Embed Size (px)
Citation preview

David Wilson, MD• Electrophysiologist at the
CardioVascular Group/Gwinnett Medical Group
• Board Certified in Internal Medicine, CardiovascularDiseases, and Electrophysiology
• Special interests include
electrophysiology, pacemakers, and RF ablations
Fellowship: Harbor-UCLA
Medical Center
Residency:Harbor-UCLA Medical
Center
Medical School:Indiana University

David A. Wilson, M.D.
EARLY AF DETECTION & STROKE PREVENTION UTILIZING AUTOMATIC DAILY
DEVICE MONITORING.

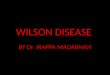
STROKES ATTRIBUTABLE TO AF - FRAMINGHAM
50-59 60-69 70-79 80-890
5
10
15
20
25
AF prevalenceEvents attributable to AFColumn1
Wolf et al. Stroke 1991;22:983-988.
Age
%

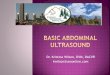
Hart RG et al. Ann Intern Med. 2007;146:857-867.
Study Year
AFASAK I 1989; 1990
SPAF I 1991
BAATAF 1990
CAFA 1991
SPINAF 1992
EAFT 1993
All trials (n=6)N=2,900
Relative Risk Reduction(95% CI)
Favors Warfarin Favors Placeboor Control
100% 50% 0 -50% -100%
Adjusted-dose warfarin comparedwith placebo or control
EFFICACY OF WARFARIN(COMPARED WITH PLACEBO OR CONTROL IN SIX STUDIES)

CASE STUDY• 64 year old male
• History of hypertension, type 2 DM
• Symptomatic bradycardia 2/2013 with subsequent pacemaker implantation 2/10/2013

ROUTINE OFFICE FOLLOW-UP• Feels well with no palpitations, active.
• Current medications metformin, lisinopril and atorvastatin and aspirin.
• BP 125/75, paced at 60 bpm.
• Pacemaker check shows normal function.
• Atrial high rate activity lasting 2 hours 11 months ago. Multiple brief episodes lasting <10 minutes

HOW WOULD YOU MANAGE THE PATIENT?A. Start amiodarone and follow for recurrent AF
B. Start aspirin and clopidogrel
C. Start NOAC or warfarin
D. Intensify monitoring

RISK ASSESSMENT
Fridberg, Eur Heart J 2012; 33:1500

TRENDS STUDY• Prospective observational study in CRM implanted patients
• Defined AF burden as longest 1 day duration in past 30 days
• Compared stroke risk in patients who in prior 30 days had:
• no AF vs AF< 5.5 hrs max/day to AF > 5.5 hrs on any of prior 30 days
• Alternative comparison is total duration AF prior 30 days with 10.8 hours cut point
Circulation: Arrhythmia and Electrophysiology 2009; 2: 474

TRENDSMETHODOLOGY
Circulation: Arrhythmia and Electrophysiology 2009; 2: 474

• 2486 patients from 116 centers, means age 71, mean CHADS2 2.2
• 53% of patients had no AF
• p 0.06 for High AF vs zero AF
TRENDS - Results TRENDS - Results
Circulation: Arrhythmia and Electrophysiology 2009; 2: 474

ASKING AGAIN, WHAT WOULD YOU RECOMMEND?• Start amiodarone and follow for recurrent AF
• Start aspirin and clopidogrel
• Start NOAC or warfarin
• Intensify monitoring

ASSERTStudy Design
-3 0 3 9 15 21 27 33 39 45 51 57
Months
Enrolled 0-8 wks
post implant
Mininum Follow up 1.75 yrsMaxmum Follow Up 5 yrsMean Follow Up 2.8 yrs
ArrhythmiaDetection
Follow Up Period
Primary Outcome: Ischemic Stroke or Systemic Embolism
Visits
Prospective Cohort DesignTo determine if device-detected atrial tachyarrhythmias are associated with anincreased risk of stroke or embolism?
Asymptomatic Atrial Fibrillation and Stroke Evaluation in Pacemaker Patients and the Atrial Fibrillation Reduction Atrial Pacing Trial

ASSERT: STUDY RESULTS
• 2580 patients enrolled following implant of first pacemaker or ICD (St. Jude Medical)• 2451 pacemaker, 129 ICD patients
• 136 participating centres, 23 countries
• Mean follow up 2.8 yrs
• 36% of patients had at least one device-detected atrial tachyarrhythmia• >6 min, >190 bpm; at mean FU of 2.8 years
• Cumulative rate of VKA use <2% per year

TIME TO FIRST DEVICE-DETECTED ATRIAL TACHYARRHYTHMIA > 6 MIN, >190 BPM
Years of Follow-up
Cum
ulat
ive H
azar
d Ra
tes
0.0
0.1
0.2
0.3
0.4
0.5
0.6
0 0.5 1.0 1.5 2.0 2.5 3.0 3.5 4.0
# at Risk Year 0.5 1.0 1.5 2.0 2.5 3.0 3.5 4.02580 2059 1842 1663 1371 1008 706 446 243
ASSERT : Time to Adjudicated AHRE(>6 minutes,>190/minute)
3 month Visit

BASELINE CHARACTERISTICSDevice-Detected Atrial Tachyarrhythmia before
3 Month Visit P-Value
NoN = 2319
YesN = 261
Age (years) (mean ± SD) 76.3 ± 6.7 77.0 ± 6.8 0.13
Male 58.7% 54.9% 0.27
History of Prior Stroke 7.2% 6.9% 0.84
History of Heart Failure 14.4% 14.9% 0.83
History of Diabetes Mellitus 29.1% 22.6% 0.03
History of Myocardial Infarction 18.4% 12.3% 0.01
CHADS2 score (mean ± SD) 2.26 ± 1.02 2.21 ± 1.11 0.47
Sinus Node Disease 42% 50% 0.01
Heart Rate 70.0 ± 11.6 67.7 ± 11.7 0.001
Systolic BP (mm Hg) 136.5 ± 20 137.2 ± 20 0.60
Baseline use of ASA 61.7% 61.3% 0.91
Baseline use of Clopidogrel 10.7% 9.6% 0.56

ASSERT: ISCHEMIC STROKE OR SYSTEMIC EMBOLISM
Years of Follow-up
Cum
ulat
ive H
azar
d Ra
tes
0.0
0.02
0.04
0.06
0.08
0.10
0 0.5 1.0 1.5 2.0 2.5
# at Risk Year 0.5 1.0 1.5 2.0 2.5+_ 261 249 238 218 178 122
2319 2145 2070 1922 1556 1197
RR=2.4995%CI 1.28-4.85P=0.007 Device-Detected Atrial Tachyarrhythmia
Detected 0-3 months
No Asymptomatic Atrial Tachycardia Detected 0-3 months
T0 at 3-month visit

PRIMARY AND OTHER CLINICAL OUTCOMES
Event
Device-Detected Atrial Tachyarrhythmia Device-Detected Atrial
Tachyarrhythmia Present vs. absentAbsent
N=2319PresentN= 261
events %/year events %/ year RR 95% CI p
Ischemic Stroke or Systemic Embolism 40 0.69 11 1.69 2.49 1.28 – 4.85 0.007
Vascular Death 153 2.62 19 2.92 1.11 0.69 – 1.79 0.67
Stroke / MI / Vascular Death 206 3.53 29 4.45 1.25 0.85 – 1.84 0.27
Clinical Atrial Fibrillation or Flutter 71 1.22 41 6.29 5.56 3.78 – 8.17 <0.001

CLINICAL OUTCOMES BY CHADS2
CHADS2
ScoreTotal Pts.
Sub-clinical Atrial Tachyarrhythmia between enrollment and 3 months Sub-clinical Atrial
TachyarrhythmiaPresent vs. absentPresent Absent
Pts. events %/year Pts. event
s %/year HR 95% CIP
(trend)
1 600 68 1 0.56 532 4 0.28 2.11 0.23 – 18.9
0.352 1129 119 4 1.29 1010 22 0.77 1.83 0.62 – 5.40
>2 848 72 6 3.78 776 18 0.97 3.93 1.55 – 9.95

ASSERT - DURATION OF EPISODES
Duration of AT >190 bpmQuartile analysis
Ischemic stroke or TEAT present vs absentRR 95% CI
6 min – 0.86 hour 1.23 0.15-4.46
0.87 – 3.63 hours 0 0-2.08
3.64 – 17.72 hours 1.18 0.14-4.28
> 17.72 hours 4.89 1.96-10.07

TRENDS COMPARED TO ASSERT• Similar events 51/2486 in TRENDS vs 59/2580 ASSERT
• Similar CHADS2 score, 2.2 both trials
• Older age in ASSERT (76 vs 71)
• Fewer males in ASSERT (58% vs 66%)
• More AF in TRENDS than ASSERT (47% vs 36%)
• TRENDS did not exclude prior clinical AF patients with 20% prior history
• 21% on warfarin at entry
• Both studies had relatively low event rates

ASSERT: RELATIONSHIP BETWEEN AHRE AND STROKE
• In ASSERT, 59 patients had stroke or SE
• 30 had no AHRE
• 9 had AHRE but only AFTER their stroke
• 20 patients had at least one AHRE > 6 minutes prior to their stroke or SE
• 3 developed persistent AF at least one month before, but only recognized clinically in 1 pt.
• 2 patients had 9-day long episodes 1-2 weeks prior
• 1 patient had 2.7 hour episode beginning 48 hours prior
• None of remaining 14 pts. had ANY AHRE > 6 minutes in 30 days before stroke or SE

Michela Brambatti et al. Circulation. 2014;129:2094-2099Copyright © American Heart Association, Inc. All rights reserved.
SUMMARY OF SUBCLINICAL ATRIAL FIBRILLATION (SCAF) OCCURRING WITHIN 1 YEAR OF STROKE OR SYSTEMIC EMBOLISM.

TRENDS COMPARED TO ASSERT• Similar events 51/2486 in TRENDS vs 59/2580 ASSERT
• Similar CHADS2 score, 2.2 both trials
• Older age in ASSERT (76 vs 71)
• Fewer males in ASSERT (58% vs 66%)
• More AF in TRENDS than ASSERT (47% vs 36%)
• TRENDS did not exclude prior clinical AF patients with 20% prior history
• 21% on warfarin at entry
• Both studies had relatively low event rates
• TRENDS followed event windows, not patients

STROKE SEVERITY IN ASSERT
Healey, HRS 2015

WHAT IS THE CAUSE OF STROKE IN AF• Virchow stated 3 potential contributors
1. Abnormalities in blood flow
2. Abnormalities in the blood vessel wall
3. Interaction with blood constituents
• Atrial dilation, scarring and reduced contractility 1, 2
• CHF and mitral stenosis 1
• Spontaneous echo contrast 1
• Hypercoagulable state: increased platelet activation, thrombogenesis, endotheliial dyfunction 2, 3
• Atrial remodeling: AF begets AF
• Hypertension, DM, Age contribute to abnormal blood flow, atrial dilation, scarring and/or endothelial dysfunction
• Some of the abnormalities promoting AF may independently increase stroke risk without AF, so SCAF can serve as a risk marker

CLINICAL OUTCOMES BY CHADS2
CHADS2
ScoreTotal Pts.
Sub-clinical Atrial Tachyarrhythmia between enrollment and 3 months Sub-clinical Atrial
TachyarrhythmiaPresent vs. absentPresent Absent
Pts. events %/year Pts. event
s %/year HR 95% CIP
(trend)
1 600 68 1 0.56 532 4 0.28 2.11 0.23 – 18.9
0.352 1129 119 4 1.29 1010 22 0.77 1.83 0.62 – 5.40
>2 848 72 6 3.78 776 18 0.97 3.93 1.55 – 9.95

CLINICAL OUTCOMES BY CHADS2
CHADS2
ScoreTotal Pts.
Sub-clinical Atrial Tachyarrhythmia between enrollment and 3 months Sub-clinical Atrial
TachyarrhythmiaPresent vs. absentPresent Absent
Pts. events %/year Pts. event
s %/year HR 95% CIP
(trend)
1 600 68 1 0.56 532 4 0.28 2.11 0.23 – 18.9
0.352 1129 119 4 1.29 1010 22 0.77 1.83 0.62 – 5.40
>2 848 72 6 3.78 776 18 0.97 3.93 1.55 – 9.95

ARTESIAAPIXABAN FOR THE REDUCTION OF THROMBO-EMBOLISM DUE TO SUB-CLINICAL ATRIAL FIBRILLATION• Double blind RCT of Apixaban vs ASA
• Patients with at least one episode EHRA 6 min-24 hr duration
• CHA2DS2-VASc >= 4
• Primary outcome of stroke/STE
• Expected enrollment 3917 to show 35% RR reduction
• Start 5/2015, expected completion 7/2019

IMPACT
Healey, HRS 2015

IMPACT RESULTS
Healey, HRS 2015

REACT COMRHYTHM EVALUATION FOR ANTICOAGULATION WITH CONTINUOUS MONITORING
• Documented PAF, either clinical or subclinical with Reveal monitor implantation
• CHADS2 score 1-2
• Pilot study for safety completed 2/2015
• Plan to randomize to strategy of NOAC administration continuously vs at time of detection plus 30 days

INCREASED PATIENT ACCESS

SO WHAT’S THE FINAL VERDICT?• 2 hour AHRE 11 months prior plus brief blips, CHA2DS2-VASc 2/ CHADS2 2
• Start amiodarone and follow for recurrent AF
• Start aspirin and clopidogrel
• Start NOAC or warfarin
• Intensify monitoring while awaiting trial data

ANY QUESTIONS?

VIDEO BY DR. SHARMA AND DR. WILSON