Embed Size (px)
Citation preview
بسم هللا الرحمن الرحيم

Dr. Ahmed Abdallah Eisawy
MBBS M.Sc MD
VIRTUAL
COLONOSCOPY
Virtual colonoscopy
New Imaging Technique
• Volumetric CT or MRI data
Processed to
Virtual endoscopic images of the
colon Main Application:
Early detection of colorectal
cancer
CT Virtual Colonoscopy
Means
CT Colonography +
Volumetric data + Specialized Imaging software
Image Display
2D and 3D Why ??
• The best polyp detection by CTC occurs with
combined 2D and 3D images.
• Diagnosis of lipoma by 2D. • Decrease falsies :
-Fecal matter. -Barium remnants.
-Respiratory misregistration.
-Diverticulum with fecal matter or barium
Advantages of this procedure:
Visualization of the entire colon.
High diagnostic accuracy for polyps larger than
1 cm in diameter.
Ability to assess extracolonic abdominal and
pelvic organs.
Potential diagnostic test for colorectal cancer.
Virtual Colonoscopy Technique
The Advantages of Multi-slice
Scanning
• 1-Improved Temporal Resolution.
• 2-Improved Spatial Resolution in the Z-Axis.
• 3-Increased Concentration of Intravascular Contrast Material.
• 4-Decreased Image Noise.
• 5-Efficient X-ray Tube Use.
• 6-Longer Anatomic Coverage.
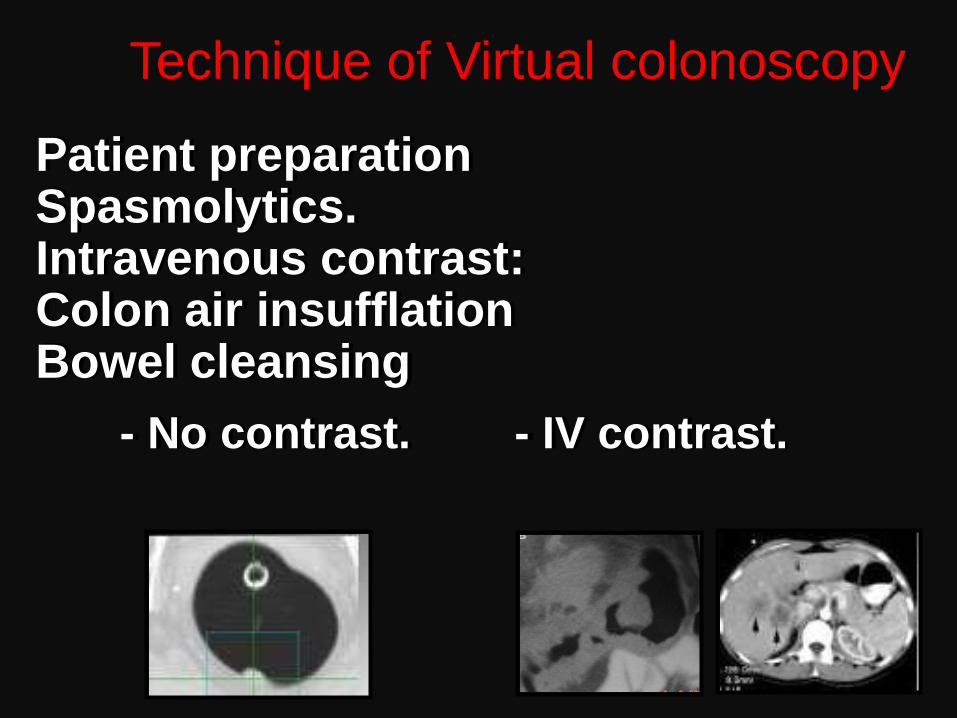
Patient preparation Spasmolytics. Intravenous contrast: Colon air insufflation Bowel cleansing
- No contrast. - IV contrast.
Technique of Virtual colonoscopy
Colon air insufflation Bowel cleansing
CONTRAST FOR VC IS AIR
.
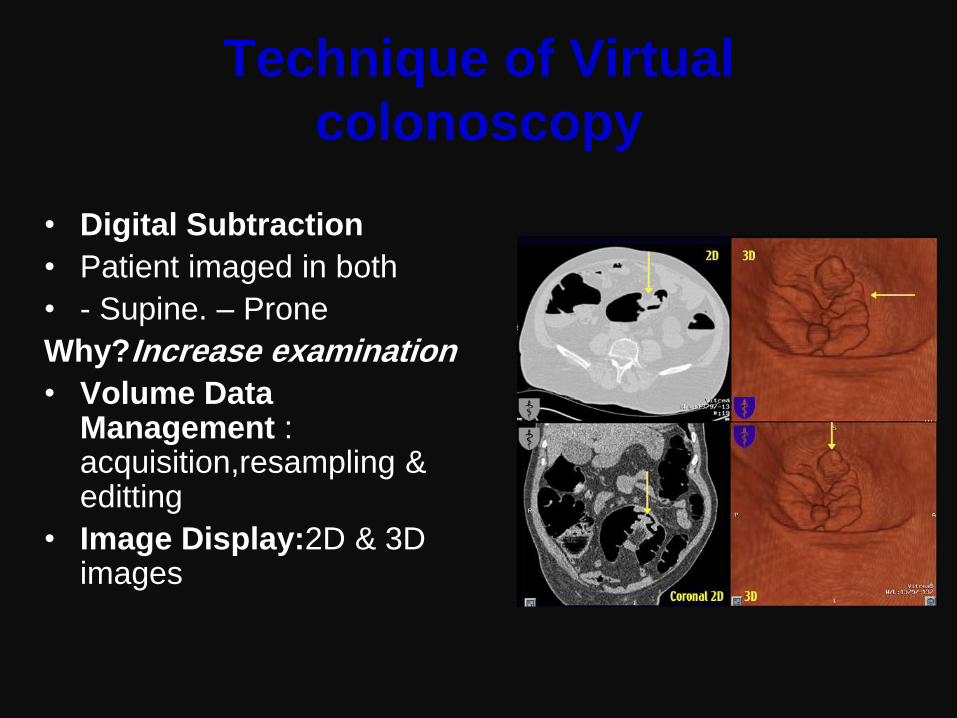
Technique of Virtual
colonoscopy
• Digital Subtraction
• Patient imaged in both
• - Supine. – Prone
Why?Increase examination
• Volume Data Management : acquisition,resampling & editting
• Image Display:2D & 3D images
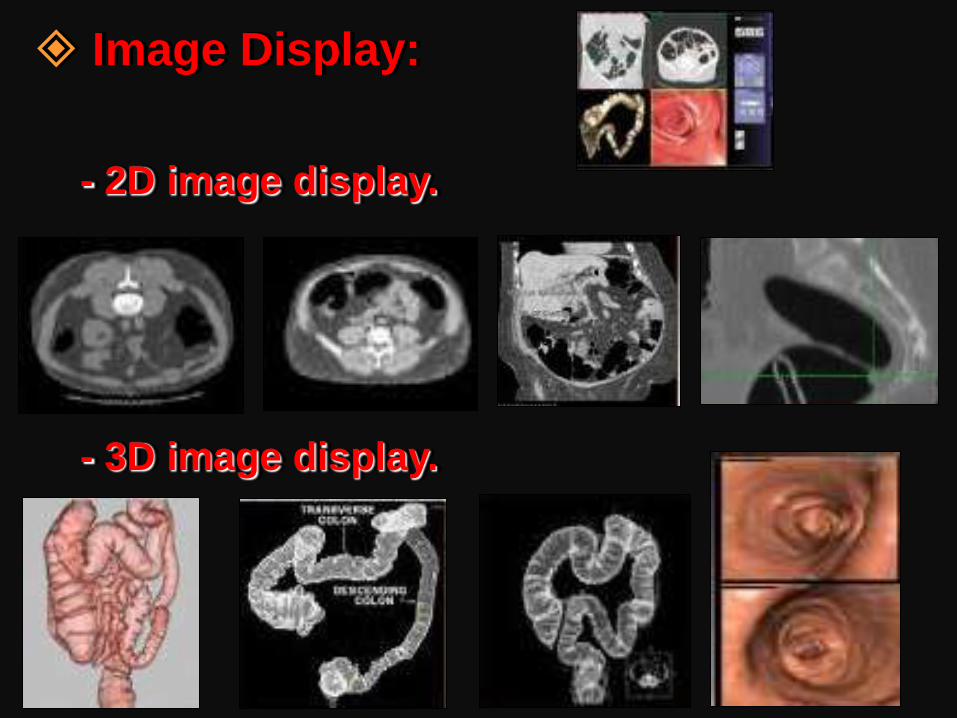
Image Display:
- 2D image display.
- 3D image display.
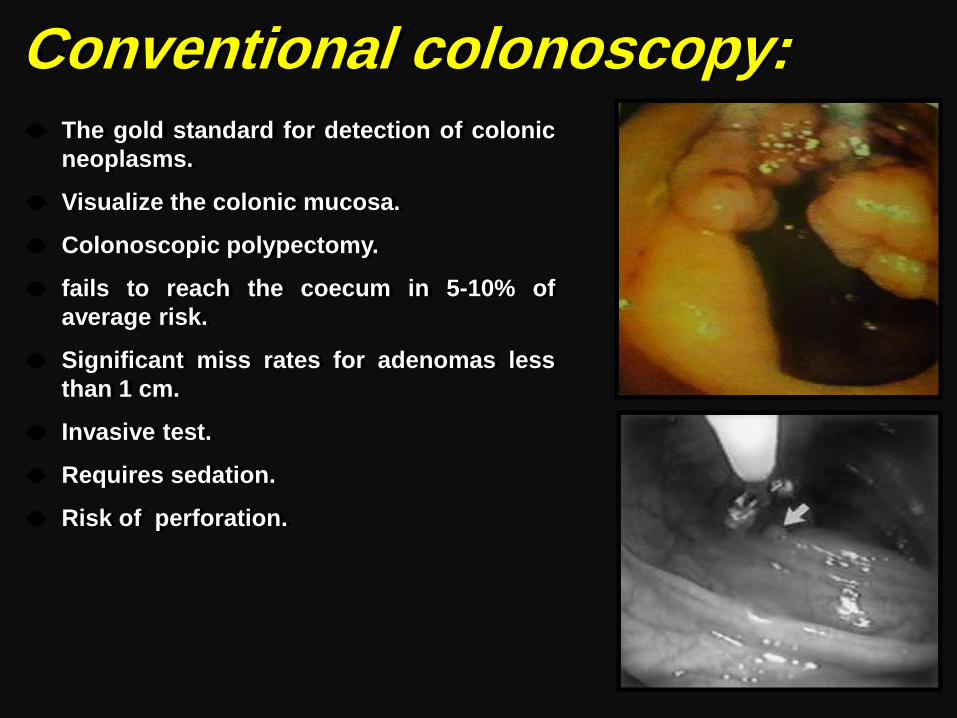
Conventional colonoscopy: The gold standard for detection of colonic
neoplasms.
Visualize the colonic mucosa.
Colonoscopic polypectomy.
fails to reach the coecum in 5-10% of
average risk.
Significant miss rates for adenomas less
than 1 cm.
Invasive test.
Requires sedation.
Risk of perforation.
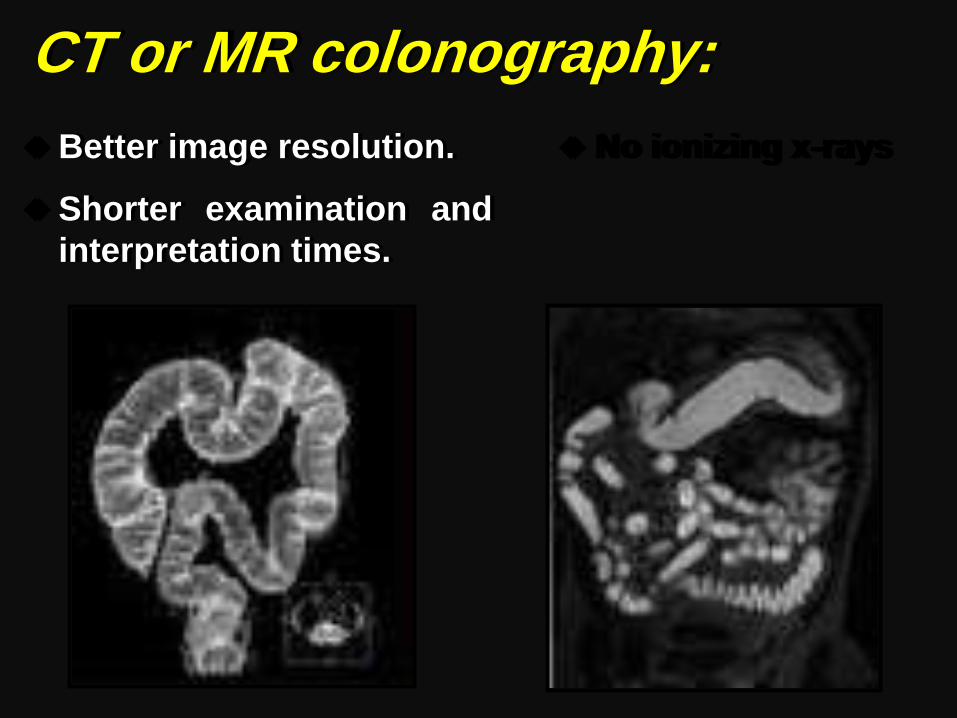
CT or MR colonography:
Better image resolution.
Shorter examination and
interpretation times.
No ionizing x-rays
Fly-through Technique
• The computations that guide the motion guide the
dynamic point of view representing a virtual volume.
VC Compared To
Conventional Colonoscopy
Advantages
• No sedation
• No analgesia
• Least intervention.
• Occlusive carcinoma.
• Extra-luminal lesion.
• Post irradiation.
Disadvantages
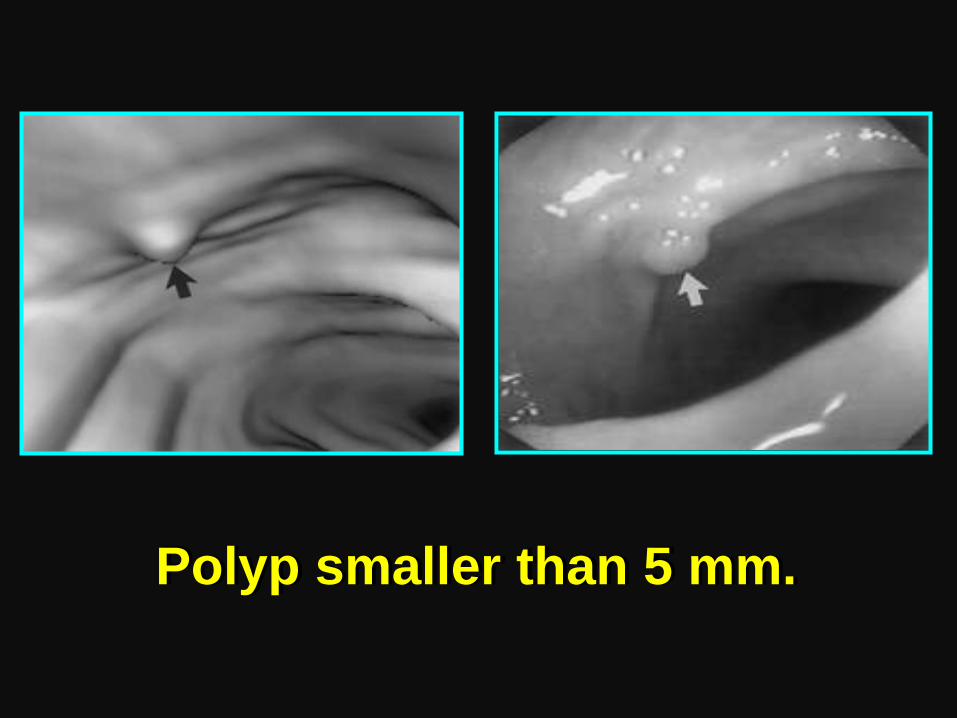
• Flat adenoma.
• Small polyp
• No therapy
Sensitivity of Virtual Colonoscopy
for the detection of colorectal
masses Virtual
Colonscopy:
• 93.8% for polyps at
least 10 mm.
• 93.9% for polyps at
least 8mm.
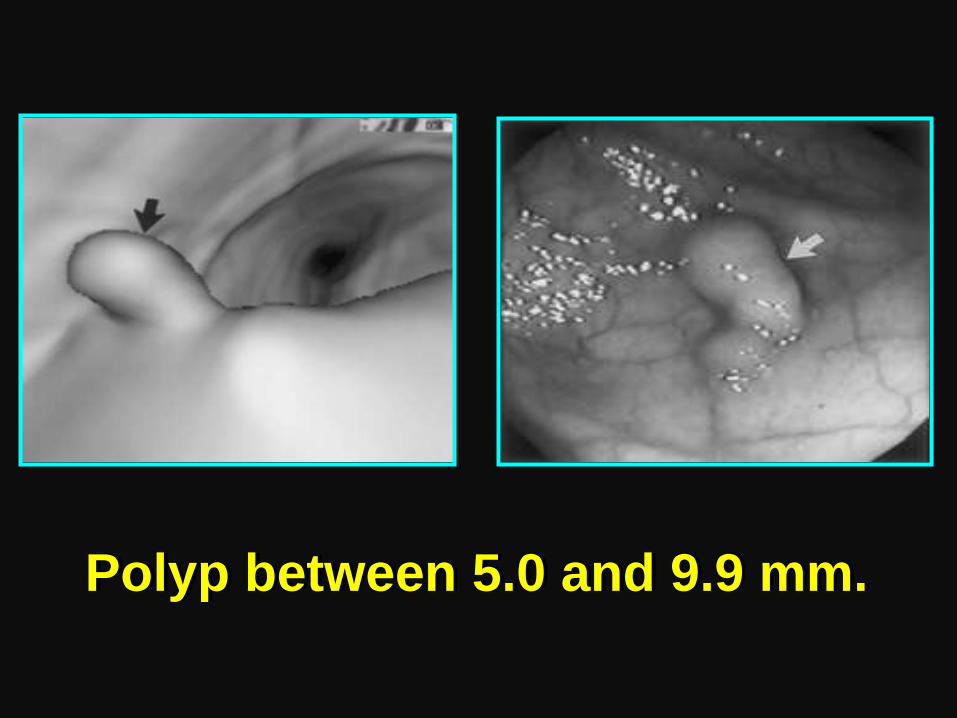
• 88.7% for polyps at
least 6mm.
Conventional Colonoscopy:
• 87.5% for polyps at least 10 mm.
• 91% for polyps at least 8 mm.
• 92.3% for polyps at least 6 mm.
Compared To
Barium Enema Radiography
Advantages
• No Barium • Little effect from retained
fluid.
• No complex overlapping of
radiographic lines.
• Infinite No. of projections on
demand
• No 2ry cathartic preparation
prior to colonoscopy
Disadvantages
• More cost.
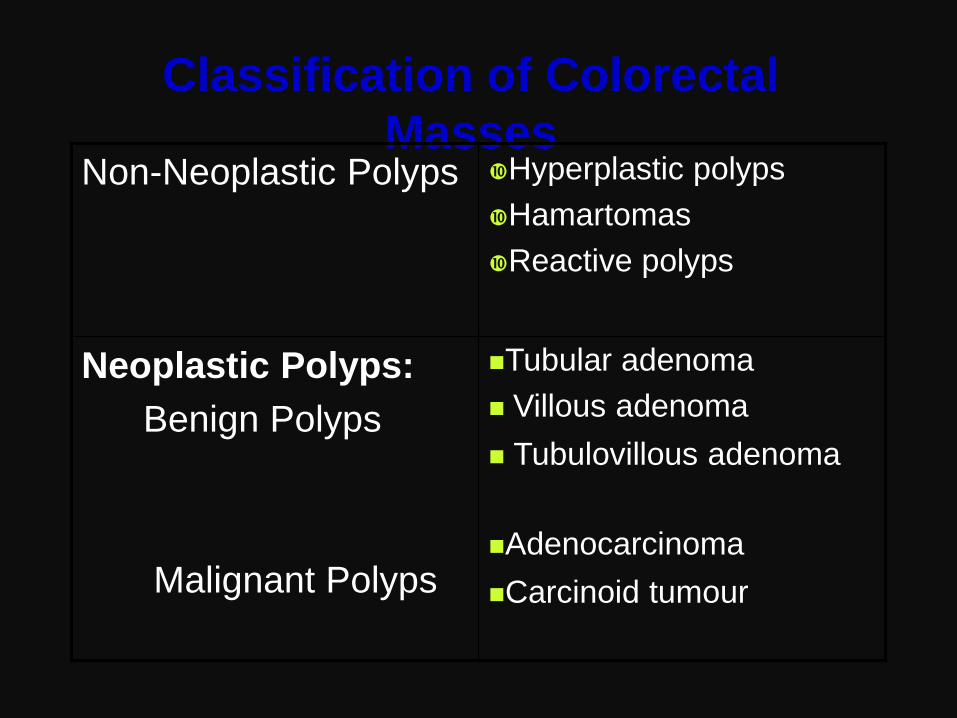
Classification of Colorectal
Masses Non-Neoplastic Polyps Hyperplastic polyps
Hamartomas
Reactive polyps
Neoplastic Polyps:
Benign Polyps
Malignant Polyps
Tubular adenoma
Villous adenoma
Tubulovillous adenoma
Adenocarcinoma
Carcinoid tumour
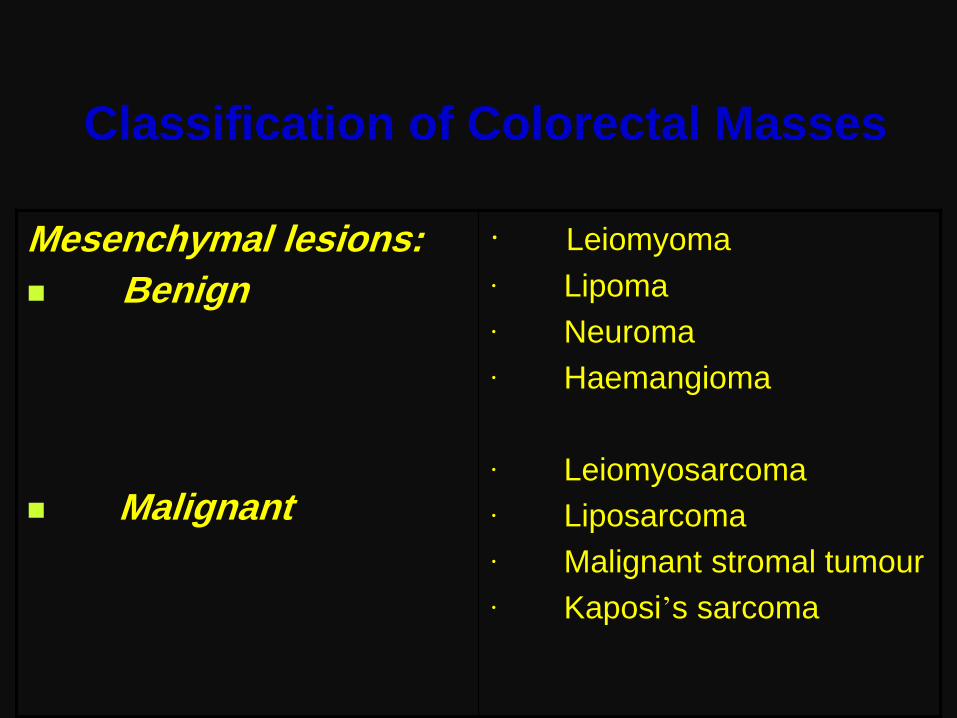
Classification of Colorectal Masses
Mesenchymal lesions:
Benign
Malignant
· Leiomyoma
· Lipoma
· Neuroma
· Haemangioma
· Leiomyosarcoma
· Liposarcoma
· Malignant stromal tumour
· Kaposi’s sarcoma
Colorectal masses by Virtual Colonoscopy
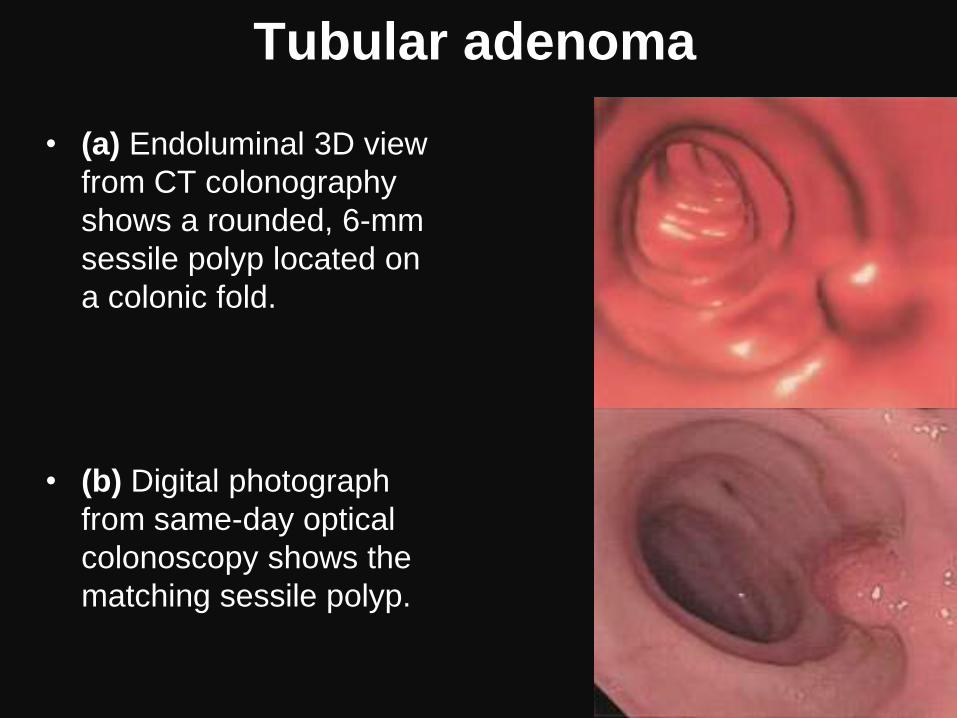
Tubular adenoma
• (a) Endoluminal 3D view
from CT colonography
shows a rounded, 6-mm
sessile polyp located on
a colonic fold.
• (b) Digital photograph
from same-day optical
colonoscopy shows the
matching sessile polyp.
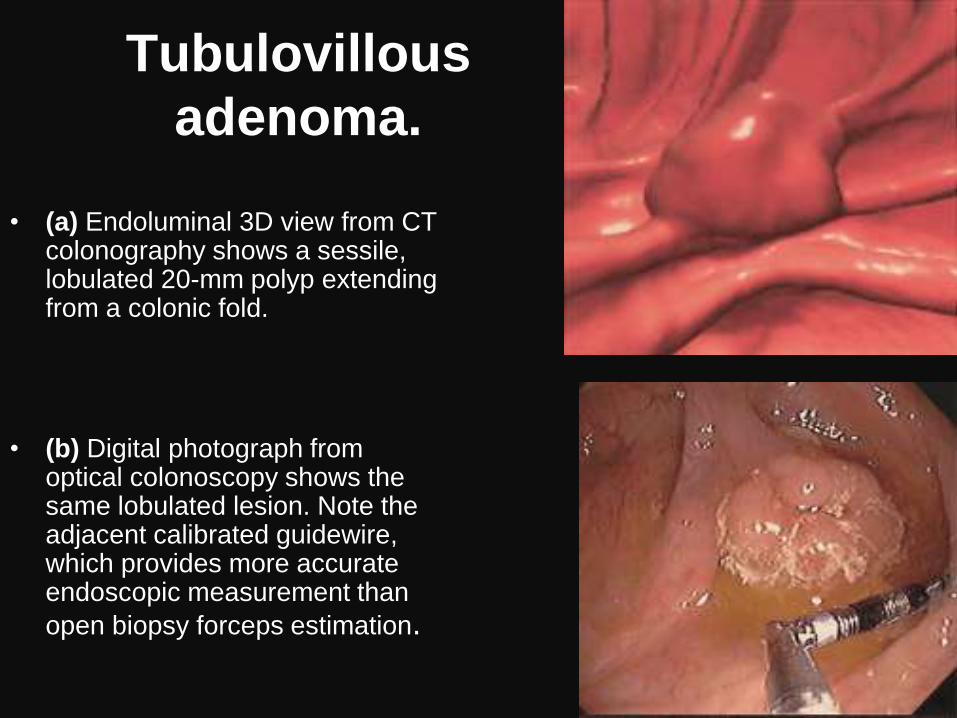
Tubulovillous
adenoma.
• (a) Endoluminal 3D view from CT
colonography shows a sessile, lobulated 20-mm polyp extending from a colonic fold.
• (b) Digital photograph from optical colonoscopy shows the same lobulated lesion. Note the adjacent calibrated guidewire, which provides more accurate endoscopic measurement than
open biopsy forceps estimation.
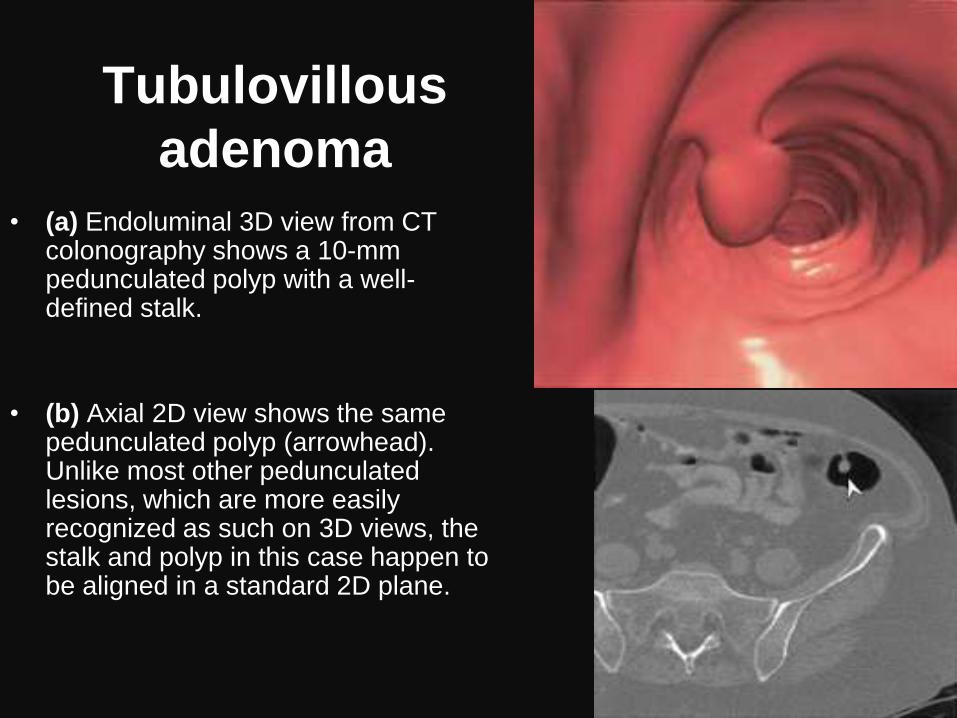
Tubulovillous
adenoma
• (a) Endoluminal 3D view from CT colonography shows a 10-mm pedunculated polyp with a well-defined stalk.
• (b) Axial 2D view shows the same pedunculated polyp (arrowhead). Unlike most other pedunculated lesions, which are more easily recognized as such on 3D views, the stalk and polyp in this case happen to be aligned in a standard 2D plane.
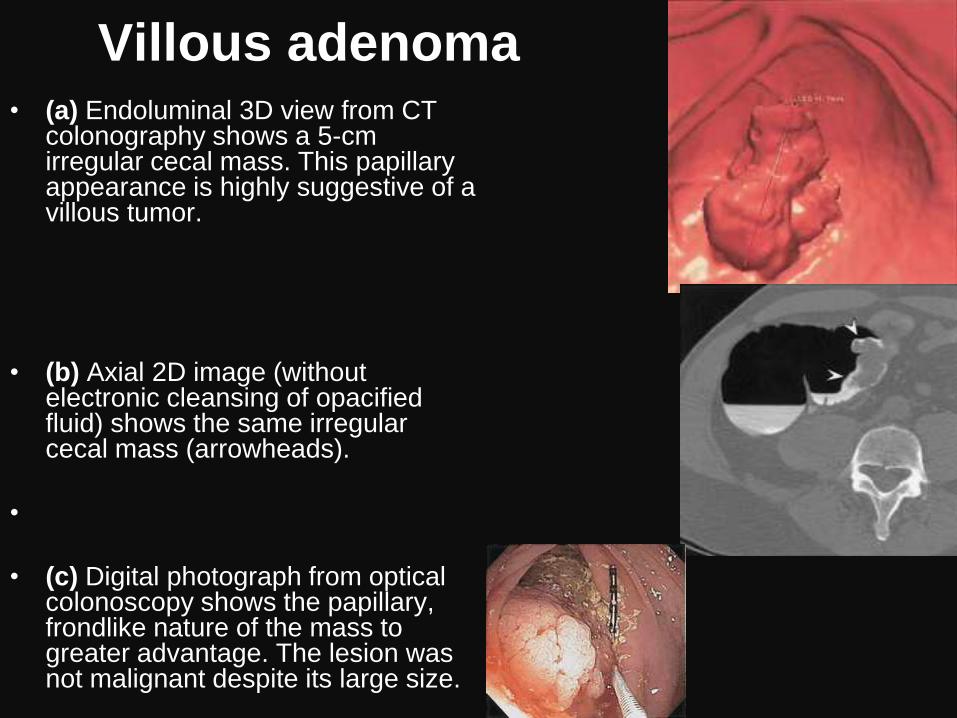
Villous adenoma • (a) Endoluminal 3D view from CT
colonography shows a 5-cm irregular cecal mass. This papillary appearance is highly suggestive of a villous tumor.
• (b) Axial 2D image (without electronic cleansing of opacified fluid) shows the same irregular cecal mass (arrowheads).
•
• (c) Digital photograph from optical colonoscopy shows the papillary, frondlike nature of the mass to greater advantage. The lesion was not malignant despite its large size.
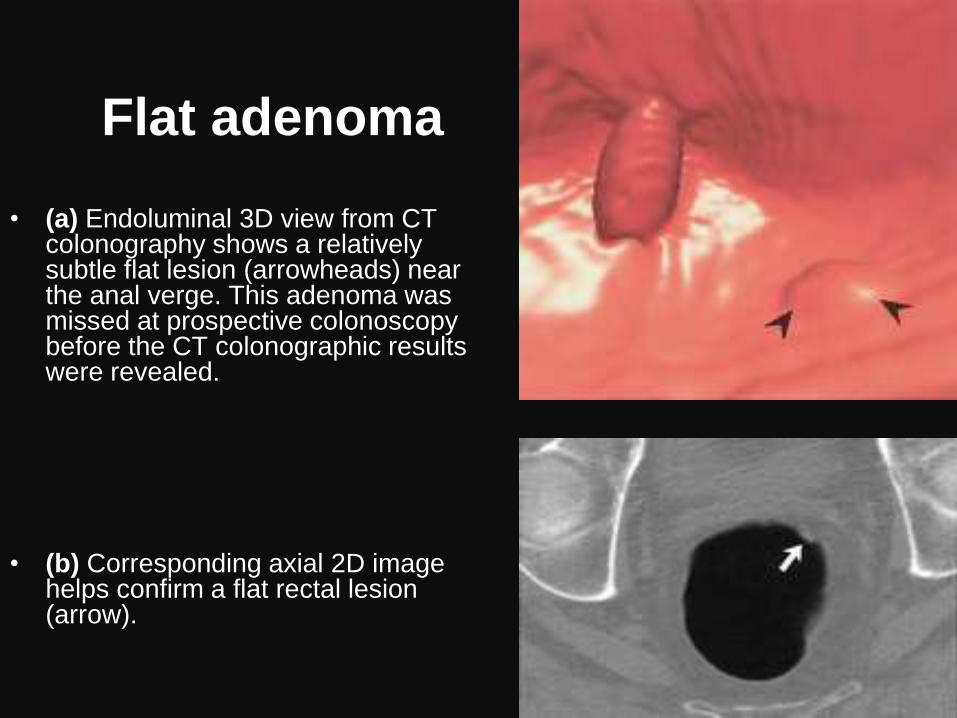
Flat adenoma
• (a) Endoluminal 3D view from CT colonography shows a relatively subtle flat lesion (arrowheads) near the anal verge. This adenoma was missed at prospective colonoscopy before the CT colonographic results were revealed.
• (b) Corresponding axial 2D image helps confirm a flat rectal lesion (arrow).
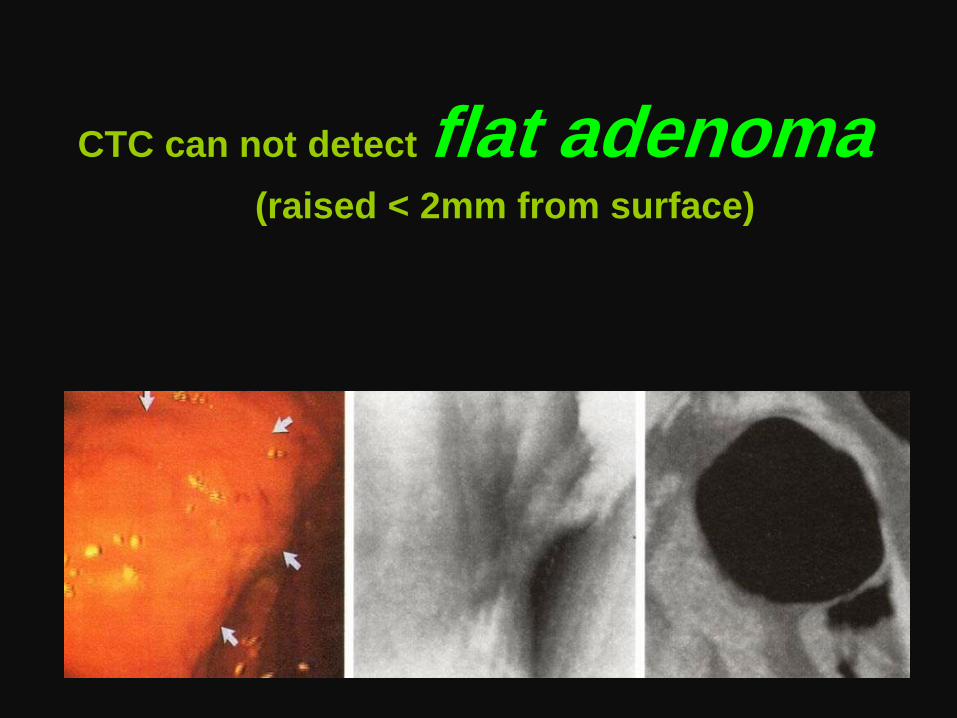
CTC can not detect flat adenoma
(raised < 2mm from surface)
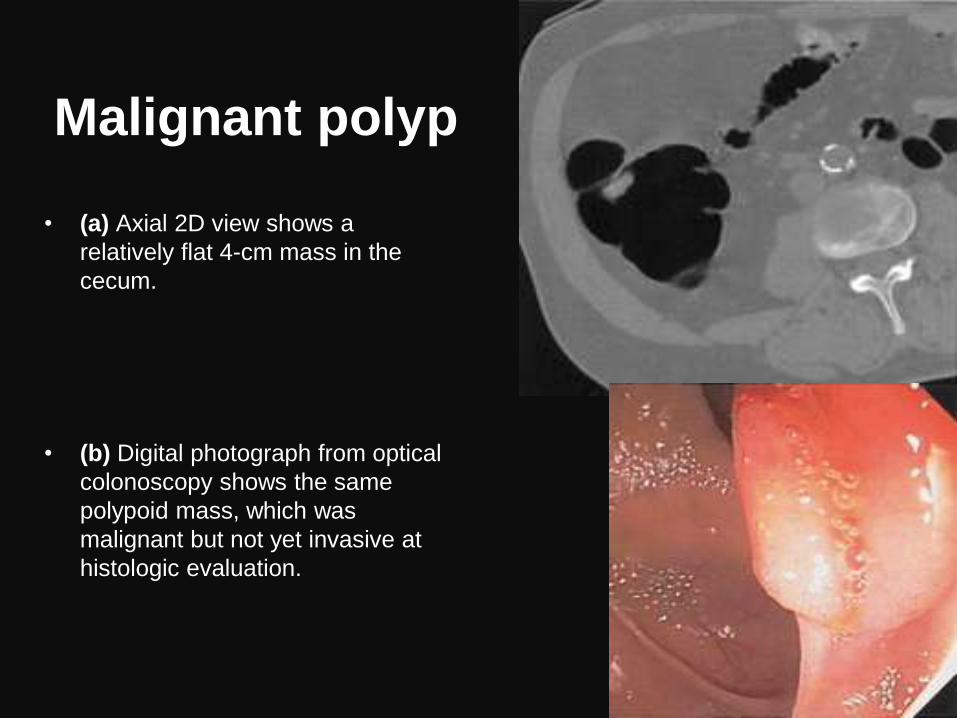
Malignant polyp
• (a) Axial 2D view shows a
relatively flat 4-cm mass in the
cecum.
• (b) Digital photograph from optical
colonoscopy shows the same
polypoid mass, which was
malignant but not yet invasive at
histologic evaluation.
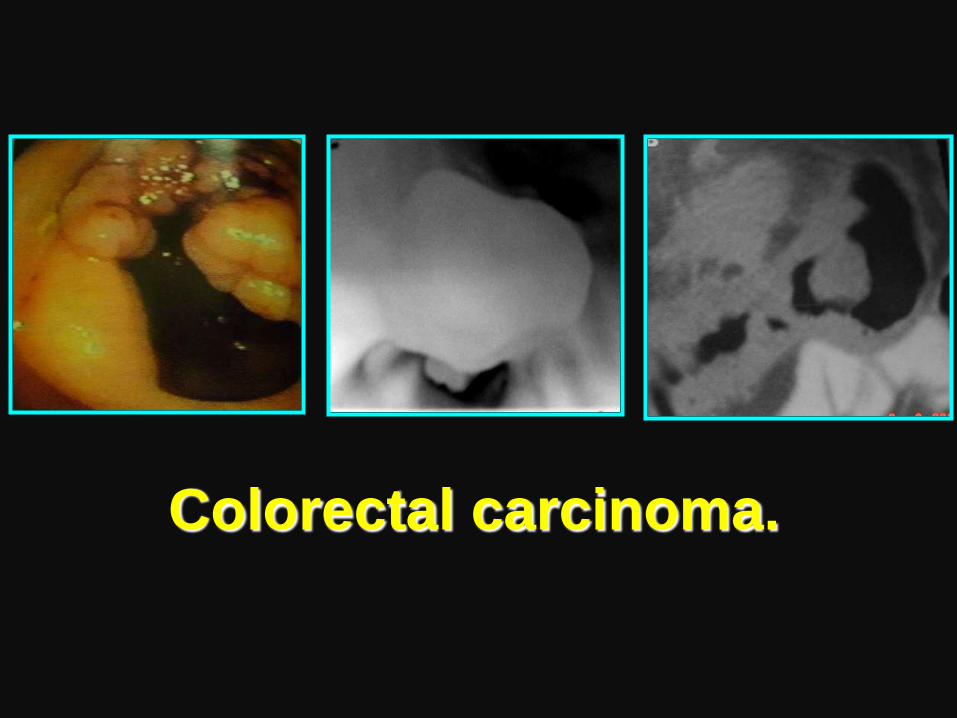
Colorectal carcinoma.
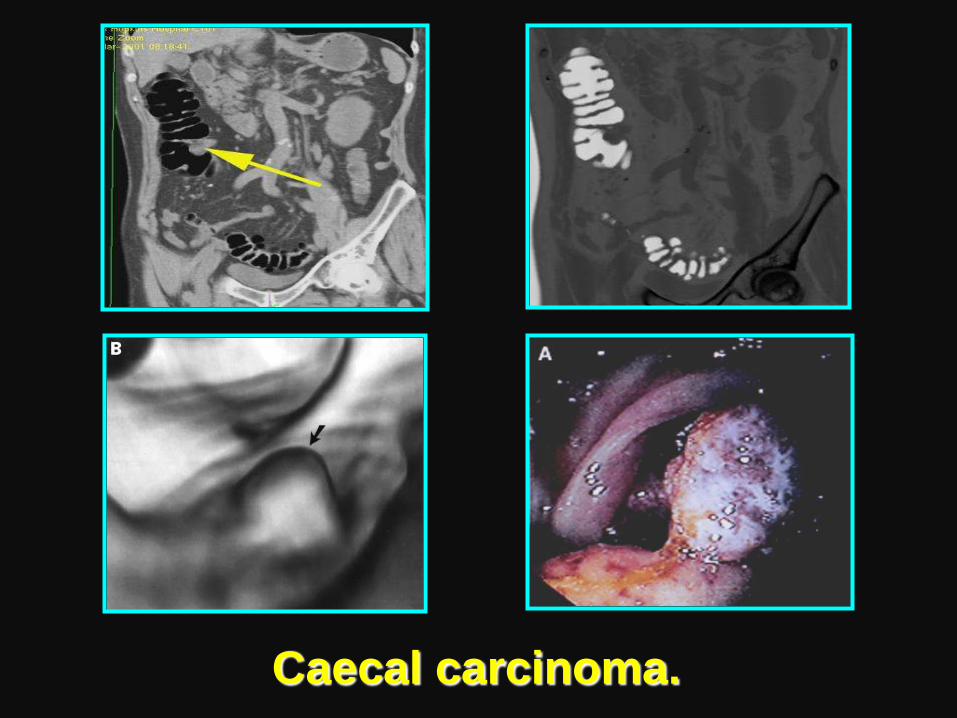
Caecal carcinoma.
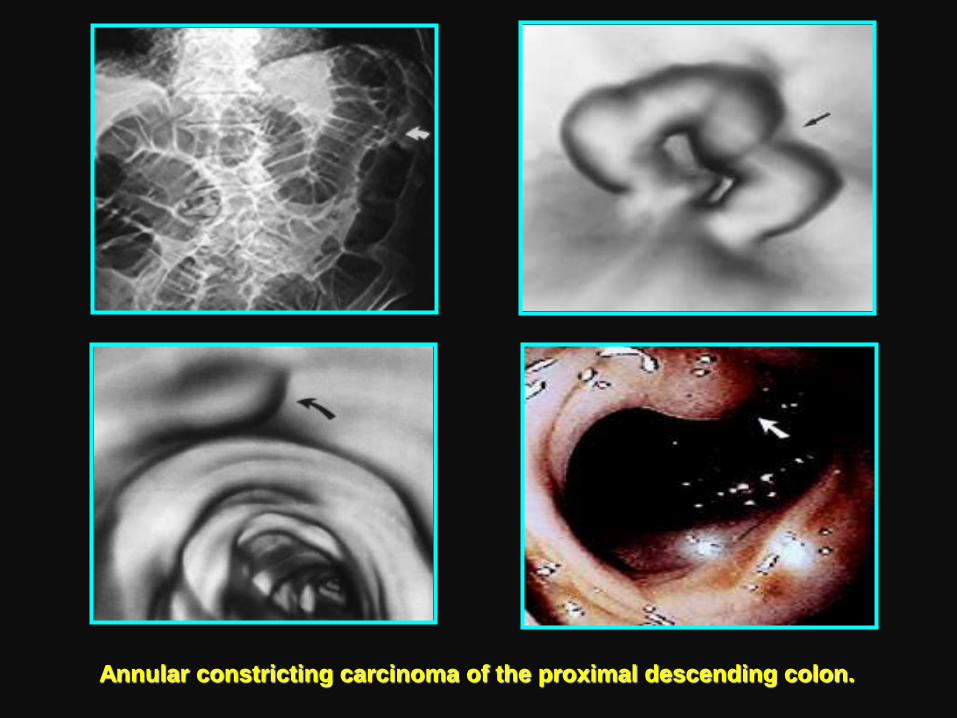
Annular constricting carcinoma of the proximal descending colon.
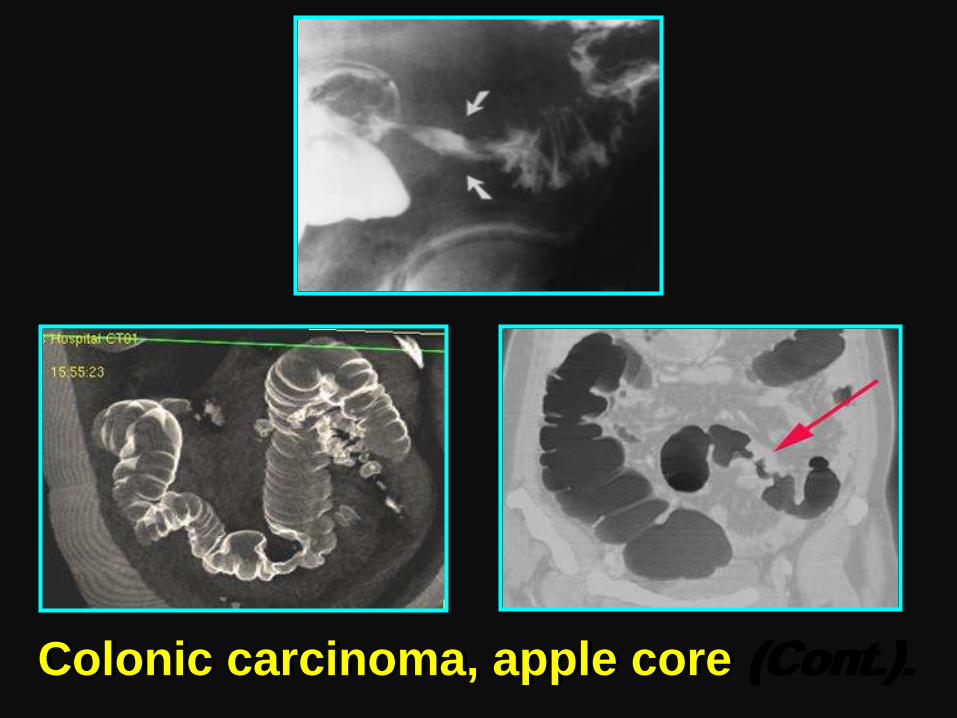
Colonic carcinoma, apple core (Cont.).
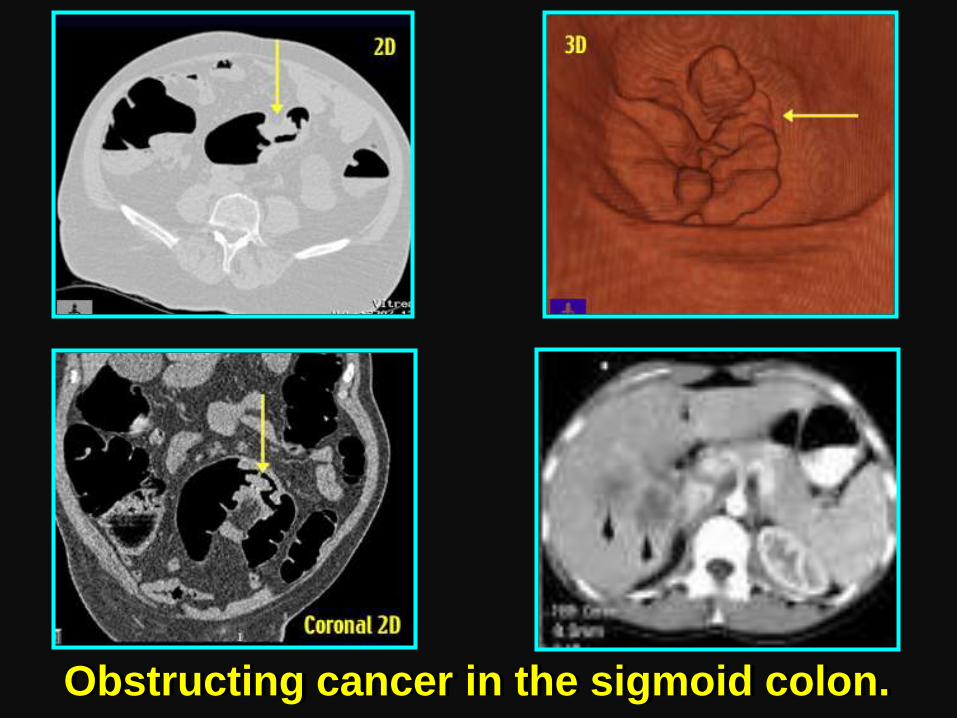
Obstructing cancer in the sigmoid colon.
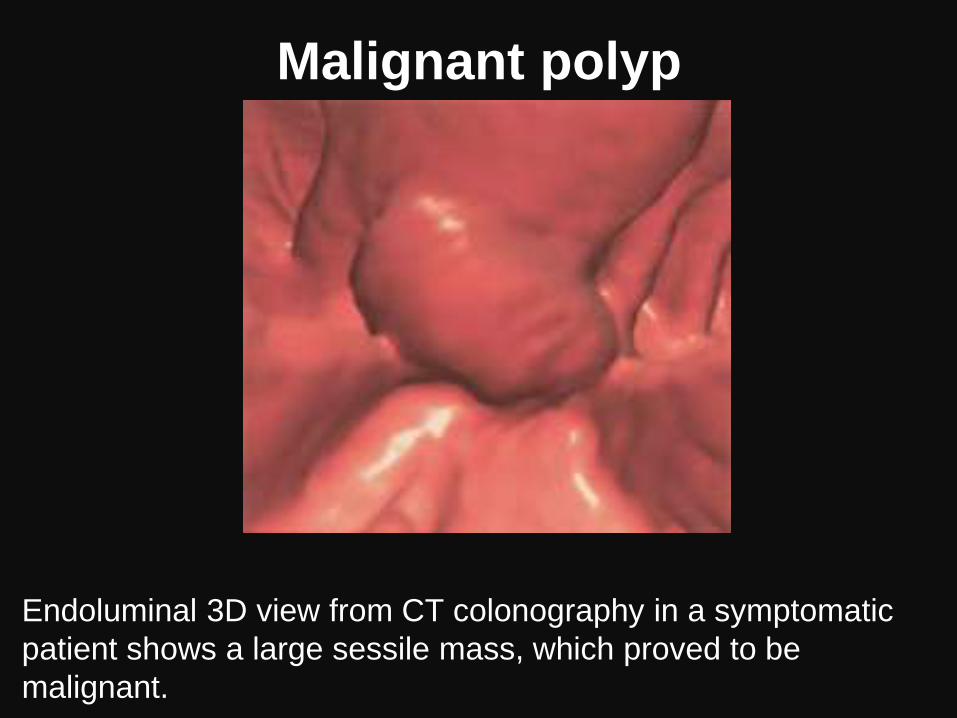
Malignant polyp
Endoluminal 3D view from CT colonography in a symptomatic
patient shows a large sessile mass, which proved to be
malignant.
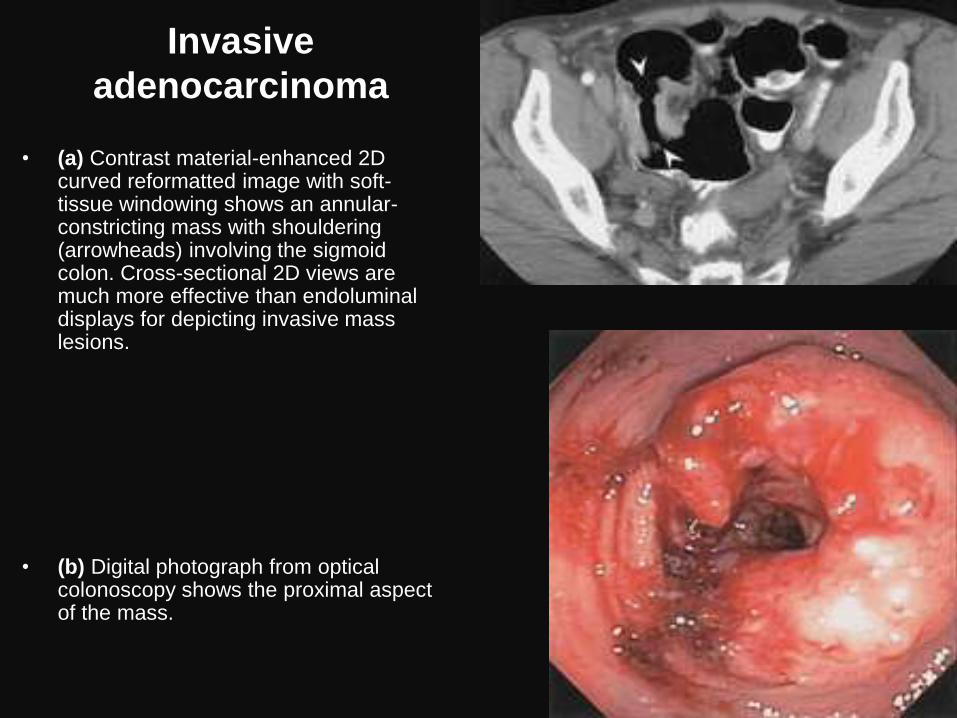
Invasive
adenocarcinoma
• (a) Contrast material-enhanced 2D curved reformatted image with soft-tissue windowing shows an annular-constricting mass with shouldering (arrowheads) involving the sigmoid colon. Cross-sectional 2D views are much more effective than endoluminal displays for depicting invasive mass lesions.
• (b) Digital photograph from optical colonoscopy shows the proximal aspect of the mass.
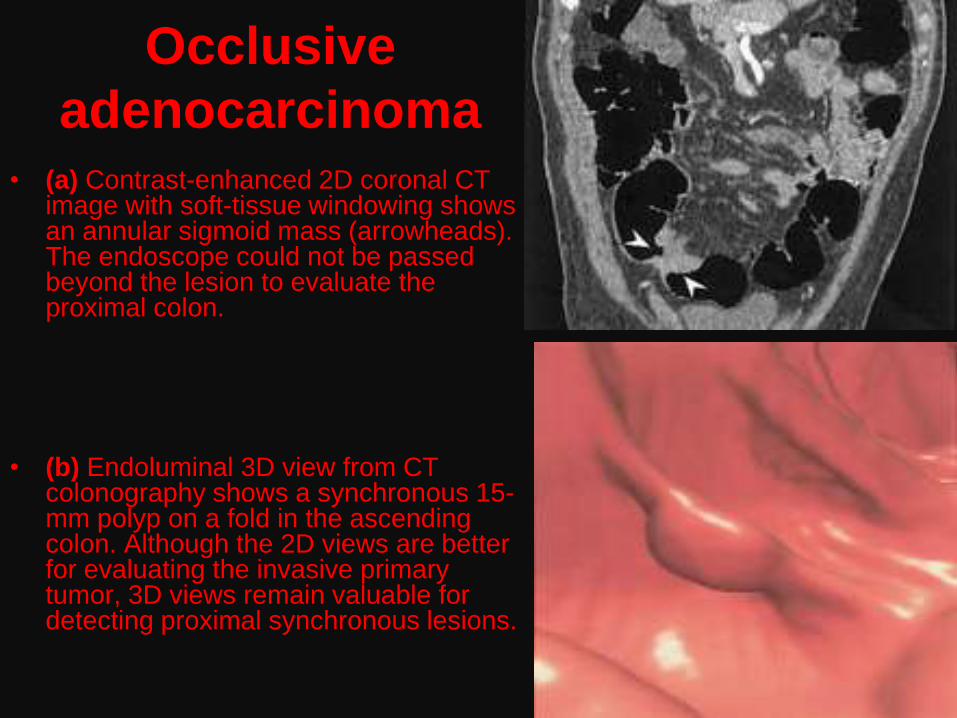
Occlusive
adenocarcinoma • (a) Contrast-enhanced 2D coronal CT
image with soft-tissue windowing shows an annular sigmoid mass (arrowheads). The endoscope could not be passed beyond the lesion to evaluate the proximal colon.
• (b) Endoluminal 3D view from CT colonography shows a synchronous 15-mm polyp on a fold in the ascending colon. Although the 2D views are better for evaluating the invasive primary tumor, 3D views remain valuable for detecting proximal synchronous lesions.
Nonneoplastic Mucosal Lesions
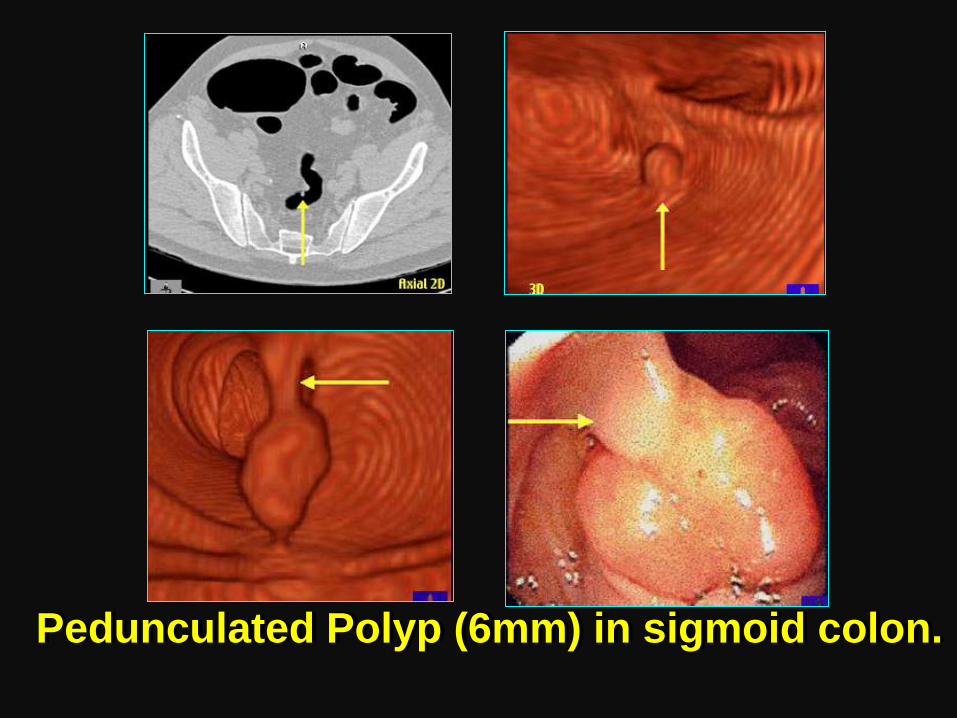
Pedunculated Polyp (6mm) in sigmoid colon.
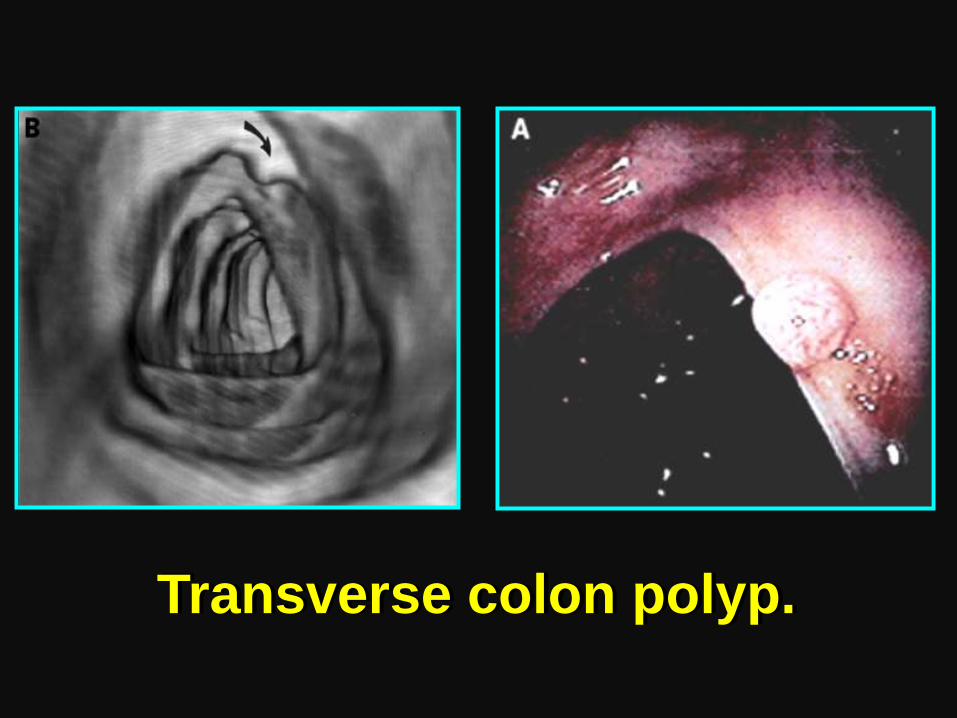
Transverse colon polyp.
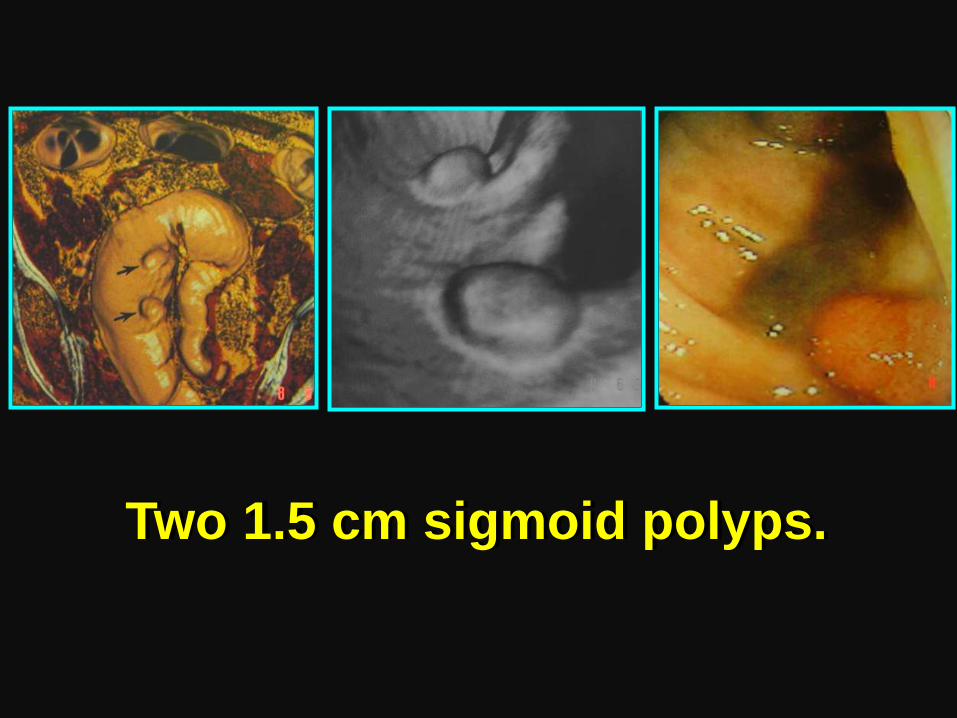
Two 1.5 cm sigmoid polyps.
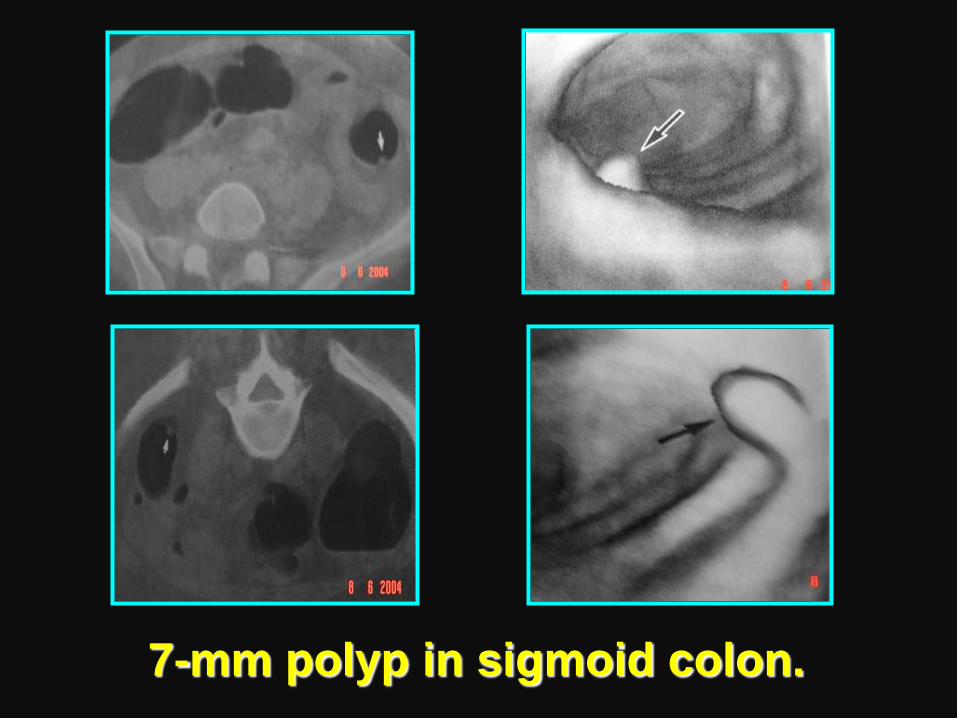
7-mm polyp in sigmoid colon.
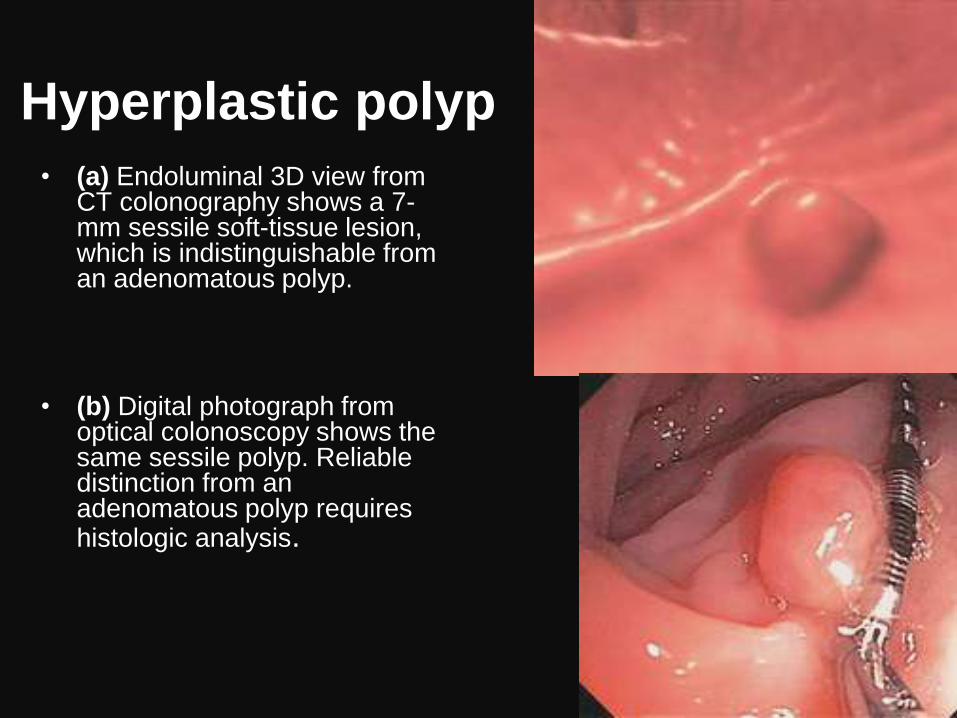
Hyperplastic polyp
• (a) Endoluminal 3D view from CT colonography shows a 7-mm sessile soft-tissue lesion, which is indistinguishable from an adenomatous polyp.
• (b) Digital photograph from optical colonoscopy shows the same sessile polyp. Reliable distinction from an adenomatous polyp requires histologic analysis.
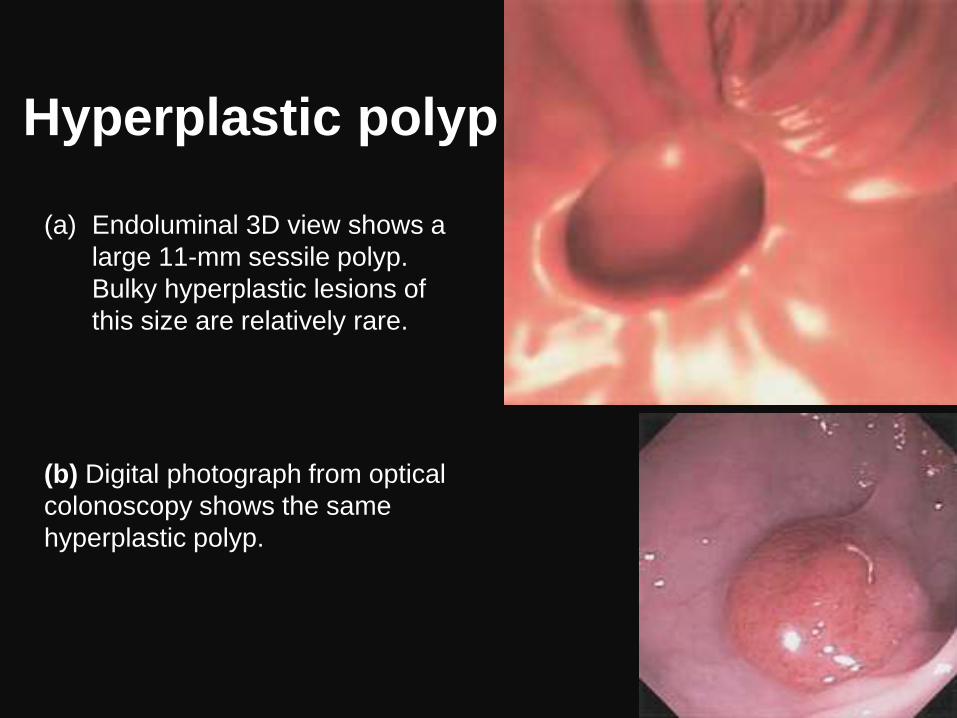
Hyperplastic polyp
(a) Endoluminal 3D view shows a
large 11-mm sessile polyp.
Bulky hyperplastic lesions of
this size are relatively rare.
(b) Digital photograph from optical
colonoscopy shows the same
hyperplastic polyp.
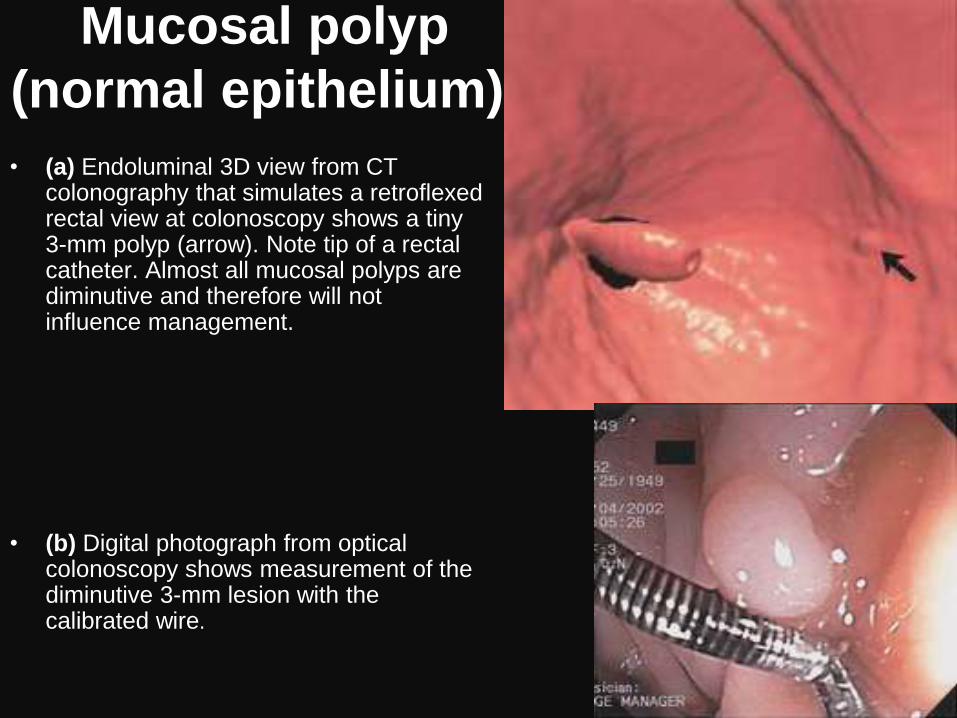
Mucosal polyp
(normal epithelium).
• (a) Endoluminal 3D view from CT colonography that simulates a retroflexed rectal view at colonoscopy shows a tiny 3-mm polyp (arrow). Note tip of a rectal catheter. Almost all mucosal polyps are diminutive and therefore will not influence management.
• (b) Digital photograph from optical colonoscopy shows measurement of the diminutive 3-mm lesion with the calibrated wire.
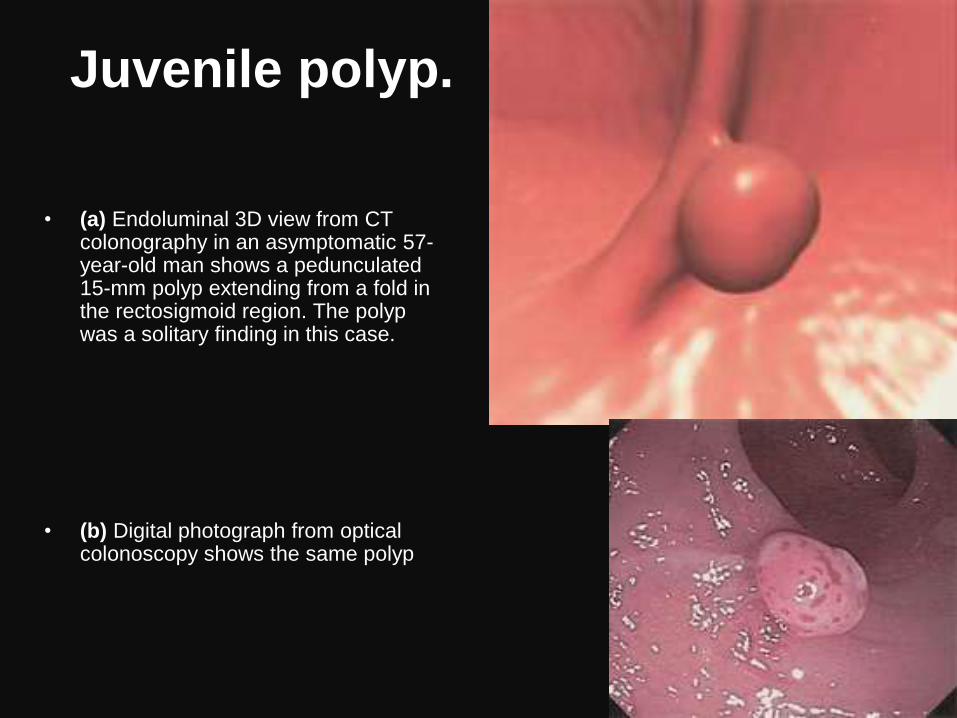
Juvenile polyp.
• (a) Endoluminal 3D view from CT colonography in an asymptomatic 57-year-old man shows a pedunculated 15-mm polyp extending from a fold in the rectosigmoid region. The polyp was a solitary finding in this case.
• (b) Digital photograph from optical colonoscopy shows the same polyp
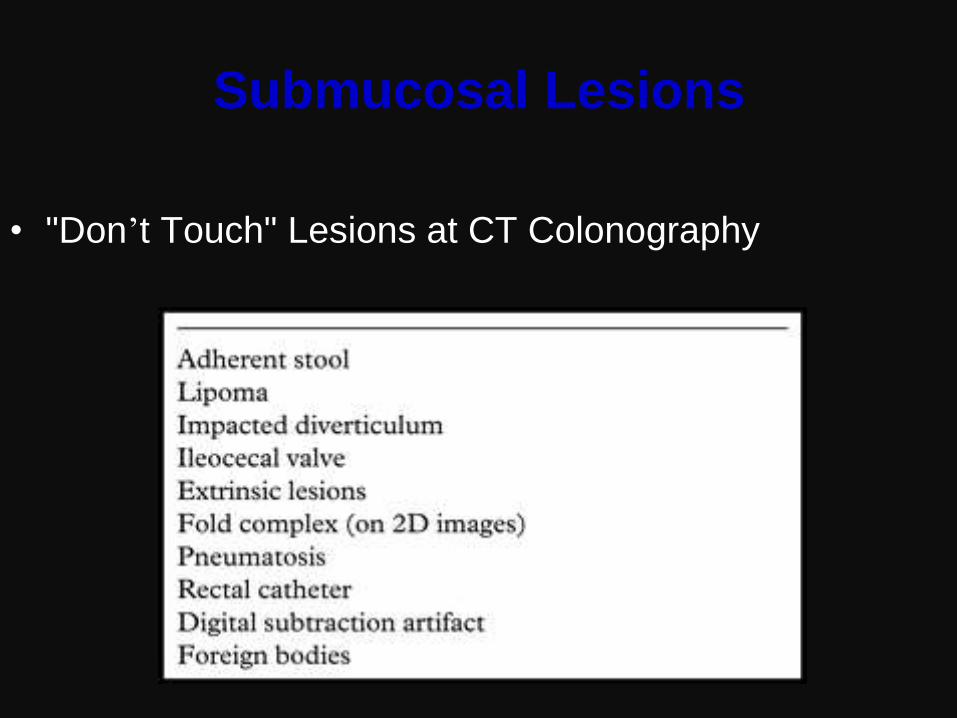
Submucosal Lesions
• "Don’t Touch" Lesions at CT Colonography
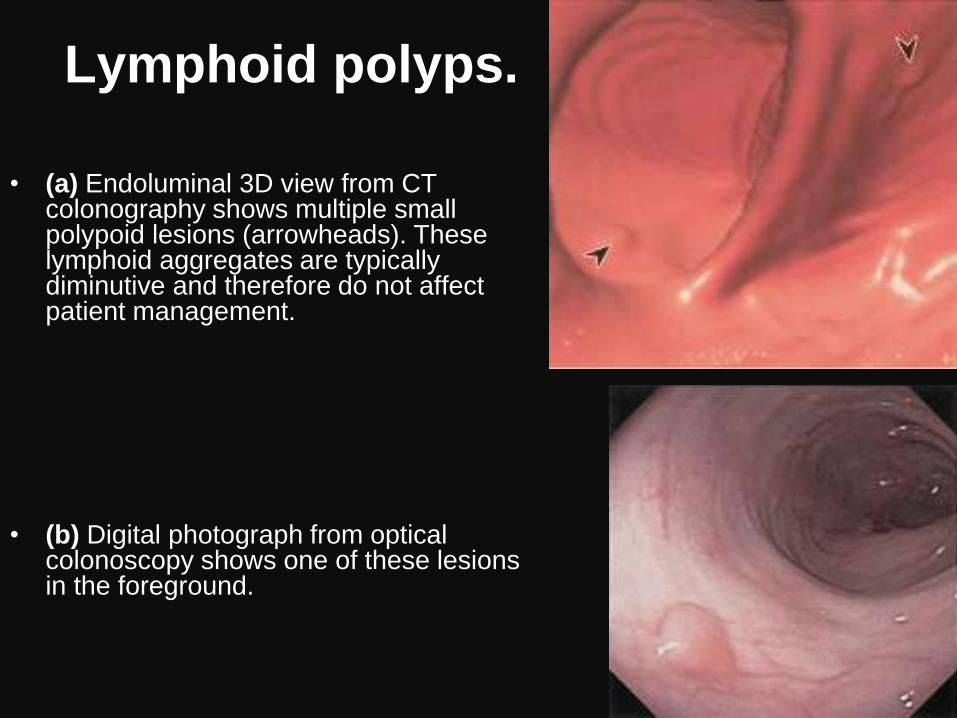
Lymphoid polyps.
• (a) Endoluminal 3D view from CT
colonography shows multiple small polypoid lesions (arrowheads). These lymphoid aggregates are typically diminutive and therefore do not affect patient management.
• (b) Digital photograph from optical colonoscopy shows one of these lesions in the foreground.
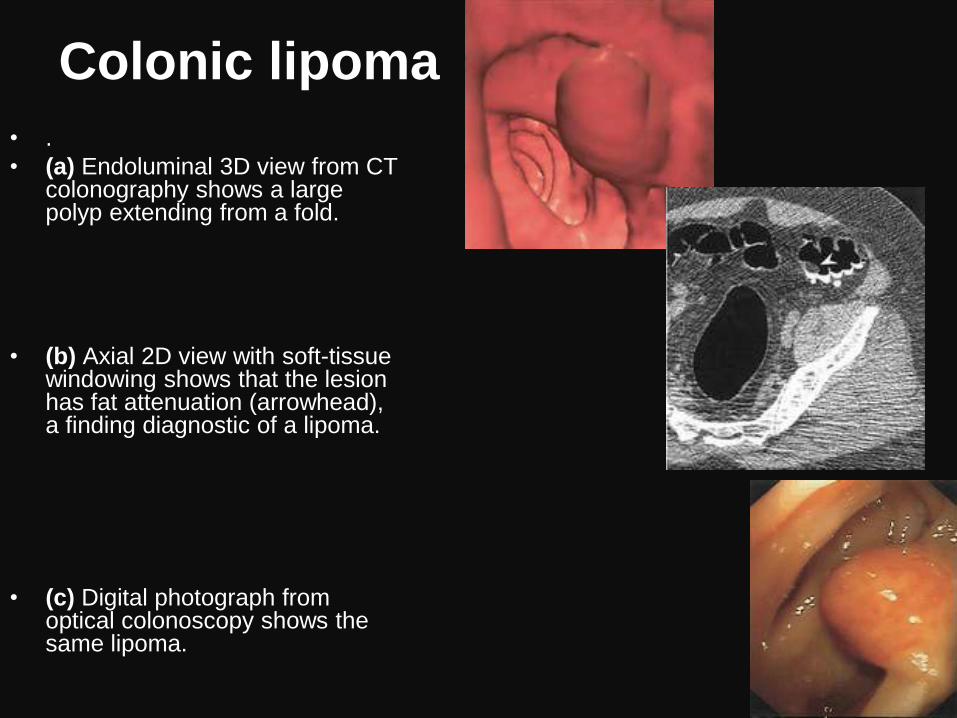
Colonic lipoma
• .
• (a) Endoluminal 3D view from CT colonography shows a large polyp extending from a fold.
• (b) Axial 2D view with soft-tissue windowing shows that the lesion has fat attenuation (arrowhead), a finding diagnostic of a lipoma.
• (c) Digital photograph from optical colonoscopy shows the same lipoma.
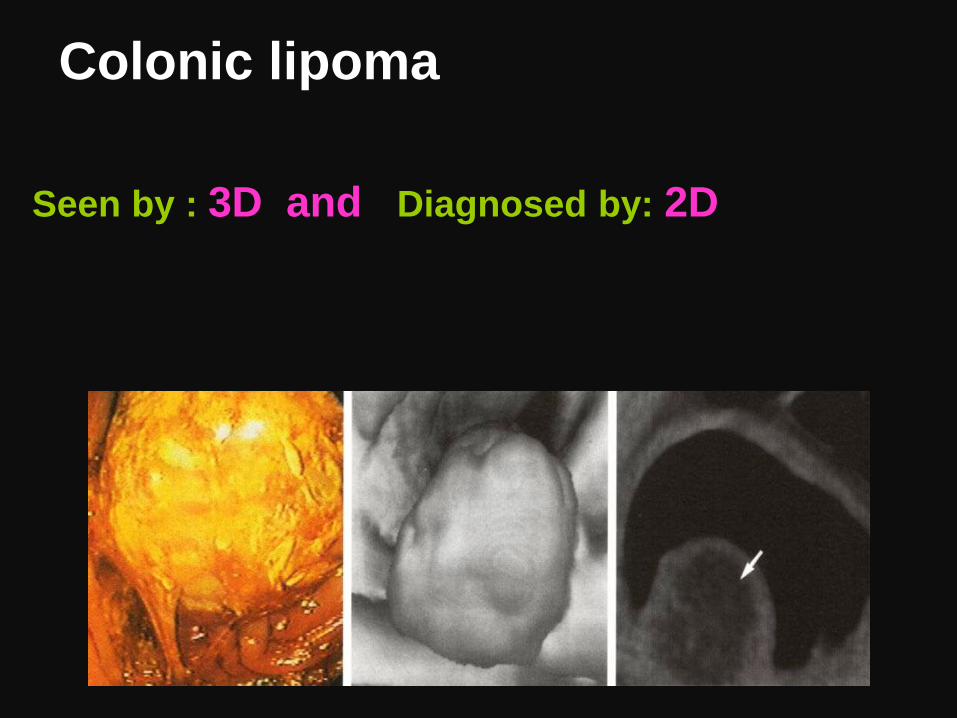
Seen by : 3D and Diagnosed by: 2D
Colonic lipoma
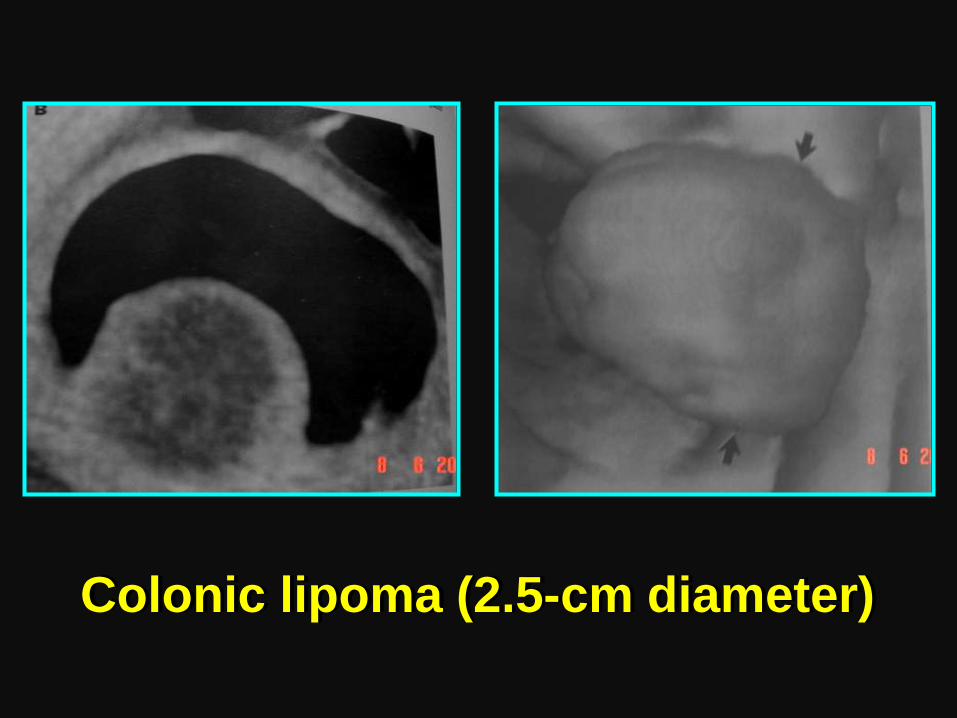
Colonic lipoma (2.5-cm diameter)
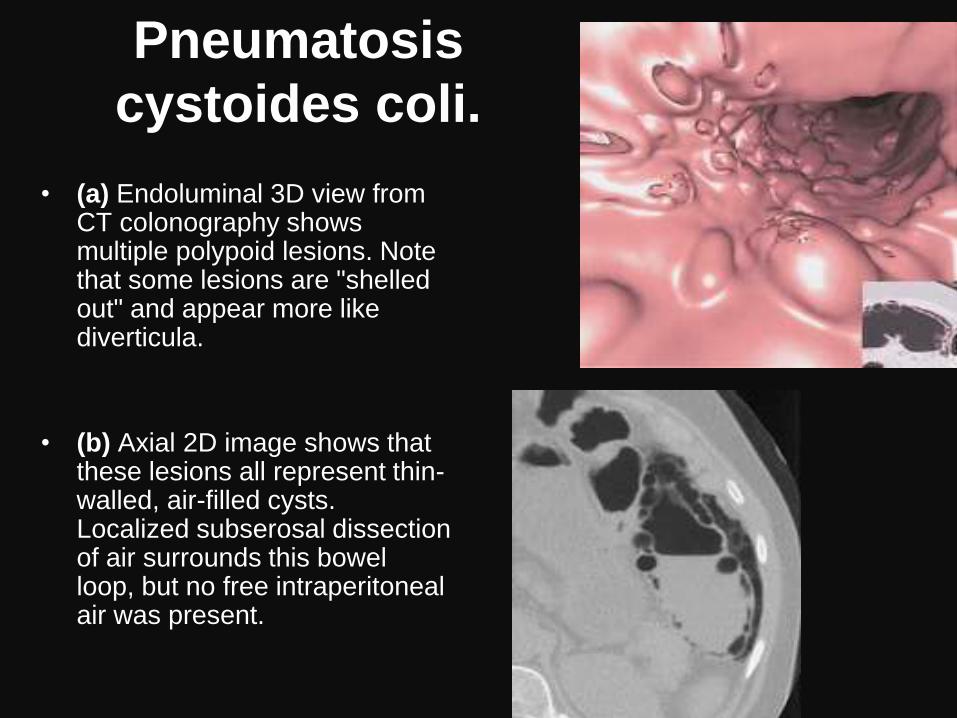
Pneumatosis
cystoides coli.
• (a) Endoluminal 3D view from
CT colonography shows multiple polypoid lesions. Note that some lesions are "shelled out" and appear more like diverticula.
• (b) Axial 2D image shows that these lesions all represent thin-walled, air-filled cysts. Localized subserosal dissection of air surrounds this bowel loop, but no free intraperitoneal air was present.
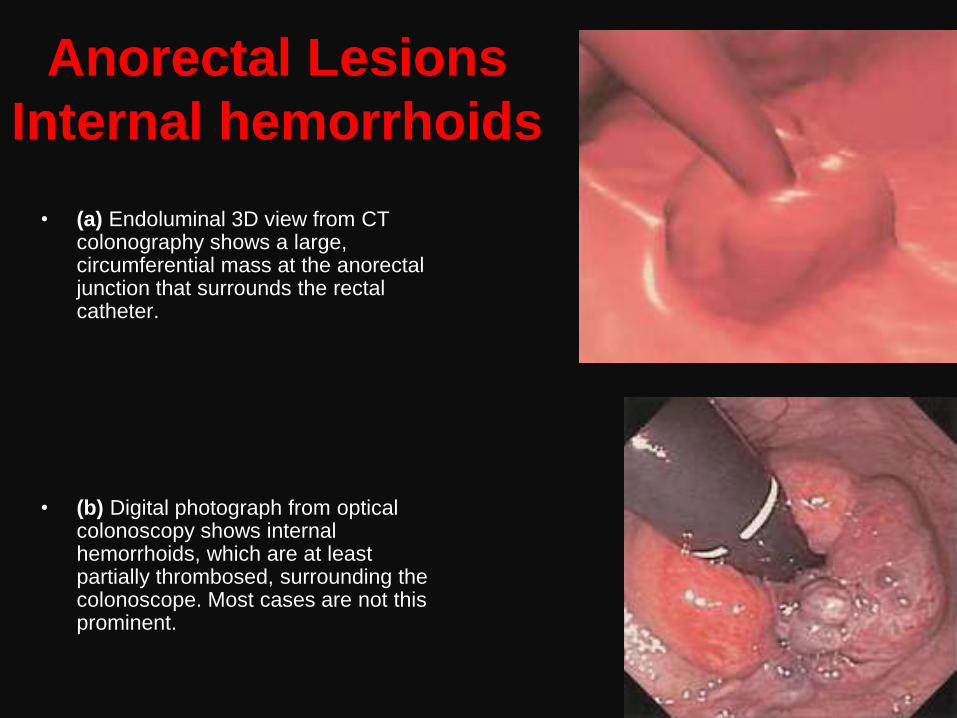
Anorectal Lesions
Internal hemorrhoids
• (a) Endoluminal 3D view from CT colonography shows a large, circumferential mass at the anorectal junction that surrounds the rectal catheter.
• (b) Digital photograph from optical colonoscopy shows internal hemorrhoids, which are at least partially thrombosed, surrounding the colonoscope. Most cases are not this prominent.
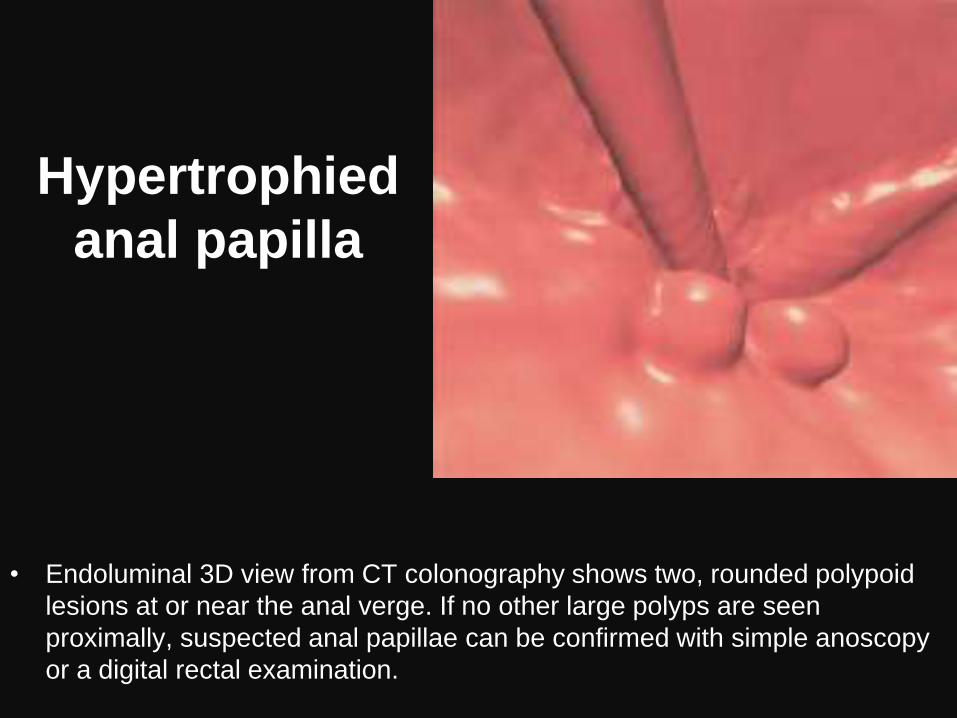
Hypertrophied
anal papilla
• Endoluminal 3D view from CT colonography shows two, rounded polypoid
lesions at or near the anal verge. If no other large polyps are seen
proximally, suspected anal papillae can be confirmed with simple anoscopy
or a digital rectal examination.
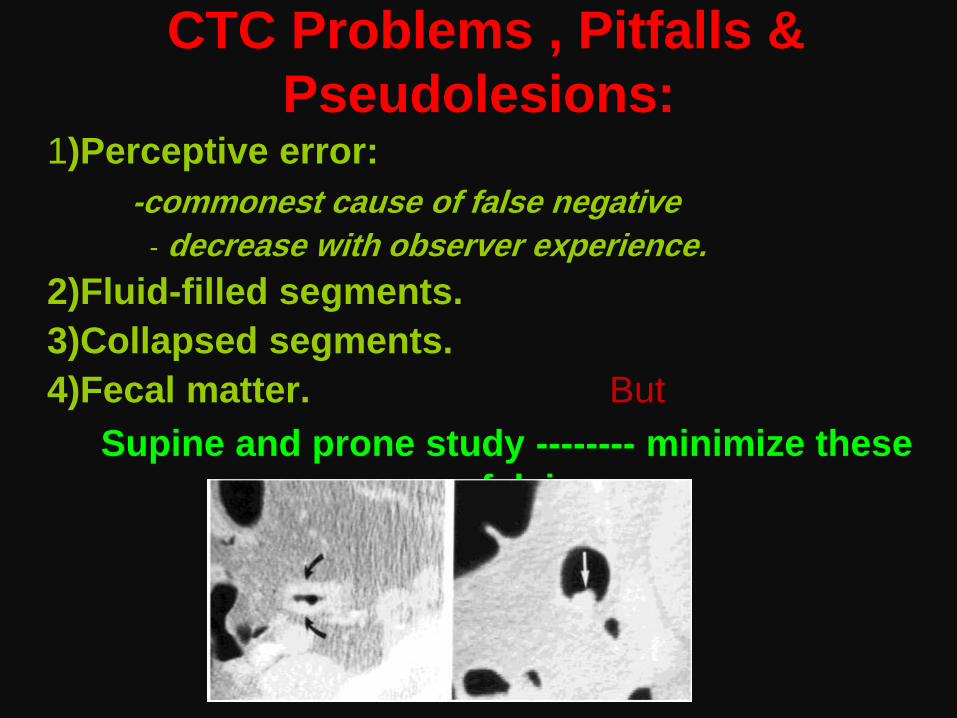
CTC Problems , Pitfalls &
Pseudolesions: 1)Perceptive error:
-commonest cause of false negative
- decrease with observer experience.
2)Fluid-filled segments.
3)Collapsed segments.
4)Fecal matter. But
Supine and prone study -------- minimize these
falsies
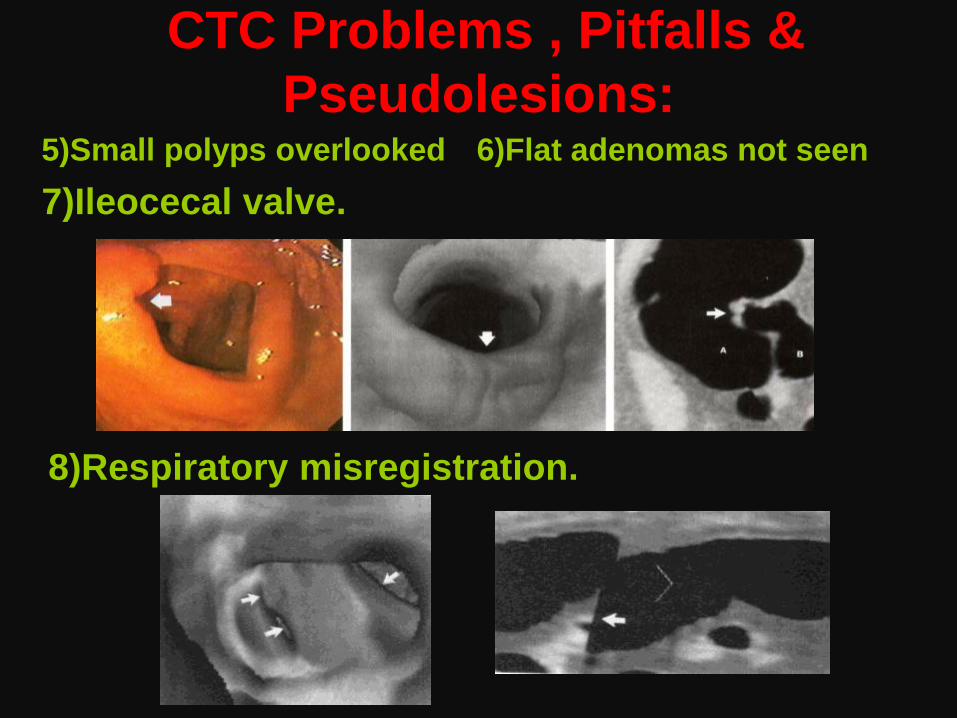
5)Small polyps overlooked 6)Flat adenomas not seen
7)Ileocecal valve.
8)Respiratory misregistration.
CTC Problems , Pitfalls &
Pseudolesions:
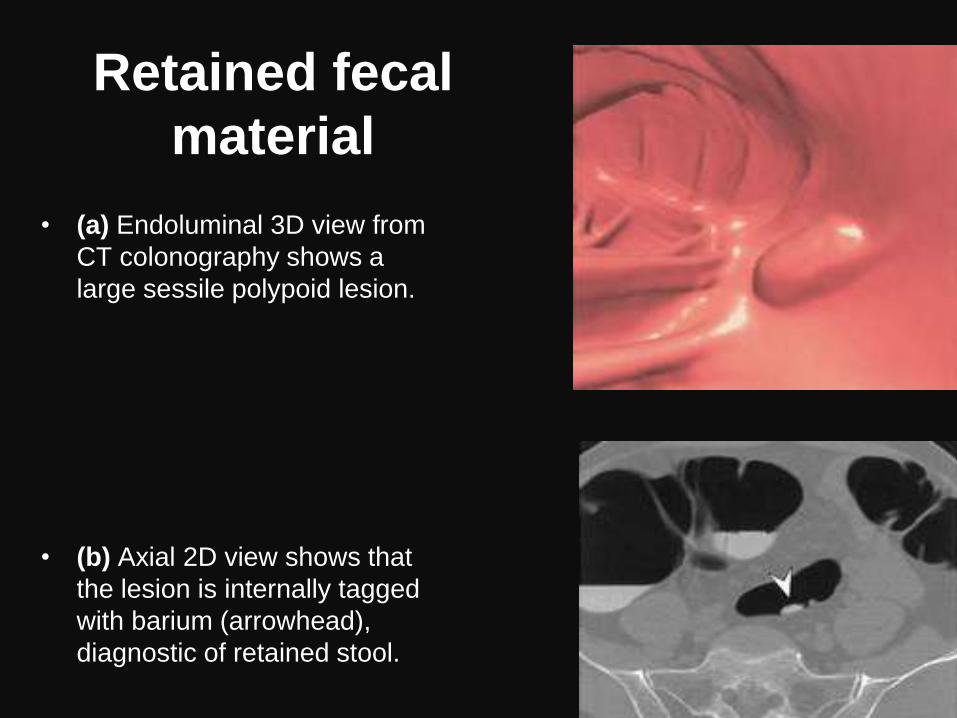
Retained fecal
material
• (a) Endoluminal 3D view from
CT colonography shows a
large sessile polypoid lesion.
• (b) Axial 2D view shows that
the lesion is internally tagged
with barium (arrowhead),
diagnostic of retained stool.
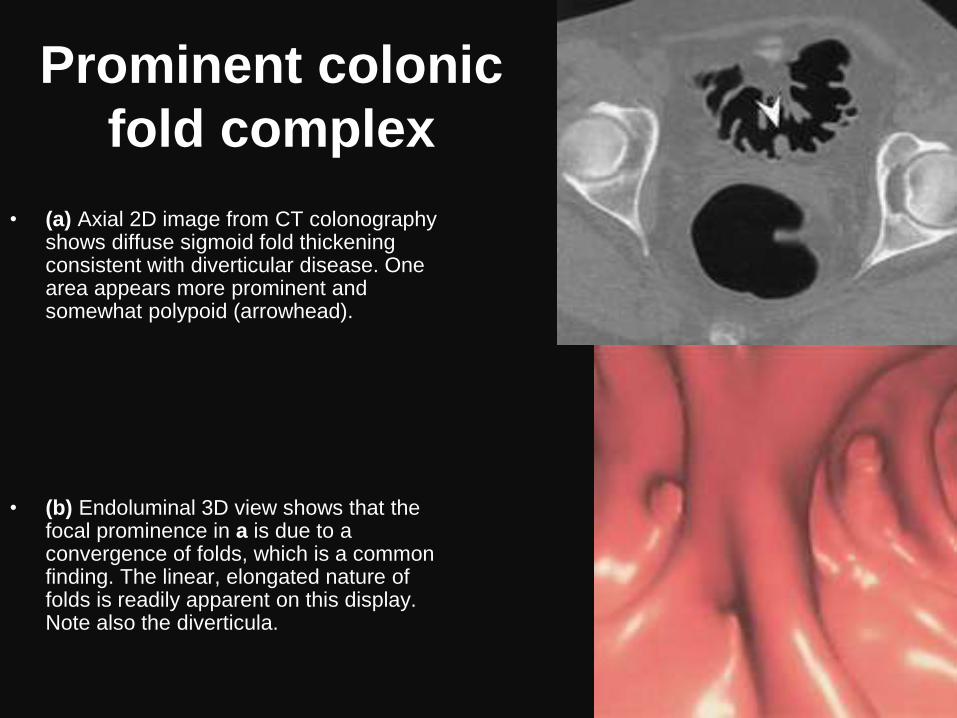
Prominent colonic
fold complex
• (a) Axial 2D image from CT colonography shows diffuse sigmoid fold thickening consistent with diverticular disease. One area appears more prominent and somewhat polypoid (arrowhead).
• (b) Endoluminal 3D view shows that the focal prominence in a is due to a convergence of folds, which is a common finding. The linear, elongated nature of folds is readily apparent on this display. Note also the diverticula.
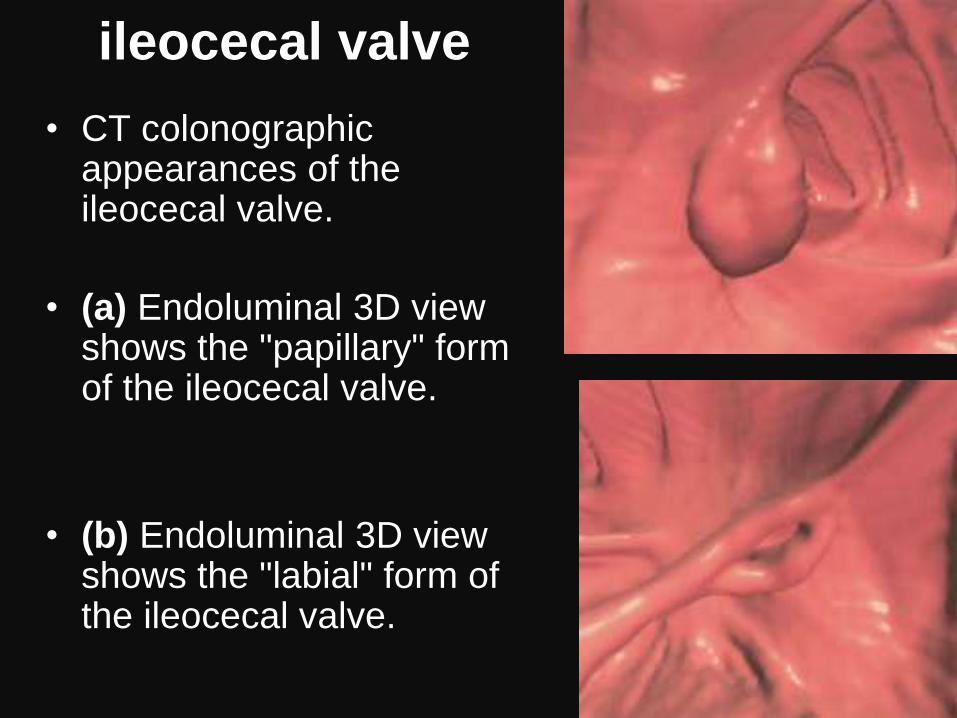
ileocecal valve
• CT colonographic appearances of the ileocecal valve.
• (a) Endoluminal 3D view shows the "papillary" form of the ileocecal valve.
• (b) Endoluminal 3D view shows the "labial" form of the ileocecal valve.

Endoluminal foreign bodies
(medicine capsules).
• Endoluminal 3D view from CT colonography shows two well-circumscribed ovoid lesions that were symmetric in size and morphology. Images from 2D evaluation and 3D translucency rendering (not shown) demonstrated internal heterogeneity with areas of air attenuation internally. A third identical object was identified in the proximal colon. All three foreign bodies were readily mobile and assumed a dependent position on both supine and prone images. Immediately before CT colonography, the patient had undergone incomplete optical colonoscopy, which revealed several undigested shells of sustained-release capsules.
MRC is a promising modality
For help In detecting
Colorectal lesions > 10mm
MR Virtual Colonoscopy
(MRC)
Patients Preparation & Examination
• Standard bowel preparation.
• Rectal enema(H2O+ Gadolinium)
• Patient imaged by :
- 3D spoiled GE -2D single shot FSE
in both Why?
Increase examination accuracy.
Image Display
• 3D Endoluminal (colonoscopic) images.
• 2D Multiplanar reconstruction images. Why ?? For better evaluation of lesion
3D and 2D
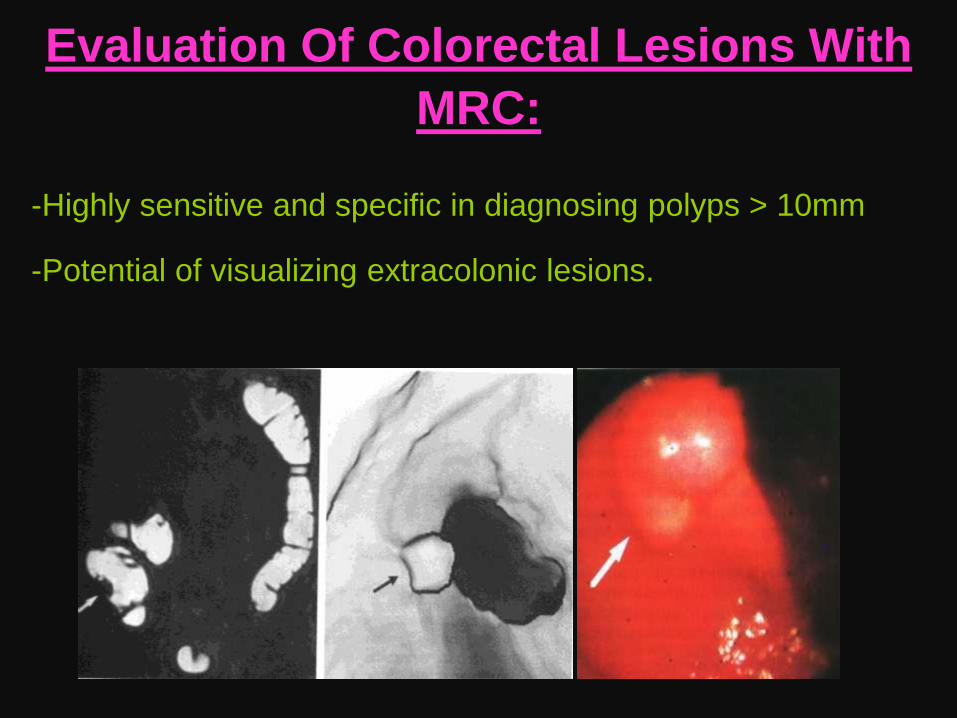
Evaluation Of Colorectal Lesions With
MRC:
-Highly sensitive and specific in diagnosing polyps > 10mm
-Potential of visualizing extracolonic lesions.
MRVC Compared To
CT Colonoscopy (CTC)
Advantages
• No ionizing
radiation
• Direct imaging.
Disadvantages
• High cost ( MRI )
With (Contrast)
MRVC Compared To
Conventional Colonoscopy
Advantages
• No sedation
• No analgesia
• Least
intervention. • (+/-)Extra-luminal
lesion
Disadvantages
• High cost.
• Flat adenoma.
• Small polyp
• No therapy
Virtual Colonoscopy
Current Role
1)Preoperative evaluation of the entire colon:
• Extraluminal lesions.
• Synchronous lesions.
• Land marks to influence surgery.
In colorectal Carcinoma
2)Post operative evaluation of the colon.
3)Post irradiation evaluation of the colon.
Virtual Colonoscopy
Promise
To become a primary method for
colorectal cancer screening and
Return Radiologist to a Major Role In
Colon Cancer prevention