Embed Size (px)
DESCRIPTION
Brief description about Esophageal Atresia & Tracheo-Esophageal Fistula: embryology, surgical history and management of Type 2: EA & Distal TEF.
Citation preview

Esophageal atresia &
Tracheoesophageal Fistula
Dr. Abdur Rakib Talukder MRCSEdPediatric Surgeon.
Al Yamamah Hospital; KSA

Definition
• Developmental anatomical discontinuity of esophagus with or with out communication with trachea.
• 1670 William Durston first published EA in a conjoint twin.
• Isolated EA-TEF published by Thomas Hill in 1840.

Embryology
• Normal foregut embryology is still obscure.
• The division of foregut is the result of fusion of invaginating lateral longitudinal ridges that created a septum dividing the foregut into a dorsal digestive tract & ventral respiratory system; formation of tracheoesophageal septum is believed to begin caudally & end cranially.
Congenital atresia of the esophagus with tracheoesophageal fistula.
Rosenthal AH.
Arch Path 1931;12:756

Pathophysiology
• The pathogenesis is unknown.
• Occurs sporadically, highly unlikely that simple, inheritable genetic mechanism is responsible.
• Most likely heterogeneous & multifactorial and involves multiple genes & complex gene-environment interactions.

Theories of EA & TEF
• Esophageal occlusion & failure of recanalization.
• Spontaneous deviation of tracheoesophageal septum.
• Abnormal migration of putative tracheoesophageal septum.
• Mechanical obstruction.
• Teratogen: doxorubicin.
• Component of cephalic neurocristopathy.
• HOX D group of genes.
• Defect in signaling pathway of the extracellular, organ differentiation- promoting glycoprotein sonic hedgehog (Shh).
Pattern of cardiovascular anomalies associated with esophageal atresia.
Morini F, Cozzi DA, Harris BH
J Pediatric Surg 1996;31:53

Classification
• In 1929 E. C. Vogt, a radiologist classified the anomaly anatomically:
• Type 1: absent esophagus.
• Type 2: EA without TEF.
• Type 3: EA with fistula:
• a: EA with proximal TEF
• b: EA with distal TEF
• c: EA with proximal & distal TEF.
• Type 4: isolated TEF with intact esophagus.

7.8% 0.8% 85.7% 1.4% 4.2%

Risk Factor
• Adriyamycin rat model.
• Mother with prolong exposure to contraceptive pills.
• Exposed to progesterone & estrogen during pregnancy.
• Infant of Hypothyroid, diabetic mother and after intrauterine exposure to thalidomide.
A syndrome of multiple congenital anomalies associated with teratogenic expouser.
Nora AH, Nora JJ
Arch Environ Health 1975;30:17

Epidemiology • Finland 1 in 2440; US & Australia 1 in 4500 live birth.
• 62% male, (2.29 for TEF alone, 1.44 for EA-TEF & 1.33 for EA ).
• Non white have lower prevalence than white population.
• Increased risk with first pregnancy, mother <20 yrs, and increasing age.
• Multiple birth: (TEF-3.7%; EA-TEF 4.9% EA 8.8% ).
• Chromosomal anomalies 6%-10% (trisomy 18).
• Empirical risk: 0.5%-2% recurrent risk in of one affected child; 20% if more than one sibling affected, 3%-4% in an affected child born to affected parents.
The epidemiology of EA & TEF in Europe
Depaepe A, Dolk H, Lechat MF
EUROCAT Working Group. Arch Dis Child 1993;238:686

Association
• Overall incidence 50-70%
• Anatomical: Cardiovascular 35%
Genitourinary 24%
Gastrointestinal 24%
Neurologic 12%
Musculoskeletal 20%
Familial occurrence of EA with & with TEF
Pletcher BA, Frieds JS, Greg WR.
AM J Med GENT 1991;39:380

Structural Association• VECTRAL association: 20%
Vertebral: 17%
Anal 12%
Cardiac 20%
Renal 16%
Limb 5%
• CHARGE association: ( Cloboma, Heart defect, Atresia choanae, developmental Retardation, Genital hypoplasia, Ear deformity).
• Schisis association: (omphalocele, neural tube defect, cleft lip & palate and genital hypoplasia).
Familial occurrence of EA with & with TEF
Pletcher BA, Frieds JS, Greg WR.
AM J Med GENT 1991;39:380

Syndrome Association:
• DiGeorge Sequence.
• Polysplenia sequence.
• Holt-Oram Syndrome.
• Peirre Robin Sequence.
• Feingold Syndrome.
• Fanconi Syndrome.
• Townes-Brock Syndrome.
• Bartsocas-Papas Syndrome.
• McKusic-Kaufman Syndrome.
Familial occurrence of EA with & with TEF
Pletcher BA, Frieds JS, Greg WR.
AM J Med GENT 1991;39:380

• Other less common anomaly: Choanal atresia 5.2%,
Facial cleft 7.2%,
Abdominal wall defect 4.3%,
Diaphragmatic hernia 2.9%
Descriptive epidemiology of alimentary tract atresia.
Harris J, Kallen B, Robert E
Teratology 1995;52:15

Abnormality:
• 47% incidence of tracheobronchial abnormalities: ectopic or absent right upper lobe, congenital bronchial stenosis and a decreased ratio of circumferential cartilaginous trachea to membranous trachea.
• EA associated with abnormalities of Vagal nerve innervations that are not related to surgical intervention to repair.
Anomalies of the tracheobronchial tree in infants with EA
Usui N, Kamata S, Ishikawa
J Pediatric Surg 1996;31:258.

Diagnosis
• Postnatal:
• Most infants with EA are symptomatic in the first few hours. earliest sign is excessive salivation, typically first feeding is followed by regurgitation, choking and coughing other features are cyanosis with or with out feeding, respiratory distress, inability to swallow and inability to pass a feeding tube in the stomach.
• If distal fistula present the abdomen distends.

Prenatal detecttion:
• USG relies on finding of an anechoic area in the middle of the neck, small or absent stomach bubble and associated maternal polyhydroamnios; predictive value 20-40%,
• Fetal MRI may be a useful adjunct for diagnosis.
Comparison of MRI & USG in the prenatal diagnosis of thoracic abnormality.
Matsuoka S, Takeuchi K, Yamanaka
Fetal Diag 2003;18:447

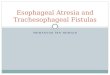
A: Transverse section: fluid-filled stomach.
B: Coronal section: blind-ending pouch of esophagus.
Coronal scan neck and chest:shows dilated blind-ending proximal esophageal pouch.
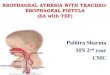
A B

Axial T2 of the thorax: no esophagus Sagittal T2: Note fluid filled blind ending esophageal pouch.

Radiology
• Plain chest X-ray with a NGT: coiled NGT at upper pouch.
• A few ml of air can be injected through the tube & used as contrast to distend upper pouch as frontal & lateral films taken. If necessary 0.5-1ml of diluted barium can be used-if barium used fluoroscopy advisable to detect proximal fistula. Air in the stomach & bowel confirm distal TEF, absence of air typically represent isolated TEF.


• Additional testing: Echocardiography,
Renal Ultra Sound ,
Chromosomal analysis.

Preoperative treatment
• NPO & IVF 10% D & hypotonic saline .
• Management to prevent further aspiration & pneumonitis: Start broad spectrum antibiotic & chest physiotherapy.
A sump catheter/double lumen Replogle Catheter for continuous low pressure negative suction.
Positioning of infants to prevent reflux: upright sitting/ head-up prone position.
• Vit K analog should be given.
• Routine ET intubation should be avoided.

Surgery
• 1869 Timothy Holmes first suggest surgical anastomosis.
• First operative attempt: 1888 Charles Steelle performed a gastrostomy, push a steel probe through the gastrostomy, simultaneously push down a bugie.
Surgical correction of congenital atresia of esophagus with TEF.
Shaw R
J Thoar Surg 1939;9:213

• 1938 Robert shaw first performed fistula ligation & primary anastomosis.
• First survivor of EA-TEF in 1939: gastrostomy , extraplural ligation of fistula, cervical esophagostomy.
Management of esophageal atresia.
Humphreys GH, Ferrer JM Jr,
Am J Surg 1964;107:406

Time of surgery
• Waterston Group A: immediate operative repair
• Waterston Group B: delayed repair
• Waterston Group C: Staged repair .
Management of esophageal atresia.
Spitz L, Kiely E, Brereton RJ, Drake D
J Pediatric Surgery 1993;17:296

Type of Surgery
• Thoracotomy: Extra-pleural
Trans pleural
• VAT

Procedure: EA with TEF
• Positioning: Infant usually positioned for a standard right posterolateral thoracotomy, with right arm extended above head & head slightly flexed. If a right sided aortic arch (2.5%) is identified a left sided thoracotomy performed.
• Anesthetic technique: minimal usage of premed, careful positioning of ET tube, manual control of adequate ventilation with minimal gas flow through fistula until it ligated.
The management of EA in neonates with right sided aortic arch.
Babu R,Pierro A Spitz L
J Pediatric Surgery 2000;35:56




Comparison of technique
Thoracotomy
• Scoliosis
• Winged scapula
• Chronic pain
• Shoulder weakness
• Chest wall deformity
• malsevelopment
VAT
• Superior visualization, Improved cosmesis.
• Limited working space, lack of articulation of instruments, tying suture under tension.
• 2-4 Hop time, 30-50% stenosis, 12-15% leak, 30-50% GER.
Feasibility of thoracoscopic repair of of EA with distal fistulaBax KMA, Van der Zee DC
J Pediatric Surg 2002;37:192

Critical Cases
• EA with Large distal fistula with RDS:
• High pressure ventilation worsen lung ventilation & abdominal distension. to improve ventilation:
Emergency thoracotomy & fistula ligation.
Gastrostomy or gstrostomy tube with under water seal.
Gastric division/banding of gastroesophageal junction.
Bronchoscopic placement of Fogarty balloon catheter through fistula.
Management of infants with EA & TEF need high pressure ventilatory support.
Leininger et al.
J Pediatric Surgery 1972;7:404


Early thoracotomy & fistula division in infants with sever RDS
who requires high pressure ventilation & delayed primary anastomosis.
Management of esophageal atresia and tracheoesophageal fistula in the neonates with sever respiratory distress syndrome.
Templeton JM Jr, Templeton JJ.
J Pediatric Surgery 1985;20:394268

Outcome
• Between 1939 to 1969 Dr. Haight did 284 infants with EA and report as 52% overall survival rate.
• 85-95% overall survival.
• H-type fistula have less association.
• VECTRAL association have high mortality .
Survival of Patients with esophageal atresia: Influence of birth weight, cardiac anomaly & late respiratory complications.
Choudhury SR, Ashcraft KW, Sharp RJ
J Pediatric Surg 1999;34:70

Risk factor & Survival
Group Survival Waterston Classification
A 100% Birth wt >2500gm, otherwise healthy
B 85% Birth wt 2000-2500, otherwise well, orHigher wt with moderate anomaly (non cardiac anomaly plus PDA, VSD, ASD)
C 65% Birth wt < 2000gm & otherwise well, orHigher wt with sever associated cardiac anomaly
Esophageal atresia: Tracheoesophageal fistula. A study of survival in 298 infantD.J. Waterston, R.E. Bonham Carter, Aberdeen E
Lancet 1962;1:819

Predictor of survival
Group Survival
I Birth weight >1500g with out major congenital heart disease
97%
II Birth weight <1500 g or major congenital heart disease
59%
III Birth weight < 1500 g and congenital heart disease
22%
Spitz Classification:
Esophageal atresia: at risk group for 1990s.
Spitz et al.
J pediatric Surg 1994;29:723

Risk for death
• Inceased risk of death & long term morbidity include:1. Lower birth wt (<1500 g) & prematurity.
2. Major CHD.
3. Sever associated anomaly & ventilator dependent
4. Long gap EA.
EA: Historical evaluationof management & results in 371 infants.
Deurloo JA, Ekkelkamp S, Schoorl M
Ann Thorac Surg 2002;73:267

Complication
• Early:
Anastomotic leak
Anastomotic stricture
Recurrent TEF
• Late:
GER
Tracheomalacia
Disordered esophageal peristalsis

Anastomotic leak• 14% to 16%, managed with adequate drainage & nutritional
support, 95% close sponteneously.
• Major disruption occur 3% to 5% of postoperative leak, typically recognized early
• Factors for leak:
Poor surgical technique
Ischeamia of esophageal ends
Use of myotomy
Excessive tension at anastomotic site
• Reoperation: control sepsis with drainage and repair by pleural or pericardial patch, with or with out intercostals muscle flap buttress.
50 yrs experience with EA & TEF.
Manning BP, Morgan RA, Coran AG
Ann Surg 1986;9:373

Anastomotic stricture
• Spitz & hitchcock defined stricture as the presence of symptoms: dysphagia & recurrent respiratory probles from aspiration or forgine bodu obstruction & narrowing noted on endoscopy.
• Stricture require dilatation occur upto 80% of patient.
• Factors responsible: Poor anastomotic technique: excessive tension, two-layered anastomosis, silk suture, Ischeamia at ends, GER, Anastomotic leak.
• Traditionally treated by dilatation: antegrade or retrograde bouginage using Savory dilator, Gruntzig balloon dilator
• 53% respond to single dilatation in the first month.
Esophageal Atresia & Tracheoesophageal Atresia
Spitz L, Hitchcock R
Churchill Livingstone, New York

Recurrent TEF
• Occur upto 3% to 14 %.
• Attributed to anastomotic leak with local infllammation & errosion through the previous site of TEF.
• Can be minimized by using: Pleural flap; Vasculrized pericardial flap; Azygos vein flap.
• 50% of recurrent fistula missed in routine contrast study, esophagography in the prone position under video fluroscopy; Bronchoscopy with cannulation of fistula is gold standerd.
• Traditionlly repaired by thoracotomy & interposition; Fibrin glue, Endoscopic eradication of TEF by chemicals or diathermy.
Recurrent EA treated with Fibrin Glue
Gutierrez, C, Barrios JE, Lluna,
J Pediatric Surgery 1994;29:1567

GERD• Occurs up to 30% to 70% .
• Probably relates to shortening of intra-abdominal portion or esophageal motor dysfunction. 9% risk of developing barrett’sesophagus.
• Suspected with GIT symptoms: vomiting, dysphagea & recurrent anastomotic stenosis; Respiratory symptoms: stridor, cyanotic spells, recurrent pneumonia, & reactive airway disease.
• Diagnosed by, upper GI dye study, 24 H pH probe data, esophageal manomatric study.
• Medical management: thickening of feeding, H2 blocker, PPI, prokinrctic agent. 45% to 75% undergo anti reflux surgery,.
Analysis of morbidity & mortality in 227 cases of EA & or TEF over 20 yrs.
Engum SA, Grosfeld JL, West KW
Arch Surg 1995;130:502

Long-Term quality of life
• The incidence of problem approaches 75% to 100% who have studied with manometry.
• Occasional dysphagia to occur as many as 50% to 90% of adults with 30% have additional chocking.
• These symptoms may improve in time, early problem with feeding intolarence & food bolus obstruction can lead to failure to thrive
• These childre must eat slowly with food choice.
Adults who survived repair of congenital EA & TEF.
Chetcuti P, Myers NA, Phelan PD
BMJ 1988;297:344

Message:
• Evaluate the patient of EA-TEF with complete care to rule out any association & stratify the risk factors with out come.
• Proper & specific pre-operative management and complete plan of management including expected post-operative complication.
• Presentation of the patient, operative & post-operative morbidity to be discussed with parents after complete assessment.