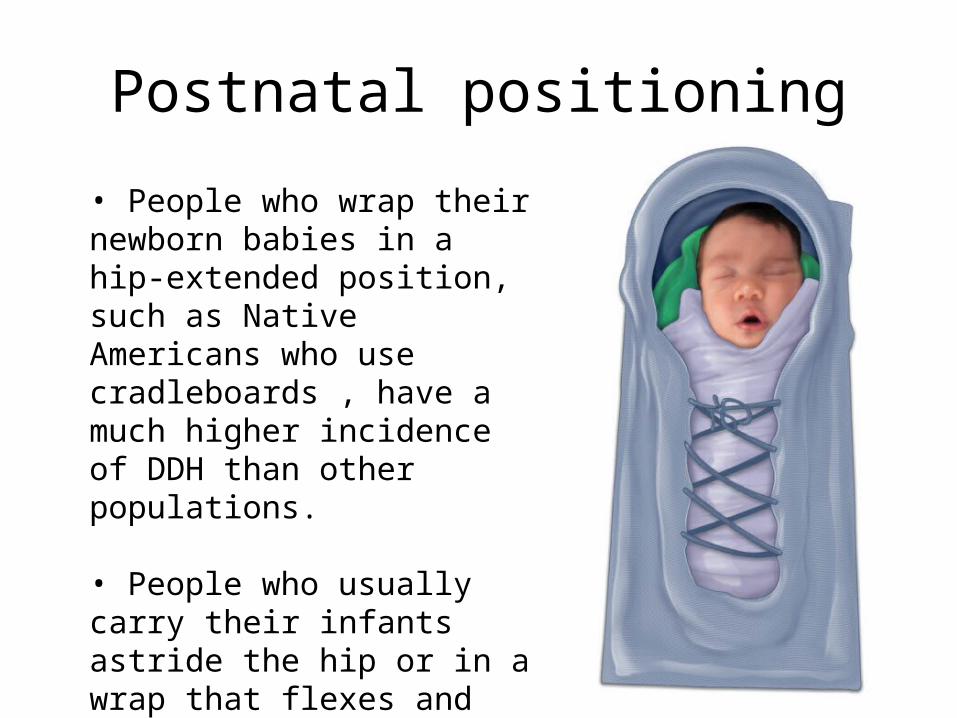
Postnatal positioning
• People who wrap their newborn babies in a hip-extended position, such as Native Americans who use cradleboards , have a much higher incidence of DDH than other populations.
• People who usually carry their infants astride the hip or in a wrap that flexes and abducts the hips have a lower incidence of DDH than other groups.
Primary acetabular dysplasia
• Acetabulum was more shallow at birth than in the earlier fetal period.
• ? May be a precursor of dislocation
Racial Predilection
• Blacks and Asians have relatively low incidences of DDH, whereas whites and Native Americans have a higher incidence.
Associated Conditions
• Torticollis (15%-20%) Strong association• Metatarsus adductus (1.5%-10%)• Oligohydramnios
Pathophysiology• Three acetabular epiphyseal centers develop and are responsible for
the Normal final contours of the hip socket:
The os acetabulum, which is the largest of the three, appears at about 8 years of age and forms along the anterior wall as part of the pubis.
The acetabular epiphysis, which also ossifies at around 8 years, forms along the superior edge of the acetabulum as part of the ilium and fuses at about 18 years
The third center is a small epiphysis in the posterior or ischial area, which develops at 9 years of age and fuses at 17 years.
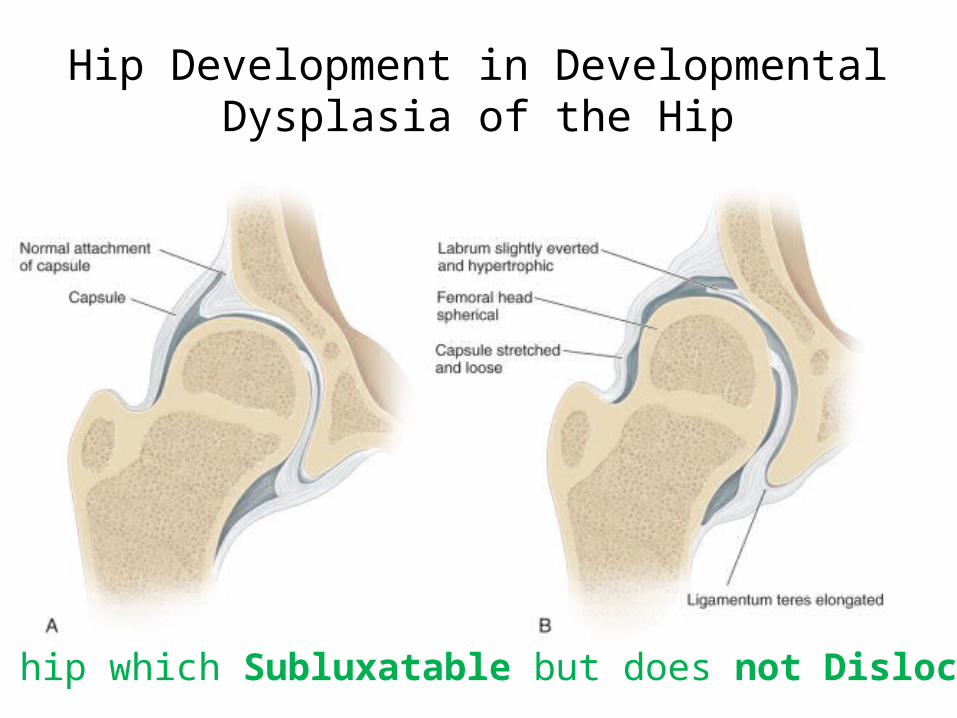
Hip Development in Developmental Dysplasia of the Hip
The hip which Subluxatable but does not Dislocatable
• Loose hyperelastic capsule, • Elongated ligamentum teres, • Slight eversion of the hypertrophied
acetabular rim (Labrum). • The femoral head is normal in shape.• Excessive femoral and acetabular antetorsion
may be present, causing anatomic instability of the hip joint.
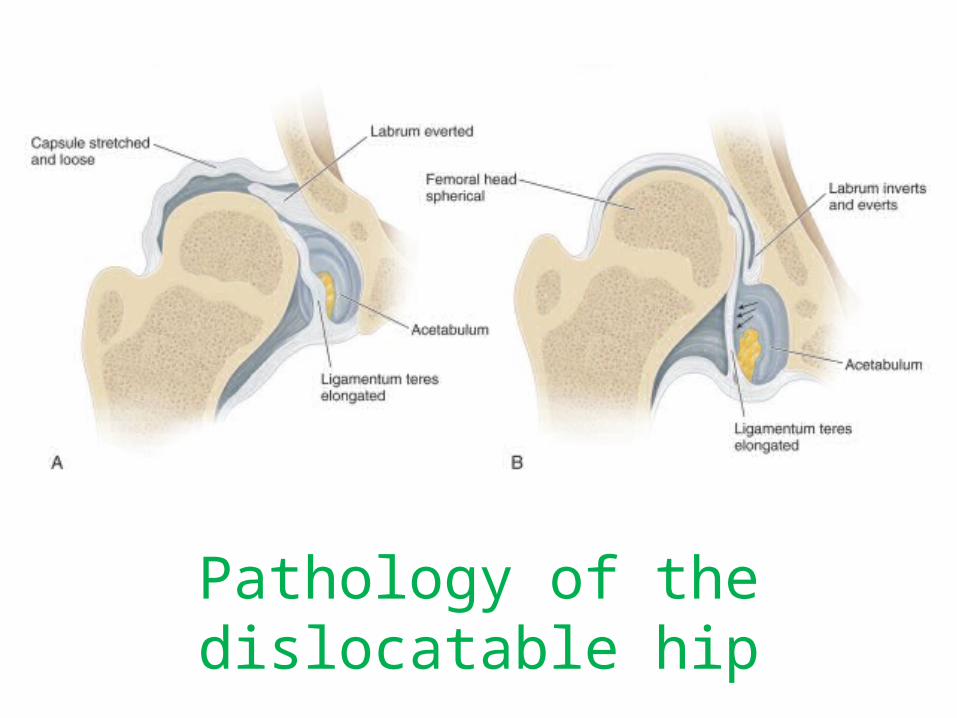
Pathology of the dislocatable hip
• The capsule is stretched out and very loose.• The ligamentum teres is markedly elongated. • The labrum is definitely everted. • Complete displacement of the femoral head out of the
acetabulum. • At the fibrocartilage-hyaline junction of the labrum with
the acetabulum, there may be inversional hypertrophic changes (neolimbus).
• The femoral head is spherical. Acetabular antetorsion is usually excessive.
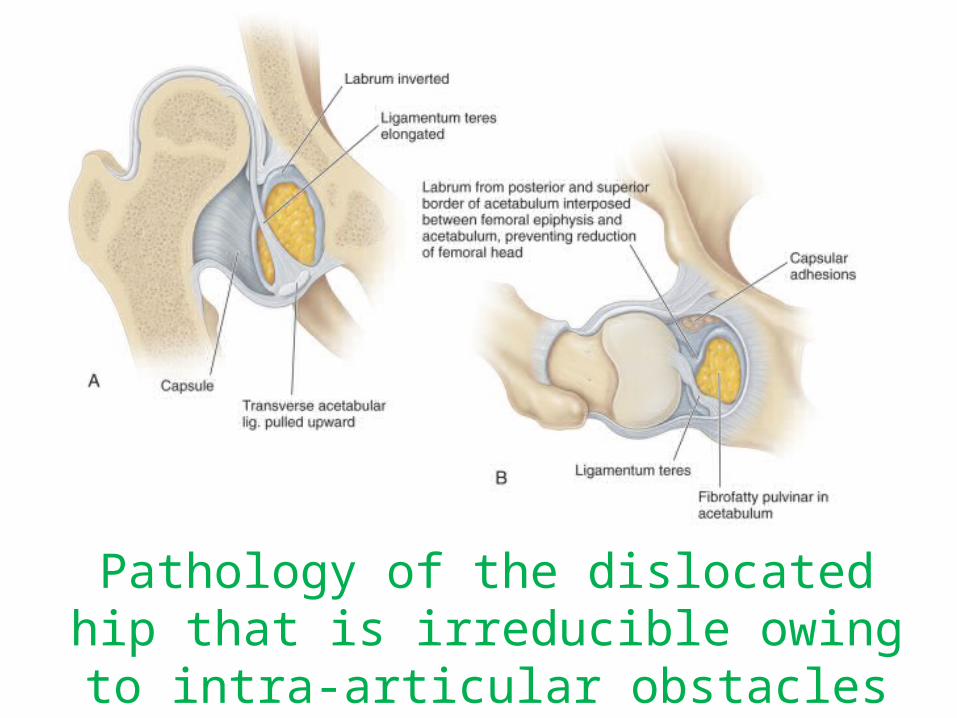
Pathology of the dislocated hip that is irreducible owing to intra-articular
obstacles
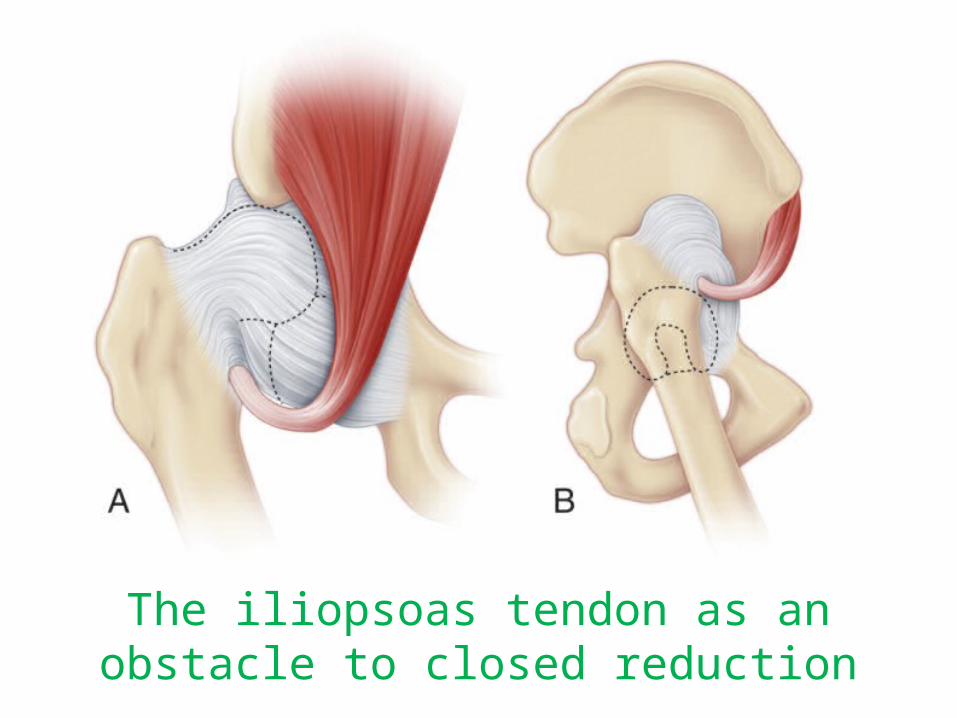
The iliopsoas tendon as an obstacle to closed reduction
Secondary barriers to reduction• Fatty tissue known as the pulvinar
• The ligamentum teres also elongates and thickens and may take up valuable space within the acetabulum
• The transverse acetabular ligament is often hypertrophic as well and may impede reduction
• External pressure and indentation of the capsule by the iliopsoas tendon. This hourglass constriction of the capsule with formation of the capsular isthmus markedly reduces the diameter of the acetabular orifice and is a barrier to closed reduction.
• Narrowing of capsule through a “Chinese finger-trap” mechanism.
• Femoral Head changes : Increase in anteversion and flattening of the medial aspect femoral head as it lies against the ilium.
Important Point
• Do not excise labrum only release of hip capsule during reduction of irreducible femoral head.
• Labrum is essential for normal development of acetabulum.
After the femoral head has been reduced
Gradual remodeling of Acetabulum
Acetabular angle gradually becomes more horizontal
Thickened cartilage will usually flatten out gradually and allow the head to seat deeply.
“Docking the head”
• Harris suggested that a hip reduced by 4 years of age could achieve “satisfactory” acetabular development. He found that significant acetabular growth continued through 8 years of age
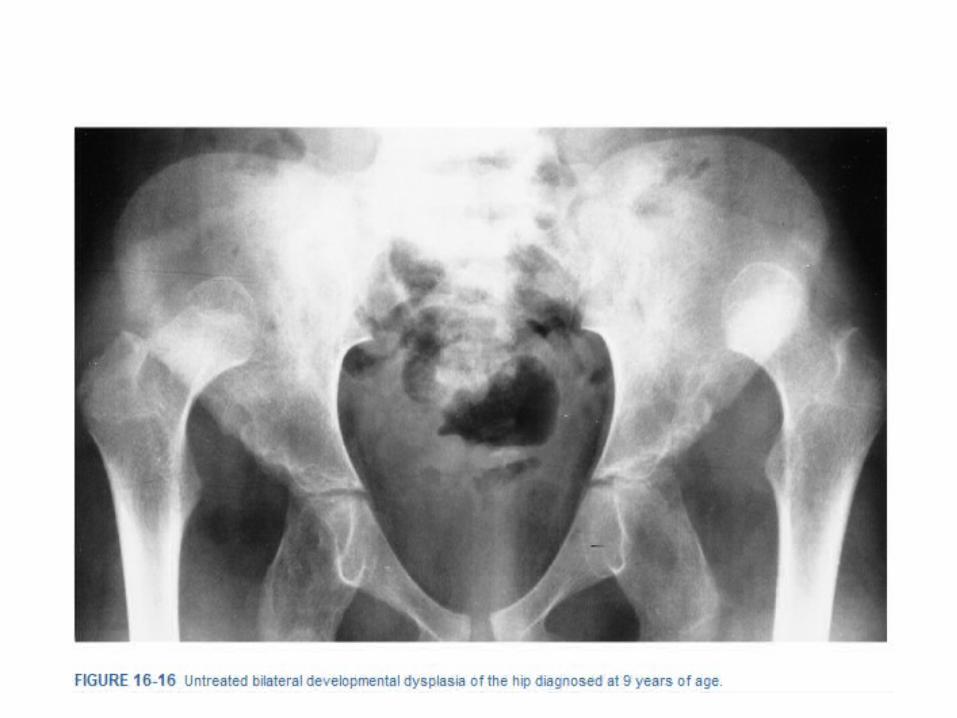
Untreated DDH
• High-riding dislocation: Fully dislocated femoral head may lie well above the acetabular margin in a markedly thickened hip capsule. Femoral head is oval and flattened medially Fully dislocated adult hips may remain free from degenerative changes for many years, even for the individual's lifetime.
Dysplasia, Subluxation, and Dislocation after the Neonatal Period
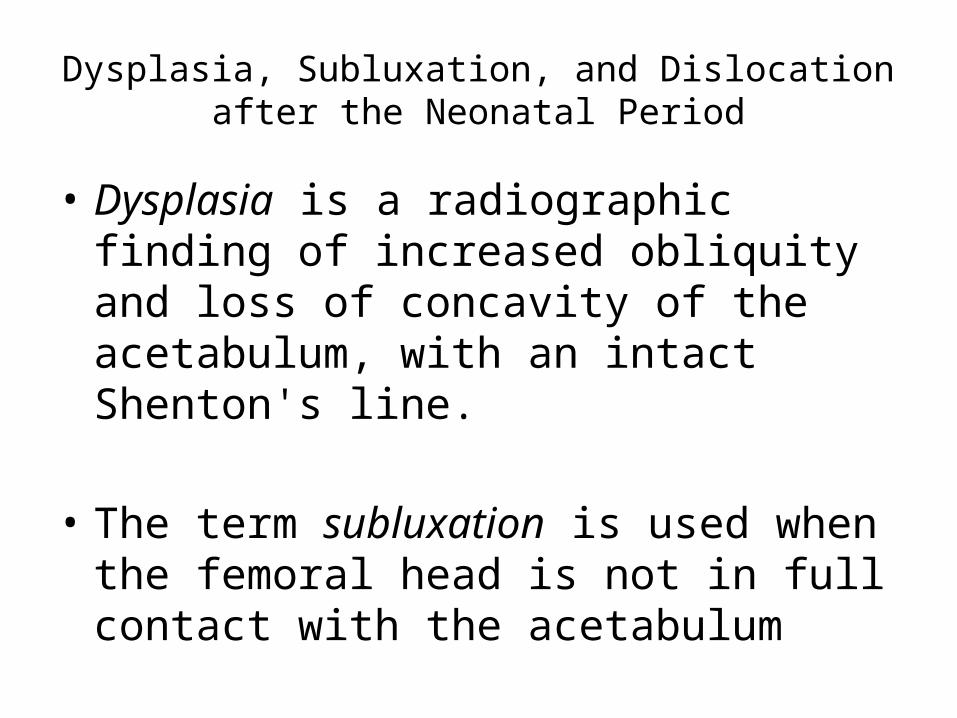
• Dysplasia is a radiographic finding of increased obliquity and loss of concavity of the acetabulum, with an intact Shenton's line.
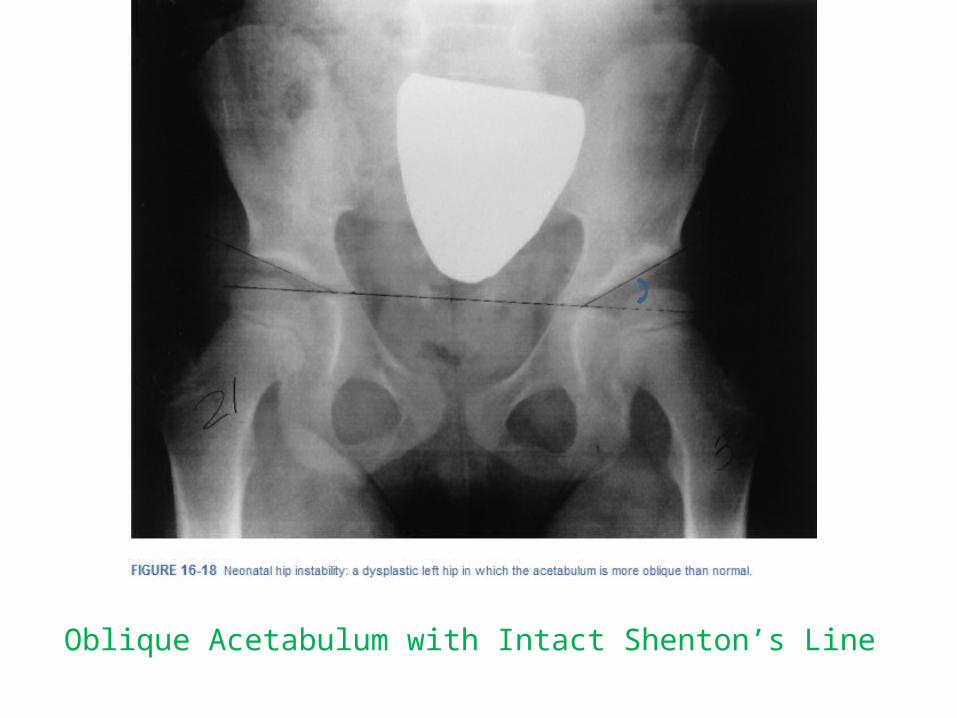
• The term subluxation is used when the femoral head is not in full contact with the acetabulum
Oblique Acetabulum with Intact Shenton’s Line
The Subluxated Hip• Widened teardrop-femoral head distance,
• Reduced center-edge angle, and• Break in Shenton's line
Complications of untreated DDH
• Degenerative hip disease – In Dysplastic & Subluxated hip
• Abductor lurch• Unilateral dislocations cause limb length inequality.• Ipsilateral valgus knee deformity• Decreased agility• Postural scoliosis• Bilateral cases are associated with significant back
pain secondary to increased lumbar lordosis
Clinical Features
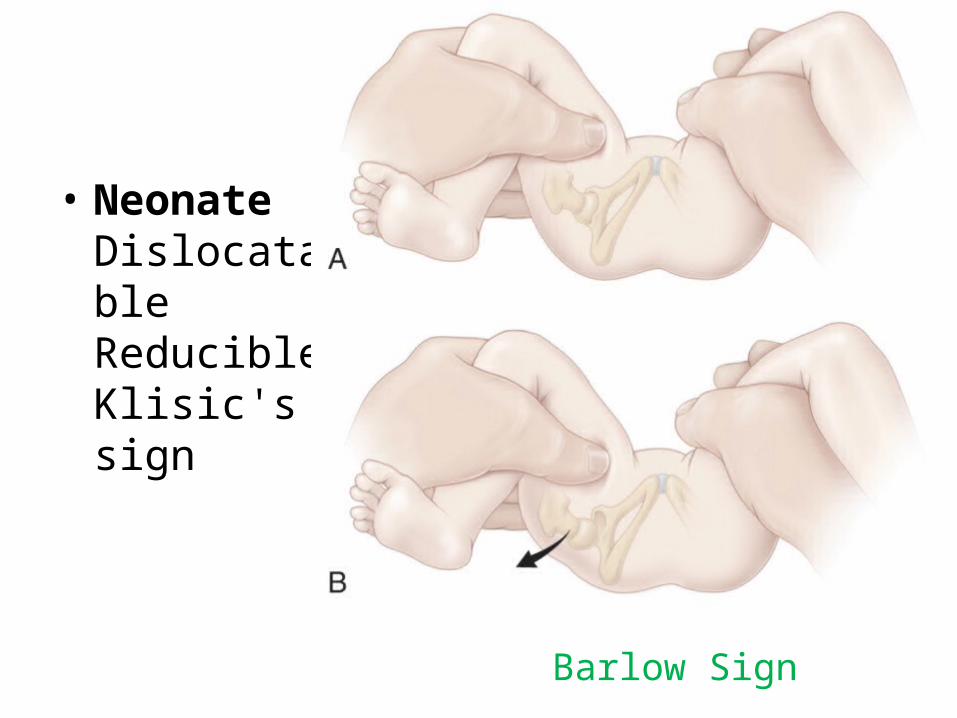
• Neonate DislocatableReducibleKlisic's sign
Barlow Sign
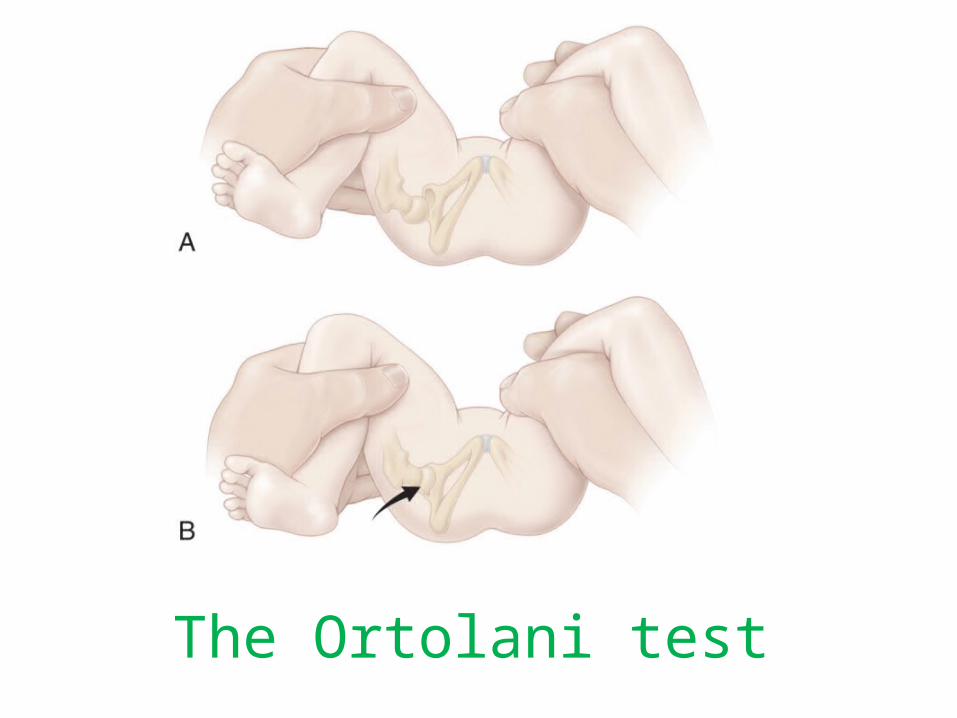
The Ortolani test
• It is possible to examine a hip for 15 maneuvers and feel the instability only the 16th time the hip is moved.
• Infant Dislocatable (occasionally) Reducible (occasionally) Klisic's sign Decreased abduction Galeazzi's sign (90 degrees of flexion) Proximal location of the greater trochanter, Pistoning of the hip. Asymmetry of thigh Folds
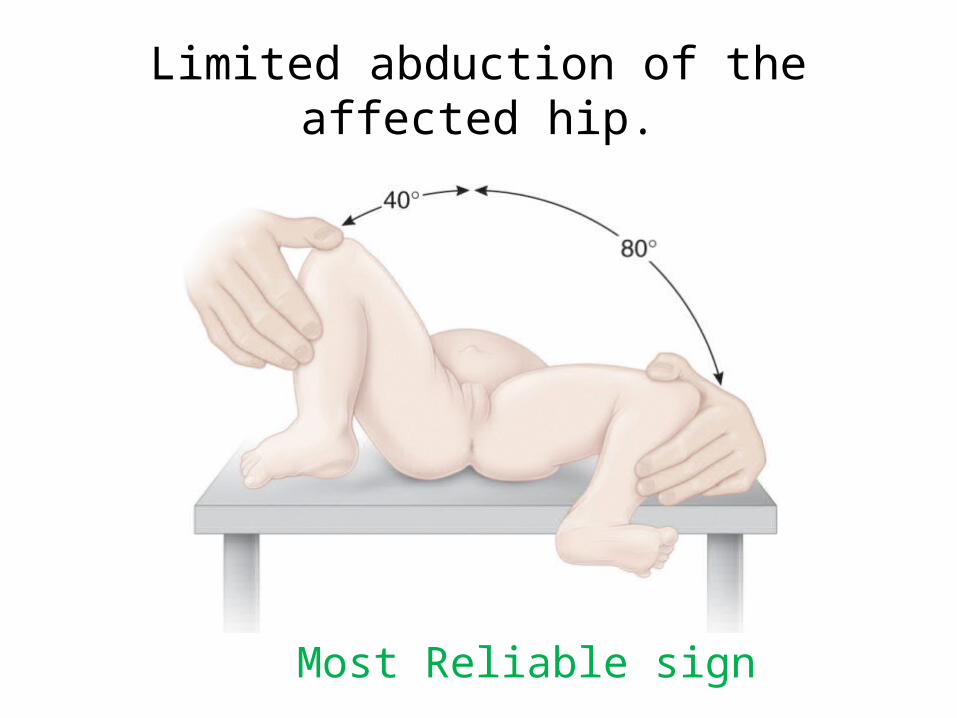
Limited abduction of the affected hip.
Most Reliable sign
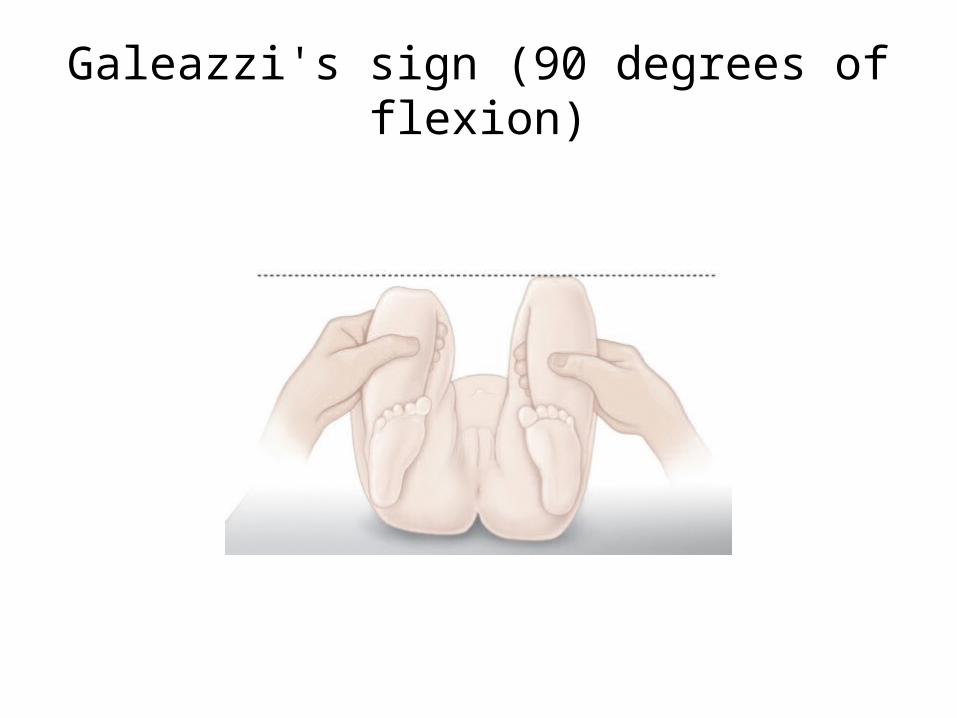
Galeazzi's sign (90 degrees of flexion)
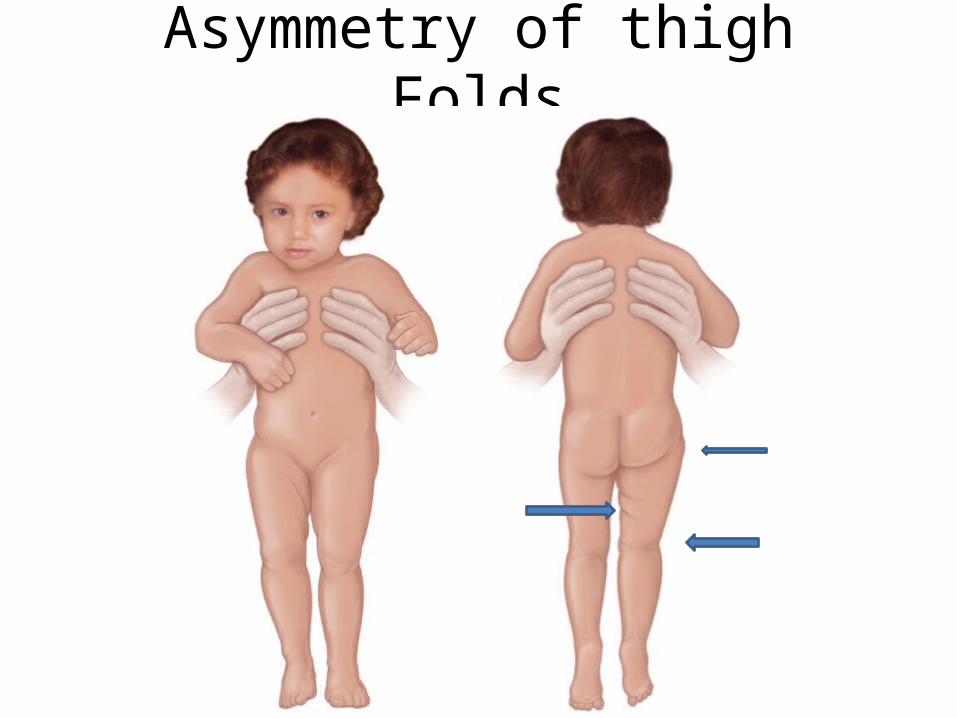
Asymmetry of thigh Folds
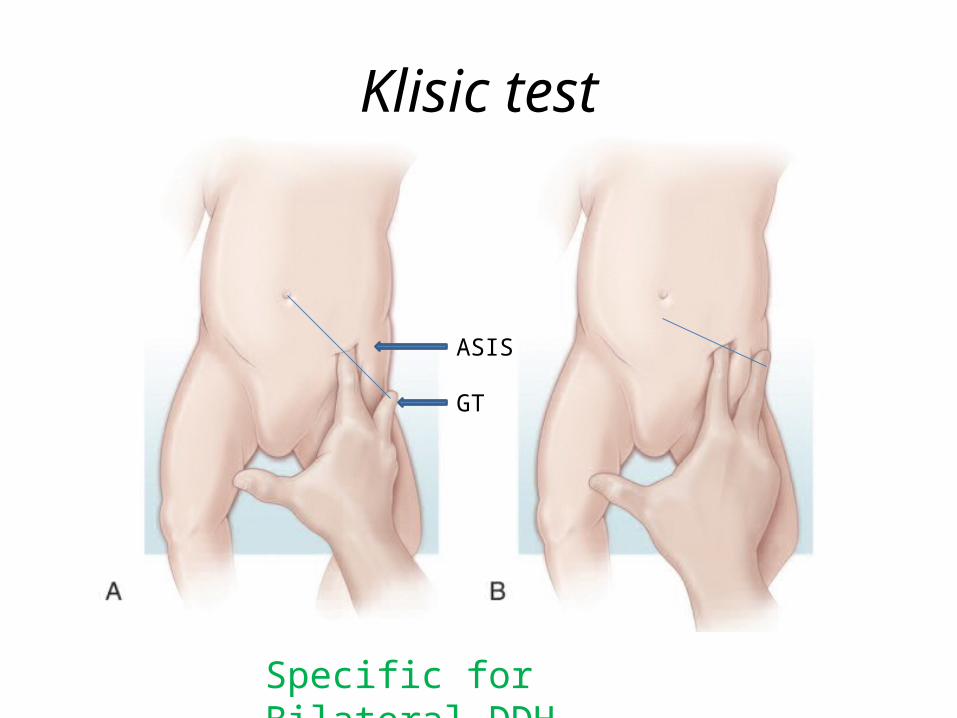
Klisic test
Specific for Bilateral DDH
GT
ASIS
Walking Child
• Remains dislocated Klisic's sign Decreased abduction Galeazzi's sign Limp Short leg Increased lordosis (bilateral) Trendelenburg's sign. There usually is excessive internal and external rotation of the dislocated hips
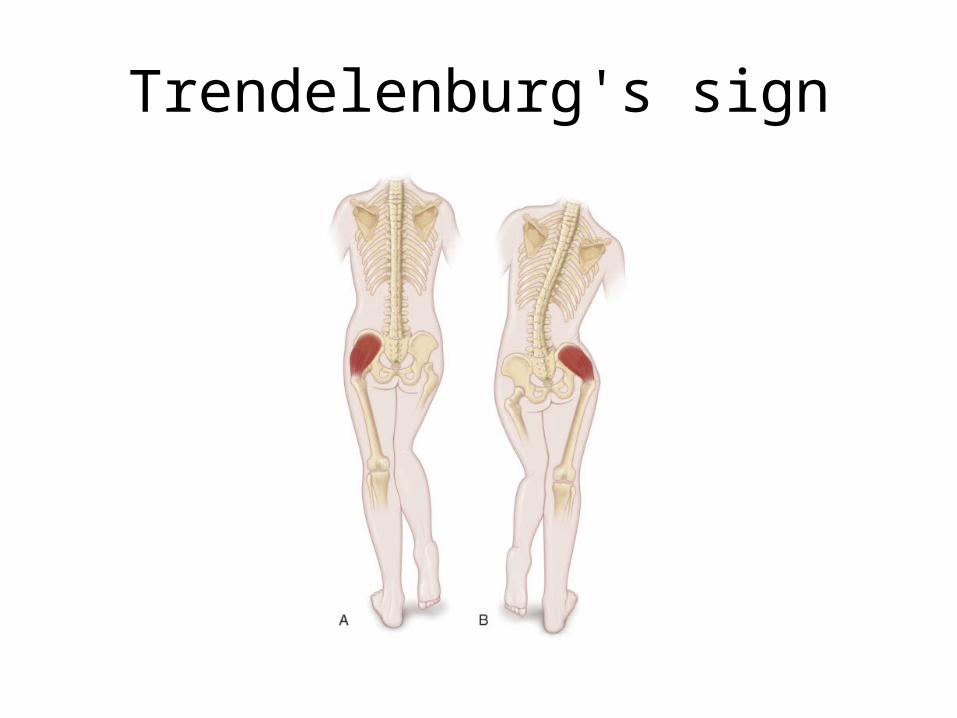
Trendelenburg's sign
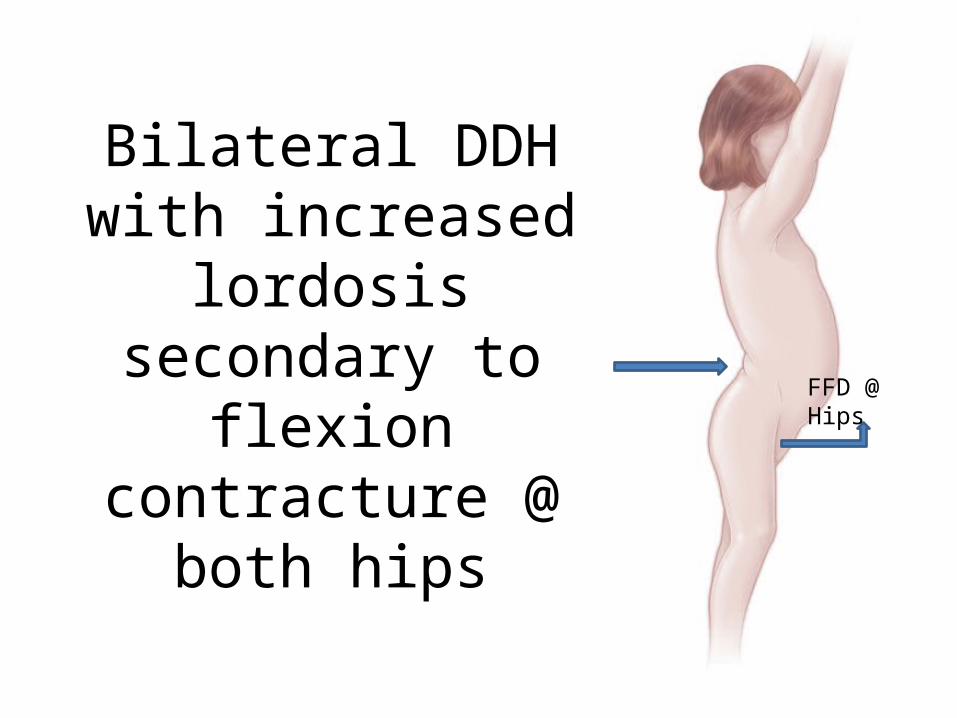
Bilateral DDH with increased lordosis
secondary to flexion contracture @ both
hips
FFD @ Hips
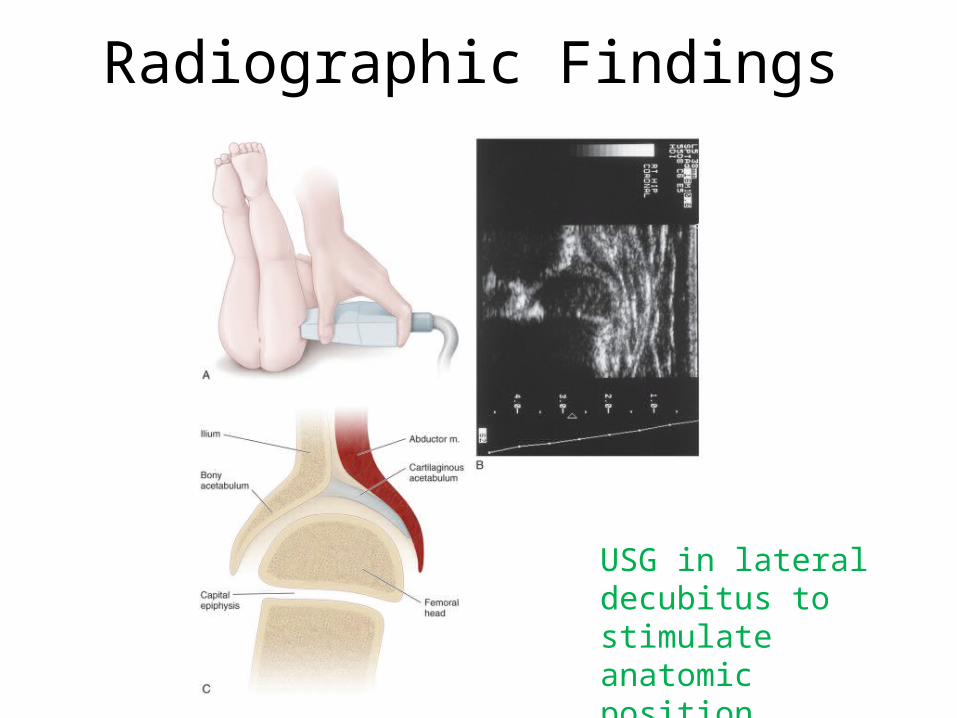
Radiographic Findings
USG in lateral decubitus to stimulate anatomic position
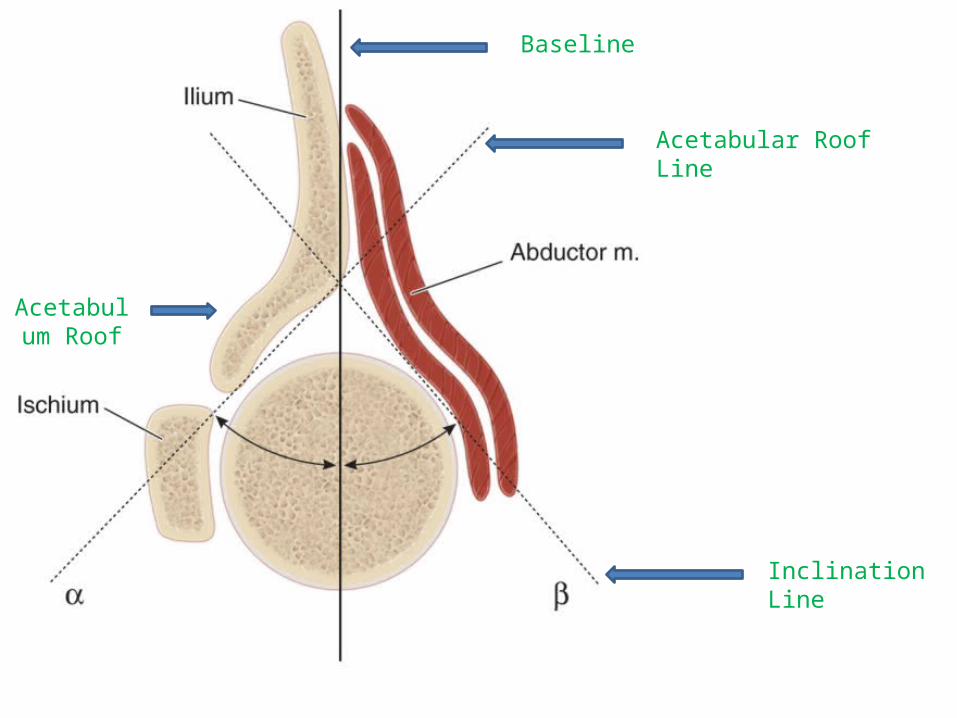
Baseline
Acetabular Roof Line
Inclination Line
Acetabulum Roof
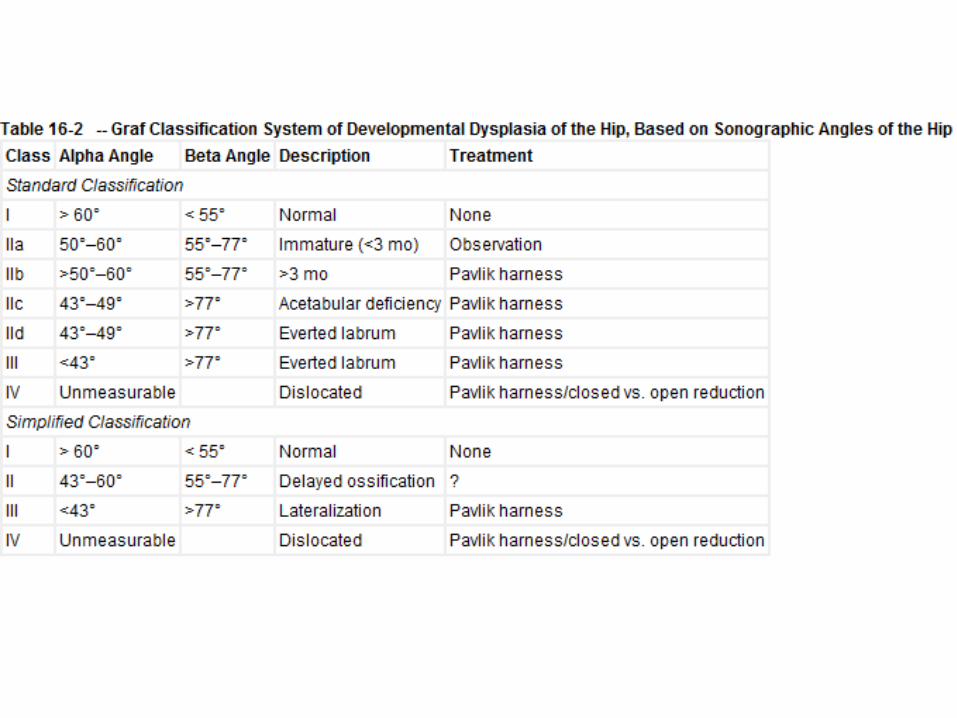
Graf Classification Based on USG
• Alpha Angle : Between Baseline & acetabulum roof line
• Beta Angle : Between Inclination line & Baseline• A smaller alpha angle indicates a shallower bony
acetabulum. A smaller beta angle indicates a better cartilaginous acetabulum.
• As the femoral head subluxates, the alpha angle decreases and the beta angle increases.
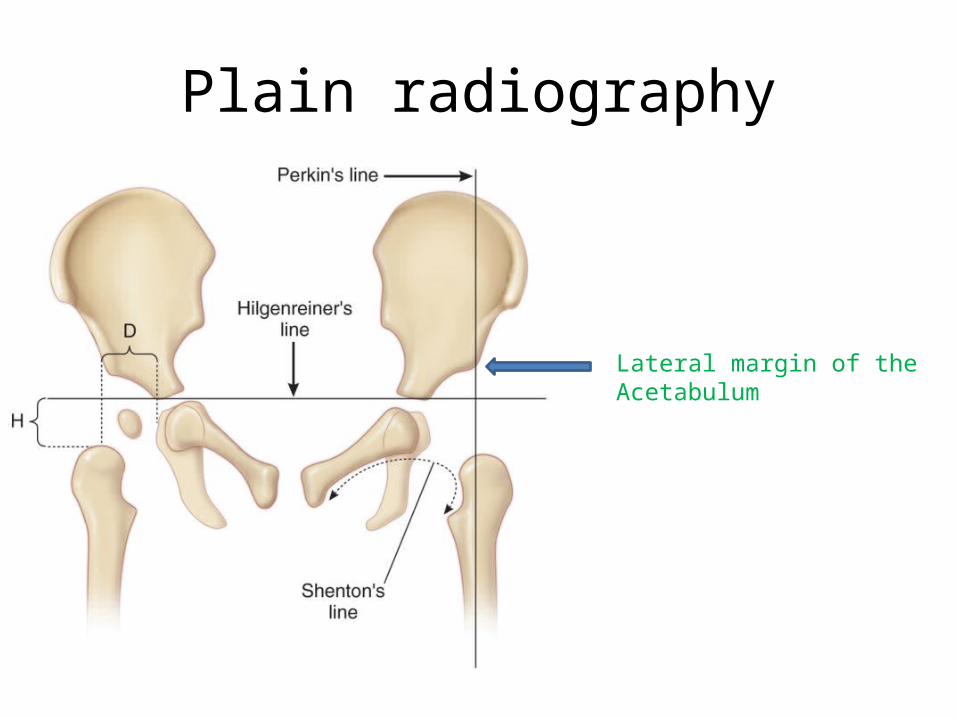
Plain radiography
Lateral margin of the Acetabulum
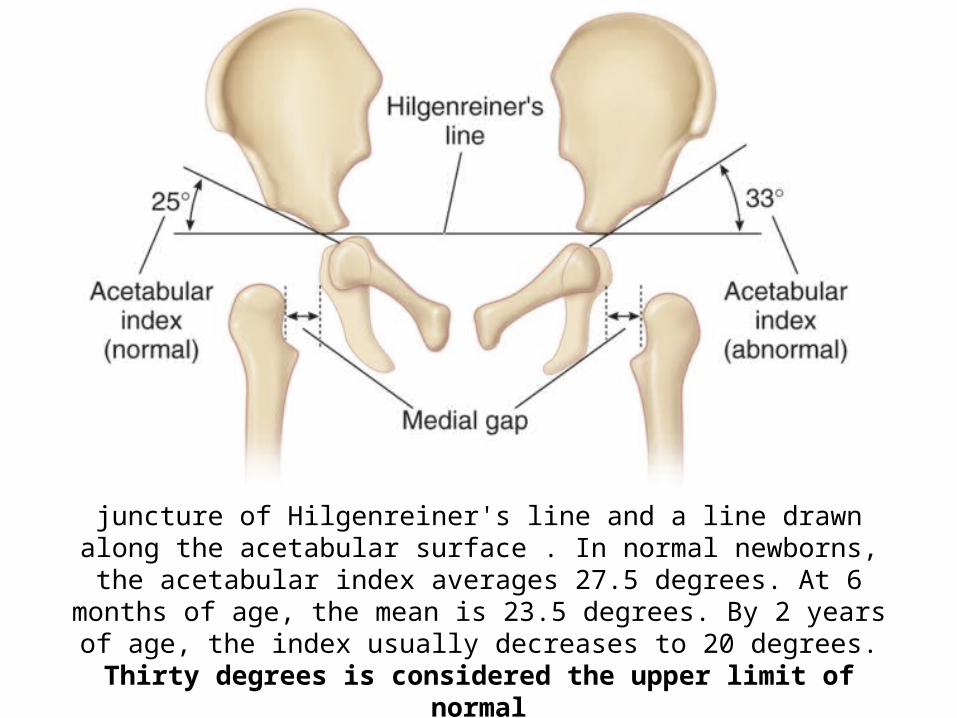
Acetabular index, which is an angle formed by the juncture of Hilgenreiner's line and a line drawn along the acetabular surface . In normal newborns, the acetabular index averages 27.5 degrees. At 6 months of age, the mean is 23.5 degrees. By 2 years of age, the index usually decreases to 20 degrees. Thirty
degrees is considered the upper limit of normal
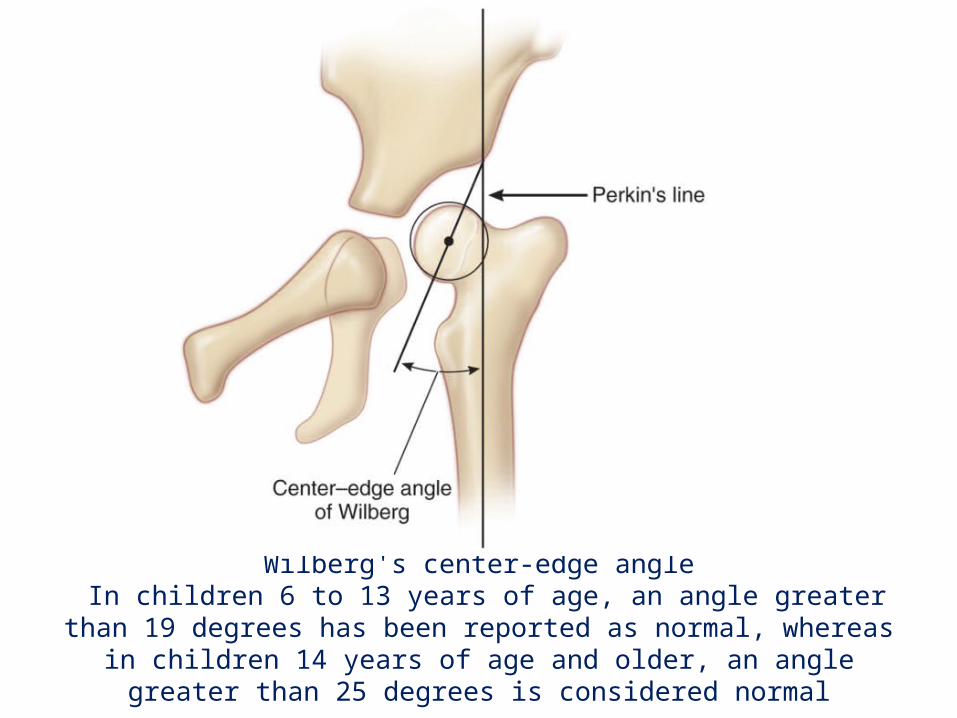
Wilberg's center-edge angle In children 6 to 13 years of age, an angle greater than 19 degrees has been reported as normal, whereas in children 14 years of age and older, an angle
greater than 25 degrees is considered normal
The acetabular teardrop• The teardrop appears between 6 and 24 months of age in a normal
hip, later in a dislocated hip.
• Dislocated or subluxated hip = the acetabular portion of the teardrop loses its convexity and the teardrop is wider from superior to inferior
• Hips in which the teardrop appears within 6 months of reduction have a better outcome than hips in which the teardrop appears later.
• The teardrops have also been described as U- or V-shaped, with a V-shaped teardrop being associated with dysplastic hips and a poor outcome
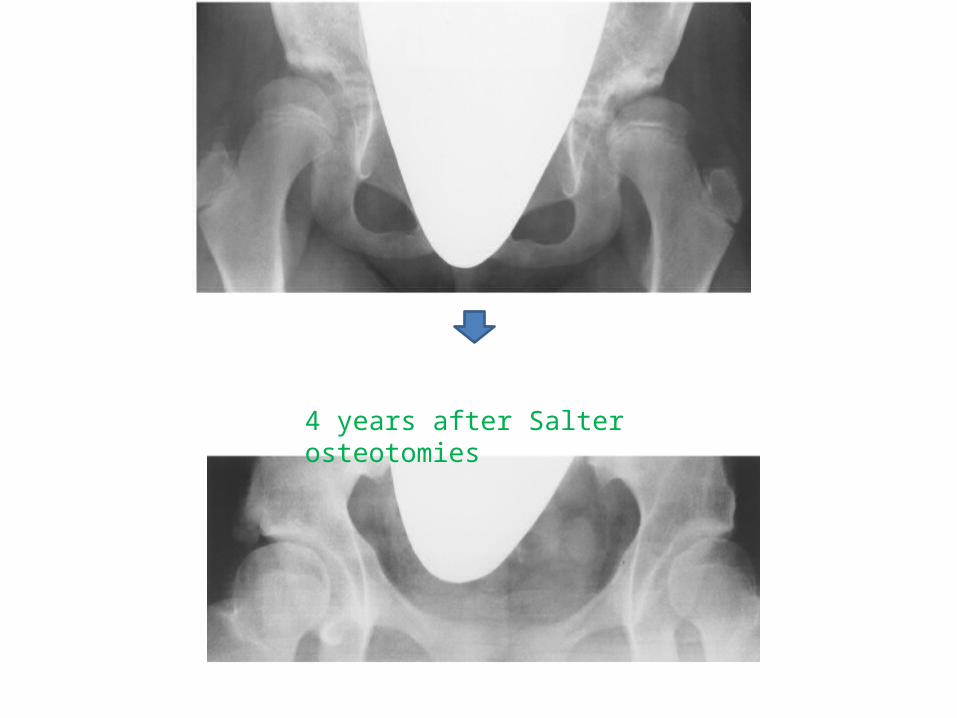
4 years after Salter osteotomies
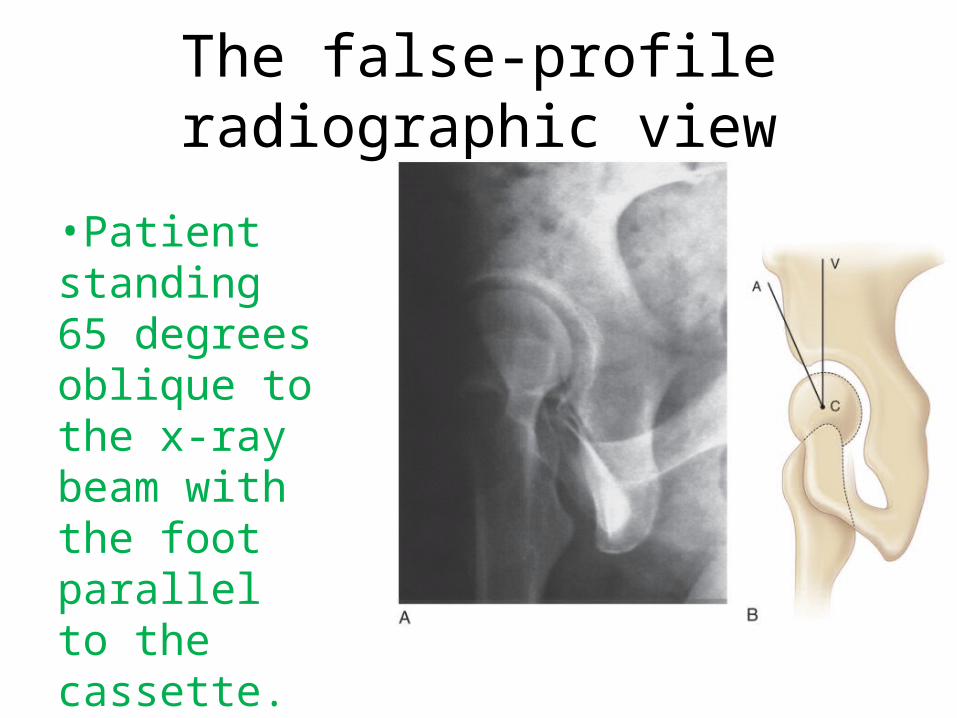
The false-profile radiographic view
•Patient standing 65 degrees oblique to the x-ray beam with the foot parallel to the cassette.
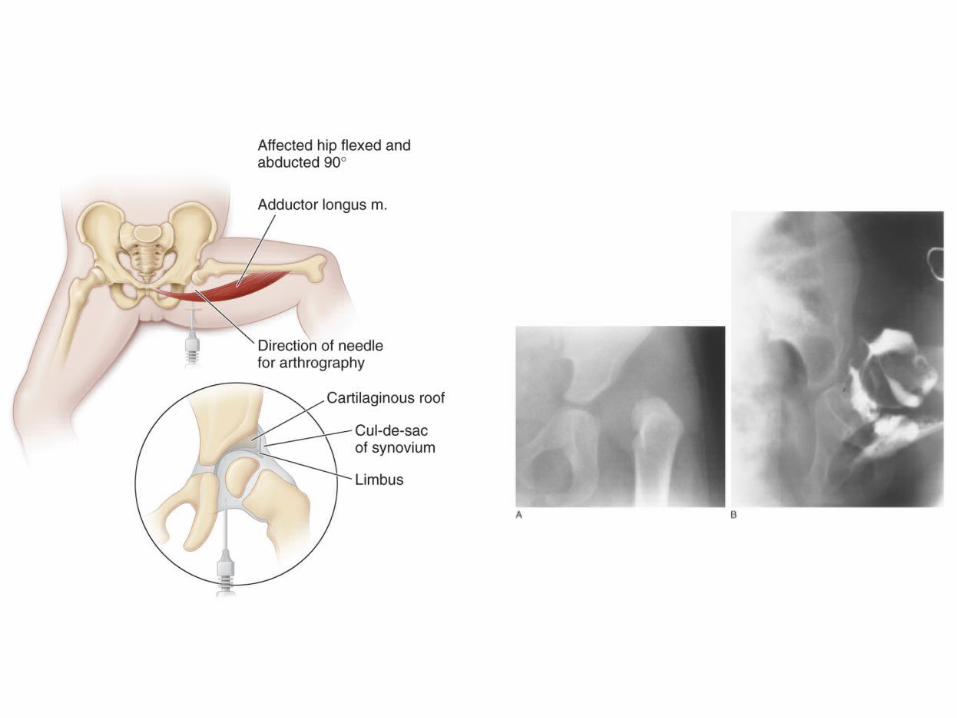
Arthrography
• Subadductor approach with image intensification.
• Needle beneath the adductor longus, about 2 cm distal to its origin.
• The needle is directed medially, aimed toward the contralateral sternoclavicular joint
• 1 mL of contrast agent is injected.
Magnetic Resonance Imaging
• Kashiwagi and associates proposed an MRI-based classification of hips with DDH.
• Group 1 hips had a sharp acetabular rim, and all were reducible with a Pavlik harness.
• Group 2 hips had a rounded acetabular rim, and almost all could be reduced with a Pavlik harness.
• Group 3 hips had an inverted acetabular rim, and none was reducible with the harness
ManagementAge-Based Guidelines for Treatment of Developmental Dysplasia of the Hip
• Neonate (<1 month): Place in Pavlik harness for 6 weeks.
• 1 to 6 months: Place in Pavlik harness for 6 weeks after hip reduce
• 6 to 18 months: ?Traction; closed reduction. If closed reduction is successful, place in cast for 3 months. If closed reduction is unsuccessful, perform open reduction. Open reduction is performed by a medial approach in children younger than 12 months of age and by an anterolateral approach in children older than 12 months of age.
• 18 to 24 months: ?Trial of closed reduction, or primary open reduction (anterolateral approach). A Salter osteotomy may or may not be part of the procedure.
• 24 months to 6 years: Perform primary open reduction (anterolateral approach) and femoral shortening, with or without a Salter osteotomy
Treatment of the Neonate:PAVLIK HARNESS:
The first indication for treatment is a hip that is dislocated and can be reduced by the examiner (Ortolani's sign) or can be subluxated by the examiner (Barlow's sign).
Hips are placed in 120 degrees of flexion
Abduction of the hips to occur by gravity alone. Abduction should never be forced by the straps on the harness
Hyperflexion of the hips may produce a femoral nerve palsy & inferior dislocation
Inadequate flexion (<90 degrees) will fail to reduce the hip
Pavlik disease : flattening of the posterolateral acetabulum
AVN (15%)
Normal on clinical examination but abnormal on ultrasonography
Close observation of such hips, with Ultrasonography repeated at 6 weeks of age
Hips that remain abnormal should
be treated With Pavlik
Harness
Hips that remain Normal No Rx
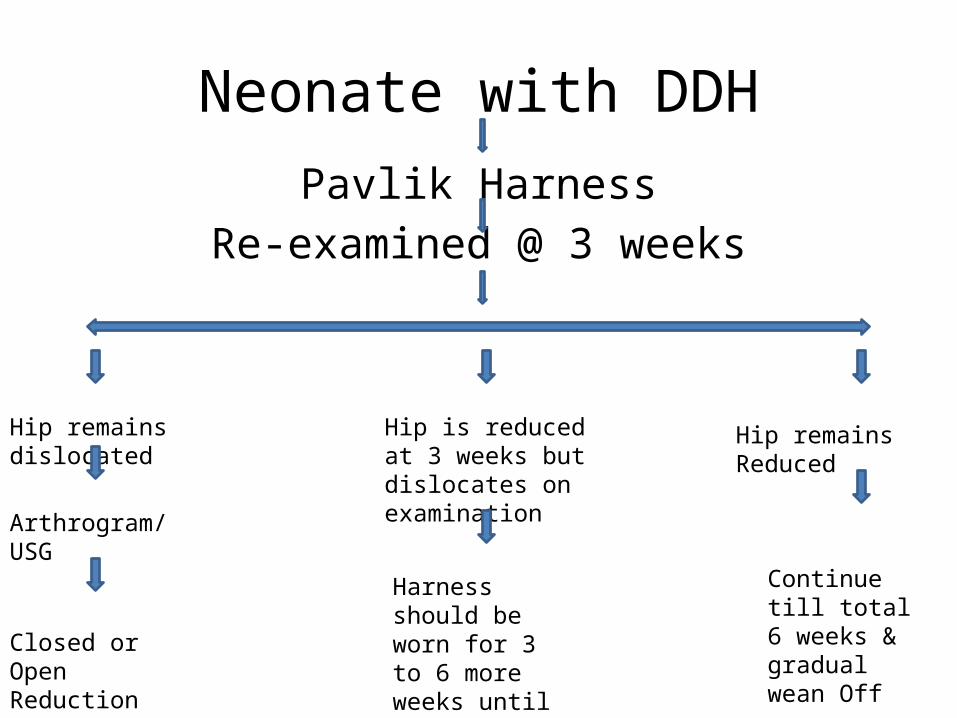
Neonate with DDHPavlik Harness
Re-examined @ 3 weeks
Hip remains dislocated Hip remains ReducedHip is reduced at 3 weeks but dislocates on examination
Arthrogram/USG
Closed or Open Reduction
Harness should be worn for 3 to 6 more weeks until the hip stabilizes
Continue till total 6 weeks & gradual wean Off
1 to 6 Months of Age
• The Pavlik harness is the first choice • If reduction is not obtained within 3 to 4
weeks, the harness should be discontinued and other treatment begun. If reduction is confirmed, the harness should be continued for about 6 weeks after stability is established.
• Treatment of older children for a longer time to encourage acetabular development.
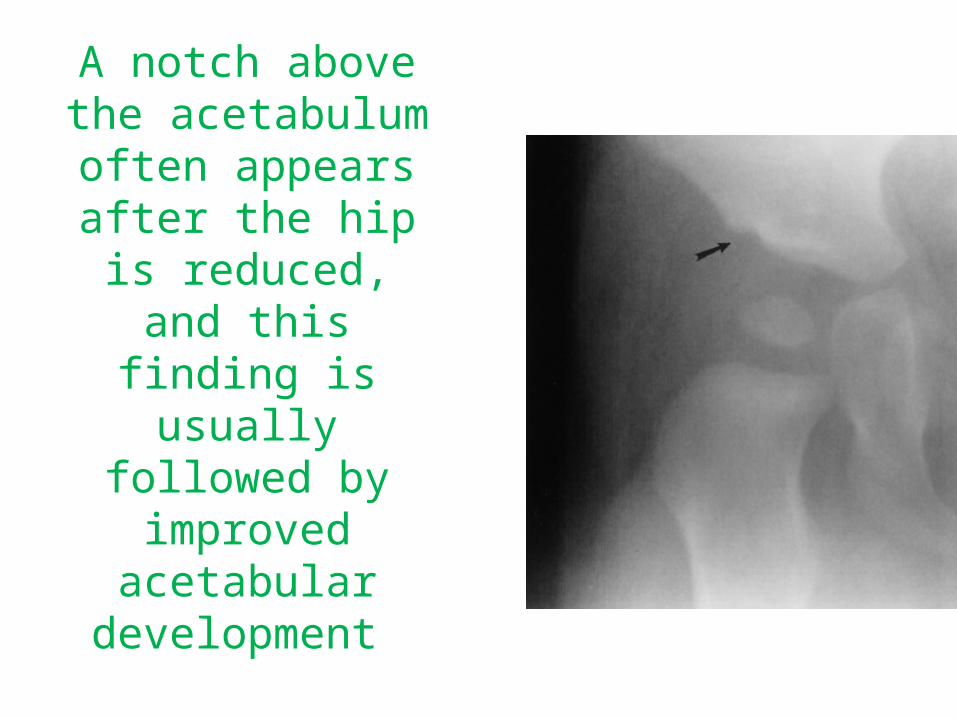
A notch above the acetabulum often appears after the hip is
reduced, and this finding is usually
followed by improved acetabular
development
OTHER SPLINTS AND BRACES
The Ilfeld splint
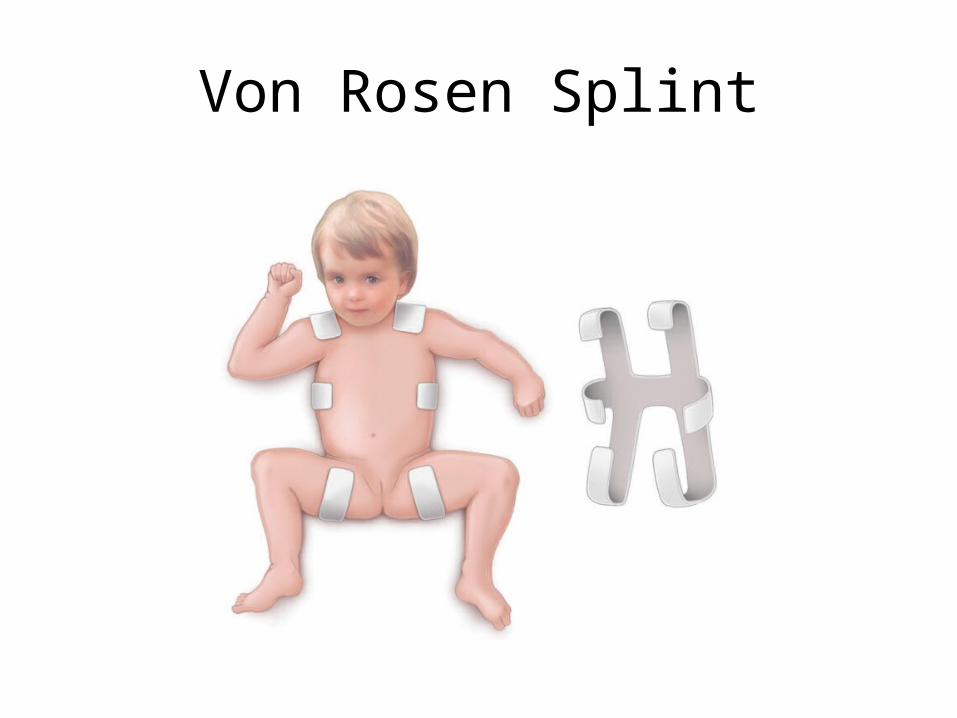
Von Rosen Splint
FREJKA PILLOW AND TRIPLE DIAPERS
• High rates of AVN• Triple diapers do not effectively position the
hips
6 Months to 2 Years of Age• The two principal methods of treatment : closed
reduction and open reduction followed by traction.
• Timing of Reduction : Reduction before appearing of Nucleus of head leads to AVN
Some advise not wait to treat a hip until the nucleus appears. The growth potential of the acetabulum declines with age, and hips reduced later will not remodel as well as those reduced earlier.(Preferable)
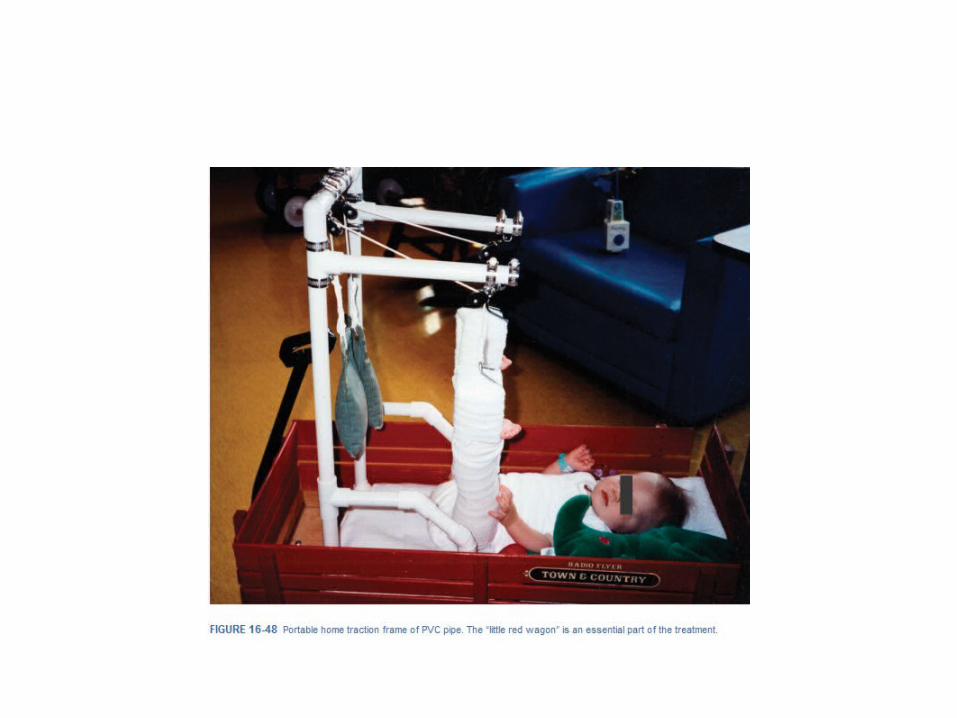
TRACTION
• Aim is to bring the femoral head to a “station” below Hilgenreiner's line.
• Lorenz or Lange position of extreme abduction without preliminary traction - 30% incidence of AVN.
• Same cast position was used after preliminary traction - 15% rate of AVN.
• Child was placed in the “human position” of 90 degrees of flexion and mild abduction, rate of AVN fell to 5%.
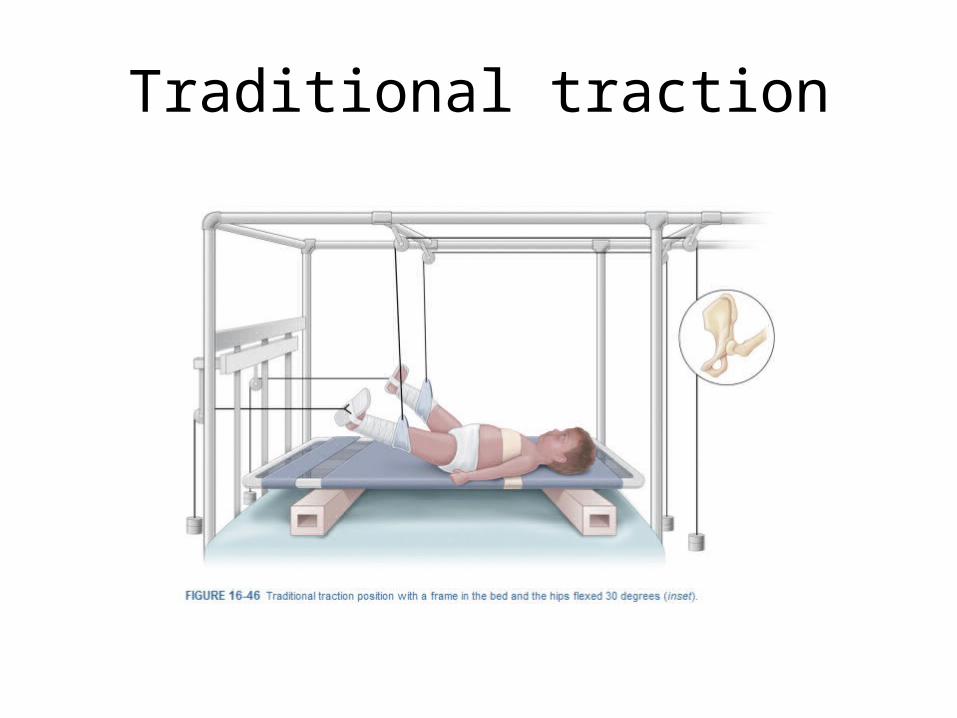
Traditional traction
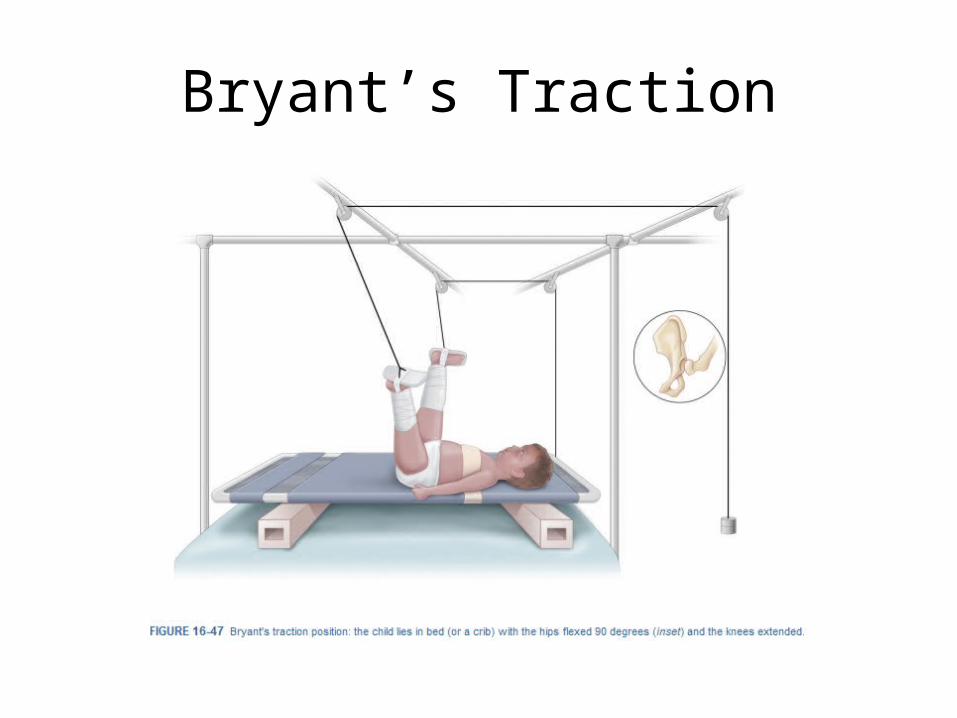
Bryant’s Traction
Closed Reduction and Casting for Developmental Dislocation of the Hip
• Better to think of positioning the hip rather than reducing it, because no real manipulation should be done may leads to AVN.
• Infant completely anesthetized
• Lift the greater trochanter with the fingers, and abduct the hip to reduce the femoral head – Hip flexion 120
• Stable Reduction - if the hip can be adducted 20 to 30 degrees from maximum abduction and extended to below 90 degrees without redislocation.
• Arthrogram - adequacy of the reduction.
• If the adductors are tight on palpation in the reduced position, tenotomy of the adductor longus performed to reduce pressure on the hip.
• Total 3 hip spica for 6 weeks duration each

Closed reduction & Hip Spica Cast
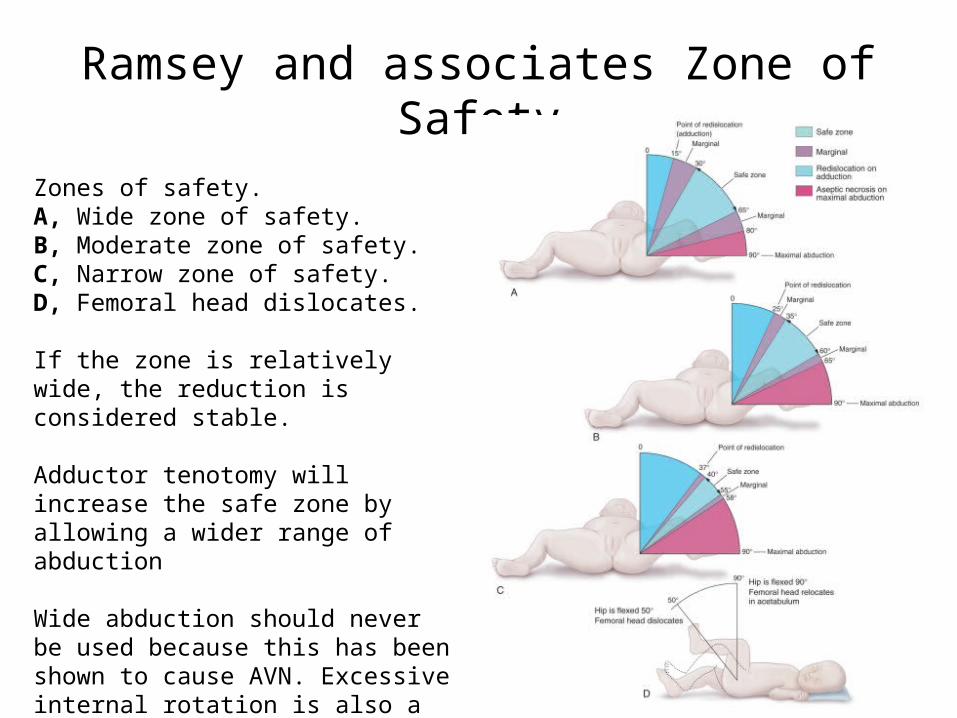
Ramsey and associates Zone of Safety
Zones of safety.A, Wide zone of safety.B, Moderate zone of safety.C, Narrow zone of safety.D, Femoral head dislocates.
If the zone is relatively wide, the reduction is considered stable.
Adductor tenotomy will increase the safe zone by allowing a wider range of abduction
Wide abduction should never be used because this has been shown to cause AVN. Excessive internal rotation is also a known cause of AVN, and must be avoided.
OPEN REDUCTION
• Indications:
failure to obtain a stable hip with a closed reduction.If there is any widening of the joint space between the femoral head and the acetabulum after closed reduction.
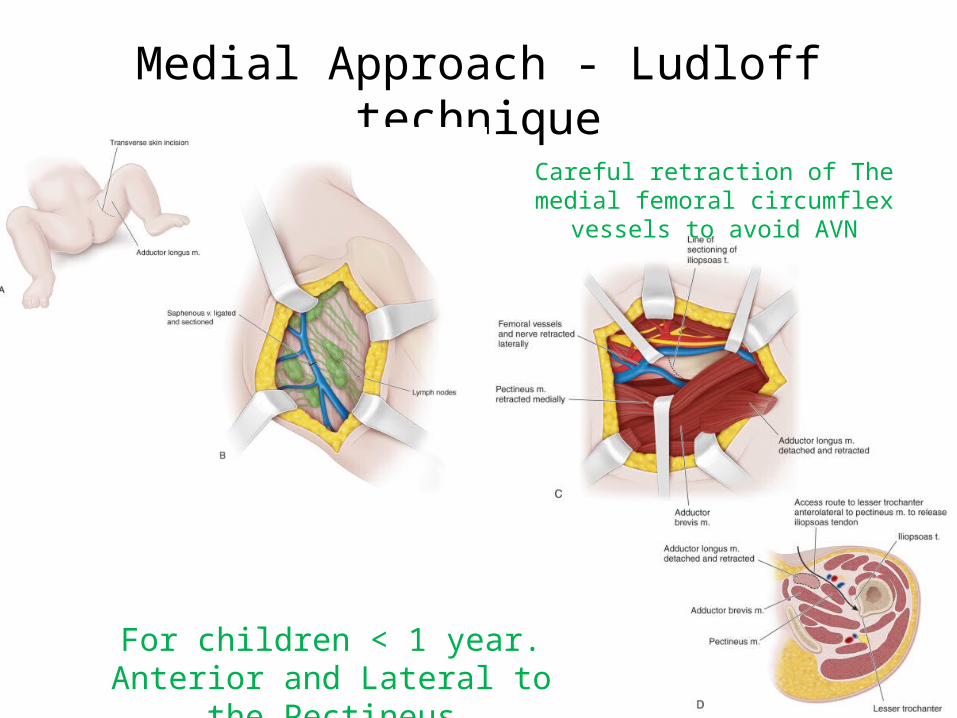
Medial Approach - Ludloff technique
For children < 1 year.Anterior and Lateral to the Pectineus
Careful retraction of The medial femoral circumflex vessels to avoid AVN
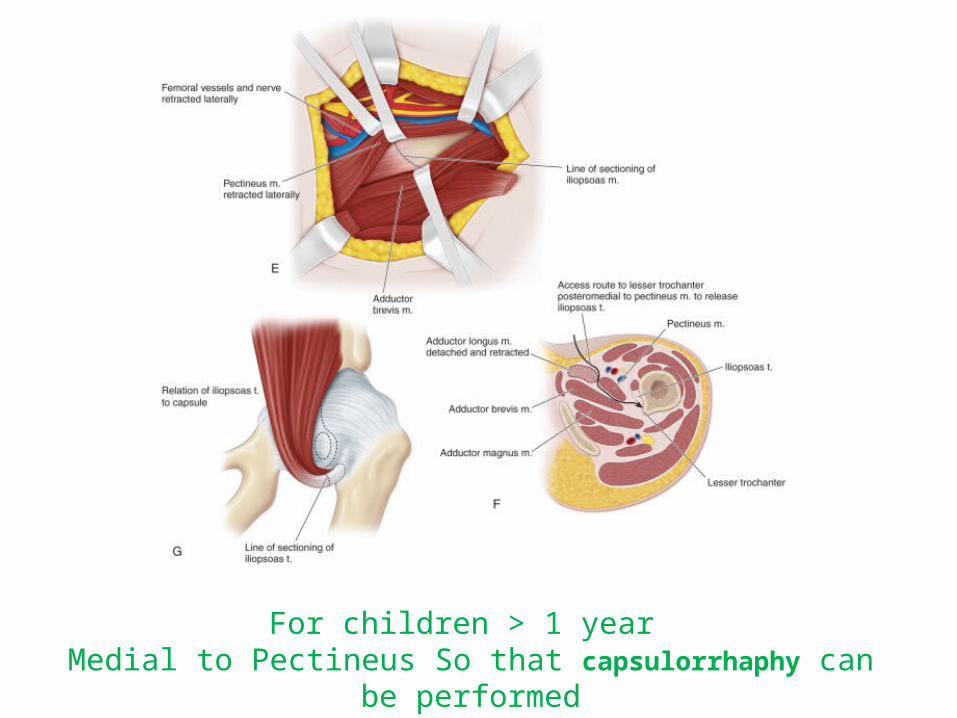
For children > 1 year Medial to Pectineus So that capsulorrhaphy can be performed
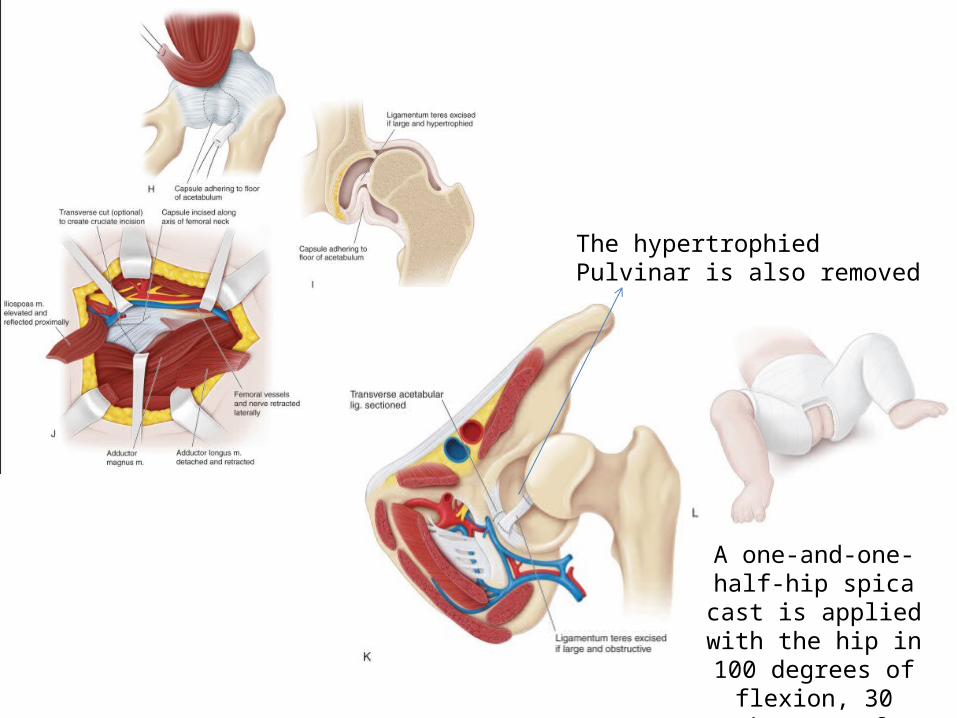
The hypertrophied Pulvinar is also removed
A one-and-one-half-hip spica cast is applied with the hip in 100 degrees of
flexion, 30 degrees of abduction and neutral
rotation
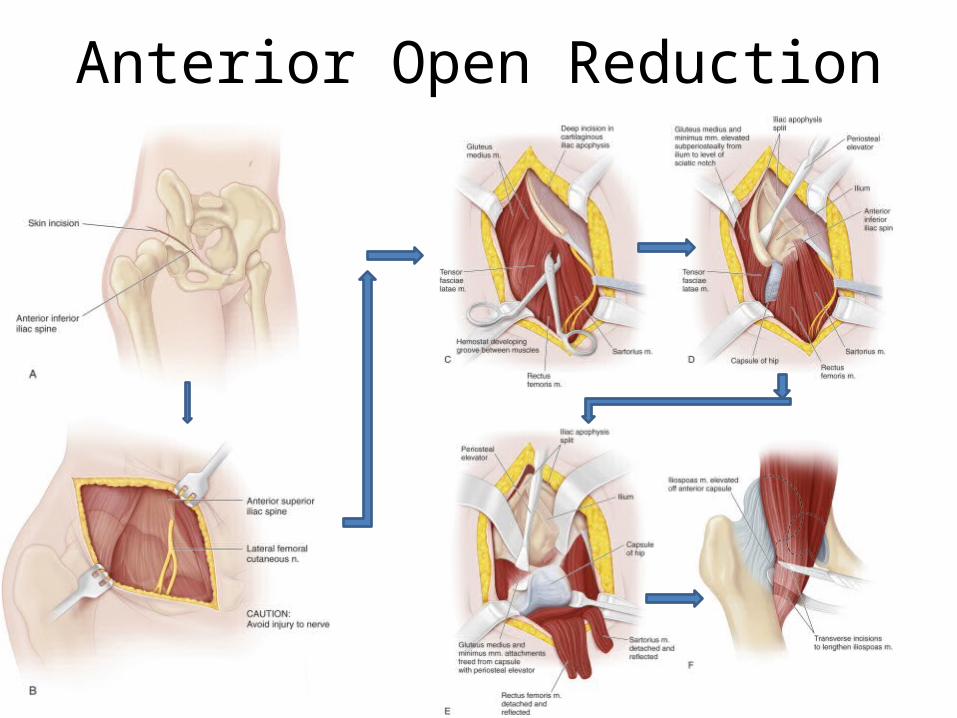
Anterior Open Reduction
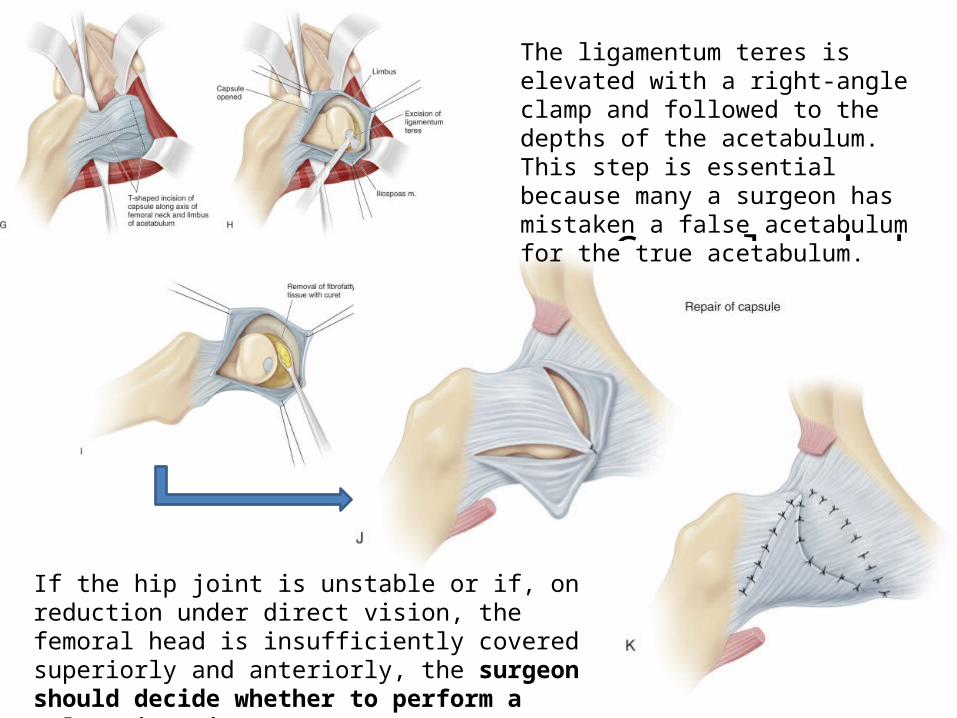
Capsulorrhahy
The ligamentum teres is elevated with a right-angle clamp and followed to the depths of the acetabulum. This step is essential because many a surgeon has mistaken a false acetabulum for the true acetabulum.
If the hip joint is unstable or if, on reduction under direct vision, the femoral head is insufficiently covered superiorly and anteriorly, the surgeon should decide whether to perform a Salter innominate osteotomy or a derotation osteotomy of the proximal femur at this time.
Pearls of wisdom
• Any redundent capsule is imbricated over this closure with nonabsorbable sutures.
• The two halves of the iliac apophysis are sutured together over the iliac crest.
• The rectus femoris and sartorius muscles are resutured to their origins.
• An AP radiograph of the hips is obtained to ensure a concentric reduction before a one-and-one-half-hip spica cast is applied.
Open Reduction combined with Femoral Shortening
• In irreducible hip, femoral shortening facilitates reduction
• If considerable force is required to reduce the hip and the reduction seems tight, the surgeon should perform a shortening femoral osteotomy to decompress the joint.
• Femoral shortening should be considered when a dislocated hip is reduced in a child older than 2 years of age.
• Perform the shortening through a separate lateral incision.
• Blade plate or simple lateral plate fixation may be used with an intertrochanteric or subtrochanteric osteotomy.

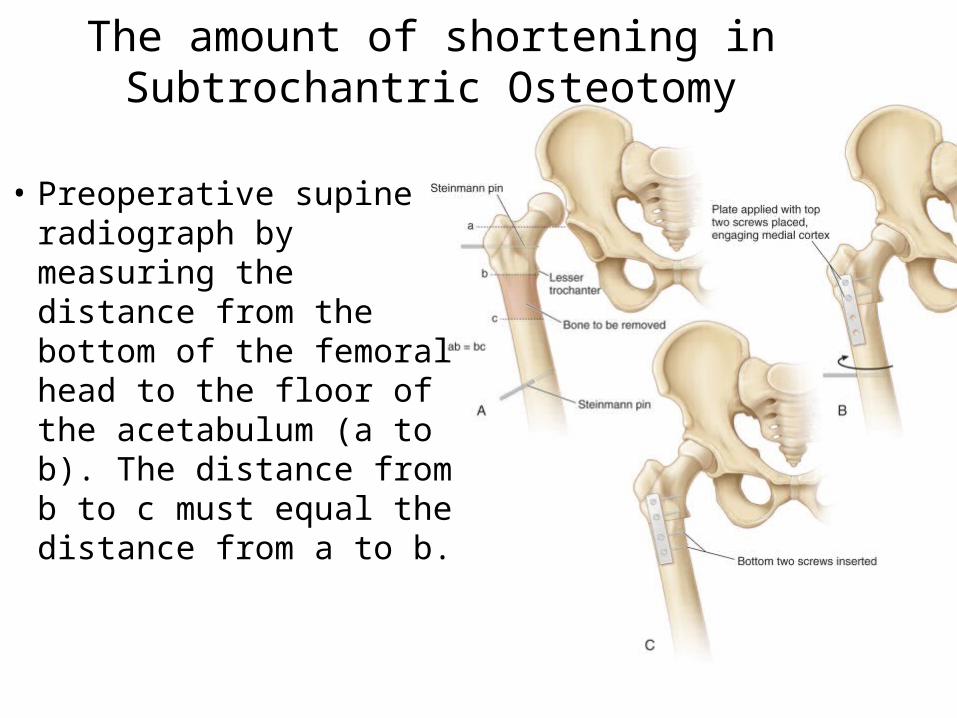
• Preoperative supine radiograph by measuring the distance from the bottom of the femoral head to the floor of the acetabulum (a to b). The distance from b to c must equal the distance from a to b.
The amount of shortening in Subtrochantric Osteotomy
• As a rule, the degree of hip decompression is adequate if the surgeon can, with a moderate force, distract the reduced femoral head 3 or 4 mm from the acetabulum.
Intertrochanteric Varus Osteotomy and Internal Fixation with a Blade Plate
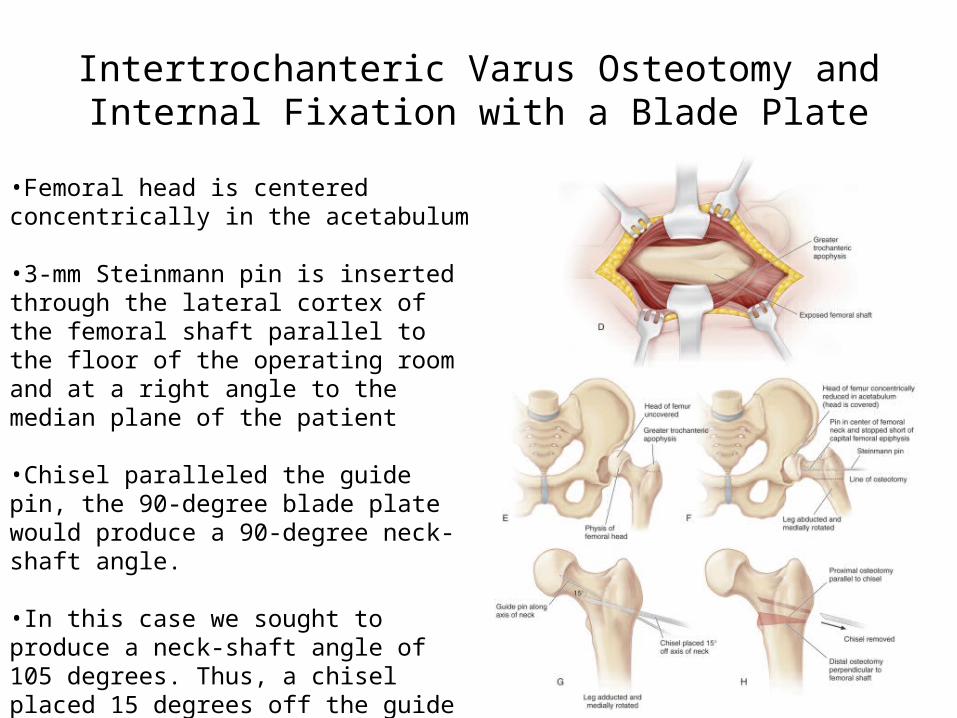
•Femoral head is centered concentrically in the acetabulum
•3-mm Steinmann pin is inserted through the lateral cortex of the femoral shaft parallel to the floor of the operating room and at a right angle to the median plane of the patient
•Chisel paralleled the guide pin, the 90-degree blade plate would produce a 90-degree neck-shaft angle.
•In this case we sought to produce a neck-shaft angle of 105 degrees. Thus, a chisel placed 15 degrees off the guide pin axis adds 15 degrees to a 90-degree neck-shaft angle, resulting in a 105-degree final angle
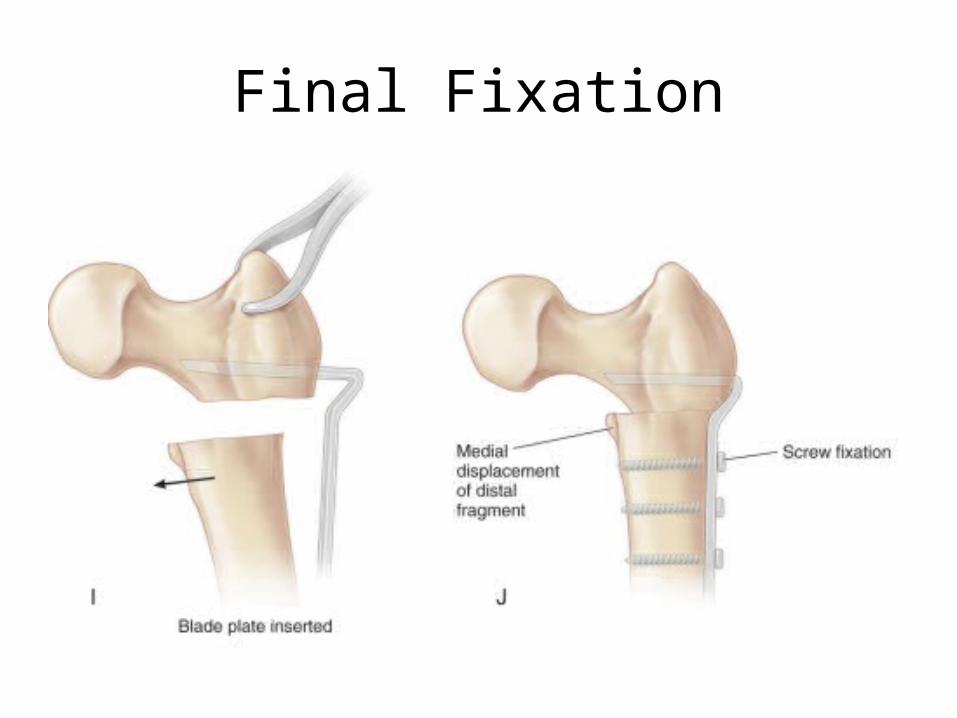
Final Fixation
Open Reduction with Innominate Osteotomy
• Children 18 months of age or older.
• If more than one third of the head is visible when femoral head placed in extension and neutral rotation and abduction.
• Salter innominate osteotomy / Pemberton or other periacetabular procedure
2 Years of Age and Older• The femoral head is usually in a more proximal location in
the older child, and the muscles that cross the hip are more severely contracted.
• Femoral shortening is an essential part of management in the older child, and with higher dislocations, greater shortening is necessary
• The older child is more likely to need a primary acetabular reorienting osteotomy, such as the Salter or Pemberton procedure.
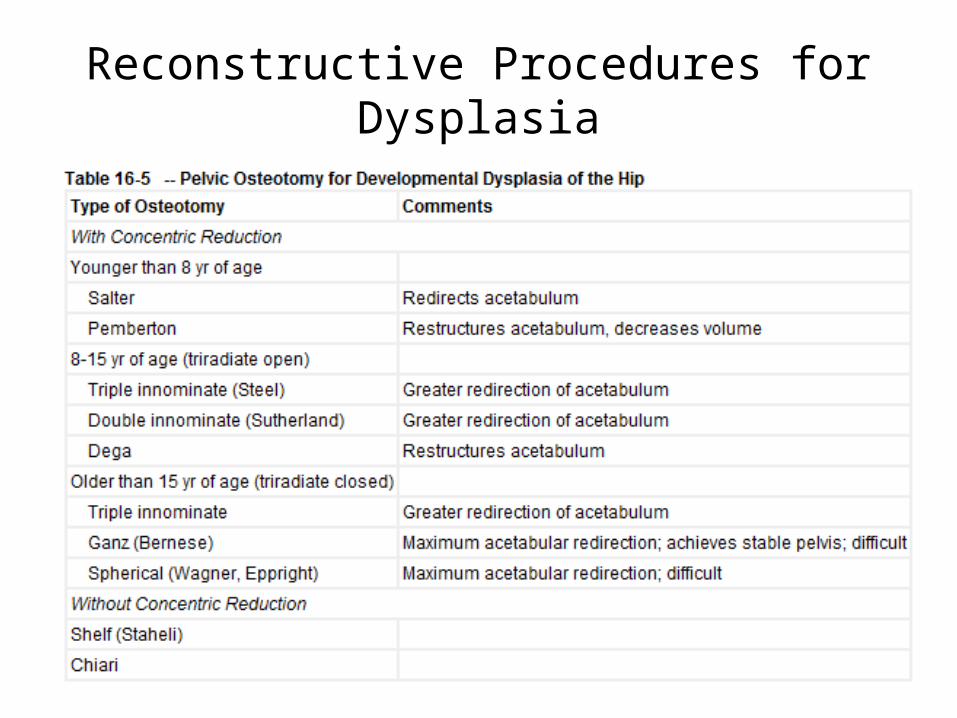
Reconstructive Procedures for Dysplasia
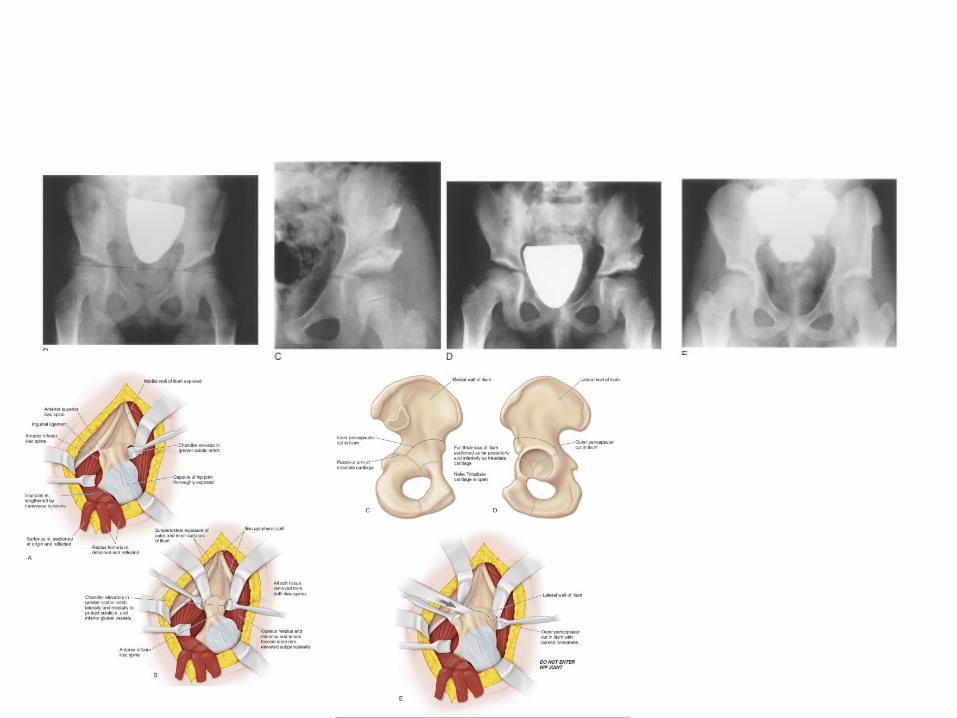
PEMBERTON OSTEOTOMY
• Repositions the acetabulum to improve anterior and lateral coverage of the femoral head.
• Osteotomy is quite stable and does not require fixation.
• Reduces the volume of the capacious acetabulum.
• Contraindicated if the acetabulum is small rela tive to the size of the femoral head.
Thank You