Embed Size (px)
Citation preview
ESOPHAGEAL ATRESIA WITH TRACHEO-ESOPHAGIAL
FISTULA
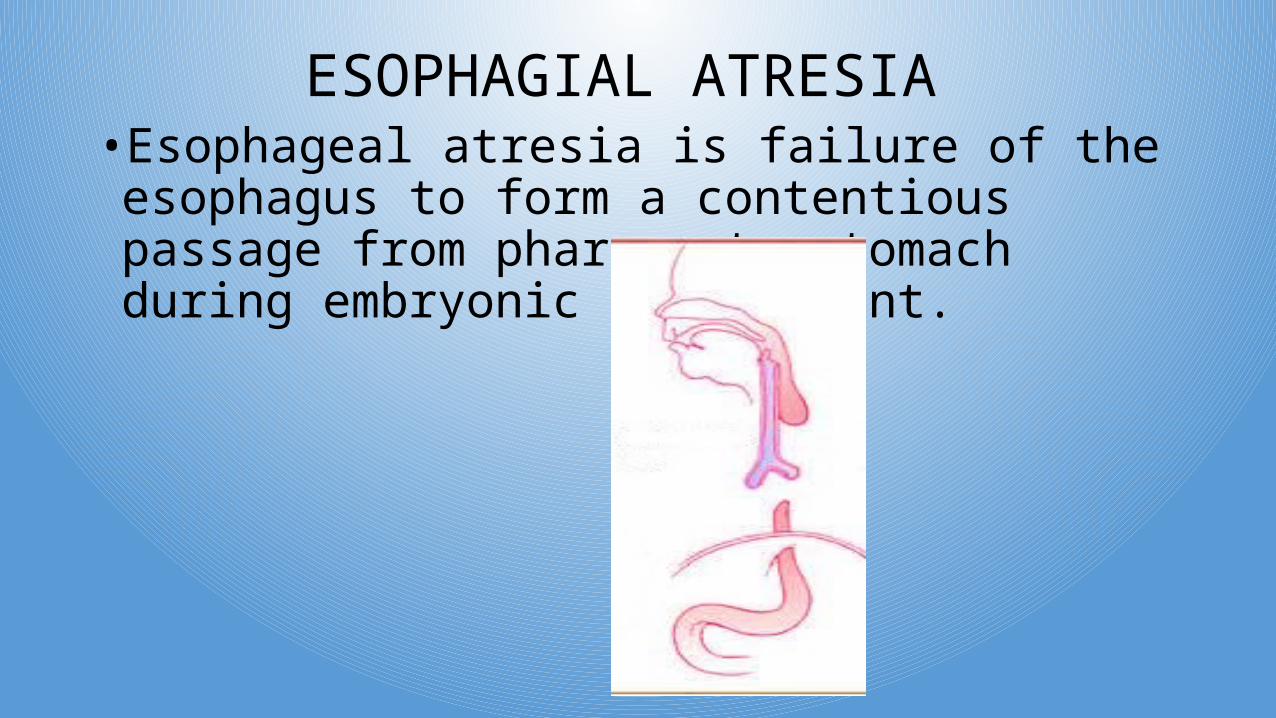
ESOPHAGIAL ATRESIA •Esophageal atresia is failure of the esophagus to form a contentious passage from pharynx to stomach during embryonic development.
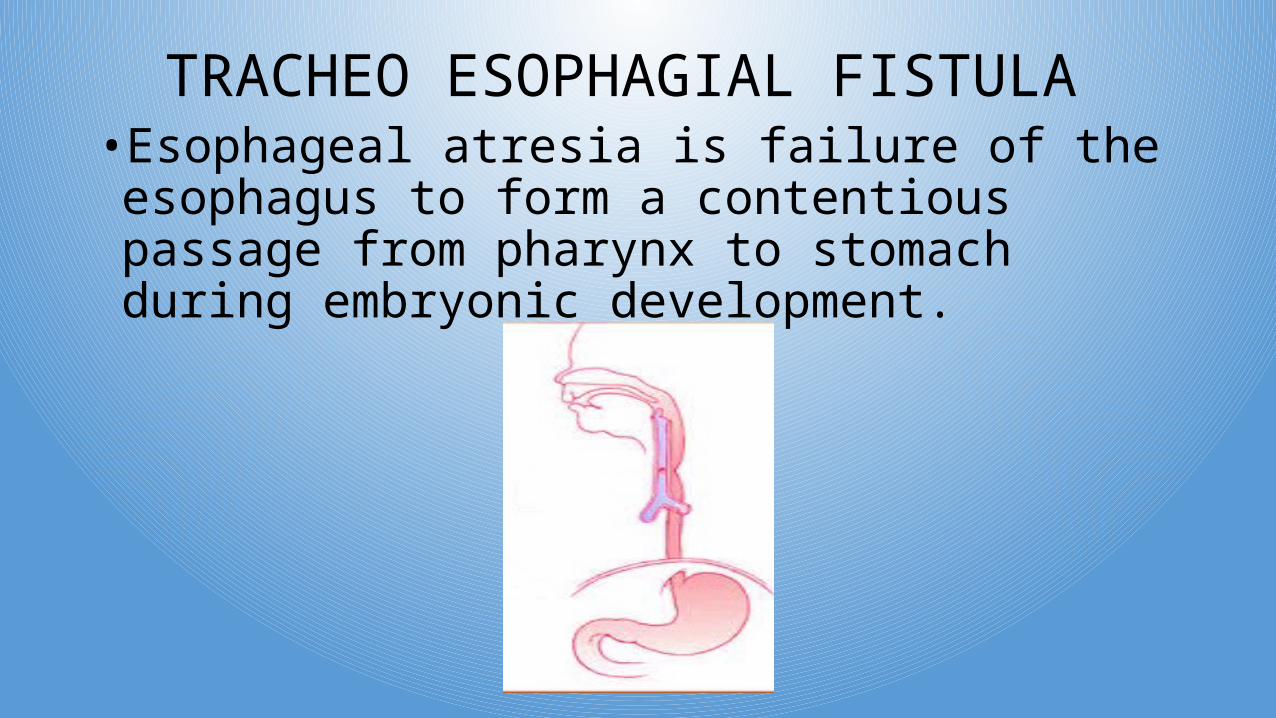
TRACHEO ESOPHAGIAL FISTULA •Esophageal atresia is failure of the esophagus to form a contentious passage from pharynx to stomach during embryonic development.
ETIOLOGY 1. GENETIC DEFECT:-
Mutation in genetic structure of baby during embryonic development may lead to abnormal development of organ.
2. TERATOGENIC STIMULI:- Radiation, maternal infection, chemicals and drugs.
3. INTRAUTERINE CAUSES:-Infections like TORCH can cross placental barrier and can leads
to intrauterine triggering.
ETIOLOGY 4. Anomalies may develop due to aberration or deviation from septum between esophagus and trachea or alteration in growth of spleen.
5. TEF :- Develop due to failure of separation of esophagus and trachea during embryonic development.6. EA:- Develops due to deficient growth of dorsal wall of esophagus.
INCIDENCE• Esophageal atresia with or without an associated TEF is the most
common esophageal malformation, occurring in approximately 1 in 3500 live births. There appears to be an equal sex incidence, but the birth weight of most affected infants is significantly lower than average, and incidence of prematurity is usually high.
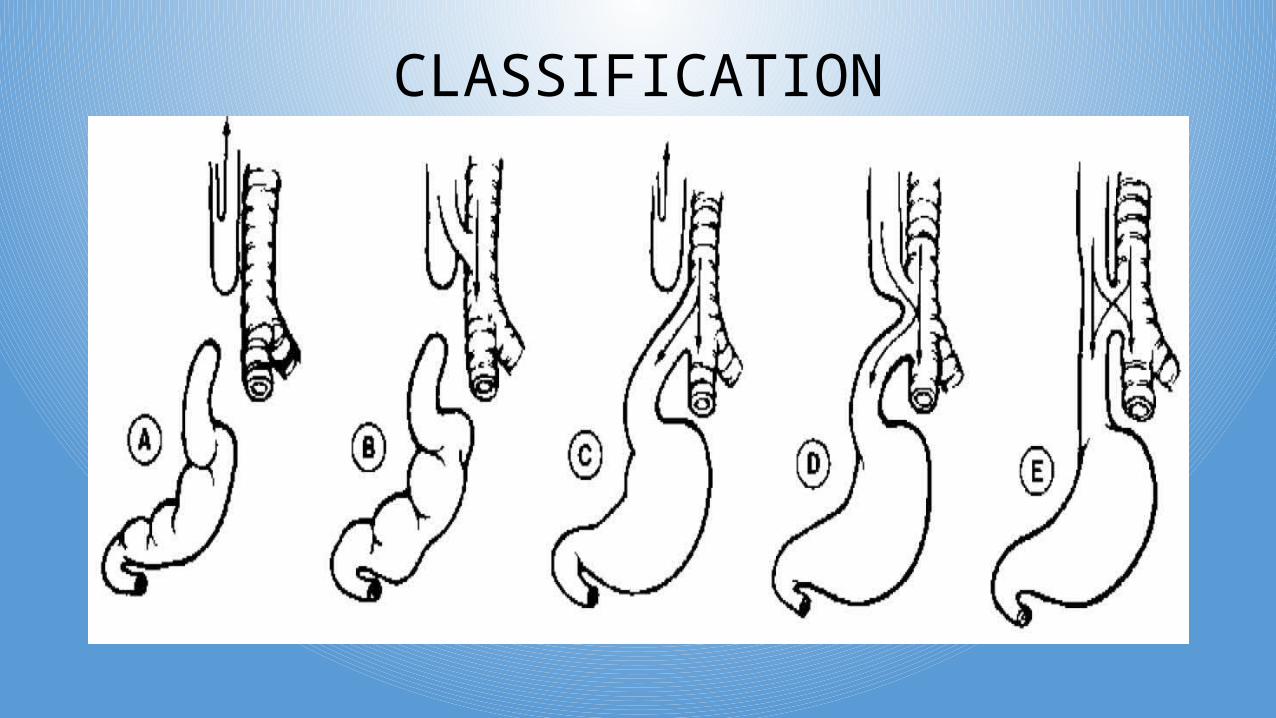
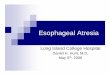
CLASSIFICATION
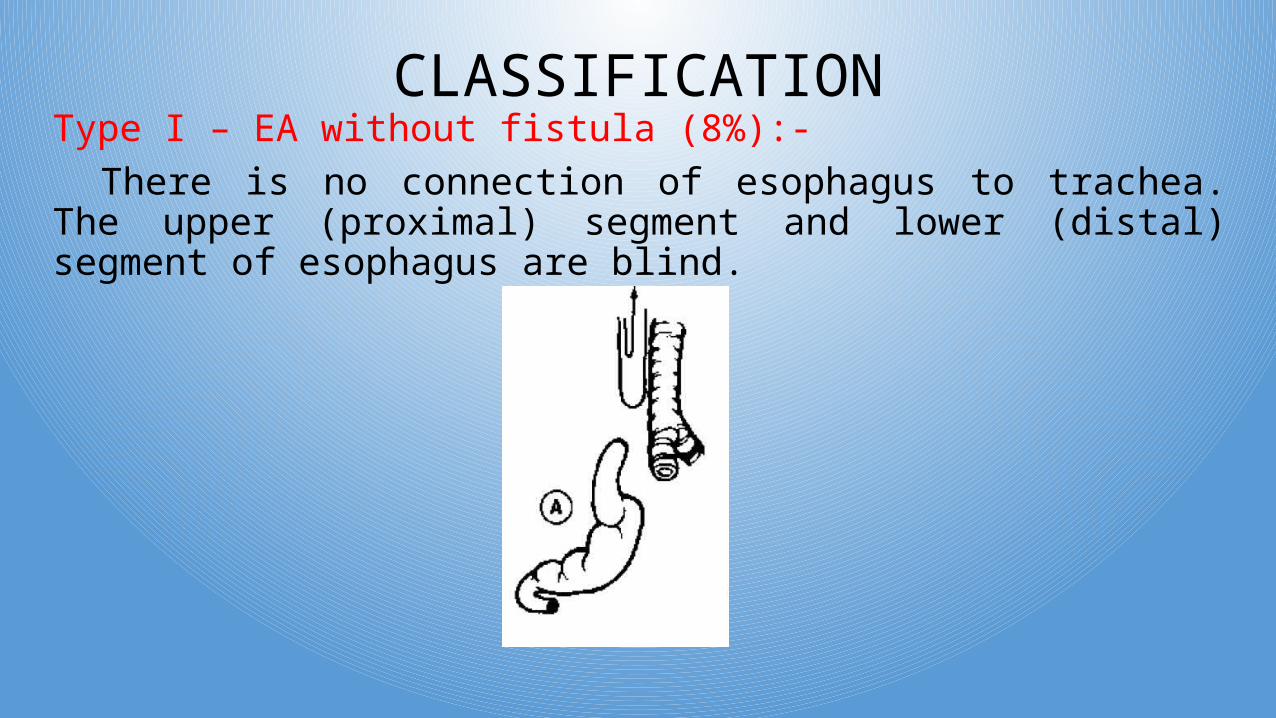
CLASSIFICATIONType I – EA without fistula (8%):-
There is no connection of esophagus to trachea. The upper (proximal) segment and lower (distal) segment of esophagus are blind.
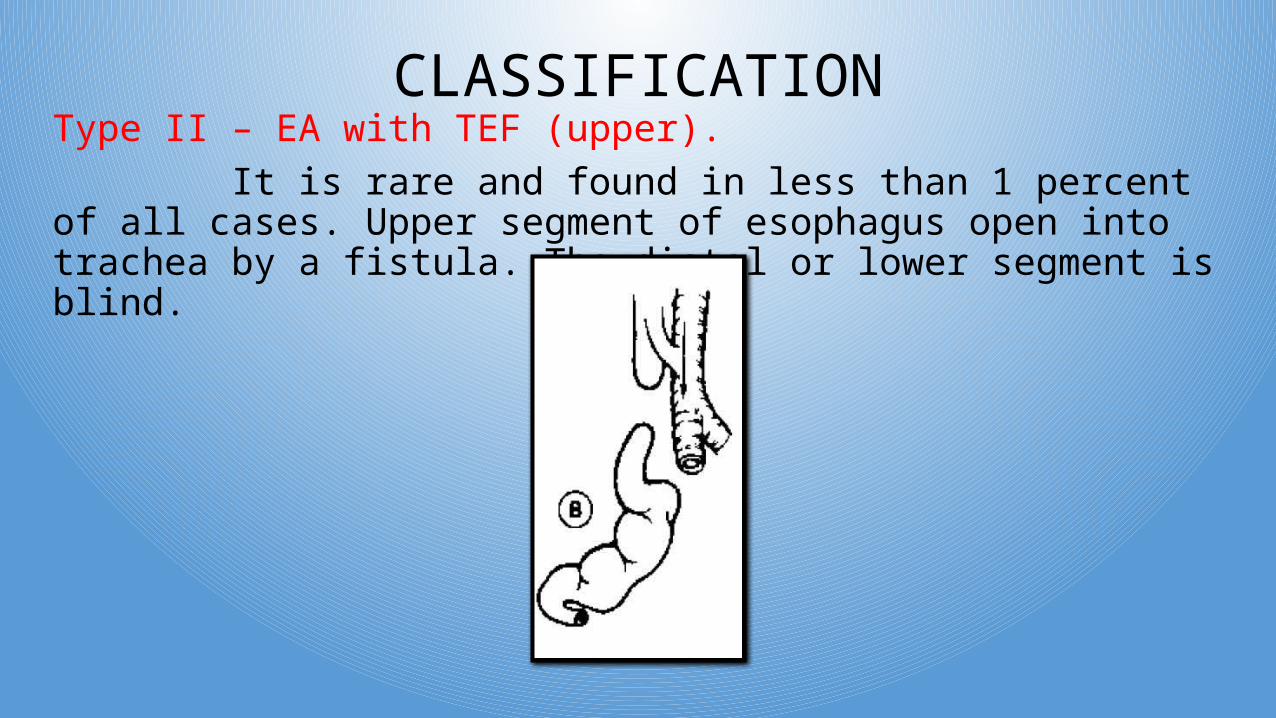
CLASSIFICATIONType II – EA with TEF (upper). It is rare and found in less than 1 percent of all cases. Upper segment of esophagus open into trachea by a fistula. The distal or lower segment is blind.
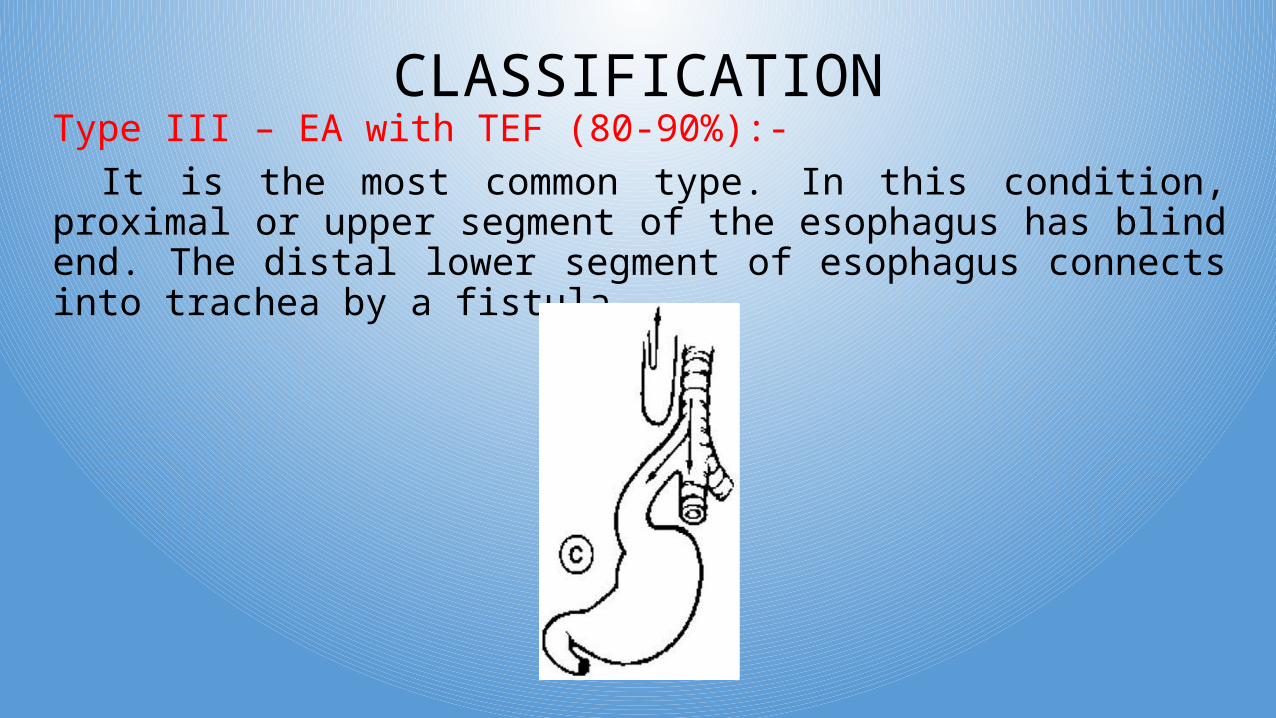
CLASSIFICATIONType III – EA with TEF (80-90%):-
It is the most common type. In this condition, proximal or upper segment of the esophagus has blind end. The distal lower segment of esophagus connects into trachea by a fistula.
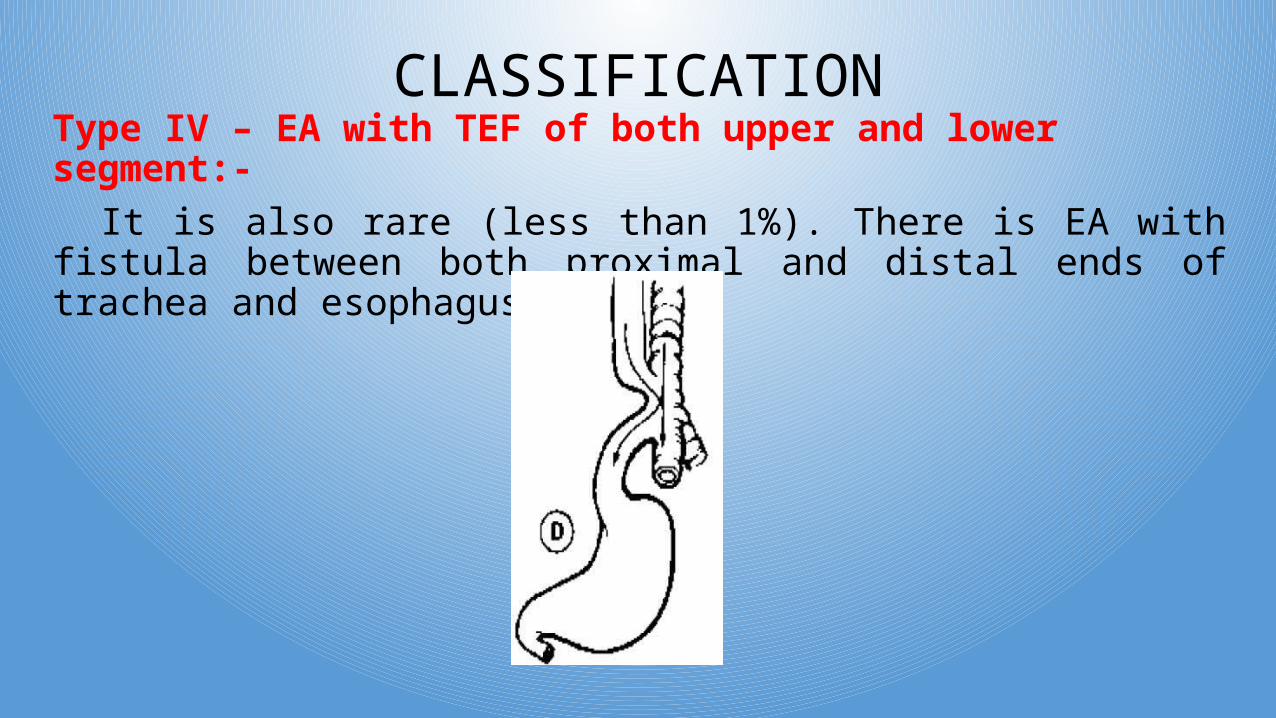
CLASSIFICATIONType IV – EA with TEF of both upper and lower segment:-
It is also rare (less than 1%). There is EA with fistula between both proximal and distal ends of trachea and esophagus.
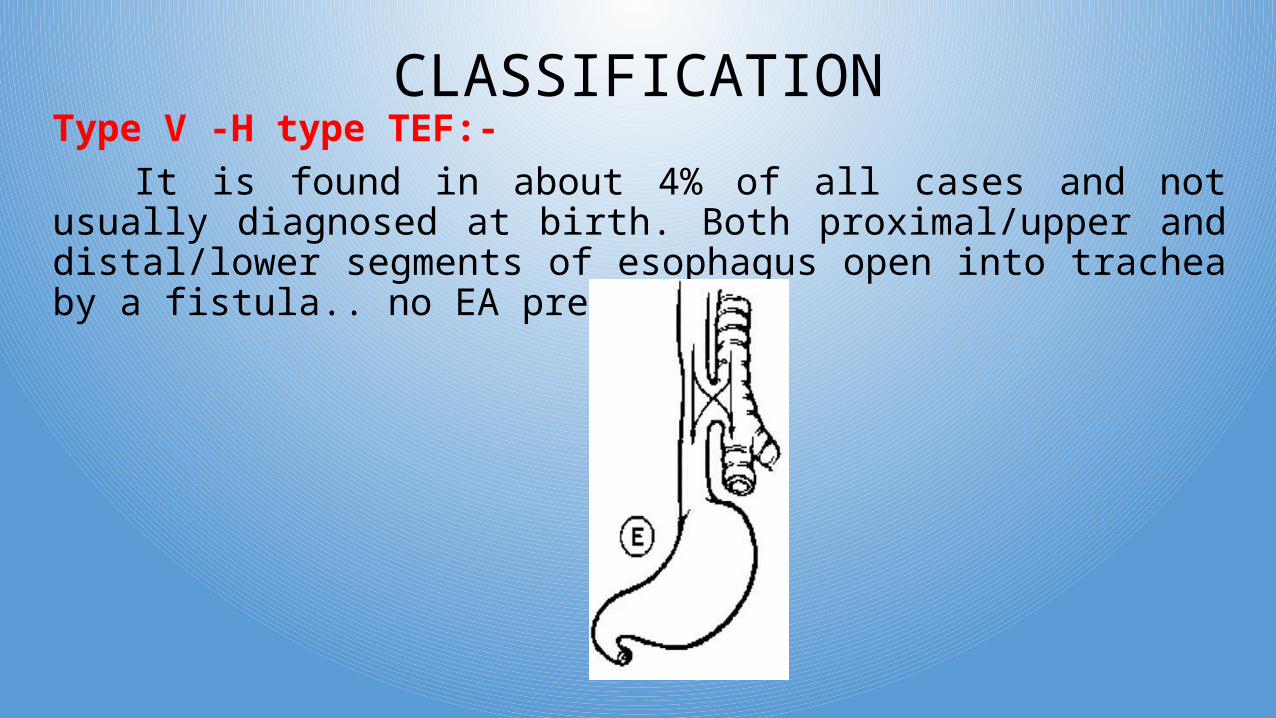
CLASSIFICATIONType V -H type TEF:-
It is found in about 4% of all cases and not usually diagnosed at birth. Both proximal/upper and distal/lower segments of esophagus open into trachea by a fistula.. no EA present.
CLINICAL MANIFESTATION1. Excessive salivation2. Constant drabbling of saliva3. Large amount of secretions from nose.4. Coughing, gaging, choking.5. Cyanosis:- Intermittent unexplained cyanosis due to laryngospasm caused by accumulated saliva.6. Regurgitation of feeding may be entering into respiratory system through fistula during inspiration.
DIAGNOSTIC EVALUATION1. CATHETERIZATION:- Inability of passing catheter from nose or mouth
to stomach indicates blind pouch or atresia.2. ANTENATAL DIAGNOSIS:- By USG of abdomen in antenatal period. 3. POSTNATAL DIAGNOSIS:- By USG, plain X-ray examination of
abdomen, chest X-ray, passing of radio opaque catheter through esophagus and conforming anomalies by X-ray.
4. BRONCHOSCOPY5. ECG and ECHOCARDIOGRAM:- To detect associated cardiac
disorders.
MANAGEMENTA) IMMIDIATE MANAGEMENT:- 1) Propped Up position:- 30* elevation. 30* to revert gastric secretion reflex.2) Neel by mouth (NBM)3) Oxygen therapy4) I.V. therapy5) Nasogastric tube feeding6) Frequent suctioning to prevent aspiration7) Saline irrigation of blind pouch & prevent blockage of tube.8) Gastrostomy:- creating a artificial opening
MANAGEMENT9) Supportive care:- Maintenance of nutritional levelPrevention of infectionAntibioticsRespiratory supportDetection and treatment of complicationsChest physiotherapyPostural drainage
MANAGEMENTB) SURGICAL MANAGEMENT:- 1.) End to end anastomosis with excision of fistula by “Right posterolateral thoracotomy” followed by “intercostal chest drainage”. Indications are:-Infant’s weight more then 2 kg.No pneumonia should be evident.Stages are:- Gastrostomy esophageal anastomosis or colonic transplant after 1 year.
NURSING MANAGEMENTPRE OPERATIVE:- - Prevent aspiration- Prevent dehydration- Infection control- Reducing parental anxietyPOST OPERATIVE:- - Maintain clear airway- Fluid balance and feeding- Analgesics for pain- Chest tube drainage

THANK YOU