Embed Size (px)
Citation preview

HYBRID APPLIANCES
Dr Shafeeq rahman

CONTENTSINTRODUCTIONCOMPONENTS OF APPLIANCESAPPLIANCES AND MODIFICATIONS HYBRID FUNCTIONAL APPLIANCES
Activator and its modifications
Frankel hybrid appliances
BASS appliance system HYBRID FIXED APPLIANCES
Herbst appliances
Churro jumper
Jasper jumper
Twin force bite corrector – double lockCONCLUSION

INTRODUCTION
• The orthodontists job is to fit together the pieces of the human craniofacial complex puzzle. • The expected outcome of this endeavor is a harmonious re-
arrangement that is not only functional, but also esthetically pleasing. • Highly sophisticated technologies from the fields of imaging,
computer graphics, robotics, computational analysis and database management are paving their way into the specialty. • Over the years, for convenience and efficiency, the specialty has
embraced various prefabricated and modified hybrid appliances.

It Implies an understanding of :
• Craniofacial Biology
• The cause of malocclusion
• The specific adaptation response to each named appliances.
•Clearly all appliances are capable of producing some changes with proper diagnostic objectivity .
•The clinician can take advantage of the best parts of the appliance.

Hybrid appliances: A component approach to dentofacial orthopedics Peter S. Vig, B.D.S., Ph.D., D. Orth., F.D.S.R.C.S.(Eng.), and Katherine W. L. Vig, B.D.S., D. Orth., F.D.S.R.C.S.(Eng.)
• Hybrid appliances are specifically customized to exploit the natural processes of growth and development. • Currently there are various “named” hybrid appliances introduced in the
market used to treat the same type of malocclusion, but their treatment approaches vary mainly due to difference in philosophies and/ or modifications from a previous appliance such as hybrid functional appliances.• Vig and Vig, had introduced ‘Component Approach’ of selecting the
components and their assemblies, resulting in appliance designs that uniquely match the needs of individual patients.• Such an approach represents a departure from the practice of adopting a
“named” appliance for the treatment of a malocclusion.

Components
• Functional appliances are no different. • All of the currently used appliances are made up in various
combinations from three basic functional components.
• These components produce basal and dentoalveolar changes by acting on the following:
1.Eruption (biteplanes)
2.Linguofacial muscle balance (shields or screens)
3.Mandibular repositioning (construction or working bite)

Eruption: Biteplanes
• Biteplanes may be flat or inclined, and anterior or
posterior, which contact single or multiple dental
units; although they are usually thought of as blocks
of acrylic resin, they may in fact be made of wire or
any other suitable material.
• Clinical experience supported by recent research
indicates that relatively low forces, if applied either
continuously or intermittently, are capable of
impeding the eruption of teeth

• A flat anterior bite plane of sufficient dimensions to disocclude the posterior teeth may be expected to have several effects.• These effects may comprise some or all of the following:
1. Differential eruption of posterior teeth 2. Non-eruption, relative or absolute intrusion of incisors 3. Incisor overbite reduction 4. Disocclusion with removal of intercuspation

Linguofacial muscle balance: Shields or screens
• Although certain elements still require experimental validation, there is little doubt that the growing dentoalveolar structures are plastic and responsive to linguofacial muscle pressures. • The so-called equilibrium theory of tooth position predicts that over
time tooth movement occurs in response to any perturbation of the homeostatic relationship between the radially directed forces of the tongue and the opposing, but smaller, forces exerted by the circumoral muscles of the lips and cheeks

Mandibular repositioning: Construction or working bite
• All of the functional appliances are constructed to a "construction" or "working" bite registration. • Such registrations of maxilla-mandibular relationships are based on
the assumption that by displacing the mandible from its rest position, and thus stretching the muscles attached to it, reflex activity tends to restore the mandible to a postural position that was originally determined by the unstretched muscles.

Modifications of activator
The bow activator of A.M. Schwarz:
•The bow activator is a horizontally split activator having a maxillary portion and a mandibular portion connected together by an elastic bow.
• This kind of modification allows stepwise sagittal advancement of the mandible by adjustment of the bow. In addition this design allows certain amount of transverse mobility of the mandible.
•The independent maxillary and the mandibular portions can have screw incorporated to allow arch expansions.

Wunderer’s modification:
• Used in treatment of Class III malocclusion.
• This type of activator is characterized by maxillary and mandibular portions connected by an anterior screw.
• By opening the screw the maxillary portion is moved anteriorly, with a reciprocal backward thrust on the mandibular portion.

• This modification of the activator is proposed by Professor G.P.F. Schmuth.
• This appliance resembles a bionator with the acrylic portion of the activator reduced from the maxillary anterior area leaving a small flange of acrylic on the palatal slopes.
• The two halves may be connected by an omega shaped palatal wire similar to bionator.
The reduced activator of cybernator of Schmuth:

The propulsor:
•Designed by Muhlemann and refined by Hotz.
•This appliance can be said to be a hybrid appliance that combines the features of both the monobloc and the oral screen.
•The propulsor is devoid of any wire components and consists of acrylic that covers the maxillary buccal portion like an oral screen.
• This acrylic portion extends into the inter occlusal area and also as a lingual flange that helps position the mandible forward.

Cutout or palate free activator:
•This is a modification proposed by Metzelder to combine the advantages of bionator and the Andersen’s activator.
•The mandibular portion of the appliance resembles an activator while the maxillary portion has acrylic covering only the palatal aspect the buccal teeth and a small part of the adjoining gingiva.
•The palate thus remains free of acrylic thereby making the appliance more convenient for patients to wear the appliance for longer hours.
•According to Dr Klaws Metzelder the appliance is excellent in mandibular positioning in TMJ dysfunction cases.

The Karwetzky modification:
•This consists of maxillary and mandibular plates joined by a U’ bow in the region of the first permanent molar.
•The maxillary and mandibular plates not only cover the lingual tissues and lingual aspects of teeth, it also extends over the occlusal aspect of all teeth.
•This type of activator allows stepwise advancement of the mandible by adjustment of the U loop.
•The U loop has a larger and a shorter arm. Based on their placement pattern we can have three types of Karwetzky activators.

Type I: Used in the treatment of Class II division I. Here the larger lower leg is placed posteriorly. Thus when the two arms of the U bow are squeezed the
lower plate moves sagitally forwards.
Type II: This is used for the treatment of Class III malocclusion. In this appliance the larger lower leg is placed anteriorly. Thus when the U bow is squeezed the mandibular plate moves distally.
Type III: They are used in bringing about asymmetric advancement of the mandible. The U bow is attached anteriorly on one side and posteriorly on the other side to allow asymmetric sagital movement of the mandible.

Herren (L.S.U) activator
Herren modified the activator in 2 ways:
1. By over compensating the ventral position of the mandible in the construction wax bite.
2. By seating the appliance firmly against the maxillary dental arch by means of clasps (arrowhead, triangular or Jackson’s)

• The construction bite is taken in a strong mandibular protrusion.
• This advanced position of the mandible causes the retractor muscles to try to bring the mandible back to original position.
• This causes a backwardly directed force on upper teeth and mesially directed force on lower teeth.
• According to Herren, with every 1 mm increase of forward position of the mandible, the sagittal force on the jaws will increase by 100 gm. The amount of forward positioning of the mandible is 3-4 mm beyond the neutral occlusion i.e. in case of Class II molar relation the mandible is brought forward to Class I molar plus an additional 3-4 mm forward. A vertical opening of 2-4 mm is recommended.

Vig designed an appliance for the treatment of patients with the following problems
Sagittal mandibular deficiency
Increase overjet and overbite
Bilateral cross bite of mandibular posterior teeth.
lack of space for eruption of second premolars
FRANKEL HYBRID APPLIANCE (AJO 1986)
Components
• Mandibular component has the features of frankle 2 appliance(Lip pads, Buccal shields, lingual pad with wire resting on the Cingulum.)
• Maxillary portion has a bilateral posterior bite block.
Mode of action
• The maxillary bite blocks prevents vertical eruption and mesial and buccal movement of the upper posterior teeth.
• Lower buccal shields prevent processes from the buccal musculature hence the lower posterior teeth can erupt vertically and laterally under the influence of the tongue pressure.
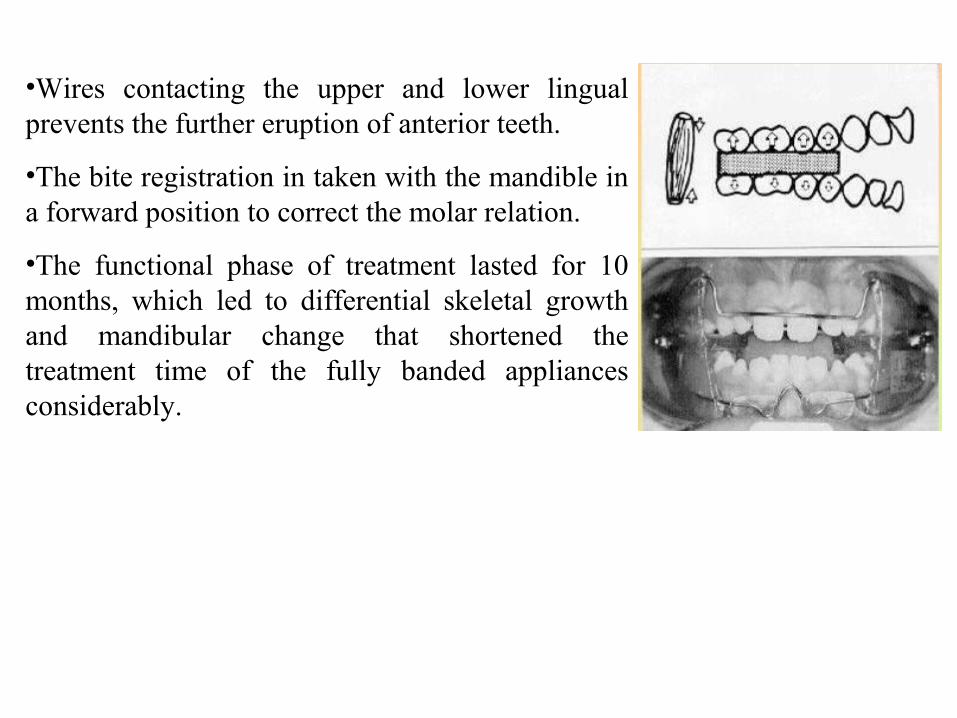
•Wires contacting the upper and lower lingual prevents the further eruption of anterior teeth.
•The bite registration in taken with the mandible in a forward position to correct the molar relation.
•The functional phase of treatment lasted for 10 months, which led to differential skeletal growth and mandibular change that shortened the treatment time of the fully banded appliances considerably.

Introduced by Neville Bass
•Used In growing patients with skeletal Class II malocclusion to optimize facial appearance and to rapidly and effectively correct the class II dental relationship.
Mode of action of Bass appliance
•A well secured maxillary splint assures control of the upper arch.• The anterior torqueing spring prevents tipping and produces bodily movement of the incisors.
THE BASS APPLIANCE SYSTEM (JCO 1987)

•The maxillary arch is expanded with a Jackscrew or spring to prevent cross bite and allow more space for dental alignment.
•The lingual pads helps to hold the mandibular incisors in a protrusive position, the pads are progressively reactivated every 6-8 weeks as the mandible develops forward.
•A rigid face bow connected to a high full headgear is used to retard maxillary growth and control vertical development of the maxillary dentition.
•Buccal screens are used to improve the soft tissue environment of the developing dentition.

Advantages
•Facial features are harmonized with good chin position.
•Balance and function of orofacial musculature is improved.
•Flattening of upper lip from retraction is avoided.
•The orthopedic phase last only 6-10 months.
•Speech quickly returns to normal ,there is no wire or acrylic lingual to the lower incisors
•There are little chances of breakage.

Designed by – Mickey Judras.
•Used for treatment of Class II malocclusion in the mixed dentition period.
Components
•Two molar bands with lingual attachments
•Connecting wire (0.040) from molar bands.
•Anterior bite plate.
•Incisal ramp
RICK – A – NATOR APPLIANCE

• The Rick – A – Nator in a very simple appliance which consists for 2 molar bands, Ist molar bands attached to an anterior bite plate.
• Initially to encourage patient compliance, the anterior bite plate is flat for one month.
• Next month the anterior bite plate places the incisor forward by the addition of an incisal ramp.
• The incisal ramp encourages the mandible to come forward which corrects the Class II molar relationship to class I and eliminates the overjet.

•ACTIVATOR HEADGEAR TREATMENT
•Head gear and activator have both been used effectively for
the treatment of Class II malocclusion.
•Hypothetically a simultaneous application of both appliances may result in number of desirable treatment effects greater than those induced by each appliance.

These changes believed to be are:
•Restraining the maxillary growth.
•Selective guidance of maxillary and mandibular dentoalveolar development.
•Some influence on mandibular growth or position.
Indications
•Adolescent patients with class II div 2 Molars.
•Preferably well formed dental arches although an abnormal arch shape or dental crowing in not necessarily contra indicated.

• Maxillary prognathism, mandibular retrognathism and decrease or increase facial height as treated differentially by varying the design and application of the appliance.
• The cervical headgear is claimed to be the most effective type of headgear for initiating an orthopedic displacement of the maxilla.
• Pfeiefer and Grobiky (Ajo 1982) preferred the use of cervical hesdgear.
• Teuscher (Ajo 1978) Recommended the use of activator and high pull headgear as means of inducing vertical land sagittal maxillary displacement, achieving auto rotation and increase forward displacement of the mandible

• In The correction of large sagittal discrepancies between maxilla and mandible, the orthopedic effect of treatment is often of small magnitude when compared with the dentoalveolar changes.
• A considerable amount of orthopedic improvement is needed in patient with large sagittal discrepancies between the maxilla and the mandibular in order to accomplish a stable, esthetically and functionally satisfactory treatment result.
HEADGEAR – HERBST APPLIANCE

• The appliances is constructed with cast splint banded to the lower arch and with bands on the upper perm Ist molar.
• The bands were linked with a palatal bar and connected to the lower splint with Herbst Telescopic arms, constantly keeping the mandible in a forward jump position.
• Addition, a plate was constructed in the jaw as an anchorage for a Headgear to be worn 12-14 a day.
• Lenant (Ajo-1993) found that prolonged retention period of over several years of activator wear was required.
• Albort oven used the functional regulator with headgear for the treatment of vertical maxillary excess.
Long face syndrome is manifested primarily by excessive lower face height.
• This may result due to a number of reasons.
• Clockwise rotation of the mandible • High angle.• Narrow arches.• excessive exposure of maxillary teeth and gingiva.• Open bite.• Short ramus.
FUNCTIONAL REGULATOR WITH HEADGEAR (Jco 85)

• The appliances consists of a regular headgear tubes to accept a face bow of a high pull headgear. The construction bite was 3-4mm protrusive, with 3-4mm inter maxillary clearance in the molar area.
• The appliance was worn 20 hours/day and the headgear 12 hrs/day, lip seal exercises are important for proper lipseal, treatment usually lasted for19 months.
Treatment of results
Maxillary skeletal – no change Maxillary dental – incisor tipped lingually Mandibular dental – no change Mandibular skeletal – chin moves forward. Vertical – changed towards Brachyfacial
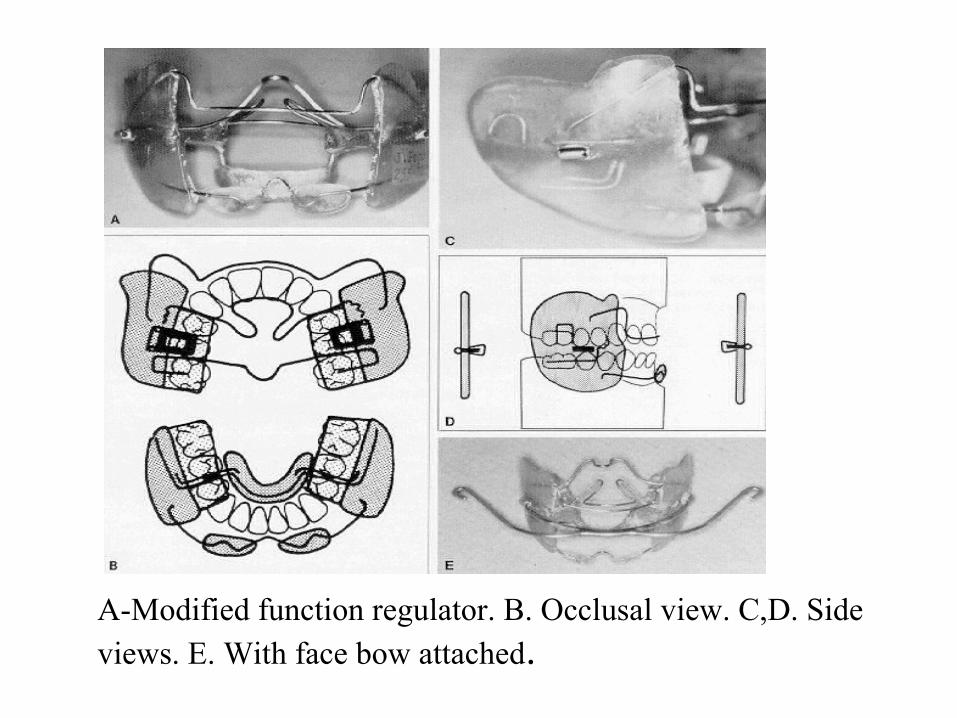
A-Modified function regulator. B. Occlusal view. C,D. Side views. E. With face bow attached.

• Robert Miller (1996) introduced this appliance which reduces the number of moving parts that can lead to breakage.
• It is easy to use and more comfortable for the patient than the conventional cantilever type Herbst.
• Instead of a screw attachment, it has a ball joint connector and it needs no retaining springs.
• To place the appliance, the maxillary sleeve attachments are fastened in a lock and key manner, after the crowns are cemented .
• The rods must be long enough so that they do not come out of the sleeves on maximum opening. They have forked ends that are crimped into the mandibular balls
FLIP LOCK HERBST APPLIANCE

• This appliance was designed to prevent accidental or intentional removal by the patient as often happens due to loose screws, but it can be removed at the chair with a loop forming plier.
• It is reactivated every six to eight weeks using 1-3 mm spilt bushing that are crimped on to the rods as needed.
• The molar tubes can be attached for fixed mechanotherapy.
• The flip lock Herbst can be combined with Jackscrew appliance.

Mandibular Advancement Locking Unit (MALU)
•The MALU consists of two tubes, two plungers, two upper “Mobee” hinges with brass pins, and two lower key hinges with brass pins.
•In the upper arch of the edgewise Herbst MALU appliance, only the Ist molars are banded, with 0.051” headgear tubes. A palatal arch can be used in cases of over expansion.
•In the lower arch, the Ist molars are banded and the anterior segment is bonded from cuspid to cuspid with 0.22” brackets. The bicuspids may be left un – bracketed to help in settling the occlusion.
MODIFIED EDGEWISE HERBST APPLIANCE

Maxillary MALU attachment with copper pin opening. B. Mandibular MALU attachment with archwire slot and copper pin opening.

by Ralph M. Clements and Alex Jacobson.
• The function of the MARS appliance is similar to that of the Herbst appliance. in that the mandible is maintained in a continuous protruded position via compressive struts.
• However there are several important differences between the two appliances.
THE MARS APPLIANCE

ADVANTAGES:
1. Requires neither soldering nor extensive laboratory procedures.
2. Has minimal incidence of breakage.
3.Does not depress the canines, open spaces in the premolar area, or flare mandibular incisors (provided the mandibular rectangular archwire is tied back to the terminal molars).
4.Is easily attached to or removed form the arch wire of a multi banded orthodontic appliance .
Appliance design
•The MARS appliance is composed of a pair of telescope struts, the ends are attached to the upper and lower arch wires of a multibonded fixed appliance by means of locking device
Each strut is composed of two separate parts; a piston or a plunger and a cylindrical or hollow tube.
These two components telescope together, forming an individual strut.
The free ends of the plunger and the hollow tube (strut) are attached to the upper and lower archwires by means of a slot and screw arrangement, which locks them securely in position on the arch wire.

Telescoping struts of MARS appliance. Locking screw is illustrated in
box at lower left-hand corner of diagram.

• The AVC consists of 2 posterior occlusal splints, one for the upper and one for the lower jaw.
• Samarium cobalt magnets are incorporated into the occlusal splints over the occlusal region of the teeth to be intruded.
• One magnet per distal quadrant is used.
• The magnets in the upper splints are incorporated in a mode to repel the magnets in the lower splints.
• Therefore the appliance is a combination of acrylic posterior bite blocks and repelling magnetic forces.
ACTIVE VERTICAL CORRECTOR

• To prevent unwanted cross bite development due to the shearing forces of repelling magnets ,angled buccal flanges are added to the lower occlusal splints to stabilize the appliance during lateral jaw movements.
• A heavy gauge stainless steel wire connects the occlusal splint of each arch.
• The magnets are cylindrical in shape with a diameter of 10mm.
• The magnets along with bite blocks measures 12mm in height.

• When the posteriors are intruded , auto rotation of the mandible take place and the mandible moves anteriorly to close the open bite.
• The AVC can be cemented or bonded.
• At end of 12 weeks the appliance can be removed and can be used as a removal appliance.

Fig. 2. Seated Active Vertical Corrector (AVC).

• The inclined plane mechanism plays an important part in determining the cuspal relationship of the teeth as they erupt into occlusion.
• Occlusal forces transmitted through the dentition provide a constant proprioceptive stimulus to influence the rate of growth and the trabecular structure of the supporting bone.
• The muscles are the prime movers that modify the bone growth to meet the demands of function via the proprioceptive feedback mechanism.
• When the appliance is removed at mealtime, the patient reverts to functioning with the mandible in a retrusive position.
TWIN BLOCK

• The strongest functional forces are applied to the dentition during mastication and the proprioceptive functional stimulus to growth is lost if the appliance is removed while eating.
• All the functional appliance that have evolved from the monobloc share the limitation that the upper and lower compartments are joined together. As a result, the patient cannot eat, speak of function normally with the appliance.
• Moreover, it is impossible for the patient to wear a single piece appliance full time.
• But the Twin Block appliance designed by William Clark (1989) can be worn for full time and it overcomes all the disadvantages of the other functional appliances.

Bite Registration
•In class II division I, a protrusive bite is registered to reduce the overjet and the disto–occlusion on average by 5-10 mm.
•The length of the patient’s protrusive path is determined by recording the overjet in centric occlusion and fully protrusive occlusion.
•The activation should not exceed 70% of the protrusive path.

• If there is an overjet of up to 10 mm , the bite may be activated edge to edge on the incisors with a 2 mm inter incisal clearance.
• This allows an overjet of up to 10 mm to be corrected on the first activation, without further activation of the Twin Blocks.
• Larger overjet invariably require partial correction , followed by reactivation after the initial correction is complete.
• Because the young patients commonly have a protrusive path of 13 mm and will tolerate activation up to 10 mm.
• Beyond this range the muscles and ligament cannot adapt to altered function.

• In the vertical dimension, a 2 mm inter incisal clearance is equivalent to an approximately 5 or 6 mm clearance in the I premolar region.
• This usually leaves 3 mm clearance distally in the molar region and ensures that the space is available for vertical development of posteriors to reduce the overbite.
• It is very important to open the bite slightly beyond the clearance of the freeway space to encourage the patient to close into the appliance, rather than to allow the mandible to drop out of contact into rest position, which is one of the disadvantages of making the blocks to thin.

The earliest Twin Blocks were designed with the following basic components;
1. A midline screw to expand the upper arch.
2. Occlusal bite blocks
3. delta Clasps on upper molars and premolars
4. Delta clasps on lower premolars (it is similar to the Adam’s clasp in principle ,but incorporates new features to improve retention, reduce metal fatigue and minimize the need for adjustment)

5. Ball end clasps on lower incisors (originally it was given on lower incisors, but it can be given only on the lower canines mesially, in mixed dentition, “C” clasps can be given on all deciduous molars)
6. Labial bow. (It should be passive. If retraction of upper incisors is done prematurely, it limits the scope for functional correction for mandibular advancement. Later the design was changed from labial bow to ball end clasps – in between upper canine and premolars.

HYBRID BITE JUMPING FUNCTIONAL APPLIANCE
• This appliance is a forward bite jumping appliance used in Skeletal Class II malocclusion which primarily induces condylar growth.• The appliance normalizes the growth pattern of the affected mandibular side to a
greater extent in younger children (3 – 7 years) than in older ones (11 years) and in mild to moderate cases rather than severe. • This appliances can be used for the treatment of hemifacial microsomia. • A study showed that low – intensity pulsed ultrasound (LIPUS) enhances
mandibular growth when combined with functional jaw orthopaedic appliances. • The treatment protocol included daily application of LIPUS for 20 minutes
along with a Hybrid Forward Bite Jumping Appliance. LIPUS application was performed for 8 − 12 months

• It can be used in all phases of treatment in the mixed or permanent dentition and with removable or fixed appliance.
• Like other mandibular protrusion appliances, the UBJ uses a telescopic mechanism, an active coil spring can be added if necessary.
• It can be used in Class II and III cases.
• the UBJ is attached to the maxillary Headgear tube with a ball pin.
• In the mandibular arch ,the sliding rods end in a 900 hook that is fixed to the each wire.
• Lower cantilever type of UBJ is also available when used with removable acrylic splints; two lateral UBJs link the maxillary molar areas and the mandibular Ist premolar areas.
THE UNIVERSAL BITE JUMPER

• They are attached to 1.2-mm ball clasps, which are constructed on the working cast and then incorporated into the thermoformed splints.
• The lower loop of the UBJ should be oriented in an antero-posterior direction.
• Re- activation is made every 6-8 weeks by crimping 2-4mm splint bushing on to the rods.
• UBJ with NiTi coil springs do not need to be activated.
• Adjusting one side or the other of the appliance can easily treat midline or asymmetrical problems.

HYBRID HYRAX APPLIANCE • Early Class III Treatment with a Hybrid Hyrax -
Mentoplate Combination: • Mentoplate approach for early Class III treatment
offers several advantages over other methods.• Such a combination produces direct force by the
Mentoplate or indirect by Hybrid Hyrax to skeletal structures. • Rapid expansion opens the midpalatal sutures for
better maxillary protraction. • Anchorage is stable and reliable with such an
appliance and no extra oral devices are required. • The placement procedure is less invasive than when
multiple miniplates are used. • The upper and lower arches remain fully accessible
for orthodontic tooth movement
The efficacy of Hybrid Hyrax-Mentoplate combination in early Class III treatment: a novel approach and pilot studyVandana Katyal,.Benedict Wilmes et al(Aust Orthod J 2016

EUREKA SPRING
• The Eureka Spring is a three part telescopic appliance fixed to the upper arch at the level of the molar band and to the lower arch distal to the cuspid. • The main component of the Eureka spring is an open
wound coil spring encased in plunger assembly.• It has esthetic acceptability because of its small size
and produces forces of only 140 - 170 grams at the points of attachment as compared to 220 - 280 grams of Jasper Jumper. • The appliance is universal and it can be applied to
both right and left side.
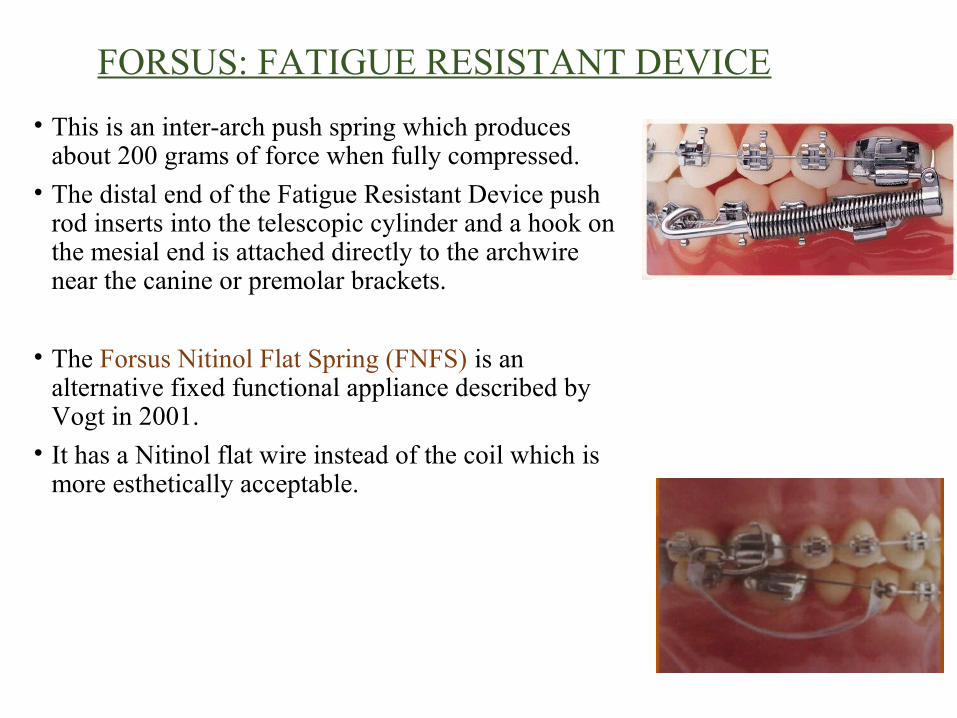
FORSUS: FATIGUE RESISTANT DEVICE
• This is an inter-arch push spring which produces about 200 grams of force when fully compressed.
• The distal end of the Fatigue Resistant Device push rod inserts into the telescopic cylinder and a hook on the mesial end is attached directly to the archwire near the canine or premolar brackets.
• The Forsus Nitinol Flat Spring (FNFS) is an alternative fixed functional appliance described by Vogt in 2001.
• It has a Nitinol flat wire instead of the coil which is more esthetically acceptable.

• Force levels remain constant from the initial setup to the time of removal. • The results are faster and more efficient.• More recently, the Forsus Fatigue - resistant Device (FRD) EZ
module was developed and has the advantage of ease of application onto molar band headgear tubes without additional implementation
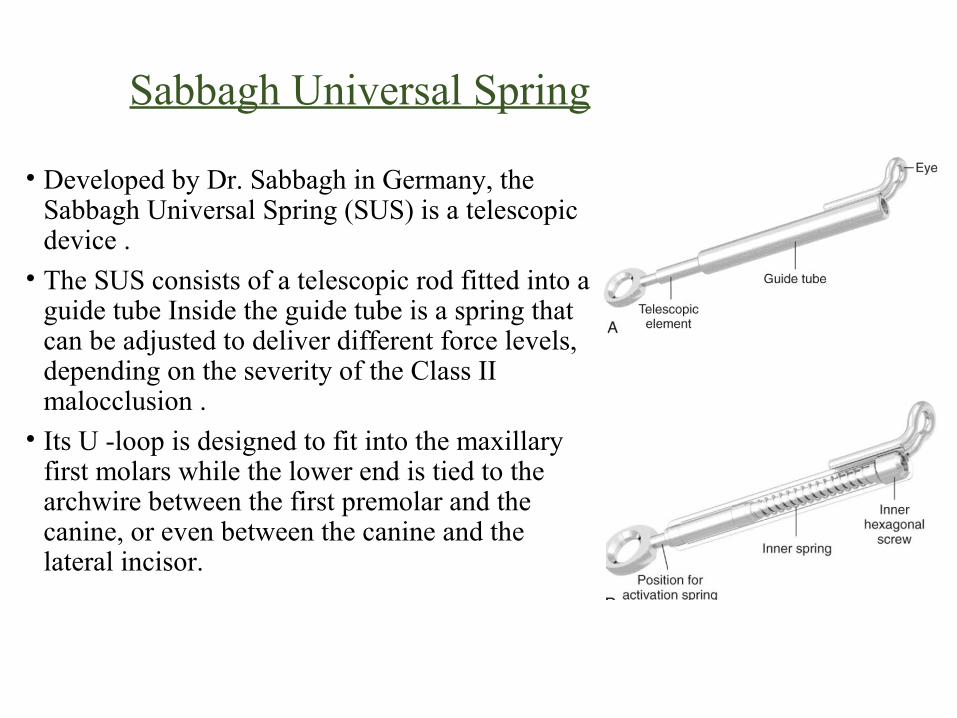
Sabbagh Universal Spring
• Developed by Dr. Sabbagh in Germany, the Sabbagh Universal Spring (SUS) is a telescopic device .• The SUS consists of a telescopic rod fitted into a
guide tube Inside the guide tube is a spring that can be adjusted to deliver different force levels, depending on the severity of the Class II malocclusion .• Its U -loop is designed to fit into the maxillary
first molars while the lower end is tied to the archwire between the first premolar and the canine, or even between the canine and the lateral incisor.

THE CALIBRATED FORCE MODULE AND ALPERN CLASS II CLOSERS
• These appliances substitute Class II elastics, applied to the inferior arch close to the molars and fixed by a screw, and mesial or distal to upper cuspids, and also fixed to the arch. Its coil spring produced a force between 150 and 200 grams. • The system generated tooth movement by
employing gentle and continuous force 24 hours a day

TWIN FORCE BITE CORRECTOR – DOUBLE LOCK:
• It is based on the system of lock-on screws. This new version facilitates the use of the appliance for Class III correction and it allows for a slightly better control of the force.

FIRST CLASS HYBRID MOLAR DISTALIZATION APPLIANCE
• It is a combination of rigid buccally and flexible palatally positioned distalization force system. It has vestibular and palatal components.• It produces rapid distalization of the maxillary first and second molars even
when the second molars have completely erupted

HYBRID MANDIBULAR ANTERIOR POSITIONING APPLIANCES FOR OBSTRUCTIVE SLEEP APNEAS
• Obstructive sleep apnea - hypopnea syndrome (OSAHS) is characterized by recurrent upper airway obstruction during sleep.• Oral appliances (OAs) provided effective and safe
long - term therapy for patients with OSAHS. • Follow-up is recommended since long - term
alterations take place, although these appear to be minimal.• these appliances hold the lower jaw forward and
open, preventing the tongue and throat tissues from collapsing the critical airway.• These appliances reduce sleep apnea associated health
risks without the need for surgery, medications, or other therapies. various appliances are:

Appliances for OSA
• SILENT NITE
SOMNOMED MAS NARVAL APPLIANCE MOSES APPLIANCE
OASYS ORAL/ NASAL AIRWAY SYSTEM

HYBRID ORTHODONTIC TREATMENT SYSTEM (HOTS): • Ikegami et al introduced an innovative method in first premolar
extraction cases.• COMPONENTS:
• Miniscrew, • Dual-dimension wires ,• Multiloop Edgewise Archwires (MEAW). • The insertion of miniscrews allowed the maxillary canines to be
retracted along the canine curvature with the round portion of the DDW (Dual-dimension Wire), along with simultaneous retraction the four incisors with the rectangular portion controlling their torque. • In the finishing stage, after the closure of the extraction space,
MEAW is used to further fine-tune the overjet, overbite, and posterior occlusal relationship.

HYBRID DISTRACTOR• It is a combined bone borne and tooth borne mandibular symphysis
distraction device. • The hybrid distractor is secured by two mandibular bone screws and
bonded circumdental wires on the mandibular canines or premolars.• These appliances vary in patient acceptance, cost, invasiveness and
patient comfort. • The skeletal component of the total expansion achieved was greater in
the hybrid distractor device as compared to other two devices. • During distraction, the hybrid distractor effected more parallel
expansion of basal and alveolar bone than the tooth borne distractor

HYBRID AESTHETIC FUNCTIONAL APPLIANCE (HAF):
• HAF appliance is intended to integrate aesthetics in functional orthodontic therapy. • It is of double plate design consisting of
thermoplastic and acrylic parts. The upper component is a vacuum formed plate, made of transparent hard polyethylene sheet with 2 mm thickness, equipped with an acrylic advancement bar positioned in the anterior midpalatal region.

• Similarly, the lower plate is constructed by thermoplastic material of the same width. • An acrylic guidance surface is placed over the plastic coverage on the
lingual surfaces of lower incisors and canines, aimed to fit the upper bar.• The posterior teeth are intentionally exposed to facilitate eruption
and leveling of a deep curve of Spee. • This appliance meets both the therapeutic as well as aesthetic
demands of young age groups

BIOBLOC ORTHOTROPICS• It a method of facial growth guidance which changes unfavorable vertical
growth to more favorable horizontal growth often resulting in corrections similar to those that result from successful Orthognathic surgery.• Biobloc appliance is another treatment modality for correction of Class II
malocclusion and have different effects compared to functional appliances. • It aims to redirect jaw growth anteriorly in a more horizontal direction so
that a better oral posture and soft tissue facial profile can be developed.• The Biobloc technique involves both the orthopedic and functional
elements

QUICK STRAIGHT TEETH
• It is the latest invisible technology that provides a very discrete and comfortable way to quickly align teeth with excellent results that can even be seen as quickly as 4 - 16 weeks.• The treatment involves a programme of 5 transparent removable
appliances that can be used singularly or in a combination to deliver the desired results to the patient:

This appliance is called the Q100 and is a individually crafted clear/invisible removable tray that will gently and gradually aligns your teeth.
The main difference being is that it has an added powerchain on the front of the tray. This powerchain is made out of elastic and is also clear like the tray
This is the flagship appliance in this systems range. All the best features from the range have been used to create the Q500. As well as having the powerchain, it also has the Q spring that focuses on aligning the front teeth forward

This is a hybrid of the Q500 appliance. The biggest difference with the Q300 is the use of a Adams clasp. The Adams clasp is used for retention and works by clipping onto the undercuts of a molar/premolar tooth. The reason behind this slight alteration is because in some cases your clinician may want your occlusal surfaces (the surface that touches the opposing tooth in your jaw) to not be covered.
This appliance is again a slight variation of the Q500 (another hybrid). The main difference added on to this device is the molar bands which are used for retention. In some cases patients may want the Q500 but may not be a suitable candidate for them. This was developed for those patients so they can still experience the benefits of the Q500.

• The aim of this study was to evaluate the effects of the headgear activator (HGA) and Herbst appliance during active treatment and retention and at follow-up in children with a skeletal Class II malocclusion.
• there were no signifi cant overall changes at follow-up except for the prognathism, i.e. maxillary prognathism decreased with treatment with the HGA while mandibulars prognathism continued to increase with HAA treatment.

CONCLUSION
•Hybrid functional appliances form an useful addition to the clinician’s orthodontic armamentarium. • But many of these appliances need further studies to
substantiate the claims made by their respective originators. With this in mind, clinicians must take great care in selecting the right patient and also pay attention to every detail in the manipulation to attain successful results with these appliances





























