Embed Size (px)
Citation preview

Future Developments in
Radiation Therapy for Prostate
Cancer
Steven J. Frank, MD
Assistant Professor
Genitourinary and Head/Neck Sections
Division of Radiation Oncology

Rectal Fistula
Sinus tract vs fistula

Rectal Necrotic Tissue
Biopsies showed
necrotic tissue

Dose-escalation is not free
• Rectal toxicity
• Urinary
• Erectile

Therapeutic ratio
Tumor control
Normal tissue complication
Total Radiation DOSE
Probability
of
EFFECT

Where are we going in
Prostate Radiation Therapy?
EBRT
• 2D
• 3D
• IMRT
• Hypofractionation
• SBRT
• Protons
• IMPT
Brachytherapy
• 1st Generation Implants
• 2nd Generation Implants
• 3rd Generation Implants
• 4th Generation Implants
• 5th Generation Implants

Where have we come from?

PSA control after conventional
dose RT (~70Gy)
IJROBP 2001;49

Higher RT doses improve
disease control
• Multiple retrospective studies show benefit to
higher doses of RT.
– MDACC (Pollack & Zagars. IJROBP 39, 1997)
– Fox Chase (Hanks et al. IJROBP 41, 1998)
– MSKCC (Zelefsky et al. IJROBP 41, 1998)
– MSKCC (Zelefsky et al. J Urol 166, 2001)
– Cleveland Clinic (Lyons et al. Urol 55, 2000)

More Grade 2 rectal complications in 78 Gy arm
[IJROBP 53, 2002]

More Grade 2+ rectal toxicity
if >25% of rectum received 70Gy

Dose-escalation w/ less
toxicity• Delivery techniques
– IMRT
– Protons
• Reduce PTV– Target localization (e.g. BAT, fiducial markers)
– Target immobilization (e.g. rectal balloon)
– Reduce CTV
• Selective dose-escalation– Intra-prostatic targets and avoidance structures

Axial Dose Distribution
75.6 Gy
60 Gy79 Gy

Sagittal Dose Distribution

Prostate:
>100%[email protected]
SV:
Rectum:
<20%V@70Gy
<35%V@60Gy
Bladder:
<25%V@70Gy
<35%V@60Gy
Femoral Heads:
<5%V@50Gy
DVH

MSKCC
Rectal toxicity (3D CRT vs. IMRT)
3DCRT
IMRT

MSKCCGU toxicity based on dose 81 vs. 86 Gy
“Among patients who received doses 75.6 Gy, the incidence
of Grade 2 urinary symptoms at 5 years was 13% compared 8%
at lower doses.” [IJROBP 53, 2002]

Dose-escalation w/ less
toxicity• Delivery techniques
– IMRT
– Protons
• Reduce PTV
– Target localization (e.g. BAT, fiducials)
– Target immobilization (e.g. rectal balloon, tracking)
– Reduce CTV
• Selective dose-escalation

21

Accelerator Systems
Linac Injector
Synchrotron

13 m diameter190 tons SAD 2.7 m

Nozzle
Snout
Couch
Image
Receptors
X-ray
tube
Articulating Floor

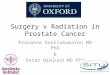
A Single Bragg Peak

Modulation of the Bragg Peak
The Bragg peak is spread out by introducing extra absorbing material before the beam enters the patient. If different thickness of such absorber are present for different fractions of the irradiation time, the narrow monoenergetic peak can be spread into a useful plateau
The Bragg peak can be spread out
to a useful plateau by the use of a
rotating stepped absorber.
Range
Modulator
Wheel

SOBP, Photons, & Bragg Peak
PSI

Aperture 2D Shaping
Lateral aspect of aperture used
to spare critical structures

Compensator 3D Distal
Shaping
As well as spreading out
the Bragg peak, the final
range itself must be
shaped to the distal
surface of the target
volume taking into account
heterogeneities

Two lateral beams.
Further improvements w/ IMPT?
Decreased integral dose.
Better dose homogeneity.
Quicker planning time.

Dose-escalation w/ less toxicity
• Delivery techniques
– IMRT
– Protons
• Reduce PTV
– Target localization (e.g. BAT, fiducials)
– Target immobilzation (e.g. rectal balloon)
• Selective dose-escalation

Sharp dose-fall off with IMRT requires
accurate DAILY target localization

25 treatment CTs
Acquired during a course
of 42 fxs treatment
Dancing Prostate
Dong (MDA), 2002

IGRT is a Process
VARIAN

Reducing PTV a.k.a.
IGRT (Image Guided Radation Therapy)
• Improve accuracy and decrease normal
tissue irradiated
• Requires daily imaging of the target
• INTER-fractional movement
• INTRA-fractional movement

IGRT
• Portal imaging
• Ultrasound (e.g. B.A.T.)
• Fiducial markers (intraprostatic)
• Volumetric on-board imaging
– In-room CT
– Cone-beam CT

BAT alignment (axial)
Bladder
Prostate
Rectum

BAT Alignment (sagittal)
Bladder
Prostate
Rectum

Ultrasound-based alignment
• Pros– Non-invasive
– Reasonably good alignment
– Visualize SV/ bladder/rectum
– Visualize prostate surface contour
– Follow-up
– New volumetric systems
• Cons
– User-subjectivity
– Patient anatomy may
affect image quality
– Impact of probe
pressure on prostate
position
– Different imaging
modality



On-Board Imager (OBI) - Varian
kV X-ray Source
aSi Imaging Panel
(2048 x 1536 pixel resol.)
Robotic Arms
- 3 pivot points
- Completely retractable
- Position feedback control
Software
- Image acquisition and registration

OBI 2D-2D manual match: pre-shift

OBI 2D-2D manual match: postshift

Fiducial-based alignment
• Pros– Less subjectivity
– Good alignment
– Allows target tracking
• Kitamura and Shirato et al.
– Better for large patients
– Basis for improved multimodality image fusion (e.g. MRI-CT)
– Ongoing MDACC study comparing fiducials vs. CT-on-rails
• Cons– Invasive
– Requires daily ports
• (unless KV imaging onboard)
– No image of SV, rectum/bladder
– No image of prostate surface contour
– Shifts may not be representative of volume
• Jaffray et al. ASTRO 2004
• Fiducials and MRI
• 47% had 3mm deformation over 90% of surface
• On average, 14% of surface deformed by >3mm (up to 9mm)

Varian ExaCT™ at MDACC
In-room CT Linac

CAT Software (3D-3D matching)
Compares Pinnacle planed patients
to volumetric images
Lei Dong, Lifei (Joy) Zhang

A closer look at contour overlay
Courtesy of Lei Dong

Step 4. Automatic Image Registration
Courtesy of Lei Dong

Step 5. Review Image Registration
(prostate is the target of alignment)
Courtesy of Lei Dong

• CT-based alignment could yield
accuracy of <3mm
– Smaller treatment margins
– Less dose to rectum, bladder
– Avoid high-dose to intra-prostatic
structures (e.g. urethra)

Robotic arm motion

Robotic arm motion

Robotic arm motion

Cone-beam CT
• Uses on board kV X-ray source and
amorphous silicon flat panel imager
• Large field of view (25 x 25 x 10 cm) and
single revolution captures images
– Unlike standard CT that uses small field of view
and many revolutions
• Inferior image quality compared to
conventional CT but may be adequate for RT
targeting

Cone Beam CT – Large GU patient
(330 lbs)
CBCT Planning CT

Post shift CBCT verification
using in-house CAT software

Cone Beam CT vs. CT on Rails
< 5 min acquisition and
reconstruction time
Patient is rotated into scanning
position on treatment couch (lateral
and vertical shifts required)
Isocenter not linked to images
Each slice is a 1 sec time average
50 cm FOV (full scan)
< 5 min acquisition and
reconstruction time
Patient is imaged in treatment
position (except for lateral shifts)
Isocenter defined in CT space
Each slice is a 60 sec time average
45 cm FOV half-scan

Dose-escalation w/ less toxicity
• Delivery techniques
– IMRT
– Protons
• Reduce PTV
– Target localization (e.g. BAT, fiducials)
– Target immobilzation (e.g. rectal balloon)
• Selective dose-escalation
– Intraprostatic GTV/OAR

Endo-rectal balloon
1. Immobilize prostate (accounts for inter-
and intrafractional motion)
2. Displaces rectum away from high dose

Shifts Detected By CT and BAT
-2.0
-1.5
-1.0
-0.5
0.0
0.5
1.0
1.5
2.0
-2.0 -1.5 -1.0 -0.5 0.0 0.5 1.0 1.5 2.0
CT Shift (cm)
BA
T S
hif
t (c
m)
RL
AP
SI No call
by BAT
Planning CT Sagittal
Same Day Sagittal CT
Same Day Axial CT
BAT Oblique Axial Sagittal
One Patient
Example
Sup.
Sup.

Is intra-fractional prostate motion a
concern?
• Daily IMRT treatment 15 minutes to setup and deliver
• Possible prostate positional change during this interval largely due to transient rectal gas
• Positional change can be large (>5 mm), but usually transient
• Clinical impact over 7-8 week treatment course is unknown

Dose-escalation w/ less toxicity
• Delivery techniques
– IMRT
– Protons
• Reduce PTV
– Target localization (e.g. BAT, fiducials)
– Target immobilzation (e.g. rectal balloon)
• Selective dose-escalation
– Intraprostatic GTV/OAR

What is needed to treat intra-
prostatic targets?
• Imaging modality beyond CT that can delineate intra-prostatic tumor– Endorectal MRI/MRS
– Dynamic contrast MRI
• Conformal delivery method– IMRT, protons, brachytherapy
• Accurate delivery– Daily imaging w/ online correction
– Target immobilization?
– Transrectal U/S guidance

Endorectal MRI
• Endorectal MRI uses a coil inside an inflatable latex balloon (50-70cc).– Coil just posterior to
prostate
• Resolution is 0.4mm per pixel pair– Body coil MRI has
resolution of 3 mm
• Accuracy is technique and reader dependent as per RDOG studies
– [Radiology 1994;192:47-54]
[Roach et al. Oncology 15:1399-1410]



Special thanks to Danny Tran & Lei Dong
75.6Gy
87.2Gy
Concomitant
boost

CT/ MRI/MRS fusion
• Define CTV more clearly
– Prostate anatomy
– Reduced side effects
• Define other CTV’s (e.g. peripheral zone, urethra)
– Selective dose-escalation (“Dose painting”)
– Reduce toxicity w/ in the prostate
• Define GTV
– Selective dose-escalation (Focal boost)

Hypofractionation
• Provide basis for larger fractional dose w/
equal or less toxicity
– / for prostate ca may be < 4 Gy» [Brenner et al. IJROBP 52:6-13]
• Hypofractionation studies:
– Kupelian et al 70 Gy (2.5Gy/Fxn) [IJROBP 53, 2002]
– MDACC ongoing randomized study
• 75.6/1.8 Gy vs. 72/2.4 Gy (BED = 78-82 Gy)

72 Gy (2.4Gy)

Cleveland Clinic-retrospective70Gy/2.5Gy vs. 78Gy/2Gy
Grade 2-3 rectal toxicity
Kupelian et al. IJROPB 53, 2002
166 (SCIMRT)
116 (3DCRT)
Median FU 21 vs. 32 mo
Only 2 pts in each group
had Gr 2+ GU toxicity.

Highest Degree of Conformal
Therapy?
Brachytherapy

1st Generation Implants:
Open Placement

Transperineal Interstitial Permanent
Prostate Brachytherapy
Ultrasound probe in
rectum for needle guidance
Perineal template to
localize needles as planned
18 gauge needle
(1.3 mm diam) for
seed placement

2nd Generation Implants:
Uniform Loading

Source Migration
Davis BJ et al., J Urol 2002; 168:1103.
*
*Coronary
artery

3rd Generation Implants
• Modified peripheral loading
– Reduced urethral dose (not urethral sparing)
– All seeds implanted in the prostate
(which means little treatment outside capsule
or high urethral dose with margin)
– CT-based dosimetry evaluation

Modified Peripheral Loading

4th Generation Implants
• Stranded seeds (Varistrand )
– Less seed migration
– Permits periprostatic seed placement
• Improved dosimetry
– Wider therapeutic margin on prostate (3 - 5
mm)
– MRI / CT fusion (better QA better implants)
– Improved Homogeneity

Intraoperative Comparison of Actual Seed Location to Preplan

PTV DVH Parameters
V100>95%
V150<60%
V200<20%D90<120%
R100<1cc

5 yr BRFS Monotherapy
• Seed monotherapy 5 yr BRFS if implant
quality questionable or poor = 34-63%
• Seed monotherapy 5 yr BRFS if implant
quality is good = 82-98%
• % positive Bx cores predicts RP BRFS
• RTOG-0232 randomized study I125/Pd103 +/-
EBRT intermediate risk patients

Transperineal Interstitial
Permanent Brachytherapy
Alone for Selected Patients
with Intermediate Risk
Prostate Cancer
Phase II Prospective Single Arm Study
David Swanson and Steven J. Frank

Stratification
• < 35% core biopsy and Gleason 7 disease
with a PSA under 10
• < 35% core biopsy and combined Gleason
scores less than 7 with a PSA 10-15
• >/= 35% core biopsy and Gleason 7 disease
with a PSA under 10
• >/= 35% core biopsy and combined Gleason
scores less than 7 with a PSA 10-15

MRI vs. CT
July 2008
Front view Front view
Notice the artifacts on CT imaging
Prostate Phantom Prostate Phantom

1.5T MRI Strand
Prostate Phantom
C4
Seed
Prostate Phantom
Oblique view Saggittal view


GU Team
• Physicians
– Seungtaek Choi
– Min Rex Cheung
– Deborah A. Kuban
– Andrew K. Lee
– Jim D. Cox
– Tom A. Buchholz
• Physicists
– Lei Dong
– Rajat Kudchadker
– Jennifer Johnson
• Dosimetrists
– Paula Berner
– Teresa Bruno
– Mandy Cunningham
• Therapists
• Nurses

![Recent developments in prostate cancer biomarker Austin ... · ness of prostate cancer and potential new treatments [15]. Molecular genetic approaches examining tumour gene expression](https://img.pdfslide.net/doc/110x75/604fc3385c266f307b2b650a/recent-developments-in-prostate-cancer-biomarker-austin-ness-of-prostate-cancer.jpg)