Embed Size (px)
Citation preview
Imaging in Constipation
Dr. Vishal Avinashi
Pediatric Gastroenterologist
BC Children’s Hospital

Objectives
• Review the criteria for diagnosing functional constipation
• Highlight the (limited) role for imaging in functional constipation
• Identify some tools in the literature that have been used for objectifying constipation
• Give some examples (including non evidence based) reasons for imaging as part of constipation evaluation

X Medical Expert (as Medical Experts, physicians integrate all of the CanMEDS Roles, applying
medical knowledge, clinical skills, and professional values in their provision of high-quality and
safe patient-centered care. Medical Expert is the central physician Role in the CanMEDS
Framework and defines the physician’s clinical scope of practice.)
Communicator (as Communicators, physicians form relationships with patients and their
families that facilitate the gathering and sharing of essential information for effective health
care.)
Collaborator (as Collaborators, physicians work effectively with other health care professionals
to provide safe, high-quality, patient-centred care.)
Leader (as Leaders, physicians engage with others to contribute to a vision of a high-quality
health care system and take responsibility for the delivery of excellent patient care through their
activities as clinicians, administrators, scholars, or teachers.)
X Health Advocate (as Health Advocates, physicians contribute their expertise and influence as
they work with communities or patient populations to improve health. They work with those they
serve to determine and understand needs, speak on behalf of others when required, and
support the mobilization of resources to effect change.)
X Scholar (as Scholars, physicians demonstrate a lifelong commitment to excellence in practice
through continuous learning and by teaching others, evaluating evidence, and contributing to
scholarship.)
Professional (as Professionals, physicians are committed to the health and well-being of
individual patients and society through ethical practice, high personal standards of
behaviour, accountability to the profession and society, physician-led regulation, and
maintenance of personal health.)
CanMEDS Roles Covered

No Disclosures

Key Article
Tabbers, M. M., C. Dilorenzo, et al. (2014). "Evaluation and Treatment of Functional Constipation in Infants and
Children: Evidence-Based Recommendations From ESPGHAN and NASPGHAN." J Pediatr Gastroenterol Nutr 58(2):
265-81.
Diagnosis of functional constipation
• “The diagnosis of functional constipation is based on history and physical examination.”
• Criteria like for all functional conditions comes from ‘ROME’ criteria


Hyams, J. S., C. Di Lorenzo, et al. (2016). "Functional Disorders: Children and Adolescents." Gastroenterology.

Diagnosis is by history and physical • Alarm signs and symptoms and
diagnostic clues should be used to identify an underlying disease responsible for the constipation

DDx beyond functional
Tabbers, M. M., C. Dilorenzo, et al. (2014). J Pediatr Gastroenterol Nutr 58(2): 265-81.


XRAYS are not a part of diagnostic criteria
• “The routine use of an abdominal radiograph to diagnose functional constipation is not indicated”
• “If only one Rome criterion is present and the diagnosis of FC is uncertain, a digital examination of the anorectum is recommended to confirm the diagnosis and exclude underlying medical conditions.”
• “A plain abdominal radiograph may be used in a child if fecal impaction is suspected but in whom physical examination is unreliable/not possible”

But…
• “In conclusion, evidence does not support the use of digital rectal examination to diagnose functional constipation.”
• “Demonstration of the presence of absence of fecal impaction has important therapeutic implications”

XRAY
• Not generally standardized reporting
• Some scoring systems described such as Barr or Leech or Blethyn
• But all rely on gold standard being clinical criteria
• Variable sensitivities / specificities

Barr, R. G., M. D. Levine, et al. (1979). "Chronic and occult stool retention: a clinical tool for its evaluation in
school-aged children." Clin Pediatr (Phila) 18(11): 674, 676, 677-9, passim.
Barr score
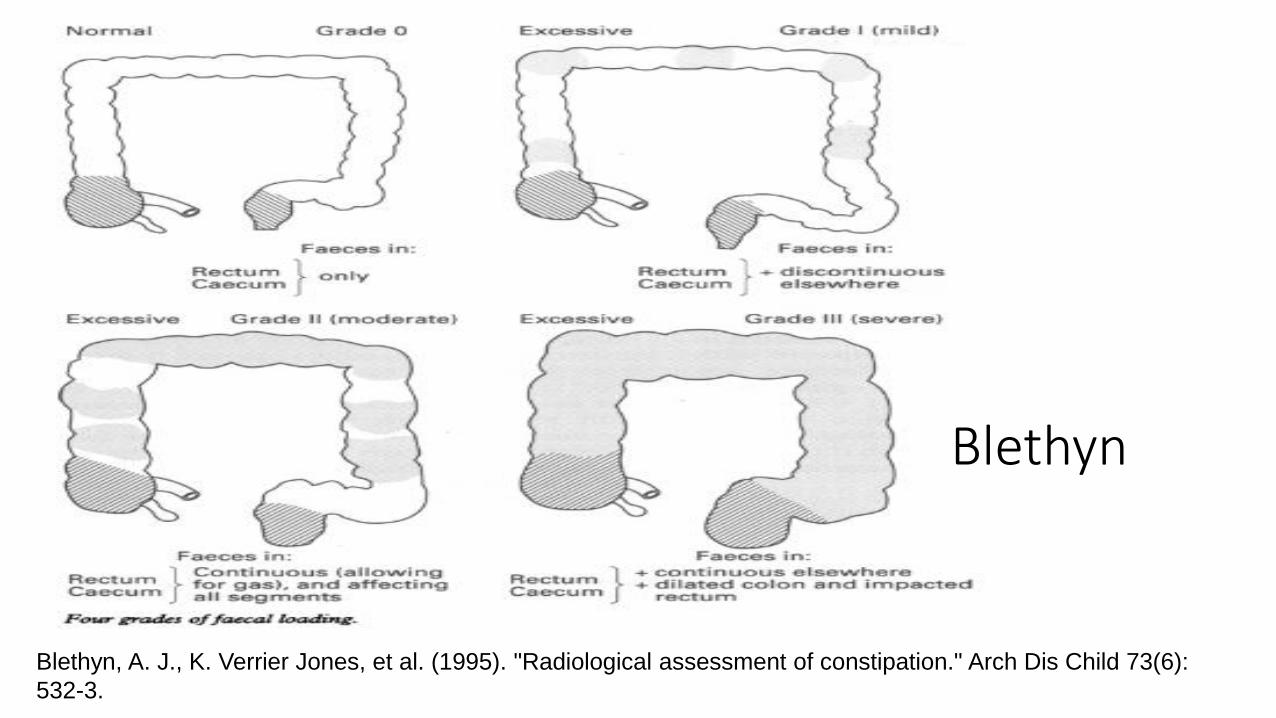
Blethyn, A. J., K. Verrier Jones, et al. (1995). "Radiological assessment of constipation." Arch Dis Child 73(6):
532-3.
Blethyn

Leech
• Each of the sections
• 0 – no visible loading
• 1 – scanty feces
• 2 – mild fecal loading
• 3 – moderate fecal loading
• 4 – severe fecal loading
• 5- Severe loading with dilatation
Leech, S. C., K. McHugh, et al. (1999). "Evaluation of a method of assessing faecal loading on plain abdominal
radiographs in children." Pediatr Radiol 29(4): 255-8.
Leech
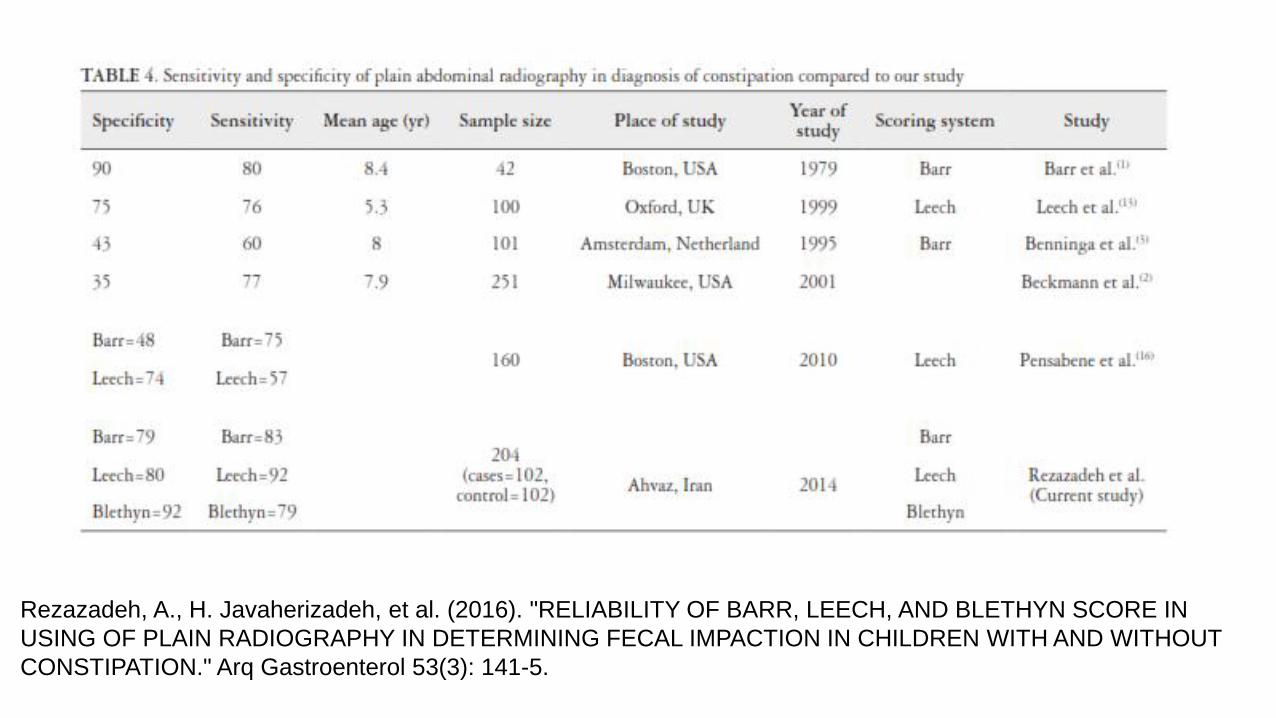
Rezazadeh, A., H. Javaherizadeh, et al. (2016). "RELIABILITY OF BARR, LEECH, AND BLETHYN SCORE IN
USING OF PLAIN RADIOGRAPHY IN DETERMINING FECAL IMPACTION IN CHILDREN WITH AND WITHOUT
CONSTIPATION." Arq Gastroenterol 53(3): 141-5.

? Colonic Transit Time
• Idea to see degree of delay and outline areas of hold up
• Generally does not offer new options
• ? Biofeedback (not evidence based in children)
• ? May have some use if considering antegrade colonic enema • Better tolerated and more available than Colonic manometry

Sitz Markers
Colonic Inertia Outlet Obstruction
Can be helpful in differentiating colonic inertia vs. outlet obstruction
http://www.sitzmarks.com/howtointerpretasitzmarkstest.aspx
Sitz Markers
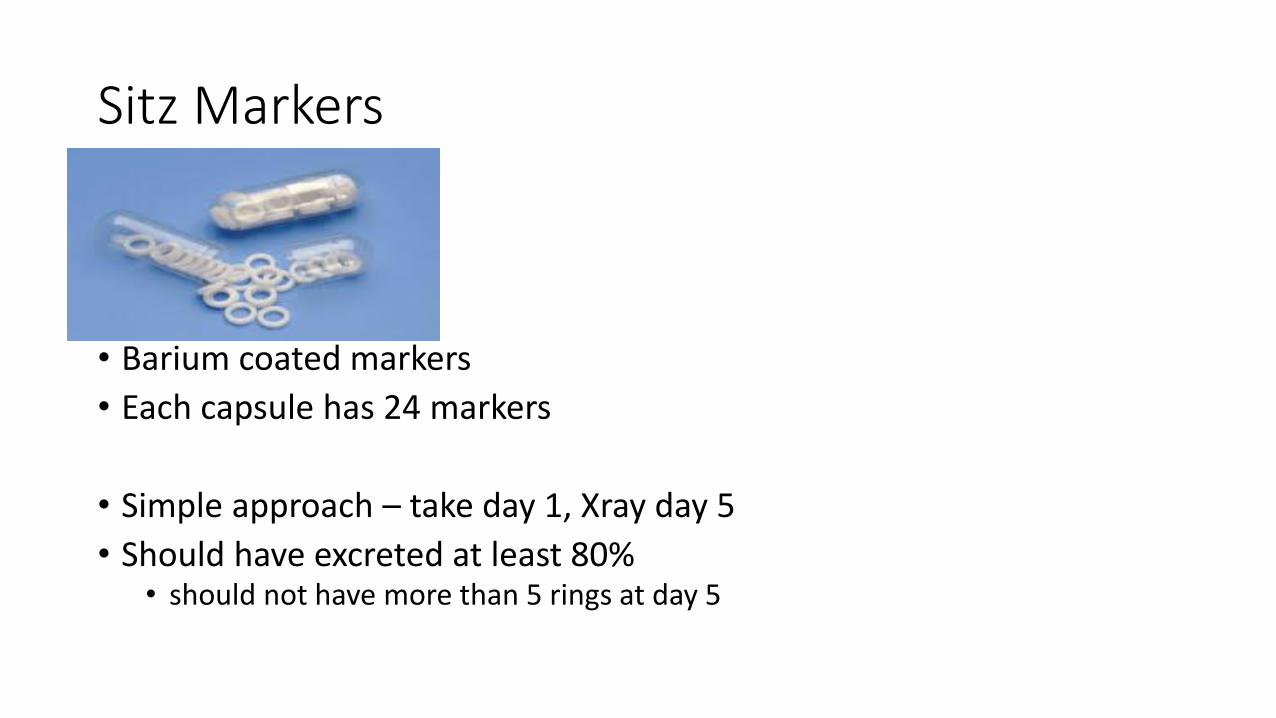
• Barium coated markers
• Each capsule has 24 markers
• Simple approach – take day 1, Xray day 5
• Should have excreted at least 80% • should not have more than 5 rings at day 5
Sitz Markers
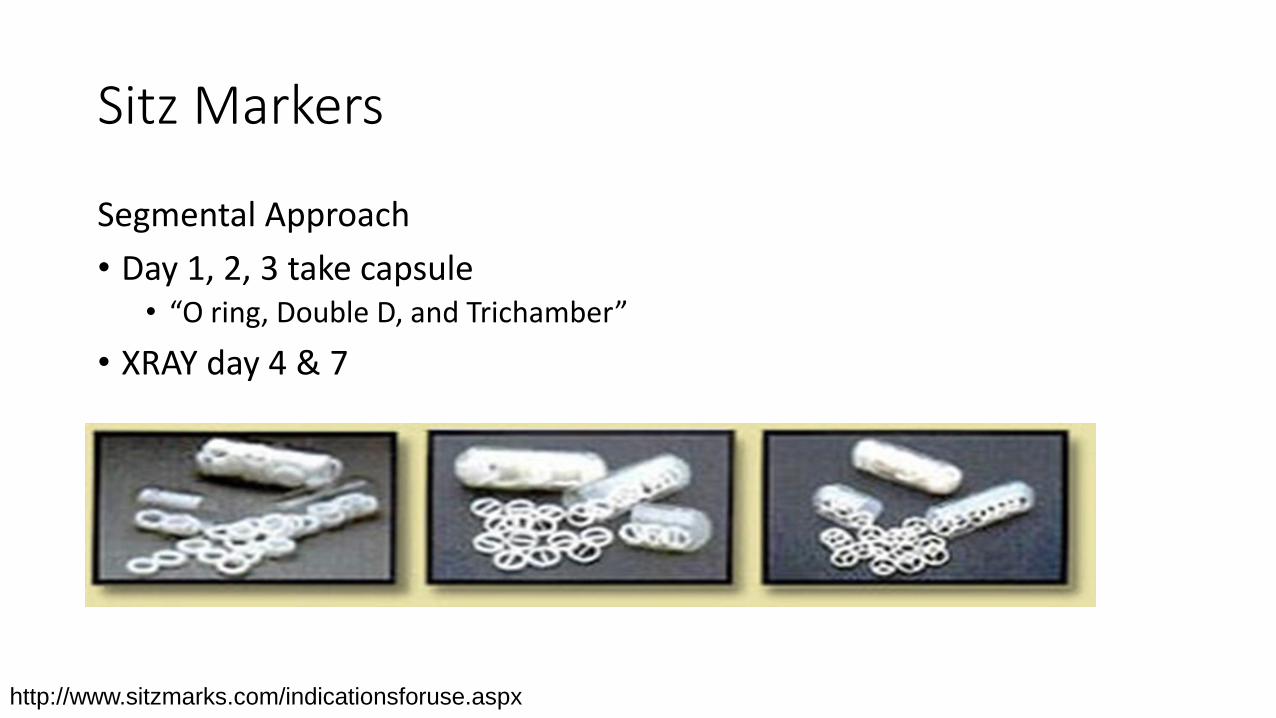
Segmental Approach
• Day 1, 2, 3 take capsule • “O ring, Double D, and Trichamber”
• XRAY day 4 & 7
http://www.sitzmarks.com/indicationsforuse.aspx

Sitz Markers
Can help calculate colonic transit time

Calculation of transit time Day 4 Day 7
Right Left Rectosigm Total Colon
Day 4 7 6 32 45
Day 7 0 0 2 2
Transit Time (hrs) 7 6 34 47
(normal) 11.3 11.3 12.4 35

Colonic Transit Time
• “In conclusion, evidence does not support the routine use of colonic transit studies to diagnose functional constipation”
but
• “Comment: The working group concluded that demonstration of a normal CTT with the prompt passage of markers suggests either nonretentive fecal incontinence (a condition in which children have fecal incontinence without having functional constipation) or an unreliable medical history.”
Other Imaging
• Transabdominal Rectal Ultrasound • Larger rectum vs. controls
• However operator dependant, and timing required bladder and bowels
• “Rectal ultrasound is not recommended to diagnose functional constipation”
• Spine imaging (MRI) • “In conclusion, evidence does not support the use of MRI of the spine in
patients with intractable constipation without other neurologic abnormalities”

Other Imaging - Barium Enema
• “Based on expert opinion, we do not recommend performing barium enema as an initial diagnostic tool for the evaluation of children with constipation.”
• “Rectal biopsy is the gold standard for diagnosing HD”
Why do some get imaging?
Chief Complaint : Abdominal Pain
• Acute (on chronic?) abdominal pain (without vomiting or diarrhea) • Emergency room
• Chronic Abdominal Pain • > 5 y.o don’t share information about their stool in a reliable manner.
• Don’t acknowledge fear of stooling
• Do not want to discuss, simply want to be “normal”
Why do some get imaging?
Encopresis
• Suspect constipation but frequency is actually increased or there is small frequent stools, often in underwear. Don’t have large BM.
• Stool in the underwear – embarrassed, bullied, does not want to do a digital rectal exam, poor QOL.
• HCP also worry about upsetting / ‘traumatizing’ with DRE

Why do some get imaging?
Doubters (Near the time of diagnosis)
• Patient / Parent don’t believe the diagnosis • ‘eat clean, fruits and vegetables, drinks well, ‘goes everyday’.
• Have tried clean out – and symptoms can be worse (more frequent, more cramps, ‘accidents’, at times feeling lack of control)

Why do some get imaging?
• Doubters (longer term)
• Treatment and clinical changes are very slow (takes months / years)
• Have been given the diagnosis, have tried treatment (often not long enough) and not improved
• Improving but don’t like the idea of ongoing medication or concerns about ‘dependance’. At times want to see if ‘ready to come off’

Why do some get imaging? The “Need” to be objectify the fecal loading
• Colonic Transit Time
• If had imaging at baseline and ‘confirmed’ in this manner
• If had a ‘score’ – and to see if there is a change
• Label of ‘megarectum’

Why do some get imaging?
• 1. Chief complaint is abdominal pain • Acute / Chronic
• 2. Suspect constipation but frequency is actually increased or there is small frequent stools. • Encopresis
• 3. Patient / HCP does not want to do a digital rectal exam • For good or not good reasons.
• 4. Doubters • Short term – clean out, don’t like diagnosis • Long term – natural history
• Not seeing improvement, reinforcing need for treatment
• 5. The ‘need’ to be objective • CTT, following up a score or ‘degree’ of fecal impaction.

Future QI project?
• Tracking AXR numbers ordered • Where are they coming from?
• Is the info for the care provider or the family?
• Asking about utility / value?

Objectives
• Review the criteria for diagnosing functional constipation
• Highlight the (limited) role for imaging in functional constipation
• Identify some tools in the literature that have been used for objectifying constipation
• Give some examples (including non evidence based) reasons for imaging as part of constipation evaluation