Embed Size (px)
Citation preview

DEPARTMENT OF ORTHOPAEDICSGANDHI MEDICAL COLLEGE, BHOPAL
Seminar On
Presented by :Dr. Radheyshyam
Moderator :- Dr. Atul Varshney- Dr. S. Gaur
Consultants :- Prof. Dr. N. Shrivastava- Dr. Sanjiv Gaur- Dr. J. Shukla- Dr. S. Tandon- Dr. S.A. Farooqui- Dr. A. Varshney- Dr. A. Gohiya- Dr. D. Maravi

Ramesh Kumar, 45 yrs. MaleHistory of RTA
Diagnosis – Fracture Supracondylar Femur Right with Compound Fracture both Bone Leg Left.
Vitals on admission Heart Rate - 88/pm, B.P. – 106/76, R.R. – 17/pm

ACUTE RESPIRATORY DISTRESS SYNDROMEAcute respiratory distress syndrome (ARDS) is a clinical
syndrome of severe dyspnea of rapid onset, hypoxemia, and diffuse pulmonary infiltrates leading to respiratory failure.
Acute lung injury (ALI) is a less severe disorder but has the potential to evolve into ARDS.
ARDS is characterized by –
1. Tachypnea & cyanosis refractive to oxygen therapy.
2. Markedly reduced lung compliance.
3. Diffuse alveolar shadowing on Chest X-Ray.
4. Pulmonary odema, congestion & Hyaline membrane on histological examination.
The first detailed clinicopathological description of ARDS was provided by Ashbaugh and colleagues.
The annual incidences of ALI and ARDS are estimated to be 30/ 100,000 and 10/100,000, respectively.

Etiology : Clinical Disorders Commonly Associated with ARDSDirect Lung Injury Indirect Lung InjuryPneumonia SepsisAspiration of gastric contents Severe traumaPulmonary contusion Multiple bone fracturesNear drowning Flail chestToxic inhalation injury Head trauma
BurnsMultiple transfusionsDrug overdosePancreatitis
Post-cardiopulmonary bypass The most common causes of ALI/ ARDS are sepsis, pneumonia, aspiration of gastric contents, and multiple trauma.

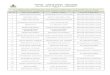
Pathophysiology :The natural history of ARDS is marked by three phases –
exudative, proliferative, and fibrotic – each with characteristic clinical and pathologic features.
Exudative Proliferative FibroticHyaline Interstitial Inflammation FibrosisMembranes Interstitial Fibrosis
Edema
Day : 0 2 7 14 21 ...

Exudative Phase :
In this phase, alveolar capillary endothelial cells and
type I pneumocytes. (alveolar epithelial cells) are injured
leading to the loss of the normally tight alveolar barrier to
fluid and macromolecules. Edema fluid that is rich in protein
accumulates in the interstitial and alveolar spaces.
Alveolar edema dependent portions of the lung
Collapse of the dependent lung decrease lung
compliance intrapulmonary shunting and hyproxemia
increase work of breathing dyspnea.

Proliferative Phase :
This phase of ARDS usually lass from day 7 to day 21.
Most patients recover rapidly and are liberated from
mechanical ventilation during this phase. Histologically, the
first signs of resolution are often evident in this phase with
the initiation of lung repair, organization of alveolar
exudates, and a shift from a neutrophil to a lymphocyte-
predominant pulmonary infiltrate. As part of the reparative
process, there is a proliferation of type II pneumocytes along
alveolar basement membranes. These specialized epithelial
cells synthesize new pulmonary surfactant and differentiate
into type I pneumocytes.

Fibrotic Phase :
Histologically, the alveolar edema and inflammatory
exudates of earlier phases are now converted to extensive
ductal and interstitial fibrosis. Acinar architecture is
markedly distrupted, leading to emphysema-like changes
with large bullae. Intimal fibroproliferation in the pulmonary
microcirculation leads to progressive vascular occlusion
and pulmonary hypertension. The physiologic
consequences include an increased risk of pneumothorax,
reductions in lung compliance, and increased pulmonary
dead space.

CLINICAL FEATURES : The patient develops progressive dyspnea and often non
productive cough usually hours or days after a recognized predisposed condition.
Acute onset progressive Dyspnea Non Productive coughTechypnea Cyanosis Refractive to oxygen therapyHypoxiaAgitation Respiratory Failure
DIAGNOSIS : Because the early features of ARDS are nonspecific high
degree of suspicion is necessary to make a diagnosis.In the majority of patients, the initial diagnosis of
ALI/ARDS is made clinically. Invasive techniques for diagnosis are of limited clinical utility.

DIAGNOSTIC CRITERIA FOR ALI AND ARDSAMERICAN EUROPEAN CONSENSUS CONFERENCE DEFINITION OF ALI & ARDS.
Oxygenation Onset Chest Radiograph Absence of Left AtrialHypertension
ALI : Acute Bilateral alveolar PCWP < 18 mmHg or no Pao2/FIo2 < or interstitial clinical evidence of 300 mmHg infiltrates increased left atrial
ARDS : pressurePao2/Flo2 < 200 mmHg
Note : ALI acute lung injury, PAO2 arterial partial pressure of O2, FIO2 inspired O2 percentage, PCWP pulmonary capillary wedge pressure.

INVESTIGATIONS :
1. Chest X-ray :
Chest radiograph in early stages are usually normal.
Chest X-ray in the initial stages reveals aleveolar &
interstitial opacities involving at least ¾ of the lung. These
characteristics are not specific for ARDS but can be
indinguishable for the cardiogenic pulmonary edema.
Unlike latter however the chest x-ray in ARDS rarely shows
cardiomegaly, pleural effusion or pulmonary vascular
redistribution.

2. Arterial Blood Gases :
In the initial stages ABG analysis shows decreased PCO2 and decreased PAO2 and alkalosis. In the latest stages there is increased PCO2 and decreased PAO2 and acidosis. Ultimately leading to respiratory failure.
3. ECG :
ECG study is essential to rule out any cardiac abnormality.
4. Echo Cardiography :
Echo Cardiography study is normal unless there is some cardiac disease.
5. CT Scan :
CT Scan shows the extensive hetrogenity.

TREATMENT :- The recognition and treatment of the underlying medical and
surgical disorders (e.g. sepsis, aspiration, trauma);- Prophylaxis against venous thromboembolism,
gastrointestinal bleeding, and central venous catheter infections;
- The prompt recognition of nosocomial infections and their treatment.
- Provision of adequate nutrition.- Fluid and Hemodynamic Management :- A reasonable
strategy is to aim to achieve the lowest intravascular volume that maintains adequate tissue perfusion as measured by urine output or other organ perfusion and metabolic acid base status. If organ perfusion cannot be maintained in the setting of adequate intravascular volume, maintained in the setting of adequate Intravascular volume, then administration of vasopressors and/ or inotropes should be used to restore end-organ perfusion.

- Glucocorticoids : Current evidence does not support their use in the care of and ARDS patients. One the other hand, if patients fail to improve after 1 week of supportive therapy and have no contraindications to glucocorticoid therapy, providers may wish to consider an empirical trial of them in an attempt to speed ARDS resolution. There is no data regarding the preference of one steroid over the other.
- Management of Mechanical Ventilation :- Ventilation in volume control mode with a tidal volume of 6 mL/kg predicted body weight plateau pressure less than 30 cm H2O has been shown to improve mortality in ALI/ARDS
compared with a larger tidal volume (12 mL/kg.).
This improvement in survival using the low tidal volume (6ml/kg) represents the most substantial benefit in ARDS mortality demonstrated for any therapeutic intervention in ARDS to date.

A STEPWISE APPROACH TO MECHANICAL VENTILATION IN ARDS
11..
Calculate Calculate predicted body predicted body weight (PBW) in weight (PBW) in KilogramKilogram
Men = 50 + 5.42 [height (cm) – 60]Men = 50 + 5.42 [height (cm) – 60]
Women = 45.5 + 5.42 [height (cm) – 60]Women = 45.5 + 5.42 [height (cm) – 60]
22..
Ventilator modeVentilator mode Volume cycle, assist controlVolume cycle, assist control
33..
Tidal volume Tidal volume (V(VTT))
Initial VInitial VTT 8 mL/kg PBW 8 mL/kg PBW
Reduce to 6 mL/kg over 2 – 4 h if ventilation Reduce to 6 mL/kg over 2 – 4 h if ventilation adequate adequate
Goal inspiratory plateau pressures < 30 Goal inspiratory plateau pressures < 30 cmHcmH22O; reduce VO; reduce VTT to as low as 4 mL/kg as to as low as 4 mL/kg as needed (and permitted by ventilation) to needed (and permitted by ventilation) to achieve this goal.achieve this goal.
44..
Oxygenation Oxygenation Pao goal = 55 – 80 mmHg or pulse oximetry Pao goal = 55 – 80 mmHg or pulse oximetry oxygen saturation 88 – 95%oxygen saturation 88 – 95%
Use the minimal amount of PEEP to keepFIoUse the minimal amount of PEEP to keepFIo22 << 0.6 and meet Pao 0.6 and meet Pao22 goal. goal.
55..
Respiratory rate Respiratory rate and acidosis and acidosis management management
Goal arterial pH = 7.30 – 7.40 Goal arterial pH = 7.30 – 7.40
If pH < 7.30, increase respiratory rate up to If pH < 7.30, increase respiratory rate up to 35 breaths/ min.35 breaths/ min.
If pH < 7.30 and respiratory rate = 35, If pH < 7.30 and respiratory rate = 35, consider starting intravenous bicarbonate (or consider starting intravenous bicarbonate (or equivalent buffer).equivalent buffer).

If the above strategy fails and the patient is suffering from
persistent hypoxemic respiratory failure, consider the
following :
1. Neuromuscular blocking agents (if not already in use)
2. Prone position ventilation
3. Recruitment maneuvers
4. Inverse ratio ventilation, nitric oxide, high- frequency
ventilation, extra corporeal membrane oxygenation, or
partial liquid ventilation as part of a clinical research trial.

PROGNOSIS :Mortality – Recent mortality estimates for ARDS range from 41 to 65%. Mortality in a ARDS is largely attributable to nonpulmonary causes, with sepsis and nonpulmonary organ failure accounting for >80% of deaths. Risk Factors for mortality :
Several risk factors for mortality to help estimate the prognosis have been identified.
Major risk factor for ARDS mortality are non-pulmonary.1. Advanced age > 75 years.2. Sepsis3. Chronic liver disease4. Chronic alcohol abuse5. Chronic immunosupression6. Chronic renal disease7. Non pulmonary organ failure.

Pre-existing organ dysfunction from chronic medical
illness is an important additional risk factor for increased
mortality.
Patient with ARDS from direct lung injury
(Pneumonia, Pulmonary Contusion & Aspiration) have
nearly twice the mortality of those with the indirect causes
of lung injury, while surgical & trauma patient with ARDS
especially those without direct lung injury have a better
survival rate.

COMPLICATIONS :
Complications are common in any critically in patients.
1. Pulmonary embolism
2. Myocardial infarction
3. GI Bleedings
4. Barotrauma : Barotrauma occurs when air dissects out of the air ways or alveolar space into surrounding tissues, leading to pneumothorax, pneumomediastinum, pneumatocele, or sub-cutaneous emphysema. Treatment of barotrauma depends on the location of the extravasated air. Pneumothorax should be considered in any mechanically ventilated patients of ARDS who develops sudden, unexplaned hypoxemia, respiratory distress, or hemodynamic instability. A chest radiograph (preferably upright) is usually sufficient to make the diagnosis, but in many cases there may not be time to obtain one and immediate thoracostomy is essential to save life.

5. Nosocomial Pneumonia : The incidence of nosocomial pneumonia in the ARDS patients is estimated to be from 15% to 60%. There is no consensus regarding the appropriate way to diagnose nosocomial pneumonia in the mechanically ventilated patient. Because patients with ALI/ARDS frequently die of uncontrolled infection, recognition, although notably difficult and treatment of nosocomial pneumonia is an important part of caring for the ALI/ARDS patient. Clinical criteria that are commonly used in the diagnosis includefever, elevated white blood cell count,purulent secretions, andpulmonary infiltrates.Regardless of the methods used for diagnosis, early appropriate empirical therapy is the mainstay of treatment for nosocomial pneumonia.

6. Multiorgan System Dysfunction : Although ALI and
ARDS are often thought of as primary pulmonary
disorders, evidence is accumulating to suggest that they
are systemic disorders with many similarities to sepsis or
SIRS. Multiorgan system dysfunction is a common
complication in ALI/ARDS, Organ dysfunction may result
from the underlying cause of ALI/ARDS, such as sepsis, or
occur independently.

7. Neuromuscular Weakness : Patient of ARDS are at high risk for developing the neuromuscular weakness that persists after resoulation of ARDS and can complicate weaning from the mechanical ventilation and rehabilitation. These clinical syndromes are commonly called critical illness polyneuropathy but actually have components of neuropathy and myopathy that can coexist or occur separately. Prolonged muscle weakness is most common in critically ill patients who are treated with glucocorticoids. In the absence of compelling clinical indication such as underlying connective tissue disease the use of glucocorticoid should not be routine.
FUNCTIONAL RECOVERY IN ARDS SURVIVORS :
Majority of patients of ARDS survivors recover nearly normal lung function. Patients usually recover their maximum lung function within 6 months.

FAT EMBOLISM SYNDROME
Fat embolism syndrome (FES) is a clinical entity first
described over 150 years ago by Bergmann. It is very
important to differentiate FES, a complex with potentially
catastrophic cardiopulmonary and cerebral dysfunction,
from fat embolization, a far more common and often
subclinical entity.
Incidence of fat embolism in polytrauma patients is
90%.
Incident of the FES is 1 – 3% in the patients with a
single major fracture.

Causes :
Fractures of the long bone.
Pelvic Trauma,
Intramedullary nailing of long-bone fractures,
Hip arthroplasty, and knee arthroplasty.
Sickle cell disease,
Acute pancreatitis
Decompression sickness
Total parenteral nutrition.
Most common cause of FES is fractures of the long bones.
Intramedullary orthopedic surgeries are the most common iatrogenic cause of FES.

PATHOPHYSIOLOGY :
In the initial phase, fat and marrow are displaced from the bones, enter the venous system, and travel through the heart to enter the lungs. There the emboli may cause shunting, severe hypoxemia, and right ventricular dysfunction.
The secondary phase may involve inflammatory mediators responsible for the interstitial edema or acute respiratory distress syndrome that may ensue.
CLINICAL FEATURES :
The principal clinical features of fat embolism syndrome are:
Respiratory Failure
Cerebral dysfunction
Petechiae

FES is most common after the 24-72 hrs. of the inciting cause

Fat embolism syndrome : above with clinical pattern of symptoms/signs; 24-72 hrs after insult:- Petechial Rash - head, neck, anterior thorax, subconjunctiva, axillae – 20-50% of cases- Respiratory – tachypnea, dyspnea, b/l crackles, hemoptysis, bilateral infiltrates, ARDS- Neurological signs – confusion, drowsiness, coma – may
resolve- Fever- Cardiovascular: tachycardia, hypotension- Retinal changes (fat or petechiae - Purtscher’s retinopathy)- Jaundice- Renal (anuria or oliguria)- Hematological
o Thrombocytopenia (>50% decrease)o Anemia (>20% decrease)o ESR >71 mm/h

DIAGNOSIS :The diagnosis of FES remains one of exclusion. A number of
authors have suggested clinical criteria for diagnosing FES. Gurd’s Criteria for the diagnosis of FES
Table-I : Gurd's Criteria
Major Criteria Petechial rash(One necessary for diagnosis) Respiratory
insufficiencyCerebral involvement
Minor Criteria (One necessary for diagnosis) Tachycardia > 120 beats/ min
Fever > 39.4°CRetinal signs – fat or petechiaeJaundiceRenal signs – anuria or oliguria
Laboratory Findings Thrombocytopenia(One necessary for diagnosis) Anemia
High ESRFat macroglobulinemia

FES Doesn't occur before 12 Hrs. and after 2 weeks of the inciting cause.
Table-II : Schonfeld's Criteria
Petechiae 5
Chest X-ray changes 4(Diffuse alveolar infiltrates)
Hypoxemia (PaO2 <9.3 kPa) 3
Fever (<38°C) 1
Tachycardia (>120 beats/ min) 1
Tachypnea (>30 breaths/ min) 1
Confusion 1
Cumulative score > 5 required for diagnosis

LABORATORY STUDIES
There is no pathognomic test during the course of a Fat
Embolic Syndrome, but a high index of suspicion is helpful in
diagnosis. Close observations should be kept for the clinical
signs and symptoms of Fat Embolic Syndrome on any
patient at risk. However, some investigations can be helpful
in conjunction with the clinical features.
1. ABGs
ABGs may show a low PaO2 and PaCO2 with a
respiratory alkalosis in the early stages but in later stages
hypoxemia and hypercapnia with respiratory acidosis may be
prominent feature due to diffusion defects.

2. Urine and Sputum Examination.
Samples may contain fat globules but these tests are non-specific.
3. Haemotological Tests.
During the acute phase of Fat Embolic Syndrome, there may be increase in FDPs, positive D-Dimer test, thrombocytopenia and other coagulation abnormalities. Patients often have a mild anemia.
4. Biochemical tests
Liver and renal function tests should performed. Serum electrolytes are mandatory. Hypocalcemia may be present due to saponification of the circulating unbound free fatty acids.

IMAGING STUDIES :
1. X-ray chest
The classical chest x-ray of fat embolism syndrome shows multiple flocculent shadows (snow storm appearance). However, the spectrum includes a diffuse, ground glass appearance or military dissemination of very fine shadows. Later, the picture may be complicated by infection or pulmonary edema.
2. Echocardiography
Transesophageal echocardiography has been used to detect fat embolism in patients who are undergoing invasive intramedullary procedures.

3. CT Scan Brain.
CT Scan brain (plain) may be normal or may reveal diffuse white-matter petechial haemorrhages consistent with microvasvular injury.
4. Spiral CT Scan chest.
Helical CT Scan chest may be normal as the fat droplets are lodged in capillary beds. Parenchymal changes consistent with lung contusion. Acute lung injury, or ARDS may be evident.
5. MRI
Scant data exist regarding MRI findings in patients with fat embolic syndrome.

TREATMENT : Mainstay of treatment in supportive. - Cardiovascular therapy including maintaining adequate
preload and positive inotropy is necessary to preserve cardiac output.
- For hypoxemia 100% oxygen via an endotracheal tube.- Other therapeutic regimens used after the development of
FES including heparinization, dextran, and parenteral ethanol cannot be recommended.
- Prophylactic corticosteroid therapy may minimize the incidence of FES.
- If possible, it is best to delay all but emergency surgery in trauma patients who develop FES until the syndrome has progressed to its full severity and stabilized or improved.
- An exception is the patient who requires fixation of fractures to halt continuing fat embolization.

Deterrence/Prevention:
Early immobilisation of fractures seems to be the
most effective way of reducing the incidence of this
condition.
Corticosteroids as prophylaxis for fat embolism syndrome
Several studies have demonstrated varying results using
corticosteroids, usually methylprednisolone, in patients
identified as being at high risk for the syndrome.
Although the data appear compelling, the optimal timing,
duration, and dose of steroids are undetermined.

DoseDose ModelModel TimingTiming Duration Duration of Studyof Study
Effect on Effect on Disease Disease IncidencIncidenc
ee
30 mg/kg30 mg/kg DogDog Pre-eventPre-event 60 min60 min NoneNone
10 mg/kg q8h for 10 mg/kg q8h for 24 h24 h
Human Human traumatrauma
At At admissionadmission
No dataNo data DeclininDecliningg
7.5 mg/kg q6h for 7.5 mg/kg q6h for 12 h or placebo12 h or placebo
Human Human traumatrauma
Within 12 Within 12 hh
2 d2 d DeclininDecliningg
PROGNOSIS :
The mortality rate from fat embolism syndrome is 5 to 15%. Even severe respiratory failure associated with fat embolism seldom leads to death.
The prognosis is worse in older patients and those with more severe injury but is not affected by gender.
Results of Randomized Controlled Trials of Corticosteroids in the Prevention of Fat Embolism Syndrome

MEDICAL/LEGAL PITFALLS:
Assuming altered mental status, fever, and hypoxia are due to fat embolism, the lack of a search for treatable or life-threatening disorders before making the diagnosis may lead to litigation if such a disorder is discovered later.
CT scan of the head is necessary to rule out intracranial pathology.
A careful search for infectious agents and possibly the institution of empiric antibiotics are necessary until an infectious source is ruled out.
Judicious use of crystalloids, colloids, and diuretics is necessary; volume depletion may precipitate shock and organ dysfunction, but volume overload may worsen the hypoxia.

EFFECT OF INTRAMEDULLARY NAILING :
Fat embolism due to IM nailing was discribed by
Kuntscher. He recommended the avoidance of nailing
after trauma in cases with severe injuries or when fat
embolism was already present. The incidence of fat
embolism depends on which bone is involved most
commonly with the femur.

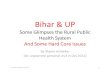
In randomised clinical study unreamed nailing was associated with a lower rate of pulmonary complications but differences was not statistically significant. IM instrumentation
Rise of IM pressure
Liberation of bone marrow contents in blood
Bone marrow contents in Lungs
Increase pulmonary arterial pressure
Decreased oxygenation & ARDS

TIMING OF FRACTURE FIXATION IN POLYTRAUMA PATIENTS :
In multiple injured patients with two sever injuries benefits of IM nailing of femoral fractures in 1st 48 hours is well established. But this should be avoided in patients who are at the risk for SIRS and organ dysfunction which include the patients with shock & sever pulmonary injuries and selected patients of sever CNS trauma when it is determined that surgery may lead to hypoxia and hypotension, that would extend the primary brain injury. Early temporary fixation is done with the external fixator in these cases to decrease the immune system stimulation leading to the SIRS. Conversion from the external fixator to the nailing is done after 4 days this duration is appropriate to allow for the reduction in inflammatory response to the initial injury.

BIBLIOGRAPHY
1. Harrison's – Principles of Internal Medicine.
2. Crouftan and Douglas – Text Book of Respiratory
Medicine.
3. Wylie's – Text Book of Anesthesia.
4. Fink's – Principles of Critical Care.