Embed Size (px)
Citation preview

HCV Alerts: Rapid Response to Practice-Changing Advances
Supported by an educational grant from AbbVie.
Practice-Changing Advances From EASL 2015

clinicaloptions.com/hepatitisHCV Alerts: Rapid Response to Practice-Changing Advances
About These Slides
Users are encouraged to use these slides in their own noncommercial presentations, but we ask that content and attribution not be changed. Users are asked to honor this intent
These slides may not be published or posted online without permission from Clinical Care Options (email [email protected])
DisclaimerThe materials published on the Clinical Care Options Web site reflect the views of the authors of the CCO material, not those of Clinical Care Options, LLC, the CME providers, or the companies providing educational grants. The materials may discuss uses and dosages for therapeutic products that have not been approved by the United States Food and Drug Administration. A qualified healthcare professional should be consulted before using any therapeutic product discussed. Readers should verify all information and data before treating patients or using any therapies described in these materials.

clinicaloptions.com/hepatitisHCV Alerts: Rapid Response to Practice-Changing Advances
Faculty
Mark S. Sulkowski, MDProfessor of MedicineMedical Director, Viral Hepatitis CenterDivisions of Infectious Diseases and Gastroenterology/HepatologyJohns Hopkins University School of MedicineBaltimore, Maryland
Program Director:
Paul Y. Kwo, MDProfessor of MedicineMedical Director of TransplantationDivision of Medicine/ Gastroenterology/Hepatology Indiana University School of MedicineIndianapolis, Indiana

clinicaloptions.com/hepatitisHCV Alerts: Rapid Response to Practice-Changing Advances
Faculty Disclosures
Mark S. Sulkowski, MD, has disclosed that he has received consulting fees from AbbVie, Achillion, Bristol‐Myers Squibb, Gilead Sciences, Janssen, and Merck; funds for research support from AbbVie, Bristol‐Myers Squibb, Gilead Sciences, and Merck; and data and safety monitoring board funding (to his institution) from Gilead Sciences.
Paul Y. Kwo, MD, has disclosed that he has received funds for research support from AbbVie, Bristol-Myers Squibb, Conatus, Gilead Sciences, Janssen, Merck, and Roche and consulting fees from AbbVie, Bristol-Myers Squibb, Gilead Sciences, Janssen, and Merck.

Managing HCV Infectionin Renal Disease
clinicaloptions.com/hepatitisHCV Alerts: Rapid Response to Practice-Changing Advances
RUBY-1: OMV/PTV/RTV + DSV ± RBV in Tx-Naive, Noncirrhotic GT1 Pts With CKD Interim analysis of multicenter, open-label phase IIIb study
Ombitasvir/paritaprevir/ritonavir 25/150/100 mg QD + dasabuvir 250 mg BID ± ribavirin* 200 mg QD for 12 wks
Key baseline characteristics
– F2 fibrosis: 30%; F3 fibrosis: 20%
– CKD stage 4 (eGFR 15-30): 35%; CKD stage 5 (eGFR < 15): 65%
– 65% of pts on hemodialysis
Pockros PJ, et al. EASL 2015. Abstract L01.
*RBV dosed 4 hrs before hemodialysis in hemodialysis pts; weekly hemoglobin assessment in Month 1 and then Wks 6, 8, 12; RBV suspended in pts with > 2 g/dL decline in hemoglobin in < 4 wks or hemoglobin < 10 g/dL; RBV dosing resumed at clinician’s discretion if hemoglobin normalized.

clinicaloptions.com/hepatitisHCV Alerts: Rapid Response to Practice-Changing Advances
RUBY-1: Safety and Interim Efficacy
OMV/PTV/RTV + DSV ± RBV well tolerated for GT1 HCV and advanced CKD
No treatment-related serious AEs, discontinuations, or significant changes in liver or renal function to date
RBV dose interruption in 8/13 GT1a pts (6 in first 4 wks)
– 4 pts received EPO, 1 pt with hemoglobin < 8 mg/dL
Most AEs mild to moderate
Interim virologic efficacy
– SVR4 in 10/10 pts reaching posttreatment Wk 4
– SVR12 in 2/2 pts reaching posttreatment Wk 12
– No virologic failures observed as of time of reporting
Pockros PJ, et al. EASL 2015. Abstract L01.
AEs Found in > 3 Pts, n
GT1b:OMV/PTV/RTV
+ DSV(n = 7)
GT1a:OMV/PTV/RTV + DSV + RBV
(n = 13)
Anemia 0 8
Fatigue 2 4
Diarrhea 1 4
Nausea 0 5
clinicaloptions.com/hepatitisHCV Alerts: Rapid Response to Practice-Changing Advances
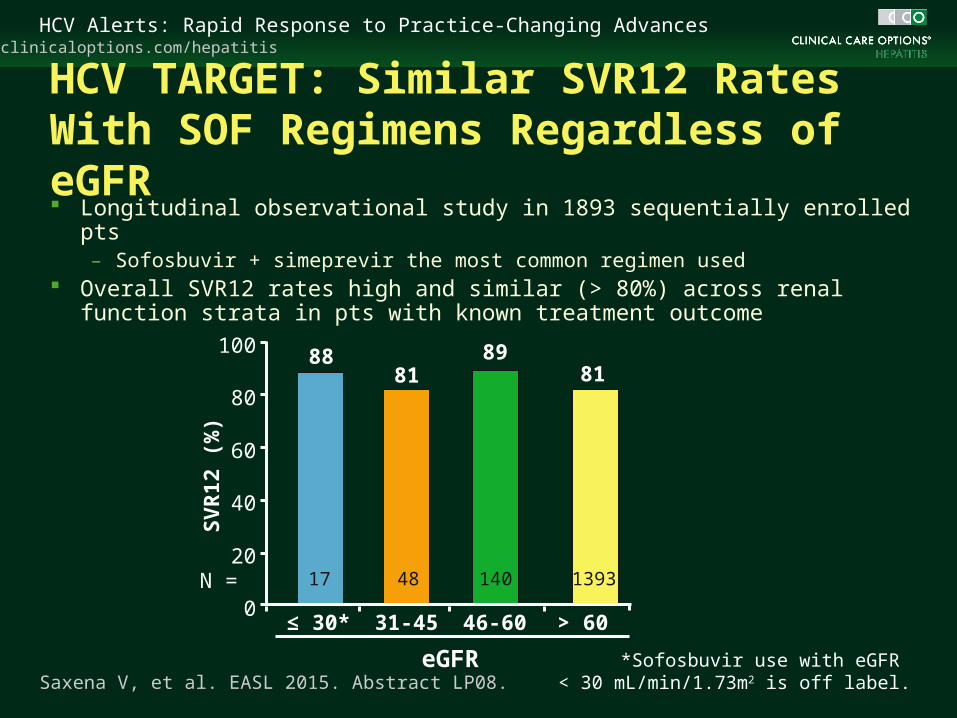
Saxena V, et al. EASL 2015. Abstract LP08.
HCV TARGET: Similar SVR12 Rates With SOF Regimens Regardless of eGFR Longitudinal observational study in 1893 sequentially enrolled pts
– Sofosbuvir + simeprevir the most common regimen used Overall SVR12 rates high and similar (> 80%) across renal function
strata in pts with known treatment outcome
81
48
88
17
≤ 30*
100
80
60
40
20
0
SV
R12
(%
)
eGFR
81
1393
89
140
31-45 46-60 > 60
N =
*Sofosbuvir use with eGFR < 30 mL/min/1.73m2 is off label.
clinicaloptions.com/hepatitisHCV Alerts: Rapid Response to Practice-Changing Advances
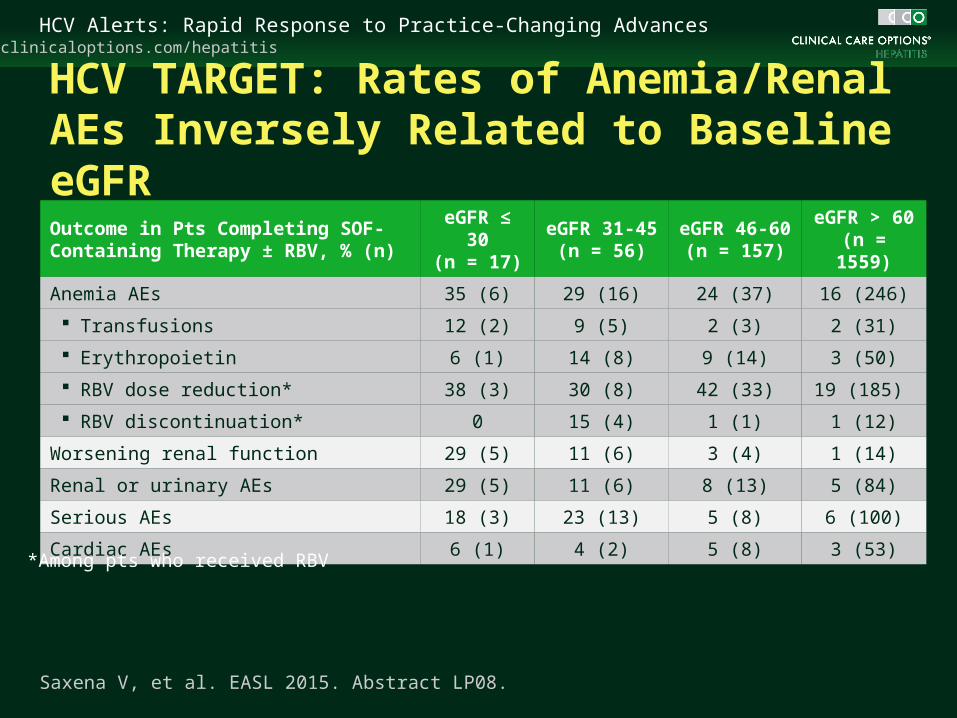
HCV TARGET: Rates of Anemia/Renal AEs Inversely Related to Baseline eGFR Outcome in Pts Completing SOF-Containing Therapy ± RBV, % (n)
eGFR ≤ 30(n = 17)
eGFR 31-45(n = 56)
eGFR 46-60(n = 157)
eGFR > 60(n = 1559)
Anemia AEs 35 (6) 29 (16) 24 (37) 16 (246)
Transfusions 12 (2) 9 (5) 2 (3) 2 (31)
Erythropoietin 6 (1) 14 (8) 9 (14) 3 (50)
RBV dose reduction* 38 (3) 30 (8) 42 (33) 19 (185)
RBV discontinuation* 0 15 (4) 1 (1) 1 (12)
Worsening renal function 29 (5) 11 (6) 3 (4) 1 (14)
Renal or urinary AEs 29 (5) 11 (6) 8 (13) 5 (84)
Serious AEs 18 (3) 23 (13) 5 (8) 6 (100)
Cardiac AEs 6 (1) 4 (2) 5 (8) 3 (53)
Saxena V, et al. EASL 2015. Abstract LP08.
*Among pts who received RBV

clinicaloptions.com/hepatitisHCV Alerts: Rapid Response to Practice-Changing Advances
Take-Home Points: HCV Therapy in the Setting of Renal Insufficiency Safety and efficacy data now available for OMV/PTV/RTV
+ DSV ± RBV in hemodialysis pts
– In pts with genotype 1a HCV, AEs remain a concern with RBV, even at low doses
Efficacy data now for available for SOF-based regimens in pts with eGFR ≤ 30
– Owing to decreased excretion of metabolite GS-331007, safety remains uncertain

Role of Resistance Testing in HCV Retreatment
clinicaloptions.com/hepatitisHCV Alerts: Rapid Response to Practice-Changing Advances
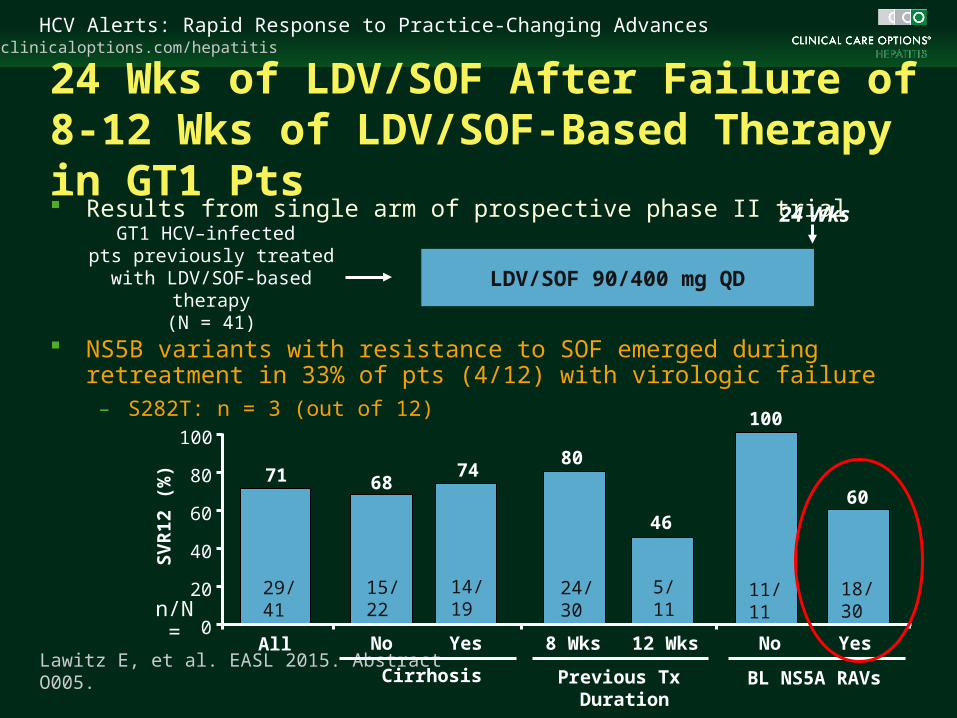
24 Wks of LDV/SOF After Failure of 8-12 Wks of LDV/SOF-Based Therapy in GT1 Pts Results from single arm of prospective phase II trial
NS5B variants with resistance to SOF emerged during retreatment in 33% of pts (4/12) with virologic failure
– S282T: n = 3 (out of 12)
Lawitz E, et al. EASL 2015. Abstract O005.
LDV/SOF 90/400 mg QD
GT1 HCV–infected pts previously treated with LDV/SOF-based therapy
(N = 41)
24 Wks
100
80
60
40
20
0
SV
R12
(%
)
All No Yes
71 6874
15/22
14/19
No Yes8 Wks 12 Wks
Cirrhosis Previous Tx Duration
BL NS5A RAVs
80
4660
100
24/30
5/11
11/11
18/30n/N =
29/41

clinicaloptions.com/hepatitisHCV Alerts: Rapid Response to Practice-Changing Advances
OPTIMIST-2: SMV + SOF for 12 Wks in Cirrhotic Tx-Naive and Tx-Exp’d GT1 Pts Multicenter, open-label, single-arm
phase III trial[1]
Key baseline characteristics
– 70% GT1a (47% with Q80K)
– 72% IL28B non-CC
– 18% black, 16% Hispanic
– 51% treatment exp’d
– 18% with platelets < 90,000 cells/mm3
– 51% with albumin < 4 g/dL
Among cirrhotic pts, SVR12 rates were lower in those with GT1a with Q80K mutation
OPTIMIST-1: No impact of Q80K seen in noncirrhotic pts with GT1a[2]
1. Lawitz E, et al. EASL 2015. Abstract LP04. 2. Kwo P, et al. EASL 2015. Abstract LB14.
100
80
60
40
20
0
SV
R12
(%
)
GT1a GT1a WithQ80K
GT1a WithoutQ80K
GT1b
60/72 25/34 35/38 26/31
8374
9284
n/N =

clinicaloptions.com/hepatitisHCV Alerts: Rapid Response to Practice-Changing Advances
Take-Home Points: Role of Resistance Testing The presence of resistance associated variants to DAAs
prior to treatment may have an impact on SVR, especially in pts with previous DAA treatment experience and/or cirrhosis
Consider resistance testing prior to retreatment in patients who fail to achieve HCV cure with DAA-based treatments

Advances in the Treatment of Genotype 3 HCV Infection

clinicaloptions.com/hepatitisHCV Alerts: Rapid Response to Practice-Changing Advances
Treatment Naive Treatment Experienced
BOSON: SVR12 in GT3 by Tx History and Cirrhosis Status
Foster GR, et al. EASL 2015. Abstract LO5.
58/70
65/72
68/71
12/21
18/22
21/23
26/34
17/36
30/35
44/54
49/52
41/54
No Cirrhosis Cirrhosis No Cirrhosis Cirrhosis
8390
96
57
8291
7682
94
47
7786100
80
60
40
20
0
SV
R12
(%
)
SOF + RBV for 16 wks SOF + RBV for 24 wks SOF + pegIFN/RBV for 12 wks
n/N =
Multicenter, randomized, open-label study
clinicaloptions.com/hepatitisHCV Alerts: Rapid Response to Practice-Changing Advances
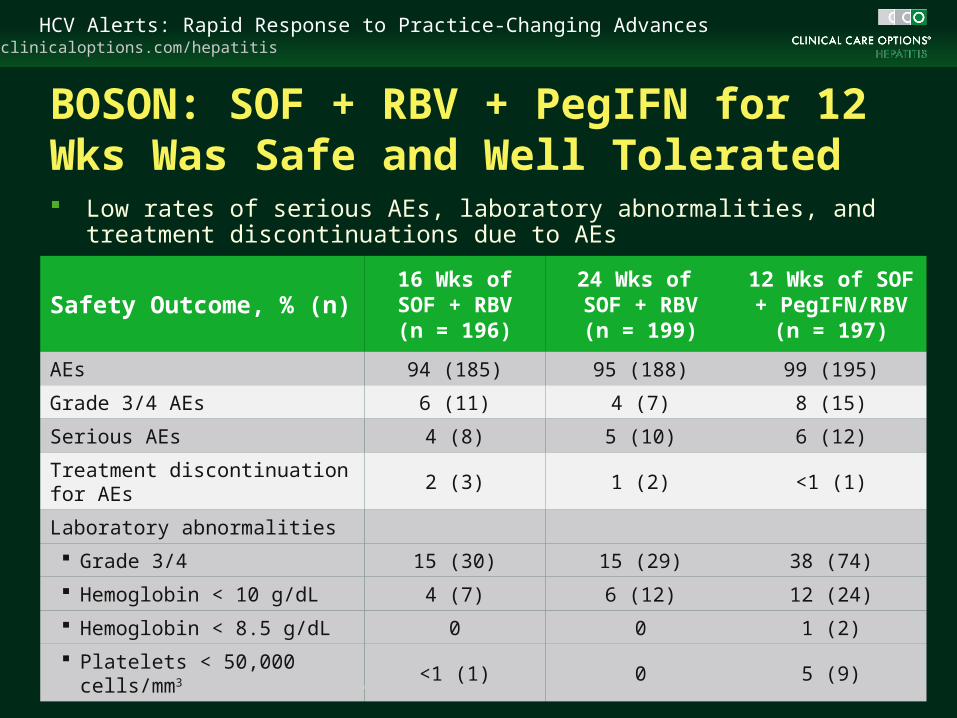
BOSON: SOF + RBV + PegIFN for 12 Wks Was Safe and Well Tolerated
Foster GR, et al. EASL 2015. Abstract LO5.
Safety Outcome, % (n)16 Wks of
SOF + RBV(n = 196)
24 Wks of SOF + RBV
(n = 199)
12 Wks of SOF + PegIFN/RBV
(n = 197)
AEs 94 (185) 95 (188) 99 (195)
Grade 3/4 AEs 6 (11) 4 (7) 8 (15)
Serious AEs 4 (8) 5 (10) 6 (12)
Treatment discontinuation for AEs 2 (3) 1 (2) <1 (1)
Laboratory abnormalities
Grade 3/4 15 (30) 15 (29) 38 (74)
Hemoglobin < 10 g/dL 4 (7) 6 (12) 12 (24)
Hemoglobin < 8.5 g/dL 0 0 1 (2)
Platelets < 50,000 cells/mm3 <1 (1) 0 5 (9)
Low rates of serious AEs, laboratory abnormalities, and treatment discontinuations due to AEs
clinicaloptions.com/hepatitisHCV Alerts: Rapid Response to Practice-Changing Advances
Take-Home Points: Treatment for Genotype 3 HCV Infection SOF + pegIFN/RBV for 12 wks may be best current option
in treatment-experienced pts with GT3 HCV infection
– Addition of pegIFN to SOF + RBV for 12 wks associated with highest rate of SVR12 in treatment-experienced pts with GT3, particularly those with cirrhosis
To achieve high SVR rates with SOF in GT3, an additional active drug may be needed
– Studies of combinations of novel DAAs with increased activity against GT3 are under way
Go Online for More From this Program!
Downloadable PowerPoint slides from each Webinar
Downloadable audio from the live Webinars
clinicaloptions.com/alerts





























