Embed Size (px)
Citation preview

GIST FOR INTERNISTSDr. Napa ParinyanitikulMedical Oncology unit Department of MedicineFaculty of MedicineKing Chulalongkorn Memorial Hospital

Introduction
Gastrointestinal-Stromal tumor (GIST) is a most common mesenchymal neoplasm of gastrointestinal organ.
Not difference in sex.
75% found in patients older than 50 years.
These tumors can arise anywhere in the GI tract.


Clinical Manifestation
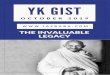
GIST may occur anywhere along the GI tract or elsewhere in the abdomen or retroperitoneum.
Emory et al. Am J Surg Pathol. 1999;23:82.
50%Stomach
25%Small
intestine
10%15%
Colon Other ( rectum, esophagus, mesentery, retroperitoneum)

Clinical Manifestation
Clinical feature : non-specific symptoms: asymptomatic: UGIB, abdominal mass, vague abdominal pain
and discomfort: Anemia, Anorexia, weight loss, nausea, fatigue: Acute intraperitoneal bleeding or perforation
Small, insignificant lesions may be found incidentally at endoscopy or at the time of surgery for other cancers as gastric cancer.

Clinical Manifestation
Average duration of presenting symptoms is 4-6 months.
Most GISTs arise from the bowel wall grow into the mucosa and cause ulceration or protrude towards the serosal side -> submucosal lesion
LN metastasis is rare presentation. But in advance GISTs may found lung or bone
metastasis.

EGD finding : submucosal lesion

Historical Classification as Other Soft-Tissue Sarcomas
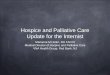
A retrospective Swedish study determined that 72% of GI tumors now identified as GIST had been originally classified as other tumors
GIST
Leiomyoma
Leiomyosarcoma
Leiomyoblastoma
Other
Kindblom et al. Ann Oncol. 2002;13:157. Abstract 577O. Kindblom. At: www.peerviewpress.com/asco2003c.
7%
13%
18%
34%
28%
N=600

Leiomyoma Leiomyosarcoma
Low-Grade GIST High-Grade GIST
Pathology : Morphologic Similarity To Smooth Muscle Tumors
Courtesy of Dr. C. Corless.

Pathogenesis
Originally arised from interstitial cell of Cajal. (ICC)
KIT-positive fibroblast-like cells
Pacemaker cells of the gut
Intercalated between intramural neurons and smooth muscle cells
Generate electrical slow waves
Loss of ICC function has been implicated in diabetic gastroenteropathy, gastroenteric arrhythmia, and Hirschsprung’s disease

Pathogenesis
GIST and ICC may arise from a common mesenchymal stem cell associated with enteric neural plexus.
GIST shares several characteristics with ICC.
ICC hyperplasia is evidence in GI tracts of pateints with familial GIST.
Takayama et al. Arch Histol cytol 2002, 65 :1-26
Wang et al. Arch Pathol Lab Med 2000, 124:1471-1475


KIT ligand : stem cell growth factor

Heinrich et al. Hum Pathol. 2002;33:484.Corless et al. Proc Am Assoc Cancer Res. 2003;44. Abstract R4447.
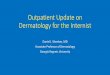
KIT and PDGFRA Mutations in GIST
Membrane
Cytoplasm
Exon 11 (67.5%)
Exon 9 (11%)
Exon 13 (0.9%)
Exon 17 (0.5%)
Exon 12 (0.9%)
Exon 18 (6.3%)
KIT (70-75%) PDGFRA 7%
Overall mutation frequency: 87.4%Wild type 10-15%
Exon 14 (0.3%)

GIST : Diagnosis
Depend on - Hx+PE - Radiology (CT scan , MRI whole abdomen,
PET/CT)- Pathology (FNA or Biopsy)


GIST : Staging
Evaluate symptoms or extend of mass
Detect metastasis
Assess tumor resectability


GIST : Biopsy
Preoperative biopsy in a resectable mass is commonly performed but may not be necessary and is associated with risks.
GISTs may be soft and fragile.
Biopsy may cause hemorrhage ad increase the risk of tumor dissemination.


GIST: Major Morphologic Patterns
Spindle Cell (70%) Epithelioid (9%)
Courtesy of Dr. C. Corless. Other-> mixed 21%

Immunohistochemistry
~95% of reported cases of GIST are positive for KIT (CD117)
Other markers often positive in GIST CD34
(mesenchymal/hematopoietic precursor cell marker) Positive in 60%-70%
Smooth-muscle actin Positive in 15%-60%
S-100 Positive in 10%
GIST rarely express desmin.Different KIT staining
patterns in GISTCourtesy of Dr. C. Corless.Miettinen and Lasota. Virchows Arch. 2001;438:1.

GIST : Management
Primary GIST Resectable GIST -> surgery (only curative Rx)
Locally advanced or Advanced GIST Neoadjuvant imatinib then surgery Palliative imatinib

Risk for tumor recurrence

Risk for tumor recurrence


SCIENTIFIC RATIONALE FOR IMATINIB IN THE TREATMENT OF ADVANCED GIST







Median OS of historical control 12 months








GIST : Imatinib resistance
Identify early tumor progression / late tumor progression
Increase dose imatinib 400 mg/d -> 800 mg/d Second-line treatment -> Sunitinib Many investigated drugs

The nodule within nodule

THANK YOU FOR YOUR ATTENTION