Embed Size (px)
Citation preview


Gastrointestinal SystemGastrointestinal System
Anatomy and Anatomy and PhysiologyPhysiology


The MouthThe Mouth Important for the Important for the
mechanical mechanical digestion of food digestion of food
The saliva The saliva contains SALIVARY contains SALIVARY AMYLASE or AMYLASE or PTYALIN that PTYALIN that starts the INITIAL starts the INITIAL digestion of digestion of carbohydrates carbohydrates

The Esophagus The Esophagus A hollow collapsible tube A hollow collapsible tube Length- 10 inches Length- 10 inches The upper third contains The upper third contains
skeletal muscles skeletal muscles The middle third The middle third
contains mixed skeletal contains mixed skeletal and smooth muscles and smooth muscles
The lower third contains The lower third contains smooth muscles and the smooth muscles and the esophago-gastric/ esophago-gastric/ cardiac sphincter is cardiac sphincter is found here found here
Functions to carry or Functions to carry or propel foods from the propel foods from the oropharynx to the oropharynx to the stomach stomach

The stomachThe stomach J-shaped organ in the J-shaped organ in the
epigastrium epigastrium Contains four parts- Contains four parts-
the fundus, the cardia, the fundus, the cardia, the body and the the body and the pylorus pylorus
The esophageal The esophageal sphincter prevents the sphincter prevents the reflux of the contents reflux of the contents into the esophagus into the esophagus
The pyloric sphincter The pyloric sphincter regulates the rate of regulates the rate of gastric emptying into gastric emptying into the duodenum the duodenum
Capacity is 1,500 ml! Capacity is 1,500 ml!

The functions of The functions of the stomach the stomach are generally to are generally to digest the food digest the food and to propel and to propel the digested the digested materials into materials into the SI for final the SI for final digestion digestion

The Glands and cells in The Glands and cells in the stomach secrete the stomach secrete digestive enzymes: digestive enzymes:
1. 1. Parietal cells-Parietal cells- HCl HCl acid and Intrinsic factor acid and Intrinsic factor
2. 2. Chief cells-Chief cells- pepsin pepsin digestion of PROTEINS! digestion of PROTEINS!
3. 3. Antral G-cells-Antral G-cells- gastrin gastrin
4. 4. Argentaffin cells-Argentaffin cells- serotonin serotonin
5. Mucous neck cells- 5. Mucous neck cells- mucus mucus

The Small The Small intestineintestine
Grossly divided into Grossly divided into the Duodenum, the Duodenum, Jejunum and Ileum Jejunum and Ileum
The duodenum The duodenum contains the two contains the two openings for the openings for the bile and pancreatic bile and pancreatic ducts ducts
The ileum is the The ileum is the longest part (about longest part (about 12 feet) 12 feet)

The intestinal glands The intestinal glands secrete digestive secrete digestive enzymes that finalize enzymes that finalize the digestion of all the digestion of all foodstufffoodstuff
Enzymes for Enzymes for carbohydrates carbohydrates - disaccharidases - disaccharidases
Enzymes for proteins Enzymes for proteins -dipeptidases and -dipeptidases and aminopeptidases aminopeptidases
Enzyme for lipidsEnzyme for lipids- intestinal lipase - intestinal lipase

The Large The Large intestineintestine
Approximately 5 feet long, Approximately 5 feet long, with parts: with parts:
1. The cecum - widest 1. The cecum - widest diameter, prone to diameter, prone to rupture rupture
2. The appendix 2. The appendix 3. The ascending colon 3. The ascending colon 4. The transverse colon 4. The transverse colon 5. The descending colon 5. The descending colon 6. The sigmoid - most 6. The sigmoid - most
mobile, prone to mobile, prone to twisting twisting
7. The rectum 7. The rectum

Absorbs water Absorbs water Eliminates wastes Eliminates wastes Bacteria in the Bacteria in the
colon synthesize colon synthesize Vitamin K Vitamin K
Appendix Appendix participates in the participates in the immune system immune system

Accessory Accessory OrgansOrgans

The LiverThe Liver The largest The largest
internal organ internal organ Located in the Located in the
right upper right upper quadrant quadrant
Contains two Contains two lobes- the right lobes- the right and the left and the left

The hepatic The hepatic ducts (right ducts (right and left) join and left) join together with together with the cystic the cystic duct to duct to become the become the common bile common bile duct duct

Functions to store Functions to store excess glucose, fats excess glucose, fats and amino acids and amino acids
Also stores the fat Also stores the fat soluble vitamins- A, soluble vitamins- A, D and the water D and the water soluble- Vitamin B12 soluble- Vitamin B12
Produces the BILE for Produces the BILE for normal fat digestion normal fat digestion
The Von Kupffer cells The Von Kupffer cells remove bacteria in remove bacteria in the portal blood the portal blood
Detoxifies ammonia Detoxifies ammonia into urea into urea

The gallbladder The gallbladder Located below the Located below the
liver liver The cystic duct joins The cystic duct joins
the hepatic duct to the hepatic duct to become the bile duct become the bile duct
The common bile duct The common bile duct joins the pancreatic joins the pancreatic duct in the sphincter duct in the sphincter of Oddi in the first of Oddi in the first part of the duodenum part of the duodenum

Stores and Stores and concentrates bile concentrates bile
Contracts during Contracts during the digestion of fats the digestion of fats to deliver the bile to deliver the bile
Cholecystokinin is Cholecystokinin is released by the released by the duodenal cells, duodenal cells, causing the causing the contraction of the contraction of the gallbladder and gallbladder and relaxation of the relaxation of the sphincter of Oddi sphincter of Oddi

The pancreasThe pancreas A retroperitoneal A retroperitoneal
gland gland Functions as an Functions as an
endocrine and endocrine and exocrine gland exocrine gland
The pancreatic duct The pancreatic duct (major) joins the (major) joins the common bile duct in common bile duct in the sphincter of Oddi the sphincter of Oddi

The exocrine function of the pancreas is the The exocrine function of the pancreas is the secretion of digestive enzymes for secretion of digestive enzymes for carbohydrates, fats and proteins carbohydrates, fats and proteins
Pancreatic amylase - carbohydrates Pancreatic amylase - carbohydrates Pancreatic lipase (steapsin) - fats Pancreatic lipase (steapsin) - fats Trypsin, Chymotrypsin and Peptidases - Trypsin, Chymotrypsin and Peptidases -
proteins proteins Bicarbonate - to neutralize the acidic Bicarbonate - to neutralize the acidic
chyme. chyme.

DiagnosticsDiagnostics

Guaiac TestGuaiac Test - detects the presence of - detects the presence of
fecal occult blood. . Positive guaiac test shown on right, as Positive guaiac test shown on right, as
would be seen for this patient. Negative would be seen for this patient. Negative result (on left) included for comparison.result (on left) included for comparison.

Fecal Occult Blood Testing-FOBT Fecal Occult Blood Testing-FOBT (Guaiac Test)(Guaiac Test)
Instruct the patient to adhere to a 3-day Instruct the patient to adhere to a 3-day meatless diet (avoid any blood-containing meatless diet (avoid any blood-containing food, cantaloupe, uncooked broccoli, turnip, food, cantaloupe, uncooked broccoli, turnip, radish, or horseradish)radish, or horseradish)
No intake of NSAIDS, aspirin and anti-No intake of NSAIDS, aspirin and anti-coagulant coagulant
Avoid Avoid citrus fruits and and vitamin C supplements supplements Screening test for colonic cancer Screening test for colonic cancer

Barium Barium swallowswallow::
A series of x-rays of A series of x-rays of the esophagus the esophagus and stomach. The and stomach. The patient drinks a patient drinks a liquid that liquid that contains barium contains barium (a silver-white (a silver-white metallic metallic compound). The compound). The liquid coats the liquid coats the esophagus and x-esophagus and x-rays are taken. rays are taken. This procedure is This procedure is also called an also called an upper GI series upper GI series

Upper GIT study: Upper GIT study: barium swallow barium swallow
Pre-test : NPO post-Pre-test : NPO post-midnight; 6-8 hours midnight; 6-8 hours before procedure before procedure
Post-test : Laxative Post-test : Laxative is ordered, increase is ordered, increase pt fluid intake, pt fluid intake, instruct that stools instruct that stools will turn white, will turn white, monitor for monitor for obstruction obstruction

Barium Barium enemaenema procedure. The procedure. The patient lies on patient lies on an x-ray table. an x-ray table. Barium liquid is Barium liquid is put into the put into the rectum and rectum and flows through flows through the colon. X-the colon. X-rays are taken rays are taken to look for to look for abnormal areas. abnormal areas.

Lower GIT study: barium Lower GIT study: barium enema enema
Examines the lower GI Examines the lower GI tract tract
Pre-test : Clear liquid Pre-test : Clear liquid diet and laxatives, NPO diet and laxatives, NPO post-midnight, post-midnight, cleansing enema prior cleansing enema prior to the test to the test
Lower GIT study: barium Lower GIT study: barium enema enema
Post-test: Laxative is Post-test: Laxative is ordered, increase ordered, increase patient fluid intake, patient fluid intake, instruct that stools will instruct that stools will turn white, monitor for turn white, monitor for obstruction obstruction


EGD EGD
(esophagogast(esophagogastroduodenoscoroduodenoscopy) py)
Visualization of the Visualization of the upper GIT by upper GIT by endoscope endoscope

Pre-test : ensure consent, NPO 8 hours, Pre-test : ensure consent, NPO 8 hours, pre-medications like atropine and pre-medications like atropine and anxiolytics anxiolytics
Intra-test: position : LEFT lateral to Intra-test: position : LEFT lateral to facilitate salivary drainage and easy facilitate salivary drainage and easy access access
Post-test : NPO until gag reflex returns, Post-test : NPO until gag reflex returns, place patient in SIMS position until he place patient in SIMS position until he awakens , monitor for complications, awakens , monitor for complications, saline gargles for mild oral discomfortsaline gargles for mild oral discomfort

ULTRASONOGRAPHYULTRASONOGRAPHY 1. A noninvasive test focuses 1. A noninvasive test focuses high-high-
frequency sound waves over an frequency sound waves over an abdominal organabdominal organ to obtain an image of to obtain an image of the structure.the structure.
2. Ultrasound can detect small abdominal 2. Ultrasound can detect small abdominal masses, fluid-filled cysts, gallstones, masses, fluid-filled cysts, gallstones, dilated bile ducts, ascites, and vascular dilated bile ducts, ascites, and vascular abnormalities.abnormalities.
3. Ultrasound with Doppler may be 3. Ultrasound with Doppler may be ordered for vascular assessment.ordered for vascular assessment.

COMPUTED TOMOGRAPHY (CT) COMPUTED TOMOGRAPHY (CT) SCANSCAN
1. This is an x-ray technique that 1. This is an x-ray technique that provides excellent anatomic definition provides excellent anatomic definition and is used to detect tumors, cysts, and is used to detect tumors, cysts, and abscesses.and abscesses.
2. The CT can also detect dilated bile 2. The CT can also detect dilated bile ducts, pancreatic inflammation, and ducts, pancreatic inflammation, and some gallstones.some gallstones.

ENDOSCOPIC PROCEDURESENDOSCOPIC PROCEDURES Endoscopy is the use of a flexible tube Endoscopy is the use of a flexible tube
(the fiberoptic endoscope) (the fiberoptic endoscope) to visualize to visualize the GI tract and to perform certain the GI tract and to perform certain diagnostic and therapeutic procedures. diagnostic and therapeutic procedures. Images are produced through a video Images are produced through a video screen or telescopic eyepiece. screen or telescopic eyepiece. The tip of The tip of the endoscope moves in four directions, the endoscope moves in four directions, allowing for wide-angle visualization. allowing for wide-angle visualization.

Customizable to meet specific surgical needs, Customizable to meet specific surgical needs, endoscopes can be fitted with scissors, knives, endoscopes can be fitted with scissors, knives,
lasers, or cameras. Here, the endoscope is fitted lasers, or cameras. Here, the endoscope is fitted with a small grasping tool to remove a toy lodged with a small grasping tool to remove a toy lodged
in the esophagus of an infantin the esophagus of an infant

PROCTOSIGMOIDOSCOPY AND PROCTOSIGMOIDOSCOPY AND COLONOSCOPYCOLONOSCOPY
1. Proctosigmoidoscopy (rectosigmoidoscopy) is 1. Proctosigmoidoscopy (rectosigmoidoscopy) is the visualization of the anal canal, rectum, and the visualization of the anal canal, rectum, and sigmoid colon through a fiberoptic sigmoidoscope. sigmoid colon through a fiberoptic sigmoidoscope.
2. Colonoscopy is the visualization of the entire 2. Colonoscopy is the visualization of the entire large intestine, sigmoid colon, rectum, and anal large intestine, sigmoid colon, rectum, and anal canal.canal.
3. Sigmoidoscopy or colonoscopy can be used to 3. Sigmoidoscopy or colonoscopy can be used to diagnose malignancy, polyps, inflammation, or diagnose malignancy, polyps, inflammation, or strictures.strictures.


34 yr old female. She also had an endoscopy 34 yr old female. She also had an endoscopy first. (bleeding and/or pain was the reason first. (bleeding and/or pain was the reason she came in.) That pinkish/white mass is she came in.) That pinkish/white mass is
cancer. It's right by/on the valve between the cancer. It's right by/on the valve between the ileum (small intestine) and cecum (large ileum (small intestine) and cecum (large
intestine.) intestine.)

TREATMENTSTREATMENTSgastrointestinalgastrointestinal
ENEMANASOGASTRIC INTUBATION
TOTAL PARENTERAL NUTRITION

PURPOSES OF ENEMA PURPOSES OF ENEMA ADMINISTRATIONADMINISTRATION
1. Bowel preparation for 1. Bowel preparation for diagnostic tests or diagnostic tests or surgery to empty the surgery to empty the bowel of fecal content.bowel of fecal content.
2. Delivery of medication 2. Delivery of medication into the colon ( such as into the colon ( such as enemas containing enemas containing neomycin to decrease neomycin to decrease the bowel’s bacteria the bowel’s bacteria count or a kayexalate count or a kayexalate enema to decrease the enema to decrease the serum potassium level)serum potassium level)

PURPOSES OF ENEMA PURPOSES OF ENEMA ADMINISTRATIONADMINISTRATION
3. To soften the stool ( oil-retention 3. To soften the stool ( oil-retention enemas)enemas)
4. To relieve gas( tidal,milk and 4. To relieve gas( tidal,milk and molasses,or fleet enemas)molasses,or fleet enemas)
5. Promote defecation and evacuate 5. Promote defecation and evacuate feces from the colon for patients with feces from the colon for patients with constipation or an impactionconstipation or an impaction

PURPOSES OF PURPOSES OF NASOGASTRIC INTUBATIONNASOGASTRIC INTUBATION
Remove fluid and gas from the stomach Remove fluid and gas from the stomach (decompression).(decompression).
Prevent or relieve nausea and vomiting Prevent or relieve nausea and vomiting after surgery or traumatic events by after surgery or traumatic events by decompressing the stomach. decompressing the stomach.
Irrigate the stomach (lavage) for active Irrigate the stomach (lavage) for active bleeding or poisoning.bleeding or poisoning.

PURPOSES OF PURPOSES OF NASOGASTRIC NASOGASTRIC INTUBATIONINTUBATION
Administer medications and feeding Administer medications and feeding (gavage) directly into the GI tract.(gavage) directly into the GI tract.
Obtain a specimen of gastric Obtain a specimen of gastric contents for laboratory studies when contents for laboratory studies when pyloric or intestinal obstruction is pyloric or intestinal obstruction is suspected.suspected.

Nasogastric Nasogastric intubationintubation

Ensuring proper Ensuring proper NG tube NG tube placement:placement:
examine the patient’s examine the patient’s mouth and throat for mouth and throat for signs of a coiled section signs of a coiled section of tubing.of tubing.
watch for respiratory watch for respiratory distress signs distress signs
try to aspirate stomach try to aspirate stomach contentscontents
auscultate for air sounds auscultate for air sounds with your stethoscope with your stethoscope (should hear a (should hear a whooshing sound in the whooshing sound in the epigastric region)epigastric region)
Secure the NG tube to Secure the NG tube to the patient’s nose with the patient’s nose with hypoallergenic tape hypoallergenic tape

TOTAL PARENTERAL TOTAL PARENTERAL NUTRITIONNUTRITION
TPN is administered to meet a TPN is administered to meet a client’s total nutritional needs when client’s total nutritional needs when oral feedings, tube feedings, and oral feedings, tube feedings, and standard IV feedings are standard IV feedings are contraindicated.contraindicated.
It’s used for client’s with various GI It’s used for client’s with various GI problems or other conditions that problems or other conditions that necessitate nutritional support such necessitate nutritional support such as some oncology clients.as some oncology clients.

IMPORTANT POINTS:IMPORTANT POINTS:
In most cases, administer TPN In most cases, administer TPN through a central vein such as through a central vein such as subclavian. The fluid is highly subclavian. The fluid is highly concentrated to provide rapid concentrated to provide rapid dilution and thus decrease the risks dilution and thus decrease the risks of peripheral inflammation and of peripheral inflammation and thrombosisthrombosis


GASTROINTESTINAL GASTROINTESTINAL DISORDERSDISORDERS

HIATAL HERNIAHIATAL HERNIA
A. ETIOLOGYA. ETIOLOGY 1. Portion of the stomach protruding 1. Portion of the stomach protruding
through a hiatus (opening) in the through a hiatus (opening) in the diaphragm into the thoracic cavity.diaphragm into the thoracic cavity.
2. May result from a congenital 2. May result from a congenital weakness of the diaphragm or from weakness of the diaphragm or from injury, pregnancy, or obesity.injury, pregnancy, or obesity.
3. Function of the cardiac sphincter 3. Function of the cardiac sphincter is lost, gastric juices enter the is lost, gastric juices enter the esophagus causing inflammation.esophagus causing inflammation.


B. CLINICAL FINDINGS:B. CLINICAL FINDINGS: 1. Subjective: 1. Subjective: substernal burning pain substernal burning pain
or fullness after eating; dyspepsia in the or fullness after eating; dyspepsia in the recumbent position; recumbent position; nocturnal dyspneanocturnal dyspnea..
2. Objective: GI series and endoscopy 2. Objective: GI series and endoscopy show protrusion of the stomach through show protrusion of the stomach through the diaphragm; regurgitation the diaphragm; regurgitation
C. THERAPEUTIC INTERVENTIONS:C. THERAPEUTIC INTERVENTIONS: 1. Small, frequent, bland feedings.1. Small, frequent, bland feedings. 2. Pharmacologic management: 2. Pharmacologic management:
antacids, antisecretory agents, antacids, antisecretory agents, antiemetics, especially those that antiemetics, especially those that promote gastric emptyingpromote gastric emptying
3. Surgical repair (done infrequently)3. Surgical repair (done infrequently) FundoplicationFundoplication

Nissen fundoplication. The fundus of the stomach is wrapped around the lower esophagus and the edges are sutured
together.

NURSING CARE:NURSING CARE: 1. Teach the client and family about 1. Teach the client and family about
the dietary regimen.the dietary regimen. 2. Encourage attempts at weight 2. Encourage attempts at weight
loss.loss. 3. Avoid constricting clothing and 3. Avoid constricting clothing and
heavy lifting.heavy lifting. 4. Encourage the client to 4. Encourage the client to sit up for sit up for
at least 1 hour after eating.at least 1 hour after eating. 5. Encourage the client to eat slowly 5. Encourage the client to eat slowly
and avoid drinking fluids with meals and avoid drinking fluids with meals to limit the volume in the stomach.to limit the volume in the stomach.

Gastroesophageal reflux Gastroesophageal reflux diseasedisease
Backflow of gastric contents, Backflow of gastric contents, doudenal contents, or both past the doudenal contents, or both past the lower esophageal sphincter (LES) into lower esophageal sphincter (LES) into the esophagus without associated the esophagus without associated belching or vomiting.belching or vomiting.
Usually occur after a mealUsually occur after a meal Occurs when LES is deficient or Occurs when LES is deficient or
pressure in stomach exceeds LES pressure in stomach exceeds LES pressure.pressure.



Gastroesophageal reflux Gastroesophageal reflux diseasediseaseCauses:Causes:
Food, alcohol, or cigarette that lower LES Food, alcohol, or cigarette that lower LES pressurepressure
Increased abdominal pressureIncreased abdominal pressure Hiatal herniaHiatal hernia Weakened esophageal sphincterWeakened esophageal sphincter
Assessment:Assessment: Burning pain in epigastric area/ heartburnBurning pain in epigastric area/ heartburn Pain after meals or when lying downPain after meals or when lying down

Gastroesophageal reflux diseaseGastroesophageal reflux disease
Decrease LES pressureDecrease LES pressure
LES relaxesLES relaxes
Gastrc contents regurgitates into the Gastrc contents regurgitates into the esophagusesophagus
Irritation of LESIrritation of LES
Inflammation and injuryInflammation and injury
Reflux esophagitisReflux esophagitis

Gastroesophageal reflux Gastroesophageal reflux diseasedisease
Nursing care:Nursing care: Frequent, small mealsFrequent, small meals Avoidance of eating before going to Avoidance of eating before going to
sleepsleep Sitting upright during and after mealsSitting upright during and after meals Sleeping with head elevatedSleeping with head elevated Antacid to neutralize acidic content of Antacid to neutralize acidic content of
the stomach and minimize irritation. the stomach and minimize irritation.

H2 blocker to inhibit gastric acid H2 blocker to inhibit gastric acid secretionsecretion
Proton pump inhibitor to reduce Proton pump inhibitor to reduce gastric aciditygastric acidity
Smoking cessation to improve LES Smoking cessation to improve LES pressure ( nicotine lowers LES pressure ( nicotine lowers LES pressure)pressure)
Surgery (if hiatal hernia is the source.) Surgery (if hiatal hernia is the source.)

GASTRITISGASTRITIS
GASTRITIS is an inflammation of the GASTRITIS is an inflammation of the gastric mucosa (the stomach lining). gastric mucosa (the stomach lining).
It may be acute or chronic. Acute It may be acute or chronic. Acute gastritis produces mucosal reddening, gastritis produces mucosal reddening, edema, hemorrhage, and erosion. edema, hemorrhage, and erosion. Chronic gastritis is common among Chronic gastritis is common among elderly people and people with elderly people and people with pernicious anemia. In chronic atrophic pernicious anemia. In chronic atrophic gastritis, all stomach mucosal layers gastritis, all stomach mucosal layers are inflamed.are inflamed.

POSSIBLE CAUSES:POSSIBLE CAUSES:Acute gastritisAcute gastritis Chronic ingestion of irritating foods, spicy Chronic ingestion of irritating foods, spicy
foods or alcoholfoods or alcohol Drugs, such as aspirin and other Drugs, such as aspirin and other
nonsteroidal anti-inflammatory drugs nonsteroidal anti-inflammatory drugs (NSAIDs)(in large doses), cytotoxic agents, (NSAIDs)(in large doses), cytotoxic agents, caffeine, corticosteroids, antimetabolites, caffeine, corticosteroids, antimetabolites, phenylbutazone, and indomethacinphenylbutazone, and indomethacin

Ingestion of poisons, especially Ingestion of poisons, especially dichlorodiphenyltrichloroethane dichlorodiphenyltrichloroethane (DDT), ammonia, mercury, carbon (DDT), ammonia, mercury, carbon tetrachloride, and corrosive tetrachloride, and corrosive substancessubstances
Endotoxins released from infecting Endotoxins released from infecting bacteria, such as staphylococci, bacteria, such as staphylococci, Escherichia coli, and salmonella, Escherichia coli, and salmonella, viruses (gastroenteritis)viruses (gastroenteritis)

GASTRITISGASTRITISBreak in the protective barrier of Break in the protective barrier of
stomach lining(prostaglandin)stomach lining(prostaglandin)
AutodigestionAutodigestion
HCL diffuses back to mucosa & injure HCL diffuses back to mucosa & injure small vesselssmall vessels
The walls & lining of stomach atrophyThe walls & lining of stomach atrophy
Destruction of the gastric glandsDestruction of the gastric glands
Hemorrhage & forms ulcerHemorrhage & forms ulcer

DIAGNOSTIC EVALUATION:DIAGNOSTIC EVALUATION:1.1. Fecal occult blood test can detect Fecal occult blood test can detect
occult blood in stools if the client occult blood in stools if the client has gastric bleeding.has gastric bleeding.
2.2. Blood studies show low Hgb level Blood studies show low Hgb level and Hct when significant bleeding and Hct when significant bleeding has occurred.has occurred.
3.3. Upper GI endoscopy with biopsy Upper GI endoscopy with biopsy confirms the diagnosis when confirms the diagnosis when performed within 24hrs of bleeding.performed within 24hrs of bleeding.
4.4. Upper GI series may be performed Upper GI series may be performed to exclude serious lesions.to exclude serious lesions.

TREATMENT:TREATMENT:-Blood transfusionBlood transfusion-I.V. fluid therapyI.V. fluid therapy-NG lavage to control bleedingNG lavage to control bleeding-Oxygen therapy, if necessaryOxygen therapy, if necessary-Partial or total gastrectomy (rare)Partial or total gastrectomy (rare)

IMPLEMENTATIONIMPLEMENTATION::1.1.If the client is vomiting, give If the client is vomiting, give antiemetics and I.V. fluids to prevent antiemetics and I.V. fluids to prevent dehydration and electrolyte imbalance.dehydration and electrolyte imbalance.2. Monitor fluid intake and output and 2. Monitor fluid intake and output and electrolyte levels.electrolyte levels.3. Offer smaller, more frequent meals 3. Offer smaller, more frequent meals to reduce irritating gastric secretions. to reduce irritating gastric secretions. Eliminate foods that cause gastric Eliminate foods that cause gastric upset. upset.

4. If surgery is necessary, prepare the 4. If surgery is necessary, prepare the client preoperatively and provide client preoperatively and provide appropriate postoperative care to appropriate postoperative care to decrease preoperative anxiety and decrease preoperative anxiety and prevent intraoperative and prevent intraoperative and postoperative complications.postoperative complications.
5. Administer antacids and other 5. Administer antacids and other prescribed medications prescribed medications

PEPTIC ULCER DISEASE PEPTIC ULCER DISEASE (PUD)(PUD)
A. ETIOLOGY:A. ETIOLOGY: 1. Ulcerations of the gastrointestinal 1. Ulcerations of the gastrointestinal
mucus and underlying tissues caused mucus and underlying tissues caused by gastric secretions that have a low by gastric secretions that have a low pH (acid)pH (acid)
2. Causes include conditions that 2. Causes include conditions that increase the secretion of hydrochloric increase the secretion of hydrochloric acid by the gastric mucosa or that acid by the gastric mucosa or that decrease the tissue’s resistance to the decrease the tissue’s resistance to the acid.acid.

PUDPUDh.pylori, acid & pepsin damages the barrierh.pylori, acid & pepsin damages the barrier
Autodigestion of acidsAutodigestion of acids
Inc.production of of acidInc.production of of acid
Dysfunction of the pyloric sphincterDysfunction of the pyloric sphincter
Large acid bolus into the doudenumLarge acid bolus into the doudenum
Mucosal inflammation & injuryMucosal inflammation & injury
Insufficient bile & p. enzymes to control the Insufficient bile & p. enzymes to control the acidacid
ulcerationulceration



THERAPEUTIC INTERVENTIONS:THERAPEUTIC INTERVENTIONS:11. Bland foods, and restriction of . Bland foods, and restriction of
irritating substances. irritating substances. 2. Antibiotic therapy if 2. Antibiotic therapy if
microorganism is identified; microorganism is identified; tetracycline, metronidazole, tetracycline, metronidazole, and bismuthand bismuth

3. Histamine H2 receptor antagonists 3. Histamine H2 receptor antagonists or proton pump inhibitors, antacids or proton pump inhibitors, antacids
4. Sedatives, tranquilizers, 4. Sedatives, tranquilizers, anticholinergics, and analgesics anticholinergics, and analgesics
5. Antiemetics5. Antiemetics

. . Surgical intervention:Surgical intervention: Billroth I: Billroth I:
removal of the removal of the lower portion of lower portion of the stomach and the stomach and attachment of attachment of the remaining the remaining portion to the portion to the duodenum.duodenum.

. Billroth II: . Billroth II: removal of the removal of the antrum and distal antrum and distal portion of the portion of the stomach and stomach and subsequent subsequent anastomosis of anastomosis of remaining section remaining section to the jejunum.to the jejunum.

Vagotomy – Vagotomy – surgical cuttting surgical cuttting of any of the of any of the branches of the branches of the vagus nerve.vagus nerve.
Antrectomy: Antrectomy: removal of the removal of the antral portion of antral portion of the stomach.the stomach.
Gastrectomy: removal of Gastrectomy: removal of 60%-80% of the 60%-80% of the
stomach.stomach.
Esophagojejunostomy Esophagojejunostomy (total gastrectomy): (total gastrectomy): removal of the entire removal of the entire stomach with a loop of stomach with a loop of
jejunum jejunum anastomosed to the anastomosed to the esophagusesophagus

Total gastrectomyTotal gastrectomy

dumping syndromedumping syndrome

The pathogenesis and The pathogenesis and manifestations of dumping manifestations of dumping
syndromesyndrome


APPENDICITISAPPENDICITIS


MEDICAL DIAGNOSIS AND TREATMENTMEDICAL DIAGNOSIS AND TREATMENT Surgical removal of the appendixSurgical removal of the appendix Management of peritonitis, shock, Management of peritonitis, shock,
dehydration, and infection dehydration, and infection Chest x-ray to differentiate appendicitis Chest x-ray to differentiate appendicitis
from pneumonia(pneumonia may cause from pneumonia(pneumonia may cause referred pain in the right lower quadrant referred pain in the right lower quadrant and thus may be misdiagnosed as and thus may be misdiagnosed as appendicitis)appendicitis)
Barium GI series and ultra-sonography to Barium GI series and ultra-sonography to differentiate appendicitis from other differentiate appendicitis from other abdominal problemsabdominal problems

DIVERTICULAR DIVERTICULAR DISEASEDISEASE

DIVERTICULAR DISEASEDIVERTICULAR DISEASE Diverticular disease has 2 clinical Diverticular disease has 2 clinical
forms: DIVERTICULOSIS and forms: DIVERTICULOSIS and DIVERTICULITIS. DIVERTICULITIS.
DiverticulosisDiverticulosis occurs when the occurs when the intestinal mucosa protrudes through intestinal mucosa protrudes through the muscular wall. The common sites the muscular wall. The common sites for diverticula are in the descending for diverticula are in the descending and sigmoid colon, but they may and sigmoid colon, but they may develop anywhere from the proximal develop anywhere from the proximal end of the pharynx to the anus.end of the pharynx to the anus.
DiverticulitisDiverticulitis is an inflammation of the is an inflammation of the diverticula that may lead to infection, diverticula that may lead to infection, hemorrhage, or obstruction.hemorrhage, or obstruction.


POSSIBLE CAUSES:POSSIBLE CAUSES:– Age (most common in people over age Age (most common in people over age
40)40)– Chronic constipation, more common in Chronic constipation, more common in
obese individualsobese individuals– Congenital weakening of the intestinal Congenital weakening of the intestinal
wallwall– Low intake of roughage and fiberLow intake of roughage and fiber– Straining during defecationStraining during defecation– StressStress– Men affected more than womenMen affected more than women

DIVERTICULAR DISEASEDIVERTICULAR DISEASELow fiber diet, constipationLow fiber diet, constipation
Musculature of the colon hyper trophiesMusculature of the colon hyper trophies
Herniation of the mucosa & submucosaHerniation of the mucosa & submucosa
Muscle weaknessMuscle weakness
Diverticula (diverticulosis)Diverticula (diverticulosis)
Trapped undigested food, fecal materialsTrapped undigested food, fecal materials
Bacteria builds up & impede blood flowBacteria builds up & impede blood flow
Inflammation (diverticulitis)Inflammation (diverticulitis)

ASSESSMENT FINDINGS:ASSESSMENT FINDINGS:
- Anorexia- Anorexia
- Stool with blood and mucus- Stool with blood and mucus
- Change in bowel habits- Change in bowel habits
- Constipation and diarrhea- Constipation and diarrhea
- Fever- Fever
- Flatulence- Flatulence
- Nausea- Nausea
- Rectal bleeding- Rectal bleeding

TREATMENT:TREATMENT:- Generally no treatment for asymptomatic - Generally no treatment for asymptomatic diverticulosisdiverticulosis- Colon resection (for diverticulitis refractory - Colon resection (for diverticulitis refractory to medical treatment)to medical treatment)- High residue diet with no seeds for - High residue diet with no seeds for diverticulosisdiverticulosis- Low residue diet with diverticulitis- Low residue diet with diverticulitis- high fiber diet- high fiber diet

- Temporary colostomy possible for - Temporary colostomy possible for perforation, peritonitis, obstruction, or perforation, peritonitis, obstruction, or fistula that accompanies diverticulitis.fistula that accompanies diverticulitis.•..

CROHN’s DISEASECROHN’s DISEASE((Regional Enteritis)Regional Enteritis)

CROHN’s DISEASECROHN’s DISEASE((Regional Enteritis)Regional Enteritis)
CROHN’s DISEASE is a chronic CROHN’s DISEASE is a chronic inflammatory disease of the small inflammatory disease of the small intestine, usually affecting the intestine, usually affecting the terminal ileum. It also sometimes terminal ileum. It also sometimes affects the large intestine, usually affects the large intestine, usually in the ascending colon. It’s slowly in the ascending colon. It’s slowly progressive with exacerbations progressive with exacerbations and remissions.and remissions.

POSSIBLE CAUSES:POSSIBLE CAUSES: Emotional upsetsEmotional upsets Fried foodsFried foods Milk and milk productsMilk and milk products UnknownUnknown

CROHN’s DISEASECROHN’s DISEASEAcute inflammation of entire intestinesAcute inflammation of entire intestines
Deep fissures & ulceration developsDeep fissures & ulceration develops
Loss of healthy intestinal surface area & bacterial Loss of healthy intestinal surface area & bacterial growthgrowth
Chronic changes include thickening of the bowel Chronic changes include thickening of the bowel wallwall
Narrowing and strictures of bowel lumenNarrowing and strictures of bowel lumen
Formation of fistula, perforation, hemorrhage, Formation of fistula, perforation, hemorrhage, obstruction, & abscessobstruction, & abscess


TREATMENT:TREATMENT: DRUG THERAPY OPTIONS:DRUG THERAPY OPTIONS: Analgesic: meperidine (Demerol), morphineAnalgesic: meperidine (Demerol), morphine Antianemic: ferrous sulfate (Feosol), ferrous Antianemic: ferrous sulfate (Feosol), ferrous
gluconate (Fergon)gluconate (Fergon) Antibiotic: sulfasalazine (Azulfidine), Antibiotic: sulfasalazine (Azulfidine),
metronidazole (Flagyl)metronidazole (Flagyl) Anticholinergic: propantheline (Pro-Anticholinergic: propantheline (Pro-
Banthine), dicyclomine (Bentyl)Banthine), dicyclomine (Bentyl)

Antidiarrheal: diphenoxylate (Lomotil)Antidiarrheal: diphenoxylate (Lomotil) Antiemetic: prochlorperazine Antiemetic: prochlorperazine
(Compazine)(Compazine) Anti-inflammatory: olsalazine Anti-inflammatory: olsalazine
(Dipentum)(Dipentum) Corticosteroid: prednisone (Deltasone)Corticosteroid: prednisone (Deltasone) Immunosupressant: mercaptopurine Immunosupressant: mercaptopurine
(Purinethol), azathioprine (Imuran)(Purinethol), azathioprine (Imuran) Potassium supplement: potassium Potassium supplement: potassium
chloride (K-Lor) administered with food, chloride (K-Lor) administered with food, potassium gluconate (Kaon)potassium gluconate (Kaon)

IMPLEMENTATION:IMPLEMENTATION: Bedrest, weigh dailyBedrest, weigh daily NPO in acute stage, TPN as ordered.NPO in acute stage, TPN as ordered. High CHON, calorie, bland, low residue High CHON, calorie, bland, low residue
diet.diet. Avoid gas-producers, irritating food, Avoid gas-producers, irritating food,
and milk products.and milk products.

Offer small frequent feedings.Offer small frequent feedings. Vitamin replacement ADEK.Vitamin replacement ADEK. IVF, I/O, tepid fluids up to 3L/day.IVF, I/O, tepid fluids up to 3L/day. Perianal care with lubricants and Perianal care with lubricants and
ointments.ointments. Hot sitz baths, monitor stools.Hot sitz baths, monitor stools. Emotional support esp. family Emotional support esp. family
members.members.

ULCERATIVE COLITISULCERATIVE COLITIS
ULCERATIVE COLITIS is a major health ULCERATIVE COLITIS is a major health problem and a potentially debilitating problem and a potentially debilitating disease. It’s a type of inflammatory bowel disease. It’s a type of inflammatory bowel disease that produces lesions primarily disease that produces lesions primarily confined to the large bowel, with confined to the large bowel, with ulcerations of the large bowel’s mucosa and ulcerations of the large bowel’s mucosa and submucosasubmucosa. .

POSSIBLE CAUSES:POSSIBLE CAUSES: GeneticsGenetics IdiopathicIdiopathic AllergiesAllergies Autoimmune diseaseAutoimmune disease Emotional stressEmotional stress Viral and bacterial infectionsViral and bacterial infections

ULCERATIVE COLITISULCERATIVE COLITISInflammation of the intestinal mucosa (rectum sigmoid Inflammation of the intestinal mucosa (rectum sigmoid
entire colon) entire colon)
InflammationInflammation
Loss epithelium with erosionLoss epithelium with erosion
UlcerationUlceration
Exudate edema with henorrhageExudate edema with henorrhage
Abscess & mucupurulent exudateAbscess & mucupurulent exudate
Necrosis and scarringNecrosis and scarring
Tissue replacement will narrow the colonTissue replacement will narrow the colon
Loss characteristics of epitheliumLoss characteristics of epithelium

ASSESSMENT FINDINGS:ASSESSMENT FINDINGS: Abdominal cramping, distention, and Abdominal cramping, distention, and
tendernesstenderness AnorexiaAnorexia Bloody, purulent, mucoid, watery stools (15 Bloody, purulent, mucoid, watery stools (15
to 20 per day)to 20 per day) DehydrationDehydration FeverFever Hyperactive bowel soundsHyperactive bowel sounds Nausea and vomitingNausea and vomiting WeaknessWeakness Weight lossWeight loss

DIAGNOSTIC EVALUATION:DIAGNOSTIC EVALUATION: Barium enema shows ulcerations.Barium enema shows ulcerations. Blood chemistry shows decreased potassium Blood chemistry shows decreased potassium
level and increased osmolality.level and increased osmolality. Hematology shows decreased Hgb level and Hematology shows decreased Hgb level and
Hct.Hct. Intestinal biopsy helps to differentiate between Intestinal biopsy helps to differentiate between
ulcerative colitis and regional enteritis.ulcerative colitis and regional enteritis. Stool specimen is positive for blood and mucus.Stool specimen is positive for blood and mucus. Urine chemistry displays increased urine Urine chemistry displays increased urine
specific gravity.specific gravity. TREATMENT:TREATMENT: Colectomy or ileostomyColectomy or ileostomy

IMPLEMENTATION:IMPLEMENTATION: Assess GI status and fluid balance to Assess GI status and fluid balance to
determine deficient fluid volume.determine deficient fluid volume. Monitor and record vital signs, intake Monitor and record vital signs, intake
and output, laboratory studies, daily and output, laboratory studies, daily weight, urine specific gravity, calorie weight, urine specific gravity, calorie count, and fecal occult blood to count, and fecal occult blood to determine deficient fluid volume.determine deficient fluid volume.

Monitor the number, amount, and Monitor the number, amount, and character of stools to determine character of stools to determine status of nutrient absorption.status of nutrient absorption.
Maintain the client’s diet; withhold Maintain the client’s diet; withhold food and fluid as necessary to food and fluid as necessary to prevent nausea and vomiting.prevent nausea and vomiting.
Administer I.V. fluids and TPN to Administer I.V. fluids and TPN to maintain hydration and improve maintain hydration and improve nutritional statusnutritional status

Types of OstomyTypes of Ostomy Ostomy = opening made Ostomy = opening made
to allow passage of urine to allow passage of urine or stool or stool – Piece of intestine is brought Piece of intestine is brought
out onto the client’s out onto the client’s abdomen. abdomen.
– Lacks nerve endings Lacks nerve endings – Doesn’t hurt to touch but Doesn’t hurt to touch but
has other implications has other implications Stoma = mouth like Stoma = mouth like
opening in the abdominal opening in the abdominal wall to drain urine or stool wall to drain urine or stool
Effluent – drainage from Effluent – drainage from stoma stoma

Ileostomy Ileostomy – End of small End of small
intestine intestine – By passes large By passes large
intestine = intestine = frequent liquid frequent liquid stools stools

Colostomy Colostomy – Large intestine Large intestine – More solid stool More solid stool

OSTOMY CAREOSTOMY CARE Referral to enterostomal therapist.Referral to enterostomal therapist. Encourage verbalization of fears/concerns.Encourage verbalization of fears/concerns. Teach character of drainage: ileostomy – liquid 4-Teach character of drainage: ileostomy – liquid 4-
6x/day, transverse colostomy – mushy OD, 6x/day, transverse colostomy – mushy OD, descending/sigmoid – soft formed q 2-3 daysdescending/sigmoid – soft formed q 2-3 days
Skin care – nystatin, karaya powder, soap/H2O Skin care – nystatin, karaya powder, soap/H2O pat drypat dry
Odor control – deodorant drops, bismuth tabs, Odor control – deodorant drops, bismuth tabs, mouthwash solutions, spinach, parsley added to mouthwash solutions, spinach, parsley added to ostomy bag.ostomy bag.
Odor – avoid gas-formers (cabbage, beans, Odor – avoid gas-formers (cabbage, beans, broccoli, cauliflower, corn, onions, eggs, fish, broccoli, cauliflower, corn, onions, eggs, fish, condiments.condiments.

Differential features of colitis & Differential features of colitis & crohn’s diseasecrohn’s disease
LocationLocation: (UC): (UC) Rectum-sigmoid-Rectum-sigmoid-
cecumcecum
EtiologyEtiology:: UnknownUnknown
Peak incidence:Peak incidence: 15-25 or 55-65 y.o.15-25 or 55-65 y.o.
StoolStool:: 10-20 liquid bloody 10-20 liquid bloody
stools per daystools per day
LocationLocation: ( crohn’s): ( crohn’s)
Terminal ileumTerminal ileum
EtiologyEtiology:: UnknownUnknown
Peak incidence:Peak incidence: 15-40 y.o.15-40 y.o.
StoolStool:: 5-6 soft loose rarely 5-6 soft loose rarely
bloody stools per bloody stools per dayday
Common complications:Hemorrhage, perforation, fistula,
nutritional deficiency

INTESTINAL INTESTINAL OBSTRUCTIONSOBSTRUCTIONS

Strangulated hernia
adhesionstumor
intussusceptionsVolvulus or twisting

INTESTINAL OBSTRUCTIONSINTESTINAL OBSTRUCTIONS

INTESTINAL INTESTINAL OBSTRUCTIONSOBSTRUCTIONS
Complications:Complications: Infection/septicemiaInfection/septicemia Gangrene of the bowelGangrene of the bowel Perforation of the bowelPerforation of the bowel Fluid imbalancesFluid imbalances

INTESTINAL OBSTRUCTIONSINTESTINAL OBSTRUCTIONS
Treatment:Treatment: Mechanical and vascular intestinal Mechanical and vascular intestinal
obstructions are generally treated obstructions are generally treated surgically; ileostomy or colostomy surgically; ileostomy or colostomy may be necessary.may be necessary.
Intestinal intubation and Intestinal intubation and decompressiondecompression
Maintain fluid and electrolyte balances Maintain fluid and electrolyte balances and adequate nutrition.and adequate nutrition.

CHOLELITHIASIS / CHOLELITHIASIS / CHOLECYSTITISCHOLECYSTITIS
A. ETIOLOGY AND PATHOPHYSIOLOGY:A. ETIOLOGY AND PATHOPHYSIOLOGY:
1.1. cholecystitis is the cholecystitis is the Inflammation of the Inflammation of the gallbladder; usually caused by gallbladder; usually caused by the presence of stones the presence of stones (cholelithiasis), which are (cholelithiasis), which are composed of cholesterol, bile composed of cholesterol, bile pigments, and calcium.pigments, and calcium.

Common locations of Common locations of gallstonesgallstonesAbnormal metabolism of
cholesterol & bile saltsGallstone fromation
Gallstones may obstruct gall bladder
Stasis of bileAutodigestion
Migration of gallstones to ductsInflammatory response
Iiritation & impaired blood flowIschemia of the gallbladder wall
Necrosis & gangrenePerforation
Abscess & peritonitis


C. THERAPEUTIC INTERVENTIONS:C. THERAPEUTIC INTERVENTIONS:
1.1.Medical managementMedical management
- Nasogastric suctioning to reduce - Nasogastric suctioning to reduce nausea and eliminate vomitingnausea and eliminate vomiting
- Narcotics to decrease pain- Narcotics to decrease pain
- Antispasmodics and anticholinergics - Antispasmodics and anticholinergics to reduce spasms and contractions of to reduce spasms and contractions of the gallbladderthe gallbladder
- Antibiotic therapy if infection is - Antibiotic therapy if infection is suspectedsuspected
- cholecystectomy- removal of the - cholecystectomy- removal of the gallbladdergallbladder

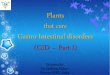
T-tube placement in the common bile duct. T-tube placement in the common bile duct. Bile fluid flows with gravity into a drainage Bile fluid flows with gravity into a drainage
collection device below the level of the collection device below the level of the common bile duct.common bile duct.

T tube care:T tube care: Semi fowlers positionSemi fowlers position Ensure that t-tube is connected to close Ensure that t-tube is connected to close
gravity draingravity drain Avoid kinks, clamping & pullingAvoid kinks, clamping & pulling MIO q shiftMIO q shift Expect 300-500ml bile colored drainage Expect 300-500ml bile colored drainage
(1(1stst 24H) 200ml/ 24H (3-4 days) 24H) 200ml/ 24H (3-4 days) Light colored stoolLight colored stool Skin care around the tubeSkin care around the tube

TREATMENT OF STONES:TREATMENT OF STONES:• CHOLESTEROL DISSOLVENT:CHOLESTEROL DISSOLVENT: MoctaninMoctanin is administered through a nasal biliary catheter to dissolve stones left in the bile duct after is administered through a nasal biliary catheter to dissolve stones left in the bile duct after
cholecystectomy. Dissolution may take 1 to 3 weeks. Observe the client for anorexia, nausea, cholecystectomy. Dissolution may take 1 to 3 weeks. Observe the client for anorexia, nausea, vomiting, and abdominal pain.vomiting, and abdominal pain.

ORAL BILE ACIDS:ORAL BILE ACIDS: ChenodiolChenodiol ( chenix ) and ( chenix ) and ursodiolursodiol
( actigall ) are administered to ( actigall ) are administered to dissolve small stones. Side effects dissolve small stones. Side effects include diarrhea ( especially with include diarrhea ( especially with chenodiol ), elevation of hepatic chenodiol ), elevation of hepatic enzymes,gastritis, and gastric ulcers. enzymes,gastritis, and gastric ulcers. Dissolution takes between 6 months Dissolution takes between 6 months and 2 years, and the success rate is and 2 years, and the success rate is only about 30 %only about 30 %

Percutaneous transhepatic dissolution Percutaneous transhepatic dissolution

Endoscopic Endoscopic sphincterotomy/retrograde sphincterotomy/retrograde cholangio-pancreatographycholangio-pancreatography

ESWL ESWL Lithotripsy is the use Lithotripsy is the use
of high-energy shock of high-energy shock waves to fragment waves to fragment and disintegrate and disintegrate biliary stones. ESWLbiliary stones. ESWL
(Extracorporeal (Extracorporeal Shock-wave Shock-wave Lithotripsy) – uses Lithotripsy) – uses soundwaves to soundwaves to pulverize gallstones pulverize gallstones (30-40mins) (30-40mins)
- suitable only for - suitable only for radiolucent stones radiolucent stones


PANCREATITISPANCREATITISPANCREATITIS is the inflammation of PANCREATITIS is the inflammation of
the pancreas.the pancreas. In acute pancreatitis, In acute pancreatitis, pancreatic enzymes are activated in pancreatic enzymes are activated in the pancreas rather than the the pancreas rather than the duodenum, resulting in tissue damage duodenum, resulting in tissue damage and autodigestion of the pancreas.and autodigestion of the pancreas.In chronic In chronic pancreatitis, chronic pancreatitis, chronic
inflammation resuinflammation results in fibrosis lts in fibrosis and and calcification of the pancreas, calcification of the pancreas, obstruction of the obstruction of the dducts, ucts, and and destruction destruction of the secreting acinar of the secreting acinar cells.cells.

POSSIBLE CAUSES:POSSIBLE CAUSES:1. Alcoholism - chronic1. Alcoholism - chronic2. Bacterial or viral infection2. Bacterial or viral infection3. Biliary tract disease - acute3. Biliary tract disease - acute4. Blunt trauma to the pancreas 4. Blunt trauma to the pancreas
or abdomenor abdomen5. Drugs: steroids, thiazide 5. Drugs: steroids, thiazide
diuretics, oral contraceptivesdiuretics, oral contraceptives

Inflammation caused premature acvtivation of enzymesCauses tissue damage
Enzymes back up and spill out into pancreatic tissue
Auto digestionAcute pancreatitis:
Hemorrhagic necrotising pancreatitis
Cell death & tissue damage Hemorrhage
Multi organ failure Shock
Chronic pancreatitis:Repeated attacks
Cell replacement of fibrous tissueInc.pressure & obstructionInflammation & destruction
Necrosis attack

ASSESSMENT FINDINGS:ASSESSMENT FINDINGS:
a.a. Abrupt onset of Abrupt onset of pain in the epigastric / pain in the epigastric / LUQ area that radiates to the shoulderLUQ area that radiates to the shoulder, , substernal area, back, and flanksubsternal area, back, and flank
b.b. Abdominal tenderness and distentionAbdominal tenderness and distention
c.c. Aching, burning, stabbing, pressing painAching, burning, stabbing, pressing pain
d.d. Knee-chest position, fetal positionKnee-chest position, fetal position, or , or leaning forward for comfort d/t abdominal leaning forward for comfort d/t abdominal painpain
e.e. Mental confusion, hypocalcemia – Mental confusion, hypocalcemia – irritabilityirritability
f.f. Nausea and vomitingNausea and vomiting

TESTS USED TO ELICIT SIGNS OF CALCIUM TESTS USED TO ELICIT SIGNS OF CALCIUM DEFICIENCYDEFICIENCY

g. g. Tachycardia, shock, hypotensionTachycardia, shock, hypotension
h. Dyspneah. Dyspnea
i. Low grade feveri. Low grade fever
j. j. Elevated serum amylase / lipase / Elevated serum amylase / lipase / glucoseglucose
k. k. Grey Turner’s, Cullens’s signGrey Turner’s, Cullens’s sign
l. Chronic l. Chronic steatorrheasteatorrhea
m. Jaundicem. Jaundice
o. o. HyperglycemiaHyperglycemia

TREATMENT: PANCREATITISTREATMENT: PANCREATITIS1.1. NPO, TPN, Bland, low-fat, high-protein diet NPO, TPN, Bland, low-fat, high-protein diet
of small, frequent meals with restricted of small, frequent meals with restricted intake of caffeine, alcohol, and gas-intake of caffeine, alcohol, and gas-forming foods forming foods
2.2. Bed restBed rest3. I.V. fluids (vigorous replacement of fluids 3. I.V. fluids (vigorous replacement of fluids
and electrolytes) BT: packed RBC, FWBand electrolytes) BT: packed RBC, FWB

4.4. Surgical intervention to treat the Surgical intervention to treat the underlying cause, if appropriateunderlying cause, if appropriate
5.5. Maintain position, patency, and low suction Maintain position, patency, and low suction of NG tube to prevent nausea and of NG tube to prevent nausea and vomiting.vomiting.
6.6. Monitor I/O, wt OD, abd girth, electrolytes.Monitor I/O, wt OD, abd girth, electrolytes.7.7. Monitor blood glucose levels.Monitor blood glucose levels.8.8. Meds: meperidine, H2 blockers, Meds: meperidine, H2 blockers,
anticholinergics, antacids, Ca gluconate, anticholinergics, antacids, Ca gluconate, pancreatic enzyme replacements (Viokase, pancreatic enzyme replacements (Viokase, Pancreatin, Pancrease)Pancreatin, Pancrease)

24–724–7 Pancreatoduodenectomy Pancreatoduodenectomy (Whipple’s procedure). (Whipple’s procedure). AA, areas of , areas of resection; resection; BB, appearance following , appearance following
resection.resection.


Cirrhosis of Cirrhosis of the liverthe liver

Lets go back to the function Lets go back to the function of the liver…of the liver…
a. Carbohydrate metabolism by liver cellsa. Carbohydrate metabolism by liver cells
-glycogenesis- glucose converted into -glycogenesis- glucose converted into glycogenglycogen
-glycogenolysis- glycogen is broken -glycogenolysis- glycogen is broken down into glucosedown into glucose
-gluconeogenesis- glucose into energy-gluconeogenesis- glucose into energy
b. Fat metabolism by liver cellsb. Fat metabolism by liver cells
c. Storing reserves of nutrients (ADEK & c. Storing reserves of nutrients (ADEK & B12)B12)

d. Filtering poisons and wastes from bloodd. Filtering poisons and wastes from blood
e. Production and synthesize variety of proteins. e. Production and synthesize variety of proteins.
Ex. Ex. AlbuminAlbumin (helps regulate the movement of (helps regulate the movement of water from the bloodstream)water from the bloodstream)
globin-globin- components of Hg (02 carrying substance components of Hg (02 carrying substance in RBC)in RBC)
globulin-globulin- group of protein that includes antibodies group of protein that includes antibodies
fibrinogen & prothrombin-fibrinogen & prothrombin- blood coagulation that blood coagulation that helps heal woundhelps heal wound

f. Regulating many chemicals found in f. Regulating many chemicals found in the blood streamthe blood stream
g. Can regenarate or grow backg. Can regenarate or grow back
h. Bile productionh. Bile production
i.i. Damaged repeatedly can cause Damaged repeatedly can cause irreversible changes that interfere irreversible changes that interfere function. function.
j. Conversion of ammonia to ureaj. Conversion of ammonia to urea

HEPATIC CIRRHOSISHEPATIC CIRRHOSIS
A. ETIOLOGY AND PATHOPHYSIOLOGYA. ETIOLOGY AND PATHOPHYSIOLOGY1. Irreversible fibrosis and degeneration of 1. Irreversible fibrosis and degeneration of
the liverthe liver
2. Several types of cirrhosis; La2. Several types of cirrhosis; Laënnec’s ënnec’s (alcoholic cirrhosis, nutritional cirrhosis) (alcoholic cirrhosis, nutritional cirrhosis) most common, biliary cirrhosis, & post most common, biliary cirrhosis, & post necrotic cirrhosisnecrotic cirrhosis
3. Incidence higher in alcoholics, who are 3. Incidence higher in alcoholics, who are often malnourished, and in those who have often malnourished, and in those who have had hepatitishad hepatitis

Chronic alcoholismChronic alcoholism
Toxic effect on hepatocytesToxic effect on hepatocytes
Liver inflammation (alcoholic hepatitis)Liver inflammation (alcoholic hepatitis)
Destructive phaseDestructive phase
Fibrosis or scar formationFibrosis or scar formation
NecrosisNecrosis
Hardened and lumpy liverHardened and lumpy liver
Liver ShrinksLiver Shrinks
Liver failureLiver failure

Hepatic circulationHepatic circulation

inc. hydrostatic pressure in portal circulation
Dec.plasma osmotic pressure
Inc.serum aldosterone & ADH
Upward pressure on diaphragm impairs respiration
inc. risk for peritonitis
Impaired digestion & absorption




C. THERAPEUTIC INTERVENTIONS:C. THERAPEUTIC INTERVENTIONS:
1.1. RestRest
2.2. Restriction of alcohol, hepatotoxic drugs. Restriction of alcohol, hepatotoxic drugs.
3.3. Vitamin therapy: especially the fat soluble Vitamin therapy: especially the fat soluble vitamins A, D, E and K and vitamin B vitamins A, D, E and K and vitamin B (thiamine chloride and nicotinic acid); zinc (thiamine chloride and nicotinic acid); zinc and calcium supplementsand calcium supplements
4.4. DiureticsDiuretics to control ascites and edema to control ascites and edema
5. 5. Neomycin and lactuloseNeomycin and lactulose may be may be prescribed for elevated blood ammonia prescribed for elevated blood ammonia levels (2-4 soft stools)levels (2-4 soft stools)
6. 6. ParacentesisParacentesis if respiratory distress occurs if respiratory distress occurs as a result of ascitesas a result of ascites

Paracentesis is a Paracentesis is a procedure to take procedure to take out fluid that has out fluid that has collected in the collected in the belly (belly (peritoneal fluid). ). This fluid buildup This fluid buildup is called is called ascites

Paracentesis SitesParacentesis Sites

Sites and position Sites and position for paracentesis. for paracentesis. AA, , Potential sites of Potential sites of needle or trocar needle or trocar insertion to avoid insertion to avoid abdominal organ abdominal organ damage. damage. BB, The , The client sits client sits comfortably; in this comfortably; in this position, the position, the intestines float intestines float back and away from back and away from the insertion site.the insertion site.

7. Surgical intervention to decrease 7. Surgical intervention to decrease portal hypertension: a portacaval portal hypertension: a portacaval
shunt or TIPSshunt or TIPS

8. Esophageal varices management8. Esophageal varices managementSengstaken-Blakemore tube:Sengstaken-Blakemore tube:

9. Dietary modification:9. Dietary modification:a. Cirrhosis:a. Cirrhosis:
1. 1. ProteinProtein as tolerated (80-100g); as tolerated (80-100g); with increasing liver damage, protein with increasing liver damage, protein metabolism is hinderedmetabolism is hindered
2. 2. High carbohydrateHigh carbohydrate, moderate , moderate fat; provides for fat; provides for energyenergy; ; vitamin, vitamin, mineralmineral, and , and electrolyte supplementselectrolyte supplements
33. Low sodium . Low sodium (500-1000mg daily); (500-1000mg daily); helps control increasing asciteshelps control increasing ascites
4. 4. Soft foods Soft foods if esophageal varices if esophageal varices are present; prevents danger of rupture are present; prevents danger of rupture and bleedingand bleeding
5. 5. AlcoholAlcohol contraindicated to avoid contraindicated to avoid irritation and malnutritionirritation and malnutrition

b. Hepatic comab. Hepatic coma
1. 1. ProteinProtein: reduced according : reduced according to tolerance; 15-30gto tolerance; 15-30g
2. 2. High calorie High calorie (1500-2000g) (1500-2000g) to prevent catabolism and to prevent catabolism and liberation of nitrogenliberation of nitrogen
33. Fluid . Fluid carefully controlled carefully controlled according to outputaccording to output

PeritonitisPeritonitis Peritonitis is Peritonitis is
the the generalized generalized inflammation inflammation of the of the peritoneal peritoneal cavity. Leading cavity. Leading intraabdominal intraabdominal infection.infection.

Intestinal motility is Intestinal motility is decreased, and fluid decreased, and fluid accumulates as a accumulates as a result of the inability result of the inability of the intestine to of the intestine to reabsorb fluid.reabsorb fluid.
Fluid will leak into the Fluid will leak into the peritoneal cavity, peritoneal cavity, precipitating fluid, precipitating fluid, electrolyte, and electrolyte, and protein losses, as well protein losses, as well as fluid depletion.as fluid depletion.

Inc. permeability
Intestinal bacteria leak out into peritoneal cavity
Bacterial peritonitis
Constant severe pain
Reflex contrxn of abdominal muscle
Hypovolemicshock
Dec. peristalsis adhesion

PYLORIC STENOSISPYLORIC STENOSIS Pyloric stenosis is Pyloric stenosis is
the obstruction of the obstruction of the pyloric the pyloric sphincter by sphincter by hypertrophy and hypertrophy and hyperplasia of the hyperplasia of the circular muscle of circular muscle of the pylorus.the pylorus.

AssessmentAssessment Risk factors/etiologyRisk factors/etiology 1. Occurs most often in firstborn, term 1. Occurs most often in firstborn, term
infants (infantile hypertrophic stenosis)infants (infantile hypertrophic stenosis) 2. More common in male infants.2. More common in male infants. 3. Seen more frequently in white infants.3. Seen more frequently in white infants.

Clinical manifestationsClinical manifestations 1. Onset of vomiting may be gradual, 1. Onset of vomiting may be gradual,
occurring in first few weeks; or forceful, occurring in first few weeks; or forceful, projectile vomiting may develop at 4 to 6 projectile vomiting may develop at 4 to 6 weeks of age.weeks of age.
2. Emesis is not bile stained but may be 2. Emesis is not bile stained but may be curdled from length of time in stomach.curdled from length of time in stomach.
3. Vomiting occurs shortly after feeding.3. Vomiting occurs shortly after feeding. 4. Infant is hungry and nurses well.4. Infant is hungry and nurses well.

5. Infant does not appear to be in pain or 5. Infant does not appear to be in pain or acute distress.acute distress.
6. Weight loss occurs, if untreated.6. Weight loss occurs, if untreated. 7. Stools decrease in number and in size.7. Stools decrease in number and in size. 8. Dehydration occurs as condition 8. Dehydration occurs as condition
progresses; hypochloremia and progresses; hypochloremia and hypokalemia as vomiting continues.hypokalemia as vomiting continues.
9. Upper abdomen is distended, and an 9. Upper abdomen is distended, and an “olive-shaped mass may be palpated in the “olive-shaped mass may be palpated in the right epigastric area.right epigastric area.

DiagnosticsDiagnostics 1. Palpation of abdominal mass.1. Palpation of abdominal mass. 2. Prolonged vomiting.2. Prolonged vomiting. 3. X-ray film and ultrasound 3. X-ray film and ultrasound
examination of abdomen.examination of abdomen.
Treatment; surgical release of the Treatment; surgical release of the pyloric muscle (pyloromyotomy)pyloric muscle (pyloromyotomy)

Celiac diseaseCeliac disease is also is also known as sprue, known as sprue, gluten enteropathygluten enteropathy, , and malabsorption and malabsorption syndrome. This syndrome. This disease is an inborn disease is an inborn error metabolism of error metabolism of rye, wheat, barley, rye, wheat, barley, and oat products. and oat products.
Celiac diseaseCeliac disease

Symptoms generally begin between the ages of Symptoms generally begin between the ages of 1 year and 5 years, but they may also occur in 1 year and 5 years, but they may also occur in those 50 to 60 years.those 50 to 60 years.
Severe malnutrition results from a loss of Severe malnutrition results from a loss of nutrients via the stool.nutrients via the stool.
Atrophy of villi of intestinesAtrophy of villi of intestines
Decrease absorptive surfaceDecrease absorptive surface
Decrease absorption of fatsDecrease absorption of fats
Malabsorption of fat soluble vitaminsMalabsorption of fat soluble vitamins
Severe malnutritionSevere malnutrition
Intolerance of gluten (BROW)
steatorrhea

AssessmentAssessment Cause: congenital defect in metabolism.Cause: congenital defect in metabolism.
Clinical manifestationsClinical manifestations 1. Symptoms begin when child has increased intake 1. Symptoms begin when child has increased intake
of gluten-type foods: cereals, breads, pastas, etc.of gluten-type foods: cereals, breads, pastas, etc. 2. Watery, pale diarrhea; steatorrhea.2. Watery, pale diarrhea; steatorrhea. 3. Vomiting, anorexia.3. Vomiting, anorexia. 4. Poor weight gain, failure to thrive.4. Poor weight gain, failure to thrive. 5. Constipation, vomiting, and abdominal pain may 5. Constipation, vomiting, and abdominal pain may
be the initial presenting signs/symptoms.be the initial presenting signs/symptoms. 6. Abdominal distention6. Abdominal distention

DiagnosticsDiagnostics 1. Stool analysis1. Stool analysis 2. Jejunal biopsy.2. Jejunal biopsy.
TreatmentTreatment Primarily dietary management; Primarily dietary management;
gluten-free dietgluten-free diet

HIRSCHSPRUNGS'S DISEASEHIRSCHSPRUNGS'S DISEASE
- - Hirschsprungs's Hirschsprungs's disease (congenital disease (congenital aganglionic aganglionic megacolon) megacolon) absence absence of innervations in a of innervations in a segment of colon segment of colon wall. Absent of wall. Absent of ganglion cells ganglion cells needed for needed for peristalsis.peristalsis.

AssessmentAssessment Risk factors/etiology; congenital, may Risk factors/etiology; congenital, may
be associated with Down syndrome.be associated with Down syndrome.
Clinical manifestationsClinical manifestations 1. varies according to age and amount 1. varies according to age and amount
of colon involved.of colon involved. 2. Inadequate or absent peristalsis.2. Inadequate or absent peristalsis. 3. Newborn.3. Newborn.
a. Failure to pass meconium within a. Failure to pass meconium within 24 to 24 to 48 hours after birth.48 hours after birth.
b. Vomitingb. Vomiting
c. Abdominal distention.c. Abdominal distention.
d. Reluctance to take fluids.d. Reluctance to take fluids.

4. Older infant.4. Older infant.
a. Passage of watery stools and diarrhea, a. Passage of watery stools and diarrhea, ribbon like stoolsribbon like stools
b. failure to thrive.b. failure to thrive.
c. Lack of appetite.c. Lack of appetite.
d. Persistent constipation, impactions.d. Persistent constipation, impactions.
DiagnosticsDiagnostics
1. Rectal biopsy.1. Rectal biopsy.
2. Barium enema.2. Barium enema.

TreatmentTreatment Surgical correction Surgical correction
usually involves usually involves creation of a temporary creation of a temporary colostomy, then a pull-colostomy, then a pull-through of the colon to through of the colon to a point near the a point near the rectum. After the rectum. After the reanastomosis has reanastomosis has healed, the temporary healed, the temporary colostomy is closed.colostomy is closed.

CLEFT LIP AND PALATECLEFT LIP AND PALATE
Cleft lip- Cleft lip- failure of maxillary and failure of maxillary and median nasal processes to fuse.median nasal processes to fuse.
- 7-8 weeks lip closes at age of - 7-8 weeks lip closes at age of gestation.gestation.
Cleft palate- Cleft palate- midline fissure of the midline fissure of the palatepalate
- 7-12 weeks palate closes at AOG- 7-12 weeks palate closes at AOG

Types of cleft lip & cleft Types of cleft lip & cleft palatepalate

CLEFT LIP AND PALATECLEFT LIP AND PALATE Manifestation:Manifestation:
1.1.Difficulty swallowingDifficulty swallowing
2.2.Distended abdomenDistended abdomen
3.3.Feeding difficultyFeeding difficulty Complication:Complication:
1.1.MalnutritionMalnutrition
2.2.Speech impedimentSpeech impediment
3.3.Possible aspirationPossible aspiration
4.4. Impaired self-esteemImpaired self-esteem

CLEFT LIP AND PALATECLEFT LIP AND PALATE Mgt/ InterventioMgt/ Intervention:n:
1.1.Surgery:Surgery: Cheiloplasty (6-12 weeks old)Cheiloplasty (6-12 weeks old) Uranoplasty- (4-6 weeks) to save Uranoplasty- (4-6 weeks) to save
speechspeech Palatoplasty (12-18 months old)Palatoplasty (12-18 months old) Feeding should be done in an Feeding should be done in an
upright positionupright position

Special nipples on feeding devices:Special nipples on feeding devices: Lamb’s nipple, flanged nipple, Lamb’s nipple, flanged nipple,
rubber-tipped medicine dropper, rubber-tipped medicine dropper, asepto syringeasepto syringe
Bubble and burp frequentlyBubble and burp frequently

CLEFT LIP AND PALATECLEFT LIP AND PALATEPost-op care (cleft lip)Post-op care (cleft lip) Metal appliance/ adhesive strips are Metal appliance/ adhesive strips are
taped to cheeks “logans bar”taped to cheeks “logans bar” Elbow restraintsElbow restraints Clear liquids initially, then formula Clear liquids initially, then formula
feeding as toleratedfeeding as tolerated Oral hygieneOral hygiene Meticulous care on suture lineMeticulous care on suture line Suctioning PRNSuctioning PRN Maintain upright positionMaintain upright position

CLEFT LIP AND PALATECLEFT LIP AND PALATE
Post-op care ( cleft palate)Post-op care ( cleft palate) Lie on abdomenLie on abdomen Fluids best taken from the cupsFluids best taken from the cups Avoid use of suction or other objects in the Avoid use of suction or other objects in the
mouthmouth Elbow restraintsElbow restraints Soft dietSoft diet Analgesic PRN- prevent crying of the Analgesic PRN- prevent crying of the
patientpatient

TRACHEOESOPHAGEAL FISTULA TRACHEOESOPHAGEAL FISTULA (TEF) with ESOPHAGEAL ATRESIA(TEF) with ESOPHAGEAL ATRESIA
TEF- An abnormal TEF- An abnormal opening in esophagus opening in esophagus and tracheaand trachea
EA- blind pouch or no EA- blind pouch or no continuous passage of continuous passage of esophagus and stomachesophagus and stomach
Causes: unknown Causes: unknown cause, malformation cause, malformation idiopathicidiopathic
Diagnostic: x-ray of Diagnostic: x-ray of abdomenabdomen

TRACHEOESOPHAGEAL TRACHEOESOPHAGEAL FISTULA (TEF) with FISTULA (TEF) with
ESOPHAGEAL ATRESIAESOPHAGEAL ATRESIA

TRACHEOESOPHAGEAL FISTULA TRACHEOESOPHAGEAL FISTULA (TEF) with ESOPHAGEAL ATRESIA(TEF) with ESOPHAGEAL ATRESIAAssessment:Assessment: Excessive salivation and droolingExcessive salivation and drooling 3 C’s of TEF3 C’s of TEF
CoughingCoughing
ChokingChoking
CyanosisCyanosis ApneaApnea Respiratory distressRespiratory distress Abdominal distensionAbdominal distension

TRACHEOESOPHAGEAL FISTULA TRACHEOESOPHAGEAL FISTULA (TEF) with ESOPHAGEAL ATRESIA(TEF) with ESOPHAGEAL ATRESIA
Surgical intervention:Surgical intervention: Division and ligation of TEF Division and ligation of TEF Anastomosis of esophagusAnastomosis of esophagus Age of surgery- 16-24 monthsAge of surgery- 16-24 months Temp. esophagostomyTemp. esophagostomy Temp. gastostomyTemp. gastostomy Post-op care: gastrostomy feedingPost-op care: gastrostomy feeding No oral intake 10-14 days post-opNo oral intake 10-14 days post-op

GastrostomyGastrostomy. . AA, Gastrostomy tube , Gastrostomy tube placement. placement. BB, The tube is fixed against , The tube is fixed against
both the abdomen and stomach walls by both the abdomen and stomach walls by cross bars. cross bars.

TRACHEOESOPHAGEAL FISTULA TRACHEOESOPHAGEAL FISTULA (TEF) with ESOPHAGEAL ATRESIA(TEF) with ESOPHAGEAL ATRESIA Nursing care:Nursing care: On NPO upon diagnosis, IV fluidsOn NPO upon diagnosis, IV fluids Frequent suctioningFrequent suctioning 02 administration02 administration Supine position with head elevated at least 30 Supine position with head elevated at least 30
degrees degrees Pacifier periodicallyPacifier periodically Complication after surgery: leak of Complication after surgery: leak of
anastomosis, strictures, esophageal motility anastomosis, strictures, esophageal motility disorderdisorder

GOOD LUCK AND GOD GOOD LUCK AND GOD BLESS!!!!BLESS!!!!
Post test after 10 Post test after 10 minutes…minutes…