Embed Size (px)
DESCRIPTION
Citation preview

Oncotype DX® Breast Cancer Assay: Results and Impact on Treatment Decisions
The French experience
Frédérique Penault-‐Llorca

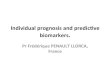
The Recurrence Score® Result Uses Key Genes Linked to CriEcal Molecular Pathways
16 BREAST CANCER RELATED GENES
ER PR Bcl2
SCUBE2
GRB7 HER2
Ki-‐67 STK15 Survivin Cyclin B1 MYBL2
Stromelysin 3 Cathepsin L2
GSTM1
CD68
BAG1
Beta-‐acKn GAPDH RPLPO GUS TFRC
5 REFERENCE GENES
Estrogen ProliferaKon HER2 Invasion Others
Paik S, et al. N Engl J Med. 2004;351:2817-‐2826. 2

The Recurrence Score® Result Has Demonstrated Clinical Validity in Numerous Landmark Studies • NSABP B-‐14: The Oncotype DX® Assay Is PrognosEc of
Distant Recurrence in Tamoxifen-‐Treated PaEents
3 10-‐Year rate of recurrence = 30.5% for High RS vs 6.8% for Low RS, p<0,001
Paik S, et al. N Engl J Med. 2004;351:2817-‐2826.

The Recurrence Score® Result Has Demonstrated Clinical Validity in Numerous Landmark Studies • NSABP B-‐20: Only the Oncotype DX® Assay is Currently Validated to Predict
Benefit From Chemotherapy
4
PATIENTS WITH HIGH RECURRENCE SCORE® RESULT 28% absolute benefit from tamoxifen + chemotherapy
4.4% absolute benefit from tamoxifen + chemotherapy
Paik S, et al. J Clin Oncol. 2006;24:3726-‐3734.

The Recurrence Score® Result Has Demonstrated Clinical Validity in Numerous Landmark Studies
• SWOG 8814: Breast Cancer-‐Specific Survival of Node-‐PosiEve PaEents by Treatment and Recurrence Score® Group
5
No benefit to CAF over Kme for low Recurrence
Score
High benefit to CAF over Kme for high
Recurrence Score
Albain KS, et al. Lancet Oncol. 2010;11(1):55-‐65.

The Recurrence Score® Result Has Demonstrated Clinical Validity in Numerous Landmark Studies • Validated results from well designed randomized cooperaEve group
clinical trials in homogenous paEent populaEons
PrognosKc for distant recurrence and predicKve for
treatment benefit
6

The Oncotype DX® Assay Provides Reproducible Results in Relevant PaEents Across a ConEnuum of ER+ Breast Cancer
Study ClassificaKon Randomized Clinical Trial
Protocol-‐Specified Treatment
Clinical Outcome Assessed
NSABP B-‐14 (2004)
ValidaKon/ Confirmatory X X 10-‐year distant recurrence rate (6.8%, 14.3%, 30.5% for low,
intermediate, high Recurrence Score® risk groups)
Gianni (2005) SupporKve X Pathologic complete response to neoadjuvant chemotherapy (high Recurrence Score was associated with higher likelihood of pCR; P = 0.005)
NSABP B-‐20 (2006)
ValidaKon/ Confirmatory X X
10-‐year distant recurrence rate (risk reducEon from the addiEon of chemotherapy in the high-‐risk group; no demonstrable relaEve risk reducEon in the low-‐risk group (0.26 vs 1.31))
Kaiser (2006) ValidaKon/ Confirmatory
10-‐year risk of breast cancer death (2.8%, 10.7%, 15.5% for low-‐, intermediate-‐, and high-‐risk groups)
Chang (2007) SupporKve X Clinical complete response to neoadjuvant chemotherapy (> 1.7-‐fold increase for paEents with high vs low score)
ECOG 2197 (2008) SupporKve X X
11.5-‐year disease-‐free recurrence (score was a significant predictor of recurrence including node-‐negaEve and node-‐posiEve disease; P < 0.0001)
Akashi-‐Tanaka (2009) SupporKve X 5-‐year recurrence-‐free survival (100%, 84%, and 73% for low-‐,
intermediate-‐, and high-‐risk groups)
SWOG 8814 (2010)
ValidaKon/ Confirmatory X X
10-‐year disease-‐free survival (60% vs 43% for low-‐ vs high-‐risk groups); 10-‐year breast cancer specific survival (low 92% T vs 87% CAF-‐T and high 54% T vs 73% CAF-‐T; test for interacEon between score and treatment P = 0.021)
Burke E, et al. Poster at St. Gallen Intn. Breast Cancer Conference. 2013. 7 Burke E, et al. Poster at St. Gallen Intn. Breast Cancer Conference. 2013.

The Oncotype DX® Assay Provides Reproducible Results in Relevant PaEents Across a ConEnuum of ER+ Breast Cancer (Cont.)
Study ClassificaKon Randomized Clinical Trial
Protocol-‐Specified Treatment
Clinical Outcome Assessed
TransATAC (2010) ValidaEon/ Confirmatory X X
9-‐year distant recurrence (4%, 12%, and 25% in low-‐, intermediate-‐, and high node-‐negaEve risk groups, 17%, 28%, and 49% in node-‐posiEve risk groups)
Toi (2010) ValidaEon/ Confirmatory
10-‐year distant recurrence risk (3.3% , 0%, 24.8% for low-‐, intermediate-‐, high-‐risk node-‐negaEve groups; low vs high P < 0.001)
Masuda (2001) SupporKve X Clinical response to neoadjuvant hormonal therapy (59%, 59%, 20% for low-‐, intermediate-‐, and high-‐risk groups)
Yardley (2011) SupporKve X Pathologic complete response to neoadjuvant chemotherapy (0%, 0%, 26% for low-‐, intermediate-‐, and high-‐risk groups; Mantel-‐Haenzel χ2 P = 0.002)
NSABP B-‐28 (2012) SupporKve X X 10-‐year distant recurrence-‐free interval (75.8%, 57.0%, and 48.0% for
low-‐, intermediate-‐, and high-‐risk groups); P < 0.001)
Burke E, et al. Poster at St. Gallen Intn. Breast Cancer Conference. 2013. 8
13 studies that included > 5,700 paEents (>3,400 node-‐negaEve and >2,080 node-‐posiEve)
Burke E, et al. Poster at St. Gallen Intn. Breast Cancer Conference. 2013.

The Oncotype DX® Assay
The Only MulE-‐gene Assay Incorporated into 4 Major Guidelines to Predict Adjuvant
Chemotherapy Benefit in ER+, HER2-‐ Early Stage Breast Cancer
1 NCCN PracEce Guidelines in Oncology. V.3.2013. 2 Harris L, et al. J Clin Oncol. 2007. 3 Goldhirsch A, et al. Ann Oncol. 2013. 4 NICE DiagnosEcs Guidance 2013.
ASCO® Guidelines Node negaKve
NCCN Guidelines® > 0.5 cm, node negaKve, N1mi
St Gallen Consensus Node negaKve, node posiKve
QuanKfies risk of recurrence as a conKnuous variable and predicts responsiveness to both tamoxifen and chemotherapy1
Provides not only prognosKc but also predicKve informaKon regarding the uKlity of cytotoxic therapy in addiKon to
endocrine therapy3
9
NICE Node negaKve
Recommended as an opKon for guidance of chemotherapy decisions in paKents at intermediate risk* of distant recurrence4
ASCO is a trademark of the American Society of Clinical Oncology. NCCN and NCCN Guidelines are trademarks of the NaEonal Comprehensive Cancer Network. The guidelines do not endorse products or therapies. *Intermediate risk of distant recurrence is defined as Nomngham PrognosEc Index score above 3.4 or being at intermediate risk by other decision making tools or protocols
Predicts the risk of recurrence and may be used to idenKfy paKents likely to benefit from tamoxifen or chemotherapy2

Oncotype DXTM assay in rouKne pracKce
• FFPE samples • Fill the form • Send a block or blank slides • Results within 8 working days by email

In France….
• No reimbursement so far! – Impact study – Medico-‐economic study – Regional iniEaEves – Results from my insEtuEon

IMPACT STUDY

ProspecKve Study of the Impact of using the 21-‐Gene Recurrence Score Assay on Clinical Decision Making in Women with Estrogen Receptor-‐posiKve, HER2-‐negaKve, Early
Stage Breast Cancer in France
Gligorov J, Pivot XB, Naman HL, Jacot W, Spaeth D, Misset JL, Largillier R, SauEere JL, de Roquancourt A, Pomel C, Rouanet P,
Rouzier R, Penault-‐Llorca FM for the Francilian Breast Intergroup
13

Overall Impact of the Oncotype DX Assay on Treatment RecommendaEons
(n=96)
60% 40%
Treatment recommendation prior to
Oncotype DX assay Recommendation after
Oncotype DX assay Recommendation after
Oncotype DX assay
Chemotherapy
No Chemotherapy
n = 30 n = 20 n = 15
89% 11%
n=41 n=5
14
36% of paKents (95% CI: 27%-‐47%) had a change in treatment recommendaKon; 5 (5%) added chemotherapy and 30 (31%) removed chemotherapy.
The proporKon of paKents recommended chemotherapy decreased from 52% pre-‐Oncotype DX assay to 26% post-‐Oncotype DX assay (p<0.001 for McNemar’s test).

Metaanalysis of 9 clinical uElity studies (7 retrospecEve, 2 prospecEve) with total n=1154 ER+, N0 EBC paEents
42%58%
Chemo + hormonal therapy
Hormonal therapy only
Overall, the RS led to a 36% change in treatment decisions • 30% from CT+HTà HT • 6% from HT à CT+HT
Hornberger J, et al. St. Gallen 2011. #P201.
6% change
RecommendaKon aoer RS in paKents with
iniKal HT recommendaKon
Treatment plan before the Oncotype DX breast cancer assay
30% change
RecommendaKon aoer RS in paKents with
iniKal CHT recommendaKon

Conclusions: • These are the first prospecEve data regarding the impact of using the Oncotype DX assay in France.
• The adjuvant treatment recommendaEon changed in 36% of the paEents arer receiving the Recurrence Score result, predominantly from chemoendocrine to endocrine treatment alone.
• The proporEon of paEents recommended chemotherapy decreased from 52% to 26% post-‐Oncotype DX assay (p<0.001). – There was a large proporEon of paEents with lobular and grade II tumors and a higher rate of low and intermediate risk paEents compared to previously reported clinical datasets.
16

Conclusions
• There was a significant improvement in physician confidence arer receiving the Recurrence Score result (signed rank test p<0.001).
• Physicians agreed or strongly agreed that the Oncotype DX assay results provided addiEonal informaEon in 79% of paEents (95% CI: 69%-‐87%) .
• The results from the study are consistent with data from studies in other countries.

Impact of the Oncotype DX® Breast Cancer Assay in N0, ER+ EBC
ProspecEve Decision Impact Studies from Various Countries
#1-‐3 posiEve lymph nodes, HT only endocrine therapy, CHT chemoendocrine therapy 1Lo S, et al. J Clin Oncol. 2010. 2Albanell et al. Ann Oncol 2011, 3Eiermann et al. Ann Oncol 2012 in press, 4Yamauchi et al. ESMO 2011,
5De Boer et al. SABCS 2011, 6Davidson JA et al. ASCO 2012, 7Holt S et al., St. Gallen 2011, #P196, 8Gligorov J et al. ASCO 2012
Study N Change rate from pre-‐ to post-‐Oncotype DX® breast
cancer assay
CHT to HT
HT to CHT
US Study1 (N0) 89 31.5% 22.5% 3.4%
Spanish Study2 (N0) 107 31.8% 20.6% 11.2%
German Study3 (N0) 244 30.3% 18.4% 11.5%
Japanese Study4 (N0) 73 30.1% 27.4% 2.7%
Australian Study5 (N0) 101 22.8% 11.9% 10.9%
Canadian Study6 (N0) 150 30% 20% 10%
UK Study7 (N0, N1itc, N1mic) 142 26.8% 18.3% 8.5%
French Study8 (N0, N1mic) 96 36% 31% 5%

Impact of the Oncotype DX® Breast Cancer Assay Decision Impact Studies from Various Countries (N0 and N+)
#1-‐3 posiEve lymph nodes, HT only endocrine therapy, CHT chemoendocrine therapy 1Lo S, et al. J Clin Oncol. 2010. 2Albanell et al. Ann Oncol 2011, 3Eiermann et al. Ann Oncol 2012 in press, 4Yamauchi et al. ESMO 2011,
5De Boer et al. SABCS 2011, 6Davidson JA et al. ASCO 2012, 7Holt S et al., St. Gallen 2011, #P196, 8Gligorov J et al. ASCO 2012
Study N Change rate from pre-‐ to post-‐Oncotype DX® breast
cancer assay
CHT to HT
HT to CHT
US Study1 (N0) 89 31.5% 22.5% 3.4%
Spanish Study2 (N0) 107 31.8% 20.6% 11.2%
German Study3 (N0) 244 30.3% 18.4% 11.5%
Japanese Study4 (N0) 73 30.1% 27.4% 2.7%
Australian Study5 (N0) 101 22.8% 11.9% 10.9%
Canadian Study6 (N0) 150 30% 20% 10%
UK Study7 (N0, N1itc, N1mic) 142 26.8% 18.3% 8.5%
French Study8 (N0, N1mic) 96 36% 31% 5%
German Study3 (N+#) 122 38.5% 27.9% 9.0%
Japanese Study4 (N+#) 17 70.6% 70.6% 0%
Australian Study5 (N+#) 50 26% 24% 2%

COST STUDY

Cost of adjuvant chemotherapy in France
• RetrospecEve study conducted in Tenon hospital
• Average cost of chemotherapy per paEent: – To the society: €14,835 – To the social security (NHS): €13,474

Cost study in France
• Average cost of chemotherapy per paEent: ▫ To the society: €14,835 ▫ To the social security (NHS): €13,474 • Chemotherapy drugs represent 40-‐43% of the total cost • Very conservaEve esEmate of the cost of chemotherapy as the costs following the full chemotherapy regimen are not taken into account: ▫ Follow-‐up visits ▫ Long term adverse events ▫ Absenteeism arer chemotherapy regimen

Cost-‐effecEveness results in case of use of OncotypeDX®
Per paKent tested Usual care Oncotype DX® Difference
Discounted cost €11,804 €11,174 € 629
Discounted Life Years
13.21 13.33 0.13
Incremental Cost-‐effecEveness RaEo
-‐ -‐ Cost-‐savings
• Expected increased Life years when treatment decisions are informed by Oncotype DX® (paEents reclassified towards chemotherapy arer recurrence score)
• Decreased overall cost when treatment decisions are informed by Oncotype DX® (decreased chemotherapy costs for paEents who are spared un-‐necessary chemotherapy)
à Using Oncotype DX® in the French setng is expected to be cost-‐savings

Consistent cost-‐effecEveness results regardless of country and local cost data
PublicaKon Reported Findings (ICER in Cost per QALY gained with Oncotype DX)
Country Threshold (Willingness to pay for 1 QALY($))
Country Comment
Lacey L et al. 2011 EUR 9,462 EUR 20,000 Ireland Cost EffecKve
Holt et al. 2011 GBP 6,232 GBP 20,000 UK Cost EffecKve
Klang et al. 2010 USD 10,700 USD 35,000 Israel Cost EffecKve
Tsoi et al. 2010 USD 63,421 USD 75,000 Canada Cost EffecKve
Paulden et al. 2011 > USD 29,000 USD 75,000 Canada Cost EffecKve
Kondo et al. 2010 USD 3,848 USD 50,000 Japan Cost EffecKve
Madaras et al. 2011 USD 14,110 USD 20,000 Hungary Cost EffecKve
O’Leary et al. 2010 AUS 9,986 AUS 18,000 Australia Cost EffecKve
de Lima Lopez et al. 2011 Improved outcomes (QALYs), reduced costs
Singapore Cost Savings
Chereau et al, SABC 2011 France Cost Savings
Hornberger et al. 2005 USA Cost Savings
Lyman et al. 2007 USA Cost Savings

Regional iniEaEves

Experience from X Pivot’s team Study flow chart
Cas$de$pa(entes$$discutés$en$RCP$de$valida(on$de$tests$biologiques$pour$la$
réalisa(on$de$Oncotype$DX®$N$=$62$
Cas$analysés$N$=$51$(82%)$
Cas$sélec(onnés$pour$la$réalisa(on$de$Oncotype$DX®$N$=$52$(84%)$
Résultats$N$=$48$(77%)$
10$cas$non$retenus$(16%)$
1$cas$$non$analysable$(2%)$$
3$cas$avec$décision$thérapeu(que$non$guidée$par$
Oncotype$DX®$(5%)$
Cas$de$pa(entes$$discutés$en$RCP$de$sénologie«$cancer$du$sein$localisés$»$$
N=$1592$1530$cas$non$retenus$pour$la$réalisa(on$de$Oncotype$DX®$
(96%)$
Figure$1$:$Flow%Chart%pour$la$réalisa(on$de$Oncotype$DX®$
Nerich et al, Bull du Cancer 2014

Recurrence Score Figure'2':'Répar..on'du'Recurrence'Score'(RS)'par'pa.entes'
0'
5'
10'
15'
20'
25'
30'
35'
40'
45'
50'
55'
60'
65'
0' 1' 2' 3' 4' 5' 6' 7' 8' 9' 10'11'12'13'14'15'16'17'18'19'20'21'22'23'24'25'26'27'28'29'30'31'32'33'34'35'36'37'38'39'40'41'42'43'44'45'46'47'48'
Pa.entes'
Valeu
r'du
'Recurrence'Score'
RS'faible'
'RS'interE'
Eméd
iaire'
RS'élevé'
Nerich et al, Bull du Cancer 2014

Cost effecKveness Cost (€) by expenditure «Oncotype DX®»
Strategy
«Standard»
Strategy
DifferenKal
Chemotherapy 20 559 75 911 -‐55 352
implantable chamber 13 928 51 425 -‐37 497
Biology tests 1 039 3 836 -‐2 797
PegfilgrasKm (drug + injecKon) 1 936 7 147 -‐5 211
Hairpiece 1 625 6 000 -‐4 375
Transport 4 527 16 716 -‐12 189
Oncotype DX® Test 111 300 / +111 300
Total coost for 48 paKentes 154 914 161 035 -‐6 121
By paKent 3 227 3 355 -‐128
Nerich et al, Bull du Cancer 2014

EXPERIENCE FROM MY INSTITUTION

Centre Jean Perrin’s cases
• From 2011 to 2014 • 57 pts – Median size : 1,9 (0,4 to 4 cm) – 51 SBR grade II, 6 grade I, no grade III – All ER Allred 8 or 9, 11 PR negaEve or low – 30 High Ki67, 12 with vascular embolies – 21 N+
• Recurrence score : 39 Low RS, 13 Intermediate RS, 3 High RS, 2 NI
• 9 paKents received CT

Conclusions
• Results of decision impact studies are very consistent across different countries - ~30% change in treatment recommendaKons aoer Oncotype DX® for node
negaKve paKents, and clinically relevant also in node-‐posiKve disease
- Treatment recommendaKons followed the Recurrence Score result
- Intermediate Recurrence Score also provides clinically relevant informaKon
- Use of the Recurrence Score result led to a clinically significant reducKon in chemotherapy use
• Cost effecKveness is demonstarted in different models • TesKng with Oncotype DX® increased confidence of physicians in adjuvant
therapy decision-‐making (N0 and N+)