Embed Size (px)
DESCRIPTION
Rntcp
Citation preview

Scientific Basis of Scientific Basis of Diagnosis and Treatment in RNTCPDiagnosis and Treatment in RNTCP
Dr Awadhesh Kumar Sharma ,Dr Awadhesh Kumar Sharma ,MDMD
Senior residentSenior resident
Department of Medicine,Department of Medicine,
M.L.B. Medical College,M.L.B. Medical College,
Jhansi, UPJhansi, UP

Tuberculosis is an infectious disease caused by Mycobacterium tuberculosis which is discovered by Robert Koch.
Pulmonary tuberculosis is the most common form of TB.
Transmission occurs by air borne spread of infectious droplets and droplet nuclei containing the tubercle bacilli.
The source of infection is a person with sputum smear-positive pulmonary TB.
Robert Koch

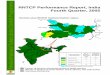
India is the highest TB burden country globally India is the highest TB burden country globally accounting for one fifth of the global incidenceaccounting for one fifth of the global incidence
Source: WHO Geneva; WHO Report 2006: Global Tuberculosis Control; Surveillance, Planning and Financing
Globally ~9 million new TB cases occur annually
Non-HBCs20%
Ethiopia3%
Philippines3%
South Africa4%
Bangladesh4%
Pakistan3%
Nigeria4%
Indonesia6%
China15%
India20%
Other 13 HBCs18%

Problem of TB in IndiaProblem of TB in India
Incidence of TB disease:Incidence of TB disease: 1.8 million new TB cases annually (0.8 1.8 million new TB cases annually (0.8
million new infectious cases)million new infectious cases)
Prevalence of TB disease:Prevalence of TB disease: 3.8 million bacteriologically positive 3.8 million bacteriologically positive
(2000)(2000)
Deaths:Deaths: about 370,000 deaths due to TB each year about 370,000 deaths due to TB each year
TB/HIV:TB/HIV: ~2.5 million people with HIV & ~1 million co infected with ~2.5 million people with HIV & ~1 million co infected with
TB-HIV TB-HIV
– About 5% of TB patients estimated to be HIV positiveAbout 5% of TB patients estimated to be HIV positive
MDR-TBMDR-TB in new TB cases in new TB cases ≤≤3% 3%
Substantial Substantial socio- economicsocio- economic impact impact

Estimated Incidence of TB in Estimated Incidence of TB in India*India*
(No. of New Smear Positive Cases per 100,000 (No. of New Smear Positive Cases per 100,000 population, per year)population, per year)
NationalNational 75 75
North ZoneNorth Zone 9595
East ZoneEast Zone 7575
West ZoneWest Zone 8080
South ZoneSouth Zone 7575
North
West East
South

NATIONAL TUBERCULOSIS CONTROL PROGRAMME
During the 1950 s & 1960 s, significant research on TB was undertaken in India & in 1962 the National TB Control Programme (NTP) was launched.
In 1992, a review of the NTP found that the desired results had not been achieved.
There was over dependence on X rays for diagnosis.

REVISED NATIONAL TB CONTROL PROGRAMME
A revised strategy to control TB was pilot tested in 1993.
The RNTCP applies the WHO recommended DOTS (Directly Observed, Short Course) strategy.
The programme was expanded in a phased manner to cover the entire country in 2005.

RNTCP – Goal and ObjectivesRNTCP – Goal and Objectives GoalGoal
– The goal of TB control Programme is to decrease The goal of TB control Programme is to decrease
mortality and morbidity due to TB and cut transmission mortality and morbidity due to TB and cut transmission
of infection until TB ceases to be a major public health of infection until TB ceases to be a major public health
problem in India. problem in India.
Objectives:Objectives:
– To achieve and maintain a cure rate of at least 85% To achieve and maintain a cure rate of at least 85%
amongst new smear positive casesamongst new smear positive cases
– To achieve and maintain a case detection of at least To achieve and maintain a case detection of at least
70% of the estimated new sputum positive TB patients 70% of the estimated new sputum positive TB patients

Scientific basis of diagnosisScientific basis of diagnosisScientific basis of the treatment regimenScientific basis of the treatment regimenBasis of intermittent chemotherapy Basis of intermittent chemotherapy Directly observed treatmentDirectly observed treatment

DiagnosisDiagnosis

How are TB cases diagnosed?How are TB cases diagnosed?
Cough for Cough for ≥≥3 weeks (3 weeks (TB suspectsTB suspects) screened from ) screened from OPD/clinics and referred for sputum microscopyOPD/clinics and referred for sputum microscopy
Sputum microscopy performed at quality assured Sputum microscopy performed at quality assured Designated Microscopy Centres (DMCs)Designated Microscopy Centres (DMCs)
If sputum is initially negative and remains so after a If sputum is initially negative and remains so after a course of antibiotic, despite persisting symptoms, then course of antibiotic, despite persisting symptoms, then X-ray chest is doneX-ray chest is done
Standard diagnostic algorithm for pulmonary TBStandard diagnostic algorithm for pulmonary TB
– Patients diagnosed as Sputum +ve and Sputum –ve Patients diagnosed as Sputum +ve and Sputum –ve PTBPTB
Extra-Pulmonary TB is diagnosed based on clinical Extra-Pulmonary TB is diagnosed based on clinical evaluation and histopathological evidenceevaluation and histopathological evidence

DIAGNOSTIC ALGORITHM FOR PULMONARY TB

Specificity
0
20
40
60
80
100
AFBmicroscopy
X-ray
%
Diagnosis by Microscopy of Patients Diagnosis by Microscopy of Patients Presenting to Health FacilitiesPresenting to Health Facilities
Microscopy is more Microscopy is more accurate than x-ray, and accurate than x-ray, and correlates with correlates with infectiousness as well as infectiousness as well as with risk of death from TBwith risk of death from TB
Virtually all patients with Virtually all patients with multiple positive direct multiple positive direct AFB smears have TBAFB smears have TB
At least half of persons At least half of persons with x-rays suggestive of with x-rays suggestive of TB do not have TBTB do not have TB

Inter-observer variability
0
5
10
15
20
25
30
35
X-ray AFBMicroscopy
%
Microscopy is More Objective and Microscopy is More Objective and Reliable than X-rayReliable than X-ray
Inter-observer variability is Inter-observer variability is much less with microscopy much less with microscopy than with x-raythan with x-ray
AFB microscopy provides AFB microscopy provides information on infectiousness information on infectiousness of the patient, which x-ray does of the patient, which x-ray does notnot
AFB microscopy allows AFB microscopy allows prioritization of cases, which x-prioritization of cases, which x-ray does notray does not
AFB microscopy is also an AFB microscopy is also an objective method to follow the objective method to follow the progress of patients on progress of patients on treatmenttreatment

Acid Fast Stain Tubercle Bacilli

Problems with Over-Reliance on Problems with Over-Reliance on X-ray for TB DiagnosisX-ray for TB Diagnosis
Misclassification of non-TB as TB, resulting in unwarranted Misclassification of non-TB as TB, resulting in unwarranted treatment and avoidable expendituretreatment and avoidable expenditure
Inability to distinguish between smear+ and smear-Inability to distinguish between smear+ and smear-negative patients, resulting in inadequate priority to true negative patients, resulting in inadequate priority to true smear+ patientssmear+ patients
Failure to give appropriate treatmentFailure to give appropriate treatment
Inability to monitor progress accuratelyInability to monitor progress accurately
Lower cure rates and increased spread of TBLower cure rates and increased spread of TB

X-rays of an Dubai based NRI engineer who complaints of cough with expectoration alongwith haemoptysis for 3 months, diagnosed there as case of pulmonary tuberculosis & antituberculosis Rx started. When he did not get relief, he visited India, here on investigation his eosinophillic count and IGE level found to be elevated & diagnosed as case of Allegric Bronchopulomonary Aspergillosis and got relief by antifungal and steroids .

Case- ICase- I
This chest X-ray of Pt. This chest X-ray of Pt. mrs. Vimla 25 yrs. old mrs. Vimla 25 yrs. old lady admitted on 7lady admitted on 7thth April April 08 with complaints of 08 with complaints of high grade fever with high grade fever with productive cough. productive cough. Treated on the line of Treated on the line of right lower lobe right lower lobe pneumonitis with IV pneumonitis with IV antibiotics for 2 weeks antibiotics for 2 weeks but did not get reliefed. but did not get reliefed. Later her sputum Later her sputum examination was done examination was done and found to be AFB and found to be AFB positive and treated on positive and treated on line of cat. I regimen.line of cat. I regimen.

Case- IICase- II
This chest X-ray of Pt. Mr. This chest X-ray of Pt. Mr. Gopesh Kumar 50 yrs. old Gopesh Kumar 50 yrs. old male admitted on 8male admitted on 8thth April April 08 with complaints of high 08 with complaints of high grade fever with productive grade fever with productive cough with chest pain and cough with chest pain and dyspnoea. TLC was 42000 dyspnoea. TLC was 42000 /cmm and polymorphs were /cmm and polymorphs were 92%.Treated on the line of 92%.Treated on the line of right upper lobe lung right upper lobe lung abcess with IV antibiotics abcess with IV antibiotics for 2 weeks but did not get for 2 weeks but did not get relief. Later his sputum relief. Later his sputum examination was done and examination was done and found to be AFB positive found to be AFB positive and on repeat chest X-ray and on repeat chest X-ray the cavity size increased & the cavity size increased & involved whole of the right involved whole of the right upper and middle lobe and upper and middle lobe and treated on the lines of cat. I treated on the lines of cat. I regimen. After that pt. regimen. After that pt. improved.improved.

0
20
40
60
80
100
Diagnosed byx-ray alone
Actual cases
%
A systematic evaluation of A systematic evaluation of well-functioning District TB well-functioning District TB Centres by the National TB Centres by the National TB Institute, Bangalore found Institute, Bangalore found that nearly 70% of the that nearly 70% of the cases diagnosed and put on cases diagnosed and put on treatment on the basis of x-treatment on the basis of x-ray, ray, did not have did not have tuberculosis at alltuberculosis at all
The proportion of cases The proportion of cases diagnosed on the basis of x-diagnosed on the basis of x-ray alone and put on ray alone and put on treatment unnecessarily is treatment unnecessarily is likely to be even higher in likely to be even higher in many centresmany centres
NTI, IJT, 1974
Over-diagnosis

Three sputum Samples collected - SPOT – Early Morning – SPOT

81%
93%100%
0%
50%
100%
First Second Third
Cum
ulat
ive
Pos
itivi
tyThree sputum smears are
optimal

Diagnosis of tuberculosisDiagnosis of tuberculosisToolsTools MeritsMerits DemeritsDemerits
Tuberculin Tuberculin testtest
Can identify infectionCan identify infection
Good epidemiological Good epidemiological tooltool
Cannot Cannot differentiate differentiate infection & diseaseinfection & disease
X-rayX-ray SensitiveSensitive Not specificNot specific
Sputum Sm. Sputum Sm. MicroscopyMicroscopy
Definitive diagnosisDefinitive diagnosis
Easy to perform at the Easy to perform at the peripheryperiphery
ReplicabilityReplicability
Less costlyLess costly
Sensitivity 60-80%Sensitivity 60-80%
Culture for Culture for MTBMTB
Highly sensitive & Highly sensitive & specificspecific
Costly, not freely Costly, not freely availableavailable
long waiting periodlong waiting period

TreatmentTreatment

Aims of TB treatmentAims of TB treatment
To decrease mortality, long-term morbidity and To decrease mortality, long-term morbidity and transmissiontransmission
To effect a permanent cure, prevent relapses and To effect a permanent cure, prevent relapses and decrease transmissiondecrease transmission
To minimize development of drug resistanceTo minimize development of drug resistance To achieve the above while minimizing drug side To achieve the above while minimizing drug side
effectseffects

Some definitions ……..Some definitions …….. Smear positive patient Smear positive patient
- A patient with at least 2 initial sputum smear - A patient with at least 2 initial sputum smear examination (direct smear microscopy) positive for examination (direct smear microscopy) positive for acid-fast bacilli (AFB).acid-fast bacilli (AFB).
- Or A patient with one sputum examination positive - Or A patient with one sputum examination positive for AFB and radiographic abnormalities consistent for AFB and radiographic abnormalities consistent with active pulmonary TB.with active pulmonary TB.
- Or A patient with one sputum specimen positive for - Or A patient with one sputum specimen positive for AFB and culture positive for M tuberculosis.AFB and culture positive for M tuberculosis.

Some definitions ……..Some definitions …….. Smear negative patient Smear negative patient
- A patient having symptoms suggestive of TB with - A patient having symptoms suggestive of TB with at least 3 sputum examinations negative for AFB at least 3 sputum examinations negative for AFB and radiographic abnormalities consistent with and radiographic abnormalities consistent with active pulmonary TB.active pulmonary TB.
- Or A patient whose diagnosis is based on culture - Or A patient whose diagnosis is based on culture positive for M. tuberculosis but sputum smear positive for M. tuberculosis but sputum smear examinations negative for AFB.examinations negative for AFB.

Types of Tuberculosis PatientsTypes of Tuberculosis Patients
New: New: A TB patient who has never had treatment for A TB patient who has never had treatment for TB or one who has taken anti TB drugs for less than TB or one who has taken anti TB drugs for less than one month.one month.
Relapse:Relapse: A TB patient who was declared cured or A TB patient who was declared cured or treatment completed by a physician, but who reports treatment completed by a physician, but who reports back to the health service and is now found to be back to the health service and is now found to be sputum smear-positive.sputum smear-positive.
Transferred inTransferred in: A TB patient who has been received : A TB patient who has been received for treatment in one Tuberculosis unit, after starting for treatment in one Tuberculosis unit, after starting treatment in another unit (TU) where(s) he has been treatment in another unit (TU) where(s) he has been registered.registered.

Treatment after default: Treatment after default: A TB patient who received A TB patient who received anti TB treatment for one month or more from any anti TB treatment for one month or more from any source and returns to treatment after having source and returns to treatment after having defaulted, i.e., not taken anti TB drugs defaulted, i.e., not taken anti TB drugs consecutively for two months or more, and who is consecutively for two months or more, and who is found to be sputum smear positive.found to be sputum smear positive.
Failure: Failure: Any TB patient who is smear positive at 5 Any TB patient who is smear positive at 5 months or more after starting treatment. Failure also months or more after starting treatment. Failure also includes a patient who was treated with category III includes a patient who was treated with category III regimen but who becomes smear positive during regimen but who becomes smear positive during treatment.treatment.
Chronic:Chronic: A TB patient who remains smear positive A TB patient who remains smear positive after completing a re-treatment regimen.after completing a re-treatment regimen.

Treatment OutcomesTreatment Outcomes
Cured: Cured: Initially sputum smear positive patient who Initially sputum smear positive patient who has completed treatment and had negative sputum has completed treatment and had negative sputum smears, on at least two occasions, one of which was smears, on at least two occasions, one of which was at the end of treatment.at the end of treatment.
Treatment Completed:Treatment Completed: A sputum smear positive A sputum smear positive patient who has completed treatment, with negative patient who has completed treatment, with negative smears at the end of Intensive phase but none at smears at the end of Intensive phase but none at the end of treatment, or the end of treatment, or
A sputum snear negative patient who has received a A sputum snear negative patient who has received a full course of treatment and has not become smear full course of treatment and has not become smear positive during or at the end of treatment.positive during or at the end of treatment.

Died:Died: Patient who died during the course of Patient who died during the course of treatment, regardless of the cause of death.treatment, regardless of the cause of death.
Failure:Failure: Any TB patient who is smear positive at 5 Any TB patient who is smear positive at 5 months or more after starting treatment ormonths or more after starting treatment or
A patient who was treated with category III but who A patient who was treated with category III but who becomes smear positive during treatment.becomes smear positive during treatment.
Defaulted:Defaulted: A patient who has not taken anti TB A patient who has not taken anti TB drugs for 2 months or more consecutively after drugs for 2 months or more consecutively after starting treatment.starting treatment.
Transferred out:Transferred out: A patient who has been transferred A patient who has been transferred to another TB unit or district and for whom the to another TB unit or district and for whom the treatment result (outcome) is not known.treatment result (outcome) is not known.

Intensive PhaseIntensive Phase
Aims for a rapid killing of bacilliAims for a rapid killing of bacilli A state of non-infectiousness within 2 weeksA state of non-infectiousness within 2 weeks Quick relief of symptomsQuick relief of symptoms Smear negativity by 2 monthsSmear negativity by 2 months Prevent development of drug resistancePrevent development of drug resistance multi-drug regimens and DOTmulti-drug regimens and DOT

Continuation PhaseContinuation Phase
Aims to eliminate remaining bacilliAims to eliminate remaining bacilli Killing of “persisters” prevents relapsesKilling of “persisters” prevents relapses Multi-drug regimens and DOT necessary even Multi-drug regimens and DOT necessary even
though risk of emergence of drug resistance is though risk of emergence of drug resistance is less as fewer bacilli remain less as fewer bacilli remain

Treatment RegimensTreatment Regimens
2H3R3Z3 /
4H3R3
New smear negative and extra-pulmonary, not seriously ill
Cat III
2H3R3Z3E3S3 /
1H3R3Z3E3 /
5H3R3E3
Previously treated smear positive (relapse, failure,
treatment after default)
Cat II
2H3R3Z3E3 /
4H3R3
New smear positive; seriously ill smear negative; seriously ill extra-pulmonary
Cat I

SymptomSymptom Drug Drug Action to be takenAction to be taken
Gastrointestinal Gastrointestinal upsetupset
Any oral medicationAny oral medication Reassure patientReassure patient
Give drugs with less waterGive drugs with less water
Do not give drugs on empty Do not give drugs on empty stomach.stomach.
Itching Itching
Burning in the hands Burning in the hands and feetand feet
IsoniazidIsoniazid Give pyridoxine 100 mg/day until Give pyridoxine 100 mg/day until symptoms subsidesymptoms subside
Joint painsJoint pains PyrazinamidePyrazinamide evaluateevaluate
Impaired visionImpaired vision EthambutolEthambutol STOP ethambutol and evaluateSTOP ethambutol and evaluate
Ringing in the earsRinging in the ears
Loss of hearingLoss of hearing
StreptomycinStreptomycin STOP streptomycin and evaluateSTOP streptomycin and evaluate
JaundiceJaundice Isoniazid, Rifampicin, Isoniazid, Rifampicin, PyrazinamidePyrazinamide
STOP if liver enzymes elevated 5 STOP if liver enzymes elevated 5 times of normal.times of normal.
Side Effect of Anti-TB Drugs

Domiciliary treatmentDomiciliary treatment
Short course chemotherapyShort course chemotherapy
Intermittent chemotherapyIntermittent chemotherapy
Directly observed treatmentDirectly observed treatment

Advantages of domiciliary Advantages of domiciliary chemotherapychemotherapy
Domiciliary chemotherapy is as effective Domiciliary chemotherapy is as effective
as sanatorium treatmentas sanatorium treatment
No additional benefit by bed rest, special No additional benefit by bed rest, special
diet etcdiet etc
No need for routine hospitalisationNo need for routine hospitalisation
Economic benefitEconomic benefit

Short Coures Chemotherapy Short Coures Chemotherapy (SCC)(SCC)
Six months of chemotherapy gives favourable results Six months of chemotherapy gives favourable results
when compared with longer terms of treatment for new when compared with longer terms of treatment for new
sputum positive TB patients.sputum positive TB patients.
Duration of treatment are adequate to prevent Duration of treatment are adequate to prevent
emergence of drug resistance.emergence of drug resistance.
SCC is more convenient and economical than SCC is more convenient and economical than
conventional treatment with longer durations.conventional treatment with longer durations.
The shorter period of time makes direct observation The shorter period of time makes direct observation
more feasible and improves patient adherence to more feasible and improves patient adherence to
tretment.tretment.

Intermittent TreatmentIntermittent Treatment As effective as daily treatmentAs effective as daily treatment
Less adverse reactionsLess adverse reactions Total drugs consumed is lessTotal drugs consumed is less Less costlyLess costly Less number of doses Less number of doses
facilitates treatment observation as less facilitates treatment observation as less number of patient visits required and prevents number of patient visits required and prevents concealed irregularity concealed irregularity

Directly Observed Treatment
DOT ensures the best possible results in treatment of
TB.
Here an observer watches and supports the patient in
taking their drugs, thereby ensuring that the patient
receives the medication.
Direct observation ensures treatment for the entire
course o with the right drugso in the right doseso at the right intervals

Patients swallows drugs in presence of observer

Why is it necessary to directly observe treatment?
At least 1/3 of patients on self-administered Rx fail to adhere to Rx
Impossible to predict which patients will take medicines
DOT necessary at least in the IP of Rx to ensure adherence and smear conversion
TB patient missing 1 attendance can be traced immediately and counseled

““This use of supervised treatment This use of supervised treatment ((now known now known
as directly observed treatmentas directly observed treatment) ) in which patients in which patients
are observed taking their anti-TB medications, are observed taking their anti-TB medications,
was shown to be essential in India”was shown to be essential in India” Fox W. Fox W.
1961 1961
Based on studies from TRCBased on studies from TRC

DDirectly irectly OObserved bserved TTreatment reatment is the Standard of Careis the Standard of Care
““Every patient with TB in this country should receiveEvery patient with TB in this country should receive
DOT” DOT” (Iseman, NEJM, 1993)(Iseman, NEJM, 1993)
““DOT has emerged as the standard of care”DOT has emerged as the standard of care”
(Bayer, Lancet, 1995)(Bayer, Lancet, 1995)
““DOT seems imperative … where the disease has DOT seems imperative … where the disease has
become epidemic”become epidemic” (Chaulk, JAMA, 1996)(Chaulk, JAMA, 1996)

DOTS- Plus The WHO working group on DOTS- Plus for MDR-TB was established in 1999 to lead the global effort to control MDR-TB (Cat. IV) (Whose sputum culture isolates are resistant to at least isoniazid and rifampicin).
Treatment is for a minimum duration of 18 months beyond sputum conversion (At least to sets of consecutive negative smears and cultures taken 30 days apart).
Regimens should consist of at least four drugs with either certain, or almost certain, effectiveness.

Drugs are administered at least six days a week.
In most cases, an injectable agent and a fluoroquinolone form the core of the regimen.
An injectable agent (an aminoglycoside or capreomycin) is used for a minimum of 6 months.

XDR- TB:XDR- TB:
XDR – TB is defined as ……..XDR – TB is defined as ……..
MDR MDR
Plus resistance to any fluoroquinolone, Plus resistance to any fluoroquinolone,
And at least one of the second line injectable And at least one of the second line injectable drugs, capreomycin, kanamycin or amikacin.drugs, capreomycin, kanamycin or amikacin.
Such extensive resistance markedly limits Such extensive resistance markedly limits treatment options because few effective and treatment options because few effective and reasonably well tolerated alternative drugs are reasonably well tolerated alternative drugs are available.available.

Tuberculosis in ChildrenTuberculosis in Children
TB in children represents 5-15% of all TB cases.TB in children represents 5-15% of all TB cases. DiagnosisDiagnosis
– Younger children with pulmonary TB rarely cough Younger children with pulmonary TB rarely cough out sputum as they usually swallow it.out sputum as they usually swallow it.
– Diagnosis of pulmonary TB by sputum Diagnosis of pulmonary TB by sputum microscopy is therefore very unlikely among microscopy is therefore very unlikely among smaller children.smaller children.
– Gastric lavage or laryngeal swabs are difficult to Gastric lavage or laryngeal swabs are difficult to carry out.carry out.
– Bacteriological confirmation is not possible in Bacteriological confirmation is not possible in most cases.most cases.

– Children will be suspected of having pulmonary Children will be suspected of having pulmonary TB if they present with fever and/or cough for TB if they present with fever and/or cough for more than 3 weeks, with or without weight loss or more than 3 weeks, with or without weight loss or no weight gain.no weight gain.
– TB should also be suspected if there is a history TB should also be suspected if there is a history of contact with a suspected or diagnosed case of of contact with a suspected or diagnosed case of active TB disease in the last 2 yrs.active TB disease in the last 2 yrs.
– Diagnosis of TB in children should be based on a Diagnosis of TB in children should be based on a combination of clinical presentation, sputum combination of clinical presentation, sputum examination (wherever possible), chest X-ray, examination (wherever possible), chest X-ray, mantoux test and history of contact.mantoux test and history of contact.

Treatment Treatment
Intermittent short-course chemotherapy given under Intermittent short-course chemotherapy given under direct observation as for adult patients, based on the direct observation as for adult patients, based on the weight of the children.weight of the children.
For children with TB meningitis on cat I regimen, the For children with TB meningitis on cat I regimen, the 4 drugs used during intensive phase should be H, 4 drugs used during intensive phase should be H, R,Z and S (instead of HRZE) as ethambutol does R,Z and S (instead of HRZE) as ethambutol does not cross the blood brain barrier easily.not cross the blood brain barrier easily.
Steroids are recommended during the early part of Steroids are recommended during the early part of the treatment of TB meningitis, with the doses being the treatment of TB meningitis, with the doses being tapered off over 6 to 8 weeks.tapered off over 6 to 8 weeks.

Chemoprophylaxis Chemoprophylaxis
Asymptomatic children under 6 yrs of age, exposed Asymptomatic children under 6 yrs of age, exposed to a patient with infectious (smear positive) TB from to a patient with infectious (smear positive) TB from the same household, need to be given 6 months of the same household, need to be given 6 months of daily isoniazid (5 mg/kg) as chemoprphylaxis daily isoniazid (5 mg/kg) as chemoprphylaxis against the disease.against the disease.

Monitoring & Evaluation Monitoring & Evaluation Whenever possible , follow up sputum examination Whenever possible , follow up sputum examination
is to be performed with the same frequency as in is to be performed with the same frequency as in adults.adults.
Since this may not be possible for the majority of Since this may not be possible for the majority of children with pulmonary TB, clinical or symptomatic children with pulmonary TB, clinical or symptomatic improvement is to be assessed at the end of the improvement is to be assessed at the end of the intensive phase of treatment and at the end of the intensive phase of treatment and at the end of the treatment.treatment.
Improvement should be judged by absence of fever Improvement should be judged by absence of fever or cough, a decrease in the size of lymph node(s), or cough, a decrease in the size of lymph node(s), weight gain, radiological assessment etc.weight gain, radiological assessment etc.

Diagnostic Algorithm for Pediatric Diagnostic Algorithm for Pediatric TuberculosisTuberculosis

Pulmonary TB Suspect
-Fever and/or cough 3 weeks
- Loss of wt./No wt. gain
- History of contact with suspected or diagnosed case of active TB
Is expectoration present?
If yes, examine 3 sputum smears
If no, then diagnosed based on a combination of
Clinical presentation
Chest X-ray
Mantoux test
History of contact
2 or 3 positives 3 negatives
Antibiotics 10-14 days
Cough Persists
Repeat 3 sputum examinations
Sputum positive TB
1 Positive
X- Ray
Suggestive of TB Negative of TB
Non TB
Negative 2 or 3 positives
X-Rays + Mantoux
Sputum Positive TB
Suggestive of TB
Sputum negative TB

Algorithm for clinical monitoringAlgorithm for clinical monitoring

Patient on treatment
Review at 2 months shows satisfactory response assessed by:
- improvement in symptoms
- no weight loss and or weight gain
Review at 2 months shows non - satisfactory response assessed by
- poor or non adherence to treatment
- weight loss
- worsening of symptoms
Follow up clinically
Clinical assessment and X-ray at completion of treatment
Refer to for assessment
(Consider sputum examination)
Sputum positive
Failure
Category II
Sputum negative or not available
-Review diagnosis
- Extend IP by 1 month
No improvement = Paediatric non-responder

TB treatment in HIV infected TB treatment in HIV infected patients patients
All new TB cases known to be HIV positive are All new TB cases known to be HIV positive are classified as seriously ill and treated with category I classified as seriously ill and treated with category I regimen. The retreatment cases are to be treated regimen. The retreatment cases are to be treated with category II regimen.with category II regimen.
The HIV positive status should not be mentioned in The HIV positive status should not be mentioned in any RNTCP records.any RNTCP records.
Routine HIV testing of all TB suspected patients is Routine HIV testing of all TB suspected patients is NOT the national policy.NOT the national policy.
Treatment interruption, due to higher occurrence of Treatment interruption, due to higher occurrence of adverse drug reactions or intercurrent opportunistic adverse drug reactions or intercurrent opportunistic infections, could also lead to an increased risk of infections, could also lead to an increased risk of relapse of TB.relapse of TB.

The current recommendations on ART are to use a The current recommendations on ART are to use a triple drug combination. A combination of triple drug combination. A combination of stavudine/zidovudine plus lamivudine plus stavudine/zidovudine plus lamivudine plus Efavirenz/Nevirapine is usually used.Efavirenz/Nevirapine is usually used.
Co-administration of Rifampicin with any of the Co-administration of Rifampicin with any of the protease inhibitors or non-nucleoside reverse protease inhibitors or non-nucleoside reverse transcriptase inhibitors should be avoided as transcriptase inhibitors should be avoided as Rifampicin induces cytochrome P450 and Rifampicin induces cytochrome P450 and substantially decrease blood levels of these substantially decrease blood levels of these antiretroviral drugs. antiretroviral drugs.
In TB patients co-infected with HIV, TB treatment In TB patients co-infected with HIV, TB treatment should be completed prior to starting ART, unless should be completed prior to starting ART, unless there is a high risk of HIV disease progression and there is a high risk of HIV disease progression and death during the period of TB treatment (i.e. a CD4 death during the period of TB treatment (i.e. a CD4 count <200/cmm or the presence of disseminated count <200/cmm or the presence of disseminated TB)TB)

ConclusionConclusion
RNTCP diagnosis and treatment RNTCP diagnosis and treatment strategies are based on scientific evidencestrategies are based on scientific evidence
In additionIn addition– It is consistent with international WHO It is consistent with international WHO
guidelines guidelines – It is consistent with International Standards of It is consistent with International Standards of
TB CareTB Care– Well documented and good RNTCP treatment Well documented and good RNTCP treatment
outcomes in millions of patients supports the outcomes in millions of patients supports the soundness of the treatment strategiessoundness of the treatment strategies