Embed Size (px)
Citation preview

Case
• Male aged 65yrs presented with the complains of progressive generalized weakness for the past 6months
• o/e pallor+, koilonychia+, smooth bald tongue+• HGB: 6gm/dl, MCV: 67fl, MCH: 20pg, RDW: 19,
TLC: 7,000cell/cumm, DLC: normal, PLT: 2lakhs/cumm
• What is the type of anemia?• What you would like the elicit in the history?

Case…. continued
• Male aged 65yrs presented with the complains of progressive generalized weakness for the past 6months
• o/e pallor+, koilonychia+, smooth bald tongue+• HGB: 6gm/dl, MCV: 67fl, MCH: 20pg, RDW: 19, TLC:
7,000cell/cumm, DLC: normal, PLT: 2lakhs/cumm• No h/o hemorrhoids, peptic ulcer, hematuria• Stool for ova/parasites: Negative• Stool for occult blood: Positive• What is the next step?

Case…. continued
• Colonoscopy: Large mass in the caecum
• Diagnosis: Carcinoma of colon

Terms
• Loss of heterozygosity – LOH• Constipation / obstipation

Colorectal CarcinomaColorectal Carcinoma
Dr.CSBR.Prasad, M.D.,

AdenocarcinomaAdenocarcinoma

AdenocarcinomaAdenocarcinoma
Small intestine: •Uncommon site for neoplasms•Tumors that may occur:– Adenocarcinoma– Carcinoid– Lymphoma– Sarcoma
Large intestine:•Common site for adenocarcinoma

Colorectal carcinoma - Colorectal carcinoma - AdenocarcinomaAdenocarcinoma

Colorectal carcinomaColorectal carcinoma
• Mostly Adenocarcinomas• 60-70yrs• < 20% of cases occur before 50yrs• M>F• Most common in developed countries– 30x less common in India / Africa

Colorectal carcinomaColorectal carcinoma
Risk factors:•Low Dietary fiber•Diet rich in fat and refined carbohydrates•Deficiencies of vitamins A, C, and E

Colorectal carcinomaColorectal carcinoma
Risk factors:
•High fat intake enhances the hepatic synthesis of cholesterol and bile acids, which can be converted into carcinogens by intestinal bacteria

Colorectal Colorectal carcinomacarcinoma

Colorectal carcinomaColorectal carcinoma
Risk factors:•Dietary modification•Pharmacologic chemoprevention

Colorectal carcinomaColorectal carcinoma
Risk factors:Dietary modification– Low fat & High fiber diet

Colorectal carcinomaColorectal carcinoma
Risk factors:Pharmacologic chemoprevention – Aspirin or other NSAIDs have a
protective effect


PathogenesisPathogenesis
• Heterogeneous genetic abnormalities• Genetic and Epigenetic abnormalitiesTwo distinct genetic pathways:1.APC/β-catenin pathway – associated with WNT and the classic adenoma-
carcinoma sequence
2.The microsatellite instability pathway

APC/β-Catenin Pathway
• APC (WNT signaling pathway) - control cell fate, adhesion, and cell polarity during embryonic development
• APC gene (5q21) down-regulate growth-promoting signals – ‘Tumor suppressor’
• An important function of the APC protein is to down-regulate β-catenin

APC/β-Catenin PathwayWNT signals through a family of cell surface receptors called frizzled (FRZ)

• 80% of sporadic colon tumors• Mutation of APC (LOH)• Additional mutations:– Activating mutations in KRAS– Mutations in SMAD2 and SMAD4– p53 mutation – Methylation of promoter region– Increase expression of telomerase
PathogenesisPathogenesis 1- Adenoma-carcinoma sequence 1- Adenoma-carcinoma sequence

PathogenesisPathogenesis 1- Adenoma-carcinoma sequence 1- Adenoma-carcinoma sequence

PathogenesisPathogenesis 2- Microsatellite instability 2- Microsatellite instability
• DNA mismatch repair deficiency • Accumulation of mutations in microsatellite repeats
(Microsatellite instability)• Most of them are silent• Mutation resulting in MSI involving:– type II TGF-β receptor (uncontrolled cell growth)– the pro-apoptotic protein BAX (survival of genetically
abnormal clones)• Mutations in the oncogene BRAF• Hypermethylation of MLH1• KRAS and p53 are not typically mutated

PathogenesisPathogenesis 2- Microsatellite instability 2- Microsatellite instability
Thus, the combination of the following is the signature of this pathway of carcinogenesis:– MSI– BRAF mutation, and – Methylation of specific targets, such as MLH1

PathogenesisPathogenesis 2- Microsatellite instability 2- Microsatellite instability

PathogenesisPathogenesis 3- Hypermethylation of 3- Hypermethylation of promoter & absence of MSIpromoter & absence of MSI
• Increased CpG island methylation in the absence of microsatellite instability
• Many of these tumors harbor KRAS mutations, but p53 and BRAF mutations are uncommon

Morphology and molecular alterations
• Sessile serrated adenomas: Mismatch repair deficiency and MSI
• Tumors with prominent mucinous differentiation and peritumoral lymphocytic infiltrates: – MSI– Frequently located in the right colon

Morphology – Carcinoma of Colon• Can occur in any part of the colonIn the proximal colon: – Polypoid, exophytic masses– Rarely cause obstruction– Symptoms occur LATELY
In the distal colon:– Annular lesions – “Napkin-ring” constriction – Luminal narrowing > Obstruction– Symptoms occur EARLY

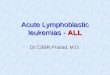
Carcinoma colonCarcinoma colonExophytic type Napkin ring type

Napkin rings

Carcinoma colonCarcinoma colon
Exophytic type Napkin ring type

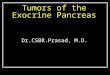
Colorectal carcinoma – infiltration in to the muscle coat

Morphology – Microscopic features
• Most tumors are composed of glands lined by tall columnar cells with features of malignancy
• Invasive tumors elicits desmoplastic response• Poorly differentiated tumors form few glands • Some produce abundant mucin - poor
prognosis• Some poorly differentiated tumors composed
of signet-ring cells

Morphology – Microscopic features

Morphology – Microscopic features

Clinical FeaturesClinical Features
• Right sided tumors: – Go undetected for long periods– Present with fatigue and weakness due to iron
deficiency anemia • Left-sided tumors: – Occult bleeding– Changes in bowel habits– Cramping left lower quadrant discomfort

Clinical FeaturesClinical Features
Clinical MAXIMClinical MAXIM: :
•The underlying cause of iron deficiency anemia in an older man or postmenopausal woman is GI cancer until proven otherwise

The two most important Prognostic Factors
1. Depth of invasion • Invasion into the muscularis propria confers
significantly reduced survival
2. Lymph node metastases

Metastases
• Metastases may involve regional lymph nodes, lungs and bones
• but LIVER is the most common site of metastatic lesions (as a result of portal drainage of the colon)
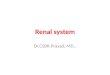
• Mets in the liver are often umbilicated

Umbilicated liver mets

Metastatic colorectal carcinoma




HNPCCHNPCC

E N D

Dr.Denis Burkitt Burkitt’s Lymphoma

Dr.Denis Birkitt Fiber and Colonic carcinoma
America is a constipated nation.... If you pass small stools, you have to have large hospitals – Denis Burkitt

Trosseau syndrome (migrating thrombophlebitis)

Sister Joseph Lilly nodule