Embed Size (px)
Citation preview
FRACTURE HUMERUS SHAFT IN ADULTS
TEAM D AUDIT
KHOULA HOSPITAL
Supervised by
Dr. Ghassan Al YASSRI
Dr. Ahmed Al-Gazzar
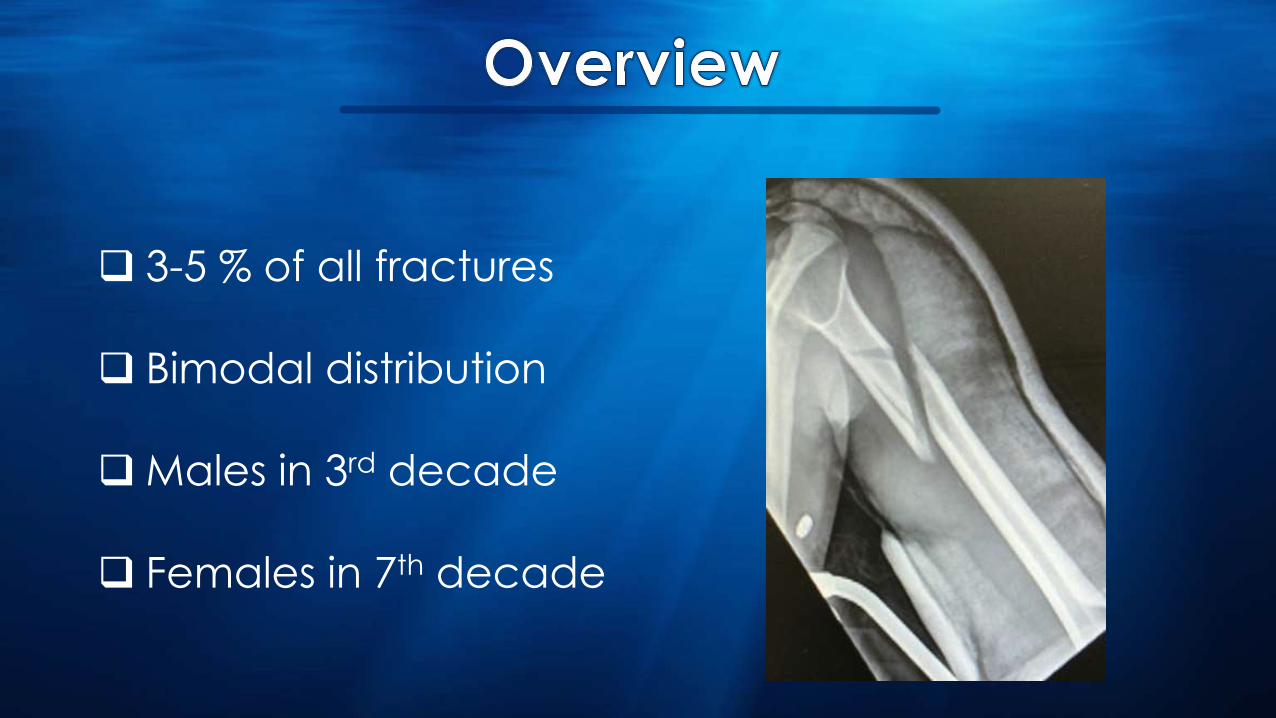
3-5 % of all fractures
Bimodal distribution
Males in 3rd decade
Females in 7th decade
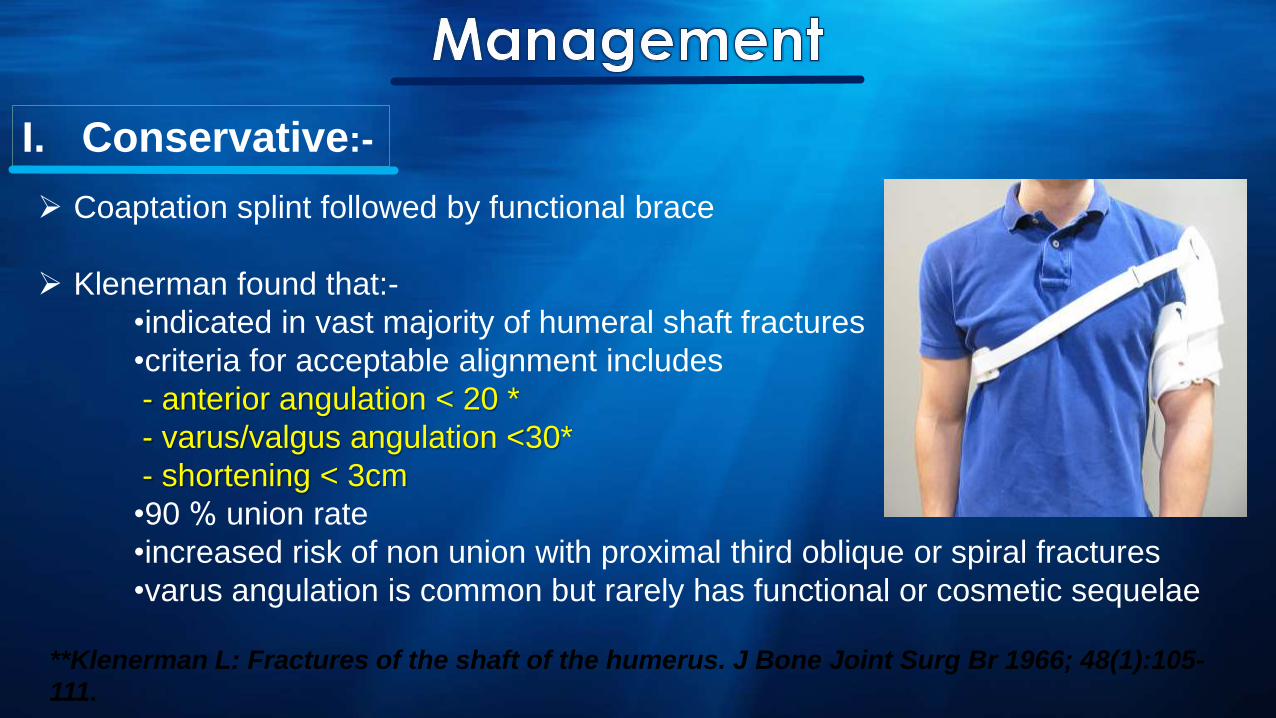
Coaptation splint followed by functional brace
Klenerman found that:-
•indicated in vast majority of humeral shaft fractures
•criteria for acceptable alignment includes
- anterior angulation < 20 *
- varus/valgus angulation <30*
- shortening < 3cm
•90 % union rate
•increased risk of non union with proximal third oblique or spiral fractures
•varus angulation is common but rarely has functional or cosmetic sequelae
**Klenerman L: Fractures of the shaft of the humerus. J Bone Joint Surg Br 1966; 48(1):105-
111.
I. Conservative:-
In the largest clinical analysis to date, Sarmiento et al reported on 922
patients treated with a functional brace for both closed and open
humeral shaft fractures:-
98% of all closed injuries and 94% of all open fractures healed.
Malunion, described as angular deformity greater than 16 degree in
any plane, 13% and 19%.
Only 2% of patients reported loss of shoulder motion
**Sarmiento A, Zagorski J, Zych G, Latta L, Capps C. Functional bracing for the treatment of fractures of
the humeral diaphysis. J Bone Joint Surg Am 2000;82:478-86.

**Sarmiento A, Zagorski J, Zych G, Latta L, Capps C. Functional bracing for the treatment of
fractures of the humeral diaphysis. J Bone Joint Surg Am 2000;82:478-86.
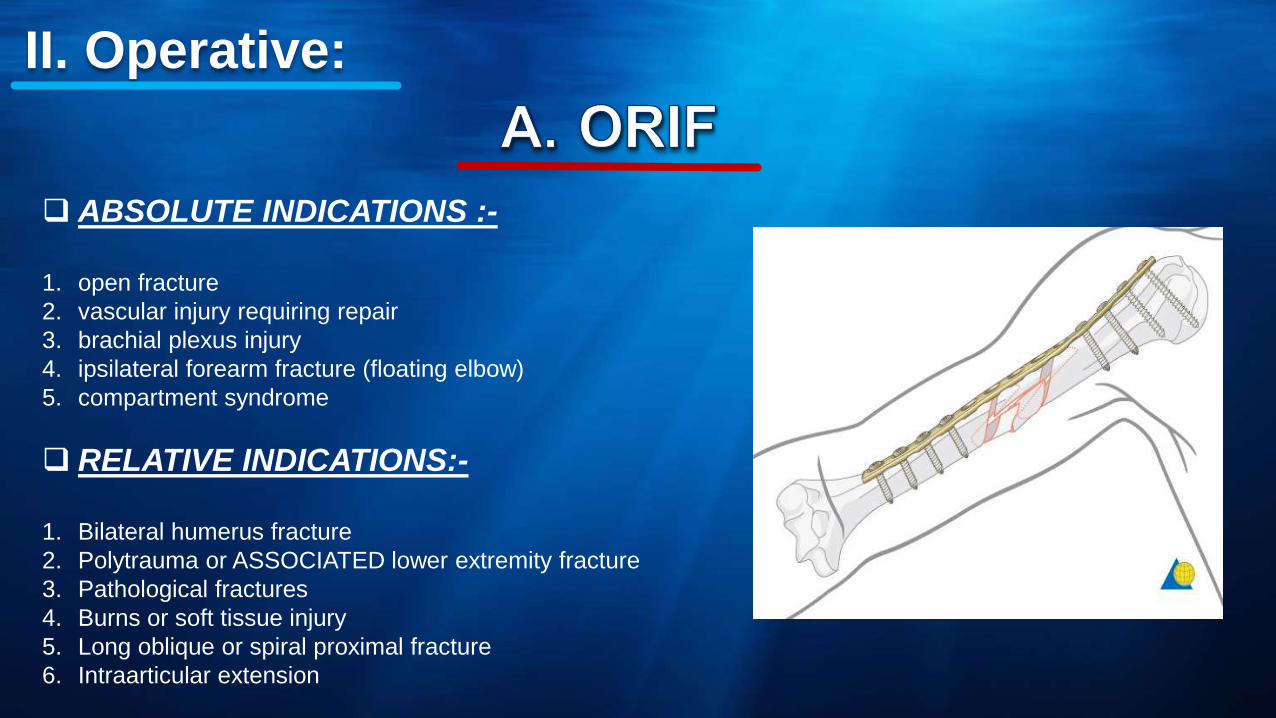
ABSOLUTE INDICATIONS :-
1. open fracture
2. vascular injury requiring repair
3. brachial plexus injury
4. ipsilateral forearm fracture (floating elbow)
5. compartment syndrome
RELATIVE INDICATIONS:-
1. Bilateral humerus fracture
2. Polytrauma or ASSOCIATED lower extremity fracture
3. Pathological fractures
4. Burns or soft tissue injury
5. Long oblique or spiral proximal fracture
6. Intraarticular extension
II. Operative:
RELATIVE INDICATIONS:-
1. pathologic fractures
2. segmental fractures
3. severe osteoporotic bone
4. overlying skin compromise limits open approach
5. polytrauma

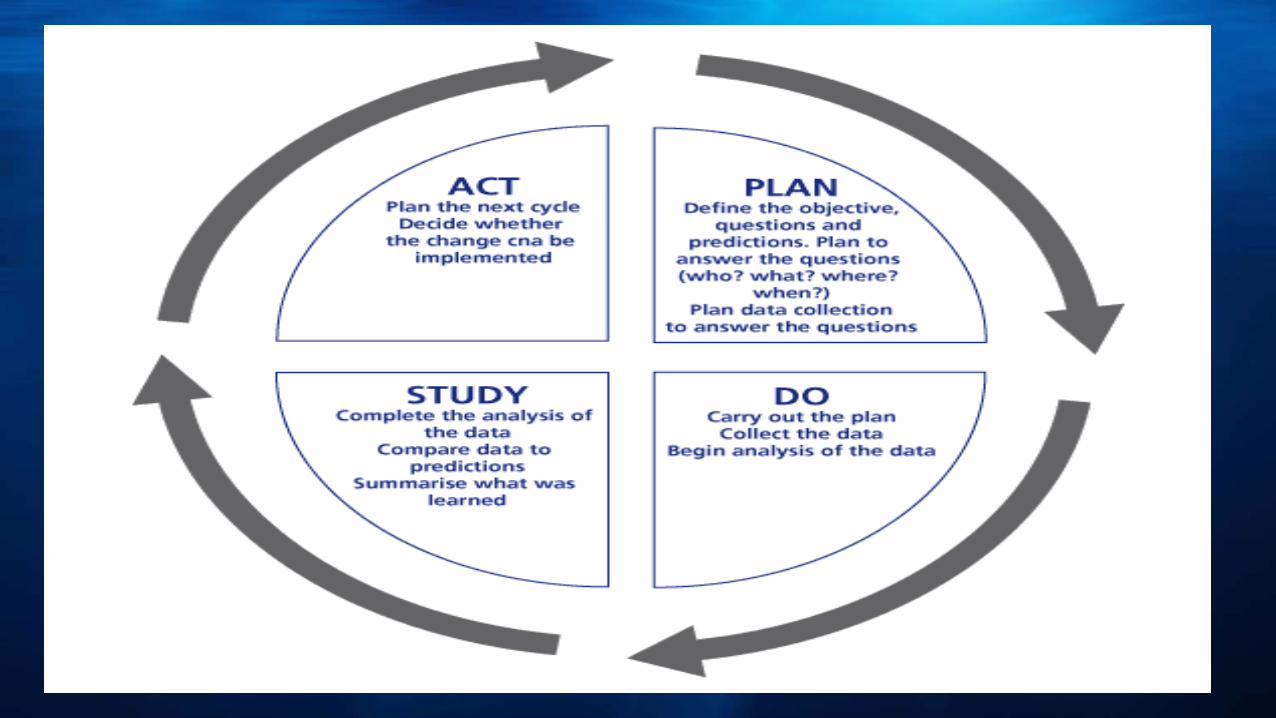
AUDIT

Outcome of the fracture
Risk factors of associated injuries with ORIF , specially the
iatrogenic radial nerve injury.
PLAN

We have analysed 57 consecutive fractures of the
humeral shaft treated over two-years period from July
2012 to July 2014
The fractures were defined by their type “ closed
versus open and by AO morphology
The data of the study is collected from khoula hospital
electronic system
We have reviewed 57 patients with fracture humerus shaft
-43
-14
55 cases with primary ORIF and 2 cases with revision fixation
Male : Female is 3:1
Age ranges from 16 – 72 years
Average age 33.2
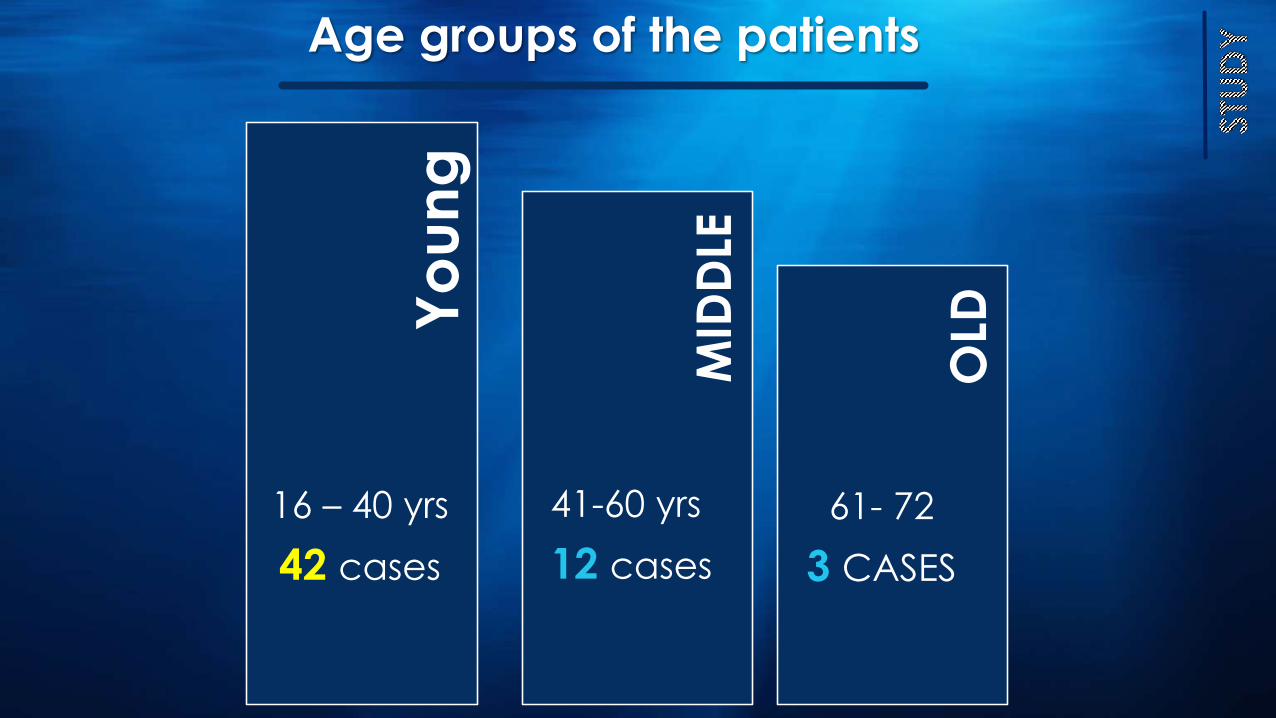
OLD
MID
DLE
Yo
un
g16 – 40 yrs
42 cases
41-60 yrs
12 cases
61- 72
3 CASES
Age groups of the patients
Interval between the incidence of injury and surgery in primary
cases ranged from 0 day to 20 weeks.
The 2 revision cases one done after 21 weeks due to re-fracture
and the other done after 3 years due to non union.
Types of Fractures
Closed fractures
• 54 cases
Open fractures
• 3 Cases
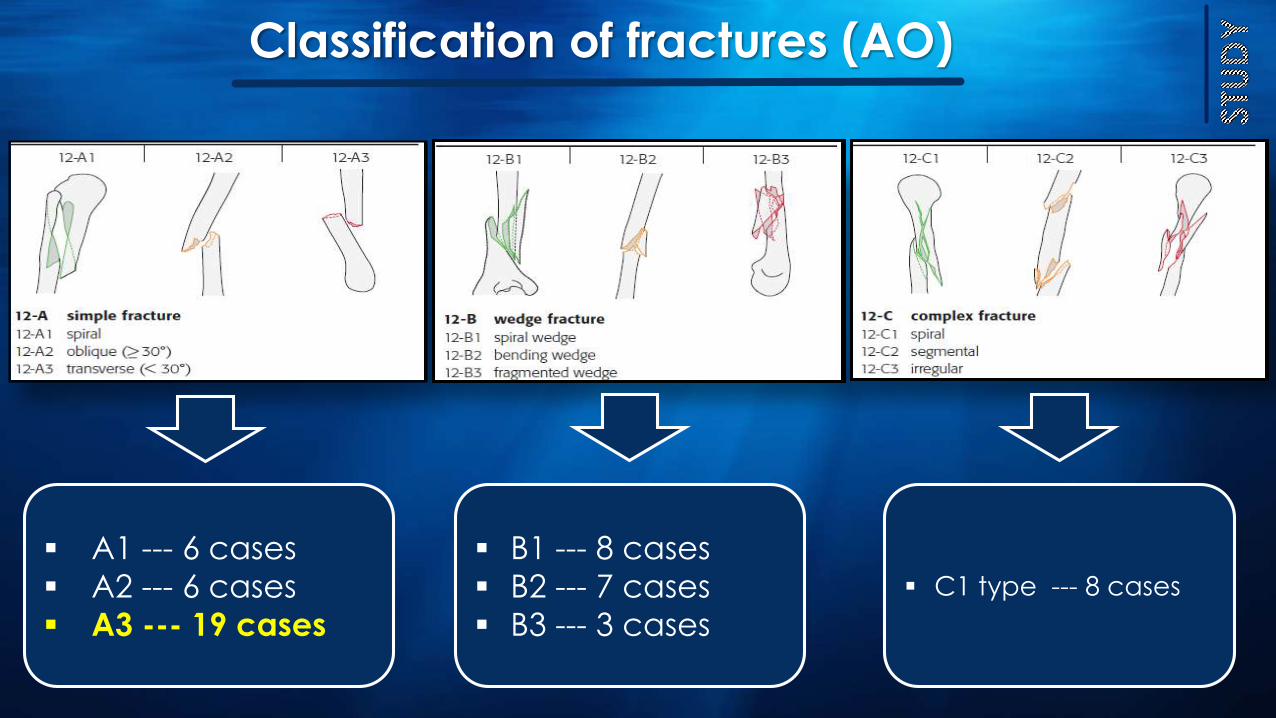
A1 --- 6 cases
A2 --- 6 cases
A3 --- 19 cases
B1 --- 8 cases
B2 --- 7 cases
B3 --- 3 cases
C1 type --- 8 cases
Classification of fractures (AO)
Associated Injuries
Radial nerve injury
8 cases
Brachial artery injury
2 cases
Multiple nerve injury
1 case
6 cases
4 primary fractures
2 revision fractures
51 cases
ORIFby
plating
ORIFby
plating + bone graft
Operative Technique
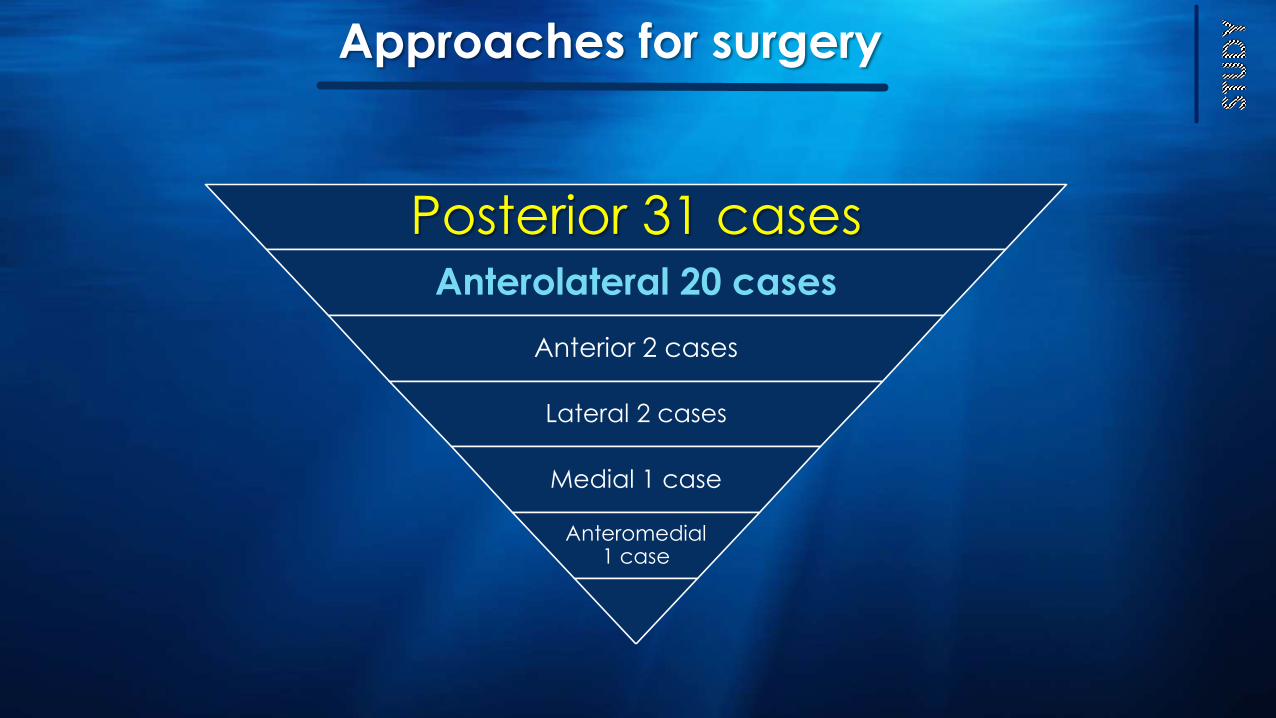
Posterior 31 cases Anterolateral 20 cases
Anterior 2 cases
Lateral 2 cases
Medial 1 case
Anteromedial 1 case
Approaches for surgery

Medical officer
1 case
Resident
1 case
Sr.consultant
2 cases specialist
25 cases
Sr.specialist
28 cases
Level of Surgeon
Supervision of surgery
supervised by Sr. consultant
•2 cases
Supervised by Sr. Specialist
•15 cases
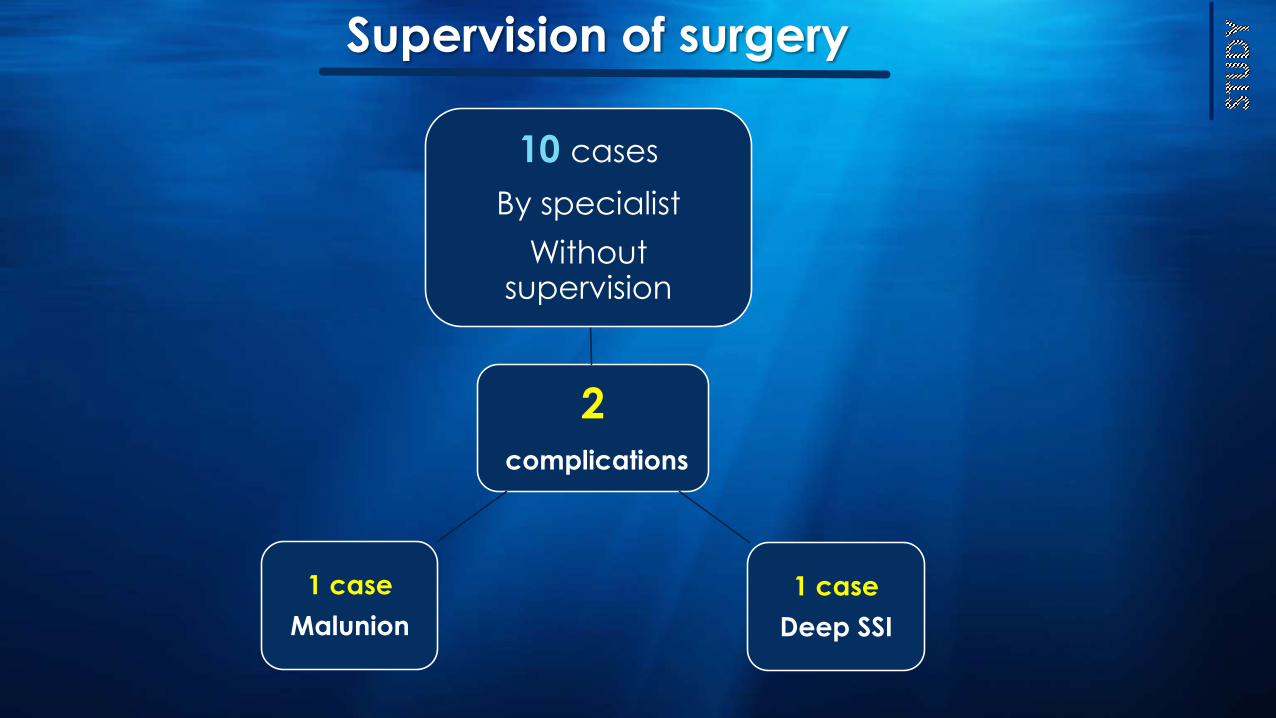
2
complications
10 cases
By specialist
Without supervision
1 case
Deep SSI
1 case
Malunion
Supervision of surgery
Complications of the fracture
9 cases with radial nerve injury 19 %
8 cases initial isolated Radial nerve injury
1 case with multiple upper limb nerve injury
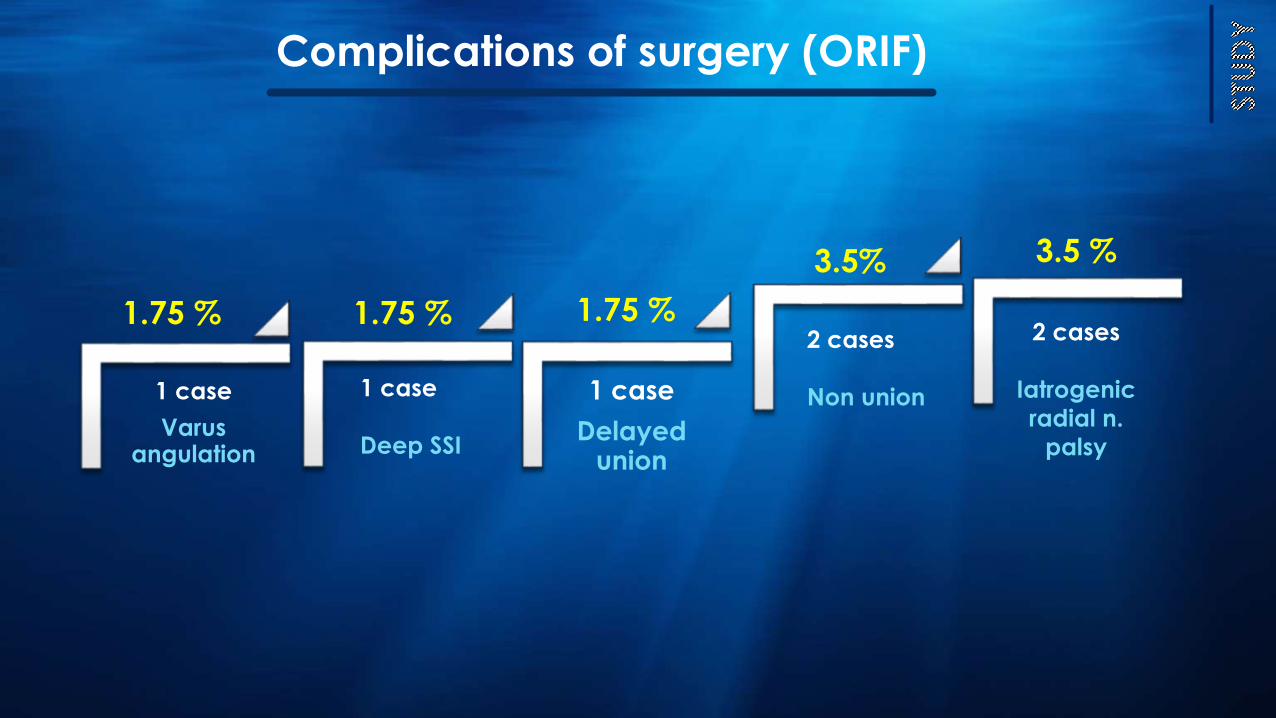
Complications of surgery (ORIF)
1 case
Varusangulation
1 case
Delayed union
1 case
Deep SSI
2 cases
Non union
2 cases
Iatrogenic
radial n.
palsy
1.75 % 1.75 % 1.75 %
3.5% 3.5 %
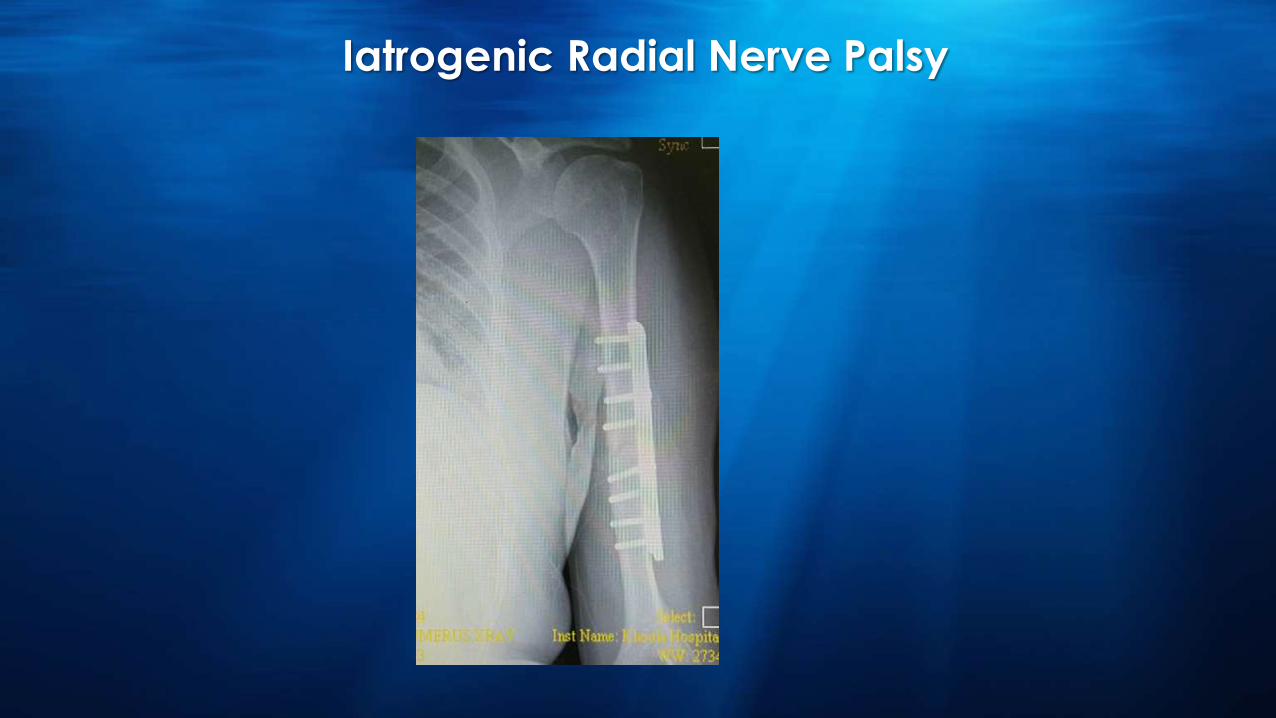
Iatrogenic Radial Nerve Palsy
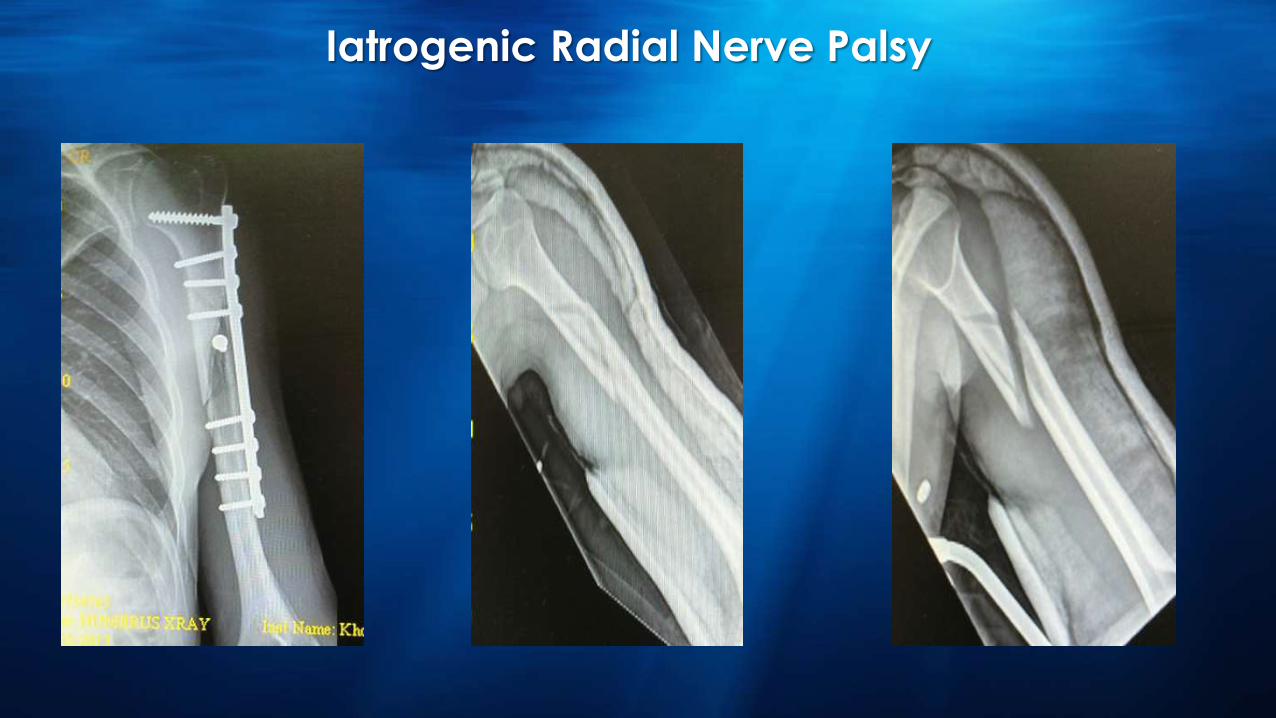
Iatrogenic Radial Nerve Palsy
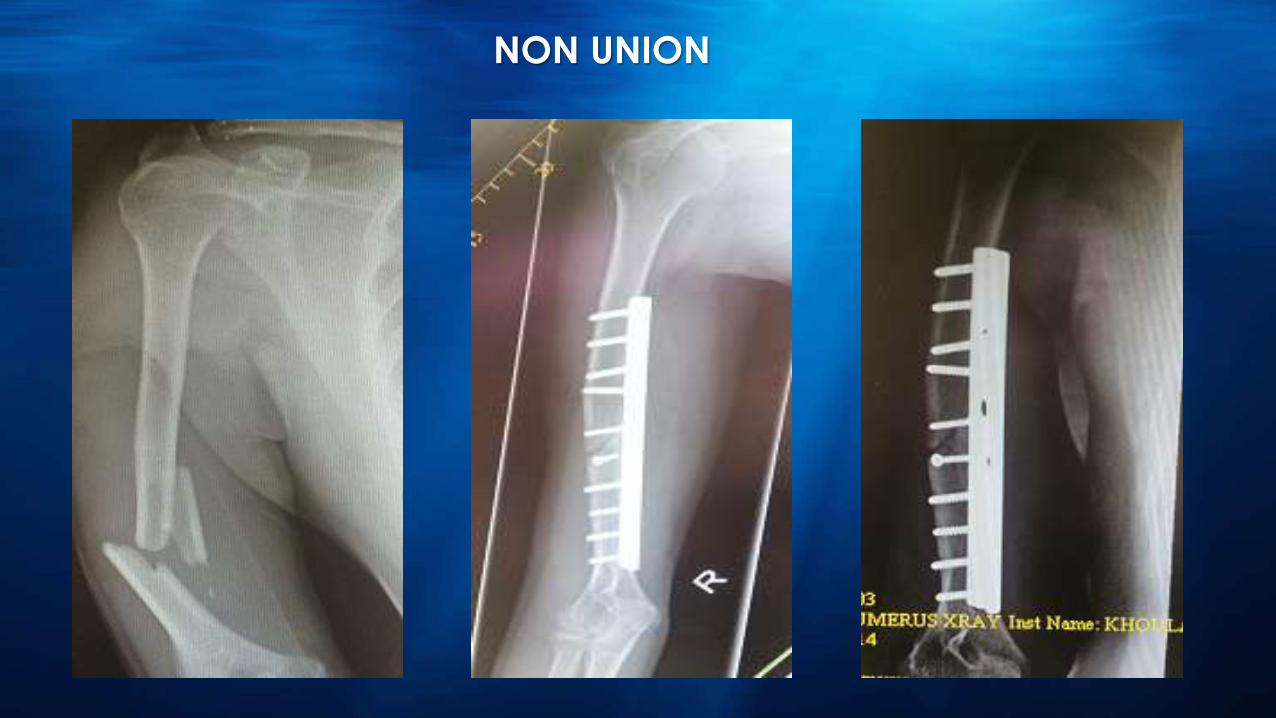
NON UNION
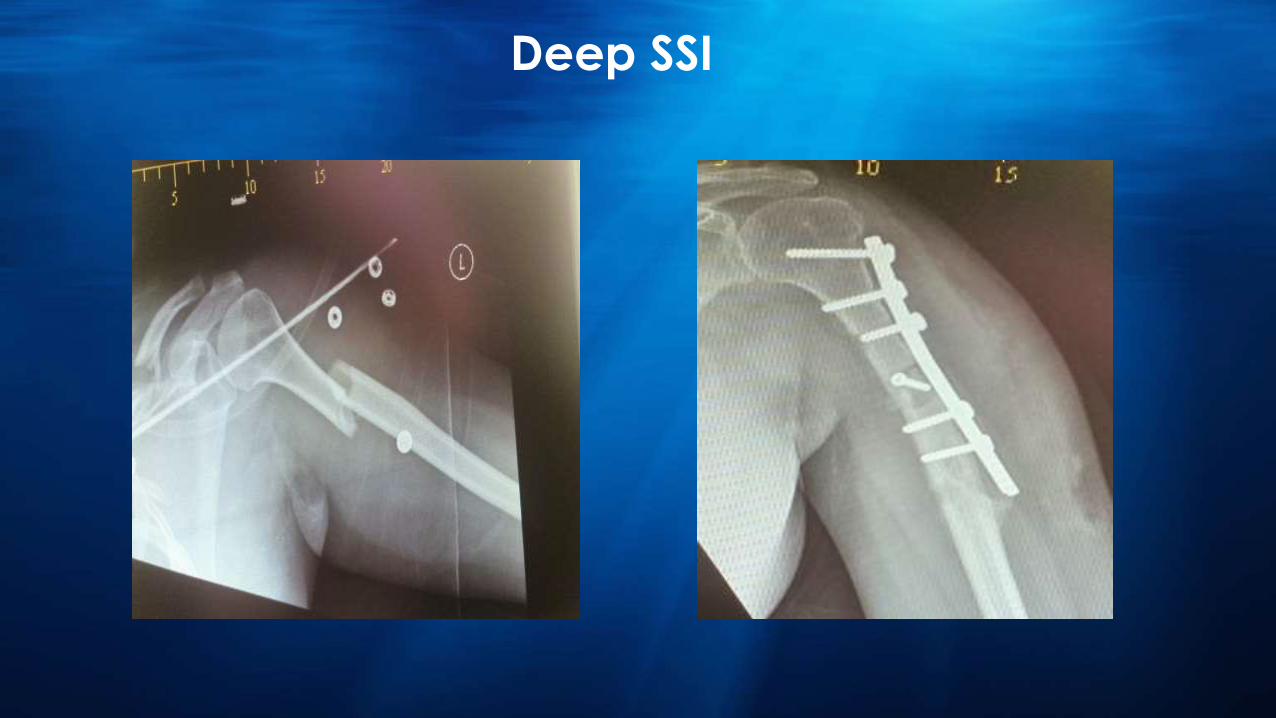
Deep SSI
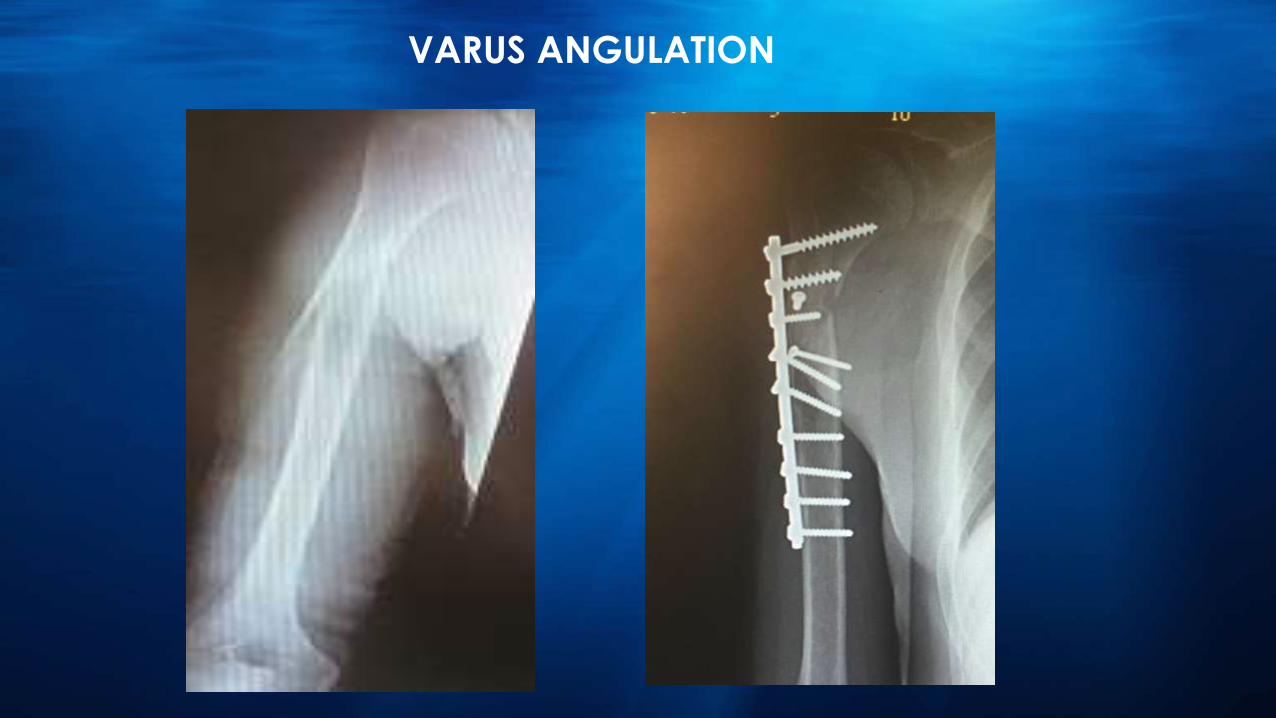
VARUS ANGULATION
9 cases of initial radial nerve injury:-
5 cases recovered completely
2 cases recovered partially
2 cases didn’t recover
There was no proper documentation of the radial nerve deficit regarding sensory and motor
Major morbidity of the fracture was the radial nerve injury
2 cases of Iatrogenic radial nerve injury didn’t recover.
Both cases were operated through anterolateral approach
Both cases were operated by specialist and supervised by Sr.
Specialist .
One case had shown radial nerve degeneration by EMG
study done after 1 year of injury .
The other case was shown to the clinic only up to 4 months
after surgery with no recovery.
Injury to the radial nerve with neuropraxia is the most frequently
encountered nerve deficit associated with humeral fractures and is
found in up to 18% of all patients.spontaneous recovery over a period
of 4 months occurs in 70% to 92% of patients managed with
observation; therefore, its presence is not an indication for open
management and nerve exploration.
Shao Y, Harwood P, Grotz M, Limb D, Giannoudis P. Radial nerve palsy associated with fractures of the
shaft of the humerus: a systematic review. J Bone Joint Surg Br 2005;87:1647-52. doi:10.1302/0301
620X.87B12.16132
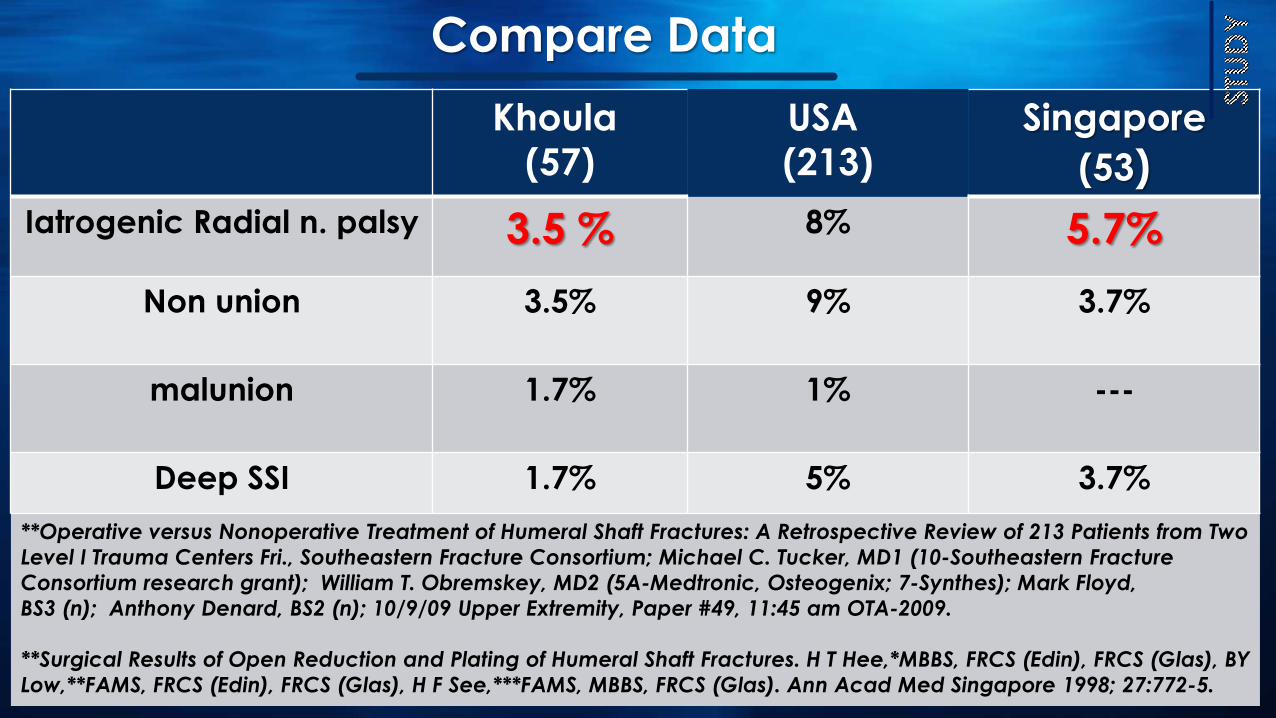
Compare Data
Khoula
(57)
USA
(213)
Singapore
(53)
Iatrogenic Radial n. palsy 3.5 % 8% 5.7%
Non union 3.5% 9% 3.7%
malunion 1.7% 1% ---
Deep SSI 1.7% 5% 3.7%
**Operative versus Nonoperative Treatment of Humeral Shaft Fractures: A Retrospective Review of 213 Patients from Two
Level I Trauma Centers Fri., Southeastern Fracture Consortium; Michael C. Tucker, MD1 (10-Southeastern Fracture
Consortium research grant); William T. Obremskey, MD2 (5A-Medtronic, Osteogenix; 7-Synthes); Mark Floyd,
BS3 (n); Anthony Denard, BS2 (n); 10/9/09 Upper Extremity, Paper #49, 11:45 am OTA-2009.
**Surgical Results of Open Reduction and Plating of Humeral Shaft Fractures. H T Hee,*MBBS, FRCS (Edin), FRCS (Glas), BY
Low,**FAMS, FRCS (Edin), FRCS (Glas), H F See,***FAMS, MBBS, FRCS (Glas). Ann Acad Med Singapore 1998; 27:772-5.
The surgical approach used in the analysed cases with iatrogenic radial
nerve palsy was anterolateral approach That means the injury to the
nerve could happened due to over traction during reduction or during
putting the hardware.
Surgeries done by specialist level with no supervision had a complication
rate of 20 %
Conclusion
Proper assessment of the neurologic deficit at the time of injury ,
pre operative and postoperative is of greatest importance.
Plan the proper approach prior to surgery according to type of
fracture , plan of fixation , associated injuries , skills of the
operating surgeon.
Where is the nerve
Length of observation for radial n. palsy remains a subject of debate.
During the observation period: Brace & aggressive ROM physiotherapy.
Recommendations


Thank you