Embed Size (px)
DESCRIPTION
Citation preview

QuickTime™ and a decompressor
are needed to see this picture.
Homeless PACT (PCMH)
David I. Rosenthal MDMedical Director – Homeless PACT, VA Asst Prof,
Section of General Internal Medicine, Yale School of Medicine
2010 HUD Report on Homelessness

QuickTime™ and a decompressor
are needed to see this picture.

QuickTime™ and a decompressor
are needed to see this picture.





• http://maketheconnection.net/stories-of-connection?experiences=11

Background
• On a typical night in 2010, more than 400,000 homeless individuals in the US (1)
• ~10% experienced chronic homelessness– Defined as homelessness >1 year or 4 episodes in the past 3 years
(1) The 2010 Annual Homeless Assessment Report to Congress. Department of Housing and Urban Development (US), Office of Community Planning and Development. Available at http://www.hudhre.info/documents/2010HomelessAssessmentReport.pdf

http://www.pathwaystohousing.org/content/our_model
QuickTime™ and a decompressor
are needed to see this picture. Housing Services OverviewHousing Services Overview

Housing First - Core Principles
Consumer choice and empowerment Separation of services and housing Services are voluntary and flexibleCommunity integrationHarm reduction and recovery oriented
QuickTime™ and a decompressor
are needed to see this picture. Housing Services OverviewHousing Services Overview

Homeless
Shelter placement
Transitional housing
Permanent housing
Leve
l of i
ndep
ende
nce
Treatment compliance + psychiatric stability + abstinence
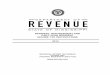
Underlying theory and values:•Transitional placements provide for stabilization and learning.•Individual change is required through treatment.•Consumers must ‘earn’ permanent housing
Treatment First Model
Tsemberis slide, 2010
QuickTime™ and a decompressor
are needed to see this picture. Housing Services OverviewHousing Services Overview

Homeless
Shelter placement
Transitional housing
Permanent housing
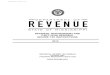
Ongoing, flexible supports
Housing First Model
Tsemberis slide, 2010
QuickTime™ and a decompressor
are needed to see this picture. Housing Services OverviewHousing Services Overview

Community Housing
15

The Eleanor and Franklin Formerly Park City--Bridgeport, CT
Permanent Supportive Housing55 Elderly & 49 Homeless Mentally Ill
Legion Woods, New Haven, CT
Permanent Supportive
Housing- 20 Units
Transitional—14 Beds
Harkness House, West Haven, CT
Kossuth Street—New Haven, CT
Yale School of Architecture
Homeownership
Community Partnerships
16

Jewett City/American Legion
2010
OpenedJune 2012

Jewett City/American Legion
18
Street View
Interior View

Why Housing First?
1. It ends homelessness2. Housing First eliminates the need for costly shelter care,
transitional and short term treatment services aimed at preparing Veterans to be housing ready.
3. Studies demonstrate the Housing First reduces ER visits, unscheduled mental health and medical hospitalization
4. Decreases the frequency and duration of homelessness
QuickTime™ and a decompressor
are needed to see this picture. Housing Services OverviewHousing Services Overview

VA Housing ProgramsDomiciliary Care for Homeless Veterans
The Domiciliary Care Program is a clinical rehabilitation and treatment program for male and female Veterans. The Domiciliary Care Program addresses goals of rehabilitation, recovery, health maintenance, improved quality of life, and community integration in addition to specific treatment of medical conditions, mental illnesses, addictive disorders, and homelessness.
Department of Housing and Urban Development/Department of Veterans Affairs Supportive Housing (HUD-VASH)Through the HUD-VASH Program, HUD and VA, through a cooperative partnership, provide long-term case management, supportive services and permanent housing support for Veterans who require these supports in order to live independently.
QuickTime™ and a decompressor
are needed to see this picture. Housing Services OverviewHousing Services Overview

VA Housing Programs, cont.Grant and Per Diem (GPD)
The Grant and Per Diem (GPD) Program funds community-based agencies providing transitional housing or service centers for homeless Veterans. A Veteran can typically reside in a GPD Program for up to 2 years.
Supportive Services for Veteran Families Program
The Supportive Services for Veteran Families (SSVF) Program is a new VA program that will provide supportive services to very low-income Veterans and their families who are in or transitioning to permanent housing. VA awards grants to private non-profit organizations and consumer cooperatives that assist very low-income Veterans and their families by providing a range of supportive services designed to promote housing stability.
QuickTime™ and a decompressor
are needed to see this picture. Housing Services OverviewHousing Services Overview

The challenge of keeping homeless people in housing
• High rate of recidivism from grant per diem housing
• Substance abuse relapse is the most commonly cited reason
– Chart review of 50 “early departure” veterans found secondary reasons of pain management, untreated mental illnesses, and relationship problems involved
– Participation in a Homeless-Oriented Primary Care model (Providence VA) reduced GPD “early departure” rate to 16%
Used with permission from Dr. O’Toole, from HPACT Cyberseminar
QuickTime™ and a decompressor
are needed to see this picture. Housing Services OverviewHousing Services Overview

Health impact of homelessness
Barrow SM, Herman DB, Córdova P, Struening EL. Mortality among homeless shelter residents in New York City. Am J Public Health. 1999 Apr;89(4):529-34
1260 NYC homeless Shelter residents

Health impact of homelessness
Barrow SM, Herman DB, Córdova P, Struening EL. Mortality among homeless shelter residents in New York City. Am J Public Health. 1999 Apr;89(4):529-34
In a 7 year follow up period~2-4x increased risk of mortality

Years of potential life lost3-3.5x to matched controls

BMJ 2009, Oct 26;339

• Large, nationwide, prospective, register-based cohort study 1999-2009 in Demark
• 32,711 in study population• Overall SMR (Standardized Mortality Ratio) 5-6x in Men, 6-7x in WomenHighest in Substance abuse disorder, higher than dual
diagnosis Nielsen SF, Hjorthøj CR, Erlangsen A, Nordentoft M. Psychiatric disorders and mortality among people in homeless shelters in Denmark: a nationwide register-based cohort study. Lancet. 2011 Jun 25;377(9784):2205-14

• Boston Health Care for the Homeless: Case control study of 558 deaths 1988-1993

Homeless Vulnerability Index• For individuals who have been homeless for at least six months, one or more following
markers place them at heightened risk of mortality:– more than three hospitalizations or emergency room visits in a year – more than three emergency room visits in the previous three months – aged 60 or older – cirrhosis of the liver– end-stage renal disease – history of frostbite, immersion foot, or hypothermia – HIV+/AIDS – tri-morbidity: co-occurring psychiatric, substance abuse, and chronic medical
condition
In Boston, 40% of those with these conditions died prematurely, underscoring the need for housing and appropriate support for this group.
Developed by Jim O’Connell, Boston Health Care for the Homeless used in practice by Common Ground, NYC

Salit SA, Kuhn EM, Hartz AJ, Vu JM, Mosso AL. Hospitalization costs associated with homelessness in New York City. N Engl J Med 1998; 338: 1734-1740
•Hospital discharge data from public hospital system of NYC 1992-1993, and private hospital data of medicaid admissions
•Of 354,494 persons discharges, identified 18,864 patients as homeless

Salit SA, Kuhn EM, Hartz AJ, Vu JM, Mosso AL. Hospitalization costs associated with homelessness in New York City. N Engl J Med 1998; 338: 1734-1740

Salit SA, Kuhn EM, Hartz AJ, Vu JM, Mosso AL. Hospitalization costs associated with homelessness in New York City. N Engl J Med 1998; 338: 1734-1740
•Average LOS 3.1 -5.1 days longer
•∆Cost in 1997 $s $4094 per dischargefor psychiatric primary diagnosis
$3370 per pt with AIDS as primary diagnosis
$2414 per pt of all causes~rough cost of monthly NYC apt

3x
$$x
Courtesy O’Toole, VA Providence Data

VERA Sustainability Capacity• New Multiple Medical and Chronic Mental Illness classes
specifically for homeless Veterans• Homelessness diagnosis (V.60) in combination with medical
conditions managed utilizing at least 7 RVUs qualify for Class 5 Price Group (Multiple Problems) VERA
• No RVU credit for ER or inpatient encounters• Price Group Differential:
– Non-reliant care: $813 – Multiple Problem care: $27,686

Ku BS, Scott KC, Kertesz SG, Pitts SR. Factors associated with use of urban emergency departments by the U.S. homeless population. Public Health Rep. 2010 May-Jun;125(3):398-405


“First Stops” when becoming homeless
• Community-based survey of 230 homeless adults• Question: “Where do you go first after becoming homeless
and for what?”• Top 5 sites:
– Soup kitchen– Welfare office– Detox center– Homeless outreach team– Emergency Department
• 62.6% of individuals with a chronic medical/mental health condition went to a health care site
• 46.4% of individuals with alcohol abuse went to a health care site
O’Toole, et al. Health Soc Care Community. 2007

Physical health concerns, homelessness and behavior change
• N=370 adults presenting to an emergency department (266 homeless; 104 housed)
• 80% of homeless adults seeking substance abuse treatment reported physical health concerns as a major reason.
• More homeless were in an action stage for wanting substance abuse treatment
• Homeless adults were almost 2.5 times more likely to report their living arrangement as a major motivation for seeking treatment
O’Toole et al. JSAT.
2008

“I’m just a doctor, how can I fix this?”

“The painfully obvious lesson for me has been the futility of solving this complex social problem solely with new approaches to medical or mental health
care...I dream of writing a prescription for an apartment, a studio, an SRO, or any safe housing
program, good for one month, with 12 refills.”
-Dr. Jim O’ConnellBoston Health Carefor the Homeless

•Large Health Survey 1999 with N=559,985•Serious mental illnesses (schizophrenia, bipolar d/o) is associated with lower utilization of primary care.

Co-located Primary Care?
Adm Policy Ment Health. 2009 Jul;36(4):255-64. Epub 2009 Mar 12.
In Los Angeles VA, usual VA care (n=130) vs. integrated care group (n=130), received more prevention services, primary care visits, fewer ED visits, but no difference in inpatient utilization or health status at 18 months.

December 2010, Vol 100, No. 12 | American Journal of Public Health O’Toole et al. | Peer Reviewed | Research and Practice | 2493
•Providence VA System
• retrospective cohort study of 177 Vets in Specialized homeless-oriented primary clinic (79) vs. traditional primary care Model (98)





Why a PACT model?

TODAY’S CARE MEDICAL HOME CARE
My patients are those who make appointments to see me
Our patients are those who are registered in our medical home
Patients’ chief complaints or reasons for visit determines care
We systematically assess all our patients’ health needs to plan care
Care is determined by today’s problem and time available today
Care is determined by a proactive plan to meet patient needs without visits
Care varies by scheduled time and memory or skill of the doctor
Care is standardized according to evidence-based guidelines
Patients are responsible for coordinating their own care
A prepared team of professionals coordinates all patients’ care
I know I deliver high quality care because I’m well trained
We measure our quality and make rapid changes to improve it
It’s up to the patient to tell us what happened to them
We track tests & consultations, and follow-up after ED & hospital
Clinic operations center on meeting the doctor’s needs
A multidisciplinary team works at the top of our licenses to serve patients
Acute care is delivered in the next available appointment and walk-ins
Acute care is delivered by open access and non-visit contacts
Used with Permission; Daniel Duffy, MD, MACP, School of Community Medicine, Tulsa, Oklahoma.

7 Core elements of Patient Aligned Care Teams
• Patient-driven – focus on the patient rather than the disease
• Team-based - care delivered by interdisciplinary team • Efficient – deliver care the patient needs when they need it
• Comprehensive – delivering while person-oriented care
• Continuous – long-term, longitudinal relationship between pt & team
• Communication – honest, respectful, reliable, culturally sensitive
• Coordination – across all elements of the health care system
Used with permission from Dr. O’Toole, from HPACT Cyberseminar

Key features of Special Population PACTs
• Access - Accommodates barriers, challenges to routine care
• Care tailored to specific needs of a population– Readiness to respond to “treatable moments”
• Case management/Care coordination– Expanded team members/communities– Capacity to address competing needs
• Care team equipped with specialized knowledge and skills
O’Toole, et al. Journal Gen Intern Med 2011
Used with permission from Dr. O’Toole, from HPACT Cyberseminar

Homeless PACT goals: PACT-PLUS
• To provide comprehensive, continuity care to a population of patients (Homeless Veterans) who have multiple deferred care needs complicated by their living arrangements
• To integrate housing objectives with clinical care objectives in care planning and delivery
• To build knowledgeable compassionate teams equipped and prepared to provide care needed by this population of patients
Used with permission from Dr. O’Toole, from HPACT Cyberseminar