Embed Size (px)
DESCRIPTION
imaging US in graft kidneys. It may be helpful in many conditions and it is safe and non invasive.
Citation preview

IMAGING OF Tx. KIDNEY

• First successful transplant 1954.• 2 years survival rate > 90 %• Eligible patients are those with ESRD &dialysis
dependent.• Common causes:• Glomerulo &pylonephritis.• Diabetic nephropathy.• PCKD.




Sonography of Normal Graft
• High-resolution colour Doppler imaging (CDI) with pulsed Doppler (PD) capability is required.• Quick & safe.• Non – invasive. • No intravenous contrast. • No ionizing radiation.

Gray Scale assess :• The normal renal transplant is easily
visualized in Rt. or LIF lying anterior to the external iliac artery and vein.
• Parenchymal echogenicity.• Definition of the cortico/medullary
junction, collecting system, surrounding soft tissues and estimation of graft volume .

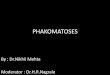
Transverse colour Doppler image of a normal renal allograft showing its normal position anterior to the external iliac vessels .

• The renal cortex is readily distinguished from the more echo-poor medulla.
• The renal sinus is normally hyperechoic in the absence of hydronephrosis.
• Small amount of fluid is often seen within the renal pelvis in the immediate postoperative period.
• volume is calculated using ellipsoid formula (0.5 x long x transverse x AP dimensions). • Small perigraft fluid collection is common; mostly
hematomas which resolve spontaneously

Sagittal scan of a normal transplant. Echopoor medullary pyramids , bright renal cortex.

Doppler Imaging
• CDI has revolutionized the evaluation of the renal transplant, allowing assessment of renal arterial perfusion and venous patency.
• Show RA anterior and posterior divisions, segmental interlobar, and arcuate arteries and corresponding veins within the graft .
• CDI is useful in differentiating prominent renal vessels from mild pelvicaliectasis which may occur as a consequence of edema at the ureteral anastomosis.


• Tx .has low arterial vascular bed resistance characterized by streamlined systolic flow and continuous forward diastolic flow .
• Normal main RA velocity is 20 - 52 cm/sec with a mean of 32 cm/sec .
• The Resistivity Index (RI) measures the resistance to arterial flow within the renal vascular bed calculated from the PD arterial waveform .
• An RI < 0.7-0.8 is considered normal , RI > 0.9 is a strong indicator of transplant dysfunction, < o.6 indicates hypo perfusion as in RAS



Causes of Elevated Resistive Index

inevitable questions in Renal Graft
1. Is there a treatable renal or extrinsic cause?
2. Is immediate medical or surgical therapy required to save the graft?
3. Is a renal biopsy required for diagnosis?

Renal Transplant Complications

Parenchymal Complications 1- Acute Tubular Necrosis (ATN)• ATN occurs in 60% of cadaveric grafts ,the most frequent complication in the
first 48 hours P.O.• ATN is due to reversible ischemic damage to the renal tubular cells prior to
engraftment. Risk factors include:1- Cadaveric graft 2- Hypotension in the donor prior to implantation (aggravated by the use of diuretics or vasoconstrictors to maintain urine output or blood pressure) 3- Long warm (over 30 minutes) and cold (over 24 hours)ischemic times. • ATN can cause severe graft dysfunction , it is usually fully reversible with only
supportive therapy. • Short-term dialysis may be required in severe cases.

U/S in ATN is quite variable . - The Tx. may appear normal.- In severe cases Tx is enlarged, grossly edematous and echo poor with effaced renal
sinus & loss of normal C/M differentiation. - Tx. with severe ATN generally have elevated RIs > 0.8 but can be normal in first 24 hours.

ATN with preserved C/M differentiation is. RI 0.88.

Rejection
• Allograft rejection is either of antibody (humoral) or cellular rejection (lymphocytes)
• Antibody-mediated rejection always involves blood vessels (vascular rejection)
• Rejection occurring within the first month PO is either acute rejection (AR) or accelerated acute rejection (AAR).
• Chronic rejection (CR) is an insidious process developing months to years PO.

Acute Rejection (AR):• Common, in 30% of cadaveric grafts. • It is important event determining the short (1 year)
and long-term (5 year) graft survival.• Is successfully treated in over 80% of cases using
selective pulsed intravenous corticosteroids --Cs-A, and the monoclonal antibody OKT3 reducing the clinical triad of a tender swollen graft, fever and rising creatinine.
• Cs-A made AR indolent process commonly diagnosed by biopsy done for asymptomatic patient with rising creatinine .

• AR is characterized pathologically by lymphocytic and polymorphonuclear cell infiltrating the interstitium (tubular ) and/or vessel walls (vascular ).
• The more severe forms of vascular AR are associated with a higher incidence of graft loss.

Sonographic hallmarks of severe AR include:1. Graft enlargement due to edema 2. Decreased cortical echogenicity and swelling
resulting in loss of C/M differentiation & effaced renal sinus.
3. Acute rejection may be accompanied by edema of the P/C system wall and focal echo-poor areas (parenchymal infarction )and perigraft fluid due to necrosis and hemorrhage

Decreased cortical echogenicity and swelling of the medullary pyramids resulting in loss of C/M differentiation.

Edema within the renal sinus fat which effacing renal sinus echo complex.

Edema of the collecting system wall.

Focal echo-poor areas of parenchymal = infarction Perigraft fluid due to necrosis and hemorrhage.

- In severe cases, PD characteristically shows reduced, absent or reversed diastolic flow with elevation of the RI .- In mild cases US can be normal & biopsy needed.

Accelerated Acute Rejection (AAR):
• Typically occurs within the first postoperative week.• Is a combined cellular and humoral immune
response; low levels of circulating antibodies or pre sensitized T- lymphocytes thought to be responsible .
• Unusually severe form of rejection, presenting with oliguria and rapidly rising serum creatinine.
• The prognosis is poor with graft loss in 60% . • U/S findings same as AR and ATN.

Chronic Rejection (CR):
• Develops months to years after post engraftment due to accumulating antibodies following repeated episodes of AR resulting in progressive vascular compromise of the graft & decline in renal function.
• On U/S , graftis small with thin echogenic cortex and relative sparing of the medullary pyramids .
• The RI is typically normal or slightly elevated. • Biopsy is often required to exclude superimposed
and potentially treatable AR.

Chronic rejection.

Cyclosporine Toxicity• Direct nephrotoxic effect of high serum levels
of Cs-A. • Can occur at any time, mostly seen in the
second or third month PO when drug doses are titrated against clinical response.
• Diagnosis established with Tx. dysfunction with high Cs-A levels.
• Sonographic findings are nonspecific and frequently normal

Vascular Complications
• Renal Vein Thrombosis or Occlusion (RVT)
• Infrequent ,< 1 % but a surgical emergency. • Usually due to extrinsic compression or mobility of
graft, kinking of lengthy vein or surgical tech. problems @ anastomosis site.
• Patients present with oliguria or anuria and elevated creatinine in the immediate PO period.
• Early detection of RVT is critical to preserve graft function as the Tx lacks normal venous ,arterial collaterals & innervation found in native kidneys thus prone to venous infarction and rupture.

• Treatment is immediate surgical exploration, thrombolysis offered to poor operative candidates.
• U/S findings in RVT include enlarged kidney with absent venous flow on CDI or PD imaging .
• Thrombus in renal vein is diagnostic ,absence does not exclude the lesion.
• Prolonged plateau-like reversal arterial flow in diastole is characteristic of RVT , when seen in combination with absent renal venous flow on CDI .

Prolonged, plateau-like reversal of diastolic flow= RVT


RVT with reversal of flow in diastole.

Renal Artery Thrombosis (RAT)
• Due to technical problems at arterial anastomosis• Tx has no collateral arterial supply, irreversible injury
will result if the ischemic time exceeds 1.5 hours. • Patients present with anuria and hypertension.• If Doppler shows no arterial flow within Tx ,
angiography is indicated to confirm the presence of arterial thrombosis.
• Immediate surgery required when diagnosis established and nephrectomy is frequently necessary

Renal Artery Stenosis (RAS)
• RAS develops in 12% ,occurs within 1 cm of the anastomosis.
• Rising creatinine ,hypertension and a bruit over the graft suggests the diagnosis.
• Percutaneous angioplasty successful in opening the stenosis in > 90% of cases, with normalization of blood pressure in 75%.
• Ultrasound shows normal kidney morphology , CDI and PD shows high velocity jet exceeding peak flow in the iliac artery

High grade Tx renal artery stenosis. High velocity jet (4.95 m/s) + Aliasing and turbulent flow.

CD image RA stenosis shows colour aliasing (arrows) at the site of the jet.

Angiography demonstrated an 85% stenosis .

• Aliasing and perivascular colour assignment are seen in high-grade stenosis.
• A low RI 0.6 or less may be highly specific for stenosis • Reduction in pulse amplitude, delayed systolic
upstroke within the renal parenchyma (parvus-tardus phenomenon) are usually seen in significant RA stenosis .
• A systolic acceleration time waveform > 0.07 s should be considered strong evidence of a high-grade RAS.
• In spite of U/S findings, angiography must be performed to locate site of RAS .

Reduction in pulse amplitude & delayed systolic upstroke of renal artery stenosis.

Urologic Complications
• Urologic complications occur in10% of renal transplants .
• Early urologic complications are generally technical and usually result from inadequate blood supply to the lower pole of the kidney, or from an imperfect anastomosis between ureter and bladder

Urinary Fistula and Urinoma
• Leaks and fistulae occur in 2-5% of grafts and account for half of the urologic complications.
• Leaks typically present within 3 weeks of surgery at the ureterovesical junction as a consequence of ischemia and necrosis of the distal ureter due to vascular insufficiency.
• This complication is skill dependent ,can be minimized by keeping the transplant ureter short, avoid excessive dissection & stenting.

• Urine leaks ( urinary ascites or urinomas) manifest as cystic fluid collections in the pelvis separate from the bladder.
• Can enlarge rapidly, but generally do not have septations unless infected.
• Diagnosis can be established by ultrasound-guided needle aspiration revealing high creatinine level in the fluid.
• This distinguishes a urinoma from PO hematoma or lymphocele, the latter having a creatinine level comparable to serum.
• The exact site of leak is best delineated by antegrade pyelography .

. Urinoma : a technetium-99m mercaptoacetyltriglycine (MAG3) study show abnormal radionuclide activity around the transplant (arrows).

• Contrast leak at the distal ureteral anastomosis

Urinoma .

Ureteral Obstruction and Hydronephrosis
• Ureteral obstruction occurs in 6% of grafts. • Approximately 90% of obstructions occur at the
ureterovesical junction due to fibrosis induced by ischemia or rejection of the ureter.
• PO ureteral edema or blood clots and peritransplant fluid collections (lymphoceles, urinomas, hematomas, and abscesses) may obstruct the ureter.
• Renal calculi are rare in the transplant kidney, < 2% .• Only half of the 18% of patients developing
hydronephrosis are truly obstructed .

Dilatation confined to the renal pelvis in the early post operative period. NO OBSTRUCTION

Obstruction

Hydronephrosis secondary to a ureteral stone .

Hydronephrosis and a lower pole stone in Tx.

• The nephrostogram shows a second stone in the distal ureter above a tight stricture causing obstruction

• Antegrade pyelogram depicting distal ureteric stricture.

Tx. main renal vein mistaken for hydronephrosis.

CDI readily confirms that this is a vessel.

• The immediate treatment of choice for obstructive hydronephrosis is decompression by percutaneous nephrostomy.
• Ureteral strictures can be managed by percutaneous balloon dilatation and stenting, long-term stenting alone, or open repair .

Lymphocele
• Very common in Tx. population, occurring in 15% of patients, mostly associated with ureteral obstruction
• Most develop within one year of transplantation. • Risk factors include incomplete ligation of the pelvic
lymphatics or a prior episode of severe rejection.• Palpable mass, leg pain and edema and impaired graft
function due to compression of the ureter are the Pt. presentations.
• Diagnosis is confirmed by needle aspiration which shows a creatinine level equivalent to serum.
• Collections are heavily septated , large but usually grow slowly

Large septated lymphocele

• The majority of lymphoceles are asymptomatic, requiring no therapy.
• Treatment options for symptomatic non infected lymphoceles include open surgical drainage, percutaneous aspiration with or without injection of a sclerosing agent and laparoscopic marsupialization .

Aspiration

Procedure Related ComplicationsHemorrhage
• The complication rate for percutaneous biopsy of the renal graft is approximately 5-8%.
• Perinephric hematomas account for 25-30% of all complications.
• Most are small and do not require additional therapy, hematomas may occasionally compress the ureter and produce hydronephrosis & impaired renal function.

Sub capsular hematoma following percutaneous biopsy (*).

Arteriovenous Fistula (AVF)
• Occurs as a consequence of simultaneous laceration of a renal artery branch and an adjacent vein during biopsy.
• Occur in 18% of biopsied kidneys but are almost always small and asymptomatic.
• Observation is the rule ,most thrombose spontaneously
• Embolization is reserved for fistulae associated with hemodynamically significant AV shunting or recurrent hematuria.

AV fistulae features include:
• Focal colour aliasing within the nidus • Perivascular colour assignment at low flow
velocity settings due to tissue vibration artifact.
• The hallmarks of AV fistulae on PD include low resistance, high velocity arterial flow within the feeding artery and high velocity arterialized venous flow in the associated draining vein

Mosaic colour assignment due to Arteriovenous fistula (AVF).

Feeding artery (a) and vein (v) seen entering/leaving the nidus of an AVF (arrow).

High velocity, low resistance flow due to AVF

Pulsatile venous flow due to AVF

Pseudo aneurysm
• Rare and may occur as a consequence of renal biopsy, infection within the graft or dehiscence of the arterial anastomosis.
• Any cystic area developing in or adjacent to the graft on serial ultrasound studies should be interrogated with Doppler to exclude the presence of pseudo aneurysm.
• CDI shows a high velocity jet from the feeding artery with eddying of blood referred to as the Yin-Yang sign within the aneurysm cavity .

Colour Doppler of pseudo aneurysm. A high velocity jet from the feeding artery enters the aneurysm sac during systole.

CDI shows the eddying of blood within the sac during diastole ("Yin-Yang" sign).

• PD shows the jet, turbulent flow within the cavity and the classic biphasic flow pattern at the pseudo aneurysm neck .
• While most regress spontaneously treatment of symptomatic lesions is by embolization or surgical repair .

Biphasic flow at the neck of a pseudo aneurysm.