Embed Size (px)
Citation preview

RESEARCH POSTER PRESENTATION DESIGN © 2012
www.PosterPresentations.com
Glomerular "full-house" immunofluorescence staining commonly indicates lupus nephritis, in which there is immune complex deposition in the sub endothelium and sub epithelium and means quite simply that all five major immunofluorescent stains on a renal biopsy (IgM, IgG, IgA, C3, and C1q) are all positive. The analogy holds true in that the "full house" in cards (3 of a kind plus a pair, to the left) is similar to the 3 types of immunoglobulins plus 2 types of complement which show positive staining. . We hereby report a case of pregnant female with class III + V lupus nephritis.
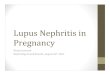
INTRODUCTIONA 23 year old African American female G2P1L1, with no significant past medical history presented at 7 weeks gestation for increasing swelling of face and lower extremities for two weeks. Also noticed foamy appearance to her urine and hematuria. No family history of renal disease. On physical exam had normal vital signs, periorbital and 2+ bilateral pitting pedal edema noted. On labs had creatinine of 0.88, total protein 4.7gm/dl, albumin of 1.7 , LDL of 268, 6-10 RBC in urine microscopic analysis, Fe Na 1.2%, 24 hour urine protein 1.658 gm/24hrs, ANA negative, complement level – normal. Ultrasound guided renal biopsy showed focal segmental endocapillary and extra capillary proliferative and membranous glomerulonephritis suggestive of lupus nephritis(ISN-RPS class III +V). Immunofluorescence showed full house granular glomerular capillary wall staining and mesangial staining for IgG,IgM,IgA,C3 and C1. Patient opted for an elective D and C. Subsequently treated with steroids and cytoxan.
CASE PRESENTATION DISCUSSION
The outlook of pregnancy for women with lupus nephritis is usually favorable if the disease (both renal and nonrenal) has been quiescent for at least 6 months before pregnancy, and if, at conception, serum creatinine is less than 140 micromol/l, proteinuria less than 3 g/24 h and blood pressure controlled. The risk of fetal loss is, however, at least 2-3 times higher than in the normal population. Management needs to be by a multidisciplinary team involving physicians and obstetricians, ideally beginning with pre-pregnancy counselling.It involves awareness of, and allowance for, physiological changes including decreased serum creatinine and increased proteinuria. Treatment of flares includes corticosteroids, hydroxychloroquine, azothioprine, Blood pressure is controlled with methyldopa, nifedipine or hydralazine. Full-house” glomerulopathy in may be the first symptom of SLE, The appearance of other clinical and biological symptoms may be delayed by several years
Trinitas Regional Medical Center
Vidya Kollu, MD Priyasha Srivastav,MD , Ria D’Souza, MD
‘Full house’ lupus nephritis in a pregnant female.