Embed Size (px)
Citation preview

Internal Medicine Reviews for National License Examination II
S a n t i S i l a i r a t a n a , M D
D i v i s i o n o f Pu l m o n a r y M e d i c i n e , D e p a r t m e n t o f M e d i c i n e , Fa c u l t y o f M e d i c i n e Va j i r a H o s p i t a l
N a v a m i n d r a d h i r a j U n i v e r s i t y
Pulmonary Medicine and Critical Care

Asthma
COPD
Pneumonia
Tuberculosis
Sepsis and septic shock
Pleural effusion

Airway Diseases: Asthma and COPD

General Steps of Approach of Airway Diseases
Typical symptoms of
airway disease
Detailed history/examination Diagnostic tests

Typical Clinical Features in Airway Diseases
Mucociliary clearance BronchospasmCoughing
Sneezing
Chronic cough Sputum production
Wheezing Dyspnea/shortness of breath
Chest tightness

Spirometry with Bronchodilator Response Test
Airflow limitation: Reduced FEV1/FVC (Normal 0.75-0.80) Reversibility: FEV1 increases >12% and 200 mL

Asthma versus COPD
Asthma COPD
Age group Typically begins in childhood Patient typically >40 years of age
Smoking No direct relationship Mainly smokers and ex-smokers
Dyspnea Episodic attacks with exposures to allergen, irritant, or exercise
Progressive shortness of breath, usually with exertion
Cough Typically a dry cough at night Productive cough, typically in the morning

Asthma

Asthma
3 Episodic breathlessness, wheezing, chest tightness
Associated with airway hyperresponsiveness2
1 Chronic inflammation of airways
5 Reversible either spontaneously or with treatment
4 Airflow limitation

Asthma Phenotypes
Asthma with obesityAllergic asthma Late-onset asthmaNon-allergic asthma
Exercise-induced asthma Occupational asthma Work-aggravated asthma Aspirin-induced asthma Asthma-COPD
overlap syndrome (ACOS)

Pathogenesis of Allergic Asthma

Airway Abnormalities in Asthma
Normal bronchiole Asthmatic bronchiole
1
2
3
4
Smooth muscle hypertrophy
Vascular proliferation Capillary leakage
Submucosal gland hypertrophy
Mucous hypersecretion

Physiologic Change in Asthma
http://www.google.co.th/url?sa=i&rct=j&q=&esrc=s&source=images&cd=&docid=Hk_PSlY10HFWQM&tbnid=YCHYLHpoyi8JSM:&ved=0CAUQjRw&url=http%3A%2F%2Fquizlet.com%2F17264799%2Frespiratory-mechanics-ii-flash-
cards%2F&ei=cwdyU_iJD9WF8gWZzoGwAQ&bvm=bv.66330100,d.c2E&psig=AFQjCNGA1cMV-5TviGGyZ
TbCe-i4J2_l_g&ust=1400068322927498
Airway Resistance
Airway narrowing ⬇
Increased resistance ⬇
Increased work of breathing ⬇
Dyspnea, muscle fatigue ⬇
Respiratory failure

General Steps of Approach: Asthma
Screening typical symptoms of asthma
Detailed history/examination
for asthma
Diagnostic tests for asthma
Evidence of variable respiratory symptoms
Evidence of variable airflow limitation

Symptoms of Asthma
Increased probability of asthma
More than one symptoms of asthma,especially in adults
Symptoms often worse at night orearly morning
Symptoms vary over time and in intensity
Symptoms are triggered by viral infection,exercise, allergen exposure, changes in weather, laughter, or irritants
Decreased probability of asthma
Isolated cough with no other respiratory symptoms
Chronic production of sputum
Shortness of breath associated dizziness,lightheadedness, paresthesia
Chest pain
Exercise-induced dyspnea with noisy inspiration

Diagnostic Tests for Asthma
Peak Expiratory
Flow
Broncho-provocation
testSpirometry Exercise
challenge testInflammatory
markers
FEV1/FVC Reversibility
Methacholine Histamine
Eucapnic hyperventilation Mannitol
Variability Reversibility
Exhaled nitric oxide (FENO) Allergy test
Serum IgE level Sputum eosinophil

(Mini-Wright) Peak Flow Meter

Peak Flow VariabilityPEF max
PEF min
PEF variability = (PEF max - PEF min)
1/2 x (PEF max + PEF min)
Diagnosis of asthma can be made when average daily diurnal PEF variability
>20%

Minimum Morning Pre-bronchodilator PEFPEF max
PEF min
Min%Max = PEF min
PEF max
Diagnosis of asthma can be made when Min%Max
<80%
Previous Guidelines

Methacholine Challenge Testing
Baseline spirometry Repeat spirometry Repeat spirometryuntil FEV1 fall 20%
or the dose of 16 mg/mL
is reached
Methacholine 0.031-0.625 mg/mL
Methacholine 2x-4x of
initial concentration
Albuterol 2 puff
Repeat spirometry

Diagnostic Algorithm for Asthma: Summary
Clinical Features Shortness of breath, Chest tightness, Recurrent wheezing, and Cough Symptoms get worse during nighttime, early morning, seasonal, allergen exposure, or exercise Presence of allergic disease or a family history of allergy or asthma (not required)
Reversibility Spirometry: FEV1/FVC <75% with FEV1 increase ≥12% AND 200 mL post bronchodilator Peak expiratory flow (PEF): Increase ≥20% or ≥60 L/min post bronchodilator
Variability Test Average diurnal PEF variability: >10% Minimum morning PEF: <80%
Bronchoprovocation Test Methacholine test: PC20 <8 mg/mL Exercise challenge test: FEV1 reduces >10%
and 200 mL

Asthma & Asthma Symptoms: Tip of the Iceberg
Airway inflammation
Bronchialhyperresponsiveness
Bronchospasm Airflow limitation
Asthma symptoms
Risk of asthma exacerbation
Treatment for Asthma (symptom) control
Treatment for Worsening/exacerbation
risk

General Principles of Asthma Management
Assessing disease severity Identify risk(s)
Provide treatment and modify risk(s)
Assessment of symptom and risk control
Step treatmentup or down to
maintain control

Initiation of TreatmentGINA 2014
Presenting symptoms Preferred initial controller
Symptoms or SABA use <2/month No waking due to asthma symptom No risk factor
No controller
Infrequent symptoms Presence of ≥1 risk factors for exacerbation Low dose ICS
Symptoms or SABA use >2/month but <2 /week Waking due to asthma ≥1/month Low dose ICS
Symptoms or SABA use >2/week Low dose ICS LTRA or Theophylline
Symptoms in most days Waking due to asthma >1/week
Medium/high dose ICS Low dose ICS/LABA
Severly symptomatic or acute exacerbationShort course of oral corticosteroids AND
High dose ICS OR Moderate dose ICS/LABA
Global Strategy for Asthma Management and Prevention. Revised 2014

Inhaled Corticosteroid Dosage
ICS Low dose (µg) Medium dose (µg) High dose (µg)
Beclometasone 200-500 500-1000 1000-2000
Budesonide 200-400 400-800 800-1600
Fluticasone propionate 100-250 250-500 500-1000
Ciclesonide 80-160 160-320 320-1280
Mometasone furoate 200-400 400-800 800-1200
แนวทางวินิจฉัยและรักษาโรคหืดในประเทศไทย V.5 สำหรับผู้ใหญ่และเด็ก พ.ศ. 2555

Level of Asthma Control
Characteristics Controlled (All of the following)
Partly Controlled (Any measure present
in any week)Uncontrolled
Daytime symptoms None (twice or less/week) More than twice/week
Three or more features of partly controlled asthma
present in any week
Limitations of activities None Any
Nocturnal symptoms/awakening None Any
Need for reliever/rescue treatment None (twice or less/week) More than twice/week
Lung function (PEF or FEV1) Normal <80% predicted or personal best (if known)
Exacerbations None One or more/year One in any week

Management Options
CPU
Uncontrolled Partly Controlled Controlled
Step up treatment
Maintain treatment and observe
Step down treatment
Step up treatment Maintain treatment and observe
3-6 Months

Stepwise Approach
Step 5
Step 4
Refer for add-on treatment
(e.g. anti-IgE)
Step 3
Medium/high doseICS/LABA
Step 1 Step 2Low dose ICS/LABAPreferred Low dose ICS
Optional Consider low dose ICS
LTRA Theo
Medium/high dose ICS Low dose ICS +LTRA Low dose ICS + Theo
High dose ICS + LTRAHigh dose ICS + Theo
Add low dose OCS
As needed short-acting beta2 agonist (SABA)
As needed short-acting beta2 agonist (SABA) or Low dose ICS/formoterol
ICS = Inhaled corticosteroids LTRA = Leukotriene receptor antagonists LABA = Long-acting beta2 agonists Theo = Theophylline OCS = Oral corticosteroids
Global Strategy for Asthma Management and Prevention. Revised 2014

Options for Stepping Down Treatment
Current Step Current medication and dose Options for stepping down
5High dose ICS/LABA
plus OCS or other add-on agents
Continue high dose ICS/LABA, reduce OCS dose Use sputum-guided approach to reduce OCS Alternate-day OCS treatment Replace OCS with high dose ICS
4
Moderate to high dose ICS/LABA maintenance treatment
Continue combination ICS/LABA with 50% reduction in ICS component by using available combination
Discontinuing LABA (more likely to lead to deterioration)
Medium dose ICS/formoterol as maintenance and reliever
Reduce maintenance ICS/formoterol to low dose, and continue as needed low dose ICS/formoterol reliever
High dose ICS plus second controller Reduce ICS dose by 50% and continue second controller
Global Strategy for Asthma Management and Prevention. Revised 2014

Options for Stepping Down Treatment
Current Step Current medication and dose Options for stepping down
3
Low dose ICS/LABA maintenance Reduce ICS/LABA to once daily Discontinuing LABA (more likely to lead to deterioration)
Low dose ICS/formoterol as maintenance and reliever
Reduce maintenance ICS/formoterol to once daily, and continue as needed low dose ICS/formoterol reliever
Moderate or high dose ICS Reduce ICS dose by 50%
2
Low dose ICS Once-daily dosing (budesonide, ciclesonide, mometasone)
Low dose ICS or LTRA Stop controller treatment (when no symptoms for 6-12 months
and no risk factor) Complete cessation of ICS (increased risk of exacerbation in adults)
Global Strategy for Asthma Management and Prevention. Revised 2014

Patient with Poor Symptom Control
1 3 42
Check inhaler technique Discuss adherence
Confirm the diagnosis of asthma
Remove potentialrisk factors
Consider treatment step up
Assess and manage comorbidities

Management of Asthma Exacerbation
Initial assessment
2nd Assessment
Intubation
Unconscious Air hunger
RR <12/min Unstable hemodynamics
A
Hx of intubationHx of steroid use
Admission in 1 year Rescue medication use
>1 canister/month
B
PR >130/min RR >30/min Wheezing
C
Incomplete sentence Accessory muscle used Abdominal paradox Unable to lie down
D
Ramathibodi action plan

Short acting bronchodilators: 4 puffs of salbutamol (100 µg) via spacer q 15-20 min
Salbutamol 1 NB via nebulizer q 15-20 min
if Any of B or D
Systemic corticosteroid: Dexamethasone 4-5 mg iv
Oral prednisolone 40 mg p.o.
PEF
3rd AssessmentA
C
D
PEF
Ramathibodi action plan

Discharge
4th Assessment
Iprotropium/fenoterol 4 puff via spacer
1 NB via nebulizer
PEFR >70% PEFR >70% + any of C
PEFR 50-70% + any of C
PEFR 50-70% + any of A, D PEFR <50%
PEFR >70%
PEFR 50-70% + any of C
Admit ward Admit ICU
PEF
Ramathibodi action plan

Treatment in Acute Care Setting
Recommended Oxygen:
to achieve arterial oxygen saturation of 93-95% low flow oxygen is preferred to high flow (100% O2)
Inhaled short-acting beta2-agonist and Iprotropium bromide: The most cost-effective and efficient delivery: pMDI with a spacer When nebulization is used, initiate with continuous therapy, followed by intermittent on-demand therapy Iprotropium bromide - greater improvement in PEF and FEV1
Systemic corticosteroids: Oral administration = intravenous administration Dose: Prednisolone 50 mg/day or Hydrocortisone 200 mg/day Duration: 5-7 days

IMPORTANT!!
Acute exacerbation of asthma = uncontrolled asthma
Review and modify treatment to prevent another exacerbation BEFORE send them home

Discharge Management
Medications Risk Reduction Uncontrolled asthma
symptoms
Excessive SABA use
Inadequate ICS
Low FEV1 (<60% predicted)
Major psychological or socioeconomic problems
Exposures: smoking, allergens
Comorbidity: obesity, rhinosinusitis
Self-management & Asthma action plan
Review inhaler technique
Review PEF technique
Provide written asthma action plan
Evaluate the patient’s response to the exacerbation
Review the patient’s use of controller treatment
Oral corticosteroids: At least 5-7 days of
Prednisolone 1 mg/kg/day (max. 50 mg/day)
Inhaled corticosteroids: Initiate (if not done)
Step up treatment for 2-4 wks Remind adherence
Reliever medications: Transfer back to as-needed use
beta2-agonist is preferred

Chronic Obstructive Pulmonary Disease (COPD)
นพ.สันติ สิลัยรัตน พบ.อายุรแพทย โรคระบบการหายใจและเวชบำบัดวิกฤตทางการหายใจแผนกอายุรกรรม ศูนยแพทยศาสตรศึกษาชั้นคลินิก โรงพยาบาลอุดรธานี
Holistic approach for COPD: Time to Treat Earlier to Prevent Future Risk
ความรูเรื่องโรคปอดอุดกั้นเรื้อรัง

Definition
3 Characterized by persistent airflow limitation
Associated with noxious particles and gases2
1 Chronic inflammation of airways
4 Exacerbation and comorbidities contribute to the overall severity
5 Preventable and treatable

Causes and Pathogenesis of COPDสาเหตุและกลไกการเกิดโรคปอดอุดกั้นเรื้อรัง

Physiologic and Health Effects of COPD
Expiratory airflow limitation
Air trapping
Hyperinflation
Inactivity
Deconditioning Activity limitation Poor quality of life
Dyspnea
Exacerbations

Diagnosisการวินิจฉัยโรคปอดอุดกั้นเรื้อรัง

Grading of COPD Severity
ระดับความรุนแรงของโรคปอดอุดกั้นเรื้อรัง
ระดับความรุนแรง Mild Moderate Severe Very Severe
FEV1/FVC <70%<70%<70%<70%
FEV1(% of
predicted)>80 50-79 30-49
<30หรือ <50 รวมกับมีภาวะ
การหายใจลมเหลวเรื้อรัง หรือมี cor pulmonale

Combined Assessment for COPD
C D
A B
RiskGOLD classification
of Airflow Limitation
1
2
3
4≥2
1
0
RiskExacerbation
history
mMRC 0-1 CAT <10
mMRC ≥2 CAT >10

B CA D
Less symptoms Low risk
MORE symptoms Low risk
Less symptoms HIGH risk
MORE symptoms HIGH risk

Modified Medical Research Council Questionnaire
สำหรับการประเมินระดับอาการเหนื่อยในผู้ป่วยโรคทางเดินหายใจ
Modified Medical Research Council Questionnaire
สำหรับการประเมินระดับอาการเหนื่อยในผูปวยโรคทางเดินหายใจ
เลือกขอใดขอหนึ่งตอไปนี้ตามอาการที่ทานเห็นวาใกลเคียงกับความรูสึกของทานมากที่สุดเลือกขอใดขอหนึ่งตอไปนี้ตามอาการที่ทานเห็นวาใกลเคียงกับความรูสึกของทานมากที่สุดเลือกขอใดขอหนึ่งตอไปนี้ตามอาการที่ทานเห็นวาใกลเคียงกับความรูสึกของทานมากที่สุด
Grade 0: รูสึกเหนื่อยเฉพาะเวลาที่ออกกำลังกายหนัก ๆ ☐
Grade 1: รูสึกเหนื่อยเวลาเดินขึ้นบันได หรือเดินขึ้นเนิน ☐
Grade 2: รูสึกเหนื่อยเมื่อเดินบนพื้นราบจนเดินไดชากวาคนทั่วไป หรือตองพักเมื่อตองเดินไกล ๆ ☐
Grade 3: รูสึกเหนื่อยจนเดินบนพื้นราบไดไมถึง 100 เมตร หรือเดินไดไมกี่นาที ☐
Grade 4: รูสึกเหนื่อยจนไมกลาออกจากบาน หรือเหนื่อยจากการทำกิจวัตรประจำวัน ☐

COPD Assessment Test
0 1 2 3 4 5 คะแนน
ฉันไม่มีอาการไอเลย ⚪ ⚪ ⚪ ⚪ ⚪ ⚪ ฉันไอตลอดเวลา
ฉันไม่มีเสมหะในปอดเลย ⚪ ⚪ ⚪ ⚪ ⚪ ⚪ ปอดของฉันเต็มไปด้วยเสมหะ
ฉันไม่รู้สึกแน่นหน้าอกเลย ⚪ ⚪ ⚪ ⚪ ⚪ ⚪ ฉันรู้สึกแน่นหน้าอกมาก
ฉันรู้สึกหายใจได้คล่องเมื่อต้องเดินขึ้นเนิน
หรือขึ้นบันไดหนึ่งชั้น⚪ ⚪ ⚪ ⚪ ⚪ ⚪
ฉันเหนื่อยหอบอย่างมากเมื่อต้องเดินขึ้นเนิน
หรือขึ้นบันไดหนึ่งชั้น
ฉันทำกิจกรรมต่าง ๆ ที่บ้านได้โดยไม่จำกัด ⚪ ⚪ ⚪ ⚪ ⚪ ⚪ ฉันทำกิจกรรมต่าง ๆ ที่บ้านได้อย่างจำกัดมาก
ฉันมีความมั่นใจที่จะออกไปนอกบ้านได้
แม้ว่าปอดฉันยังมีปัญหา⚪ ⚪ ⚪ ⚪ ⚪ ⚪
ฉันไม่มั่นใจเลยที่จะออกไปนอกบ้านเพราะ
ปัญหาที่ปอด
ฉันนอนหลับได้สนิท ⚪ ⚪ ⚪ ⚪ ⚪ ⚪ ฉันนอนหลับไม่สนิทเพราะปอดมีปัญหา
ฉันรู้สึกกระฉับกระเฉงอย่างมาก ⚪ ⚪ ⚪ ⚪ ⚪ ⚪ ฉันรู้สึกอ่อนเพลียและเหนื่อยล้า

Exacerbations and Progression of COPDการกำเริบเฉียบพลันกับการดำเนินโรค
FEV1
อายุ
ไมมีการกำเริบเสียชีวิต
เริ่มมีอาการ
เกิดการกำเริบเฉียบพลัน
ยิ่งมีการกำเริบของโรคบอย และมาก ยิ่งทำใหเสียชีวิตเร็วยิ่งขึ้นMORE exacerbations HIGHER mortality

Severity Grading and Number of Exacerbationsจำนวนครั้งเฉลี่ยของการกำเริบเฉียบพลันตอปในผูปวย COPD
0"
5"
10"
15"
20"
25"
zero" 0*1" 1*2" 2*3" 3*4" 4*6" 6*8" >8"
%"pa3ents"
Annualised"rate"of"exacerba3ons"
GOLD%Stage%3,4%(FEV1%<%50%%pred)%
Jones"et"al""Eur"Respir"J"2003;"21:"68–73""
0"
5"
10"
15"
20"
25"
30"
zero" 0*1" 1*2" 2*3" 3*4" 4*6" 6*8" >8"
%"pa3ents"
GOLD%Stage%2%%(FEV1%>%50%%pred)%
>40%%

Combined Assessment for COPDอัตราการเกิดการกำเริบปานกลาง/รุนแรงภายหลังการใช ICS
Calverley et al. NEJM 2007; 356:775-789.
0
0.3
0.5
0.8
1.0
1.3
1.5
Placebo Salmeterol Fluticasone Salmeterol/Fluticasone
0.850.930.97
1.13
25% reduction
* ** ✝�
*p < 0.001 vs placebo; †p = 0.002 vs SALM; �p = 0.024 vs FP*p < 0.001 vs placebo; †p = 0.002 vs SALM; ☨p = 0.024 vs FP Calverley et al. NEJM 2007; 356:775-789.

Combined Assessment for COPD
C D
A B
RiskGOLD classification
of Airflow Limitation
1
2
3
4≥2
1
0
RiskExacerbation
history
mMRC 0-1 CAT <10
mMRC ≥2 CAT >10

Components of COPD Management
Component 2: Symptom & Risk Management
Component 1: Identify &
Control risk factors
Component 3: Rehabilitation & Health promotion

Goals of COPD Management
แผนการรักษาผูปวยโรคปอดอุดกั้นเรื้อรัง
เพื่อคง เพื่อลด
สภาพรางกายในปจจุบันใหดีที่สุด ความเสี่ยงที่จะเกิดขึ้นในอนาคต
อาการ โครงสรางและสมรรถภาพปอด
ความถี่ของการใชยาขยาย
หลอดลมตามอาการ
โรคหรือภาวะรวม
สถานะสุขภาพ
กิจกรรมในแตละวัน
การกำเริบของโรค ความเสื่อมสถานะสุขภาพ
ความเสี่อมของโครงสราง
และสมรรถภาพปอด
โรคหรือภาวะรวม
ที่อาจเกิดขึ้นใหม
ผลขางเคียงของยาที่ใช
การเสียชีวิต
แผนการรักษา COPD
เพื่อคง เพื่อลด

Component 1: Identify and Control Risk Factors

Importance of Smoking Cessation in COPDผลของการหยุดบุหรี่กับการเปลี่ยนแปลงของสมรรถภาพปอด
Fletcher C et al. The Natural History of Chronic Bronchitis and Emphysema. 1976.Scanlon PD et al. Am J Respir Crit Care Med 2000; 161: 381-390.
Age25
ผูที่ยังคงสูบบุหรี่
ผูที่ไมสูบบุหรี่
40 70
เริ่มมีอาการ
55
เสียชีวิตเลิกบุหรี่
FEV1
Fletcher C et al. The Natural History of Chronic Bronchitis and Emphysema. 1976. Scanlon PD et al. Am J Respir Crit Care Med 2000; 161: 381-390.

Immunization for COPD Patientsการใหวัคซีนแกผูปวยโรคปอดอุดกั้นเรื้อรัง
Influenza vaccine Pneumococcal vaccine
ควรพิจารณาใหกับผูปวยทุกรายหากเปนไปไดทั้งนี้ขึ้นกับแนวปฏิบัติบริการในประเทศนั้น ๆ

Component 2: Symptom and Risk Management

Treatment Options for COPD
Patient Group First Choice Second Choice Alternative Choice
A SAMA prn SABA prn
LAMA LABA
SAMA + LABATheophylline
B LAMA LABA LAMA+LABA SAMA +SABA
Theophylline
C ICS + LABA LAMA LAMA + LABA
iPDE4 SAMA + SABA Theophylline
D ICS + LABA LAMA
ICS + LAMA ICS + LAMA + LABA ICS + LABA + iPDE4
LAMA + LABALAMA + iPDE4
Carbocysteine SAMA + SABA Theophylline
SAMA = short-acting muscarinic antagonist (anticholinergic) SABA = short-acting beta-2 agonist
ICS = inhaled corticosteroid iPDE2 = phosphodiesterase inhibito
Non ICS
ICS

สรุปหลักการใชยา สำหรับผูปวยโรคปอดอุดกั้นเรื้อรัง
ประเมินความพรอมในการใชอุปกรณ(แรงสูดยา, ความสัมพันธระหวางการสูดกับการกดยา)
เลือกอุปกรณที่เหมาะสมกับผูปวย
ติดตามผลการรักษา(อาการหอบเหนื่อย, CAT, mMRC, การกำเริบของโรค)
ปรับเพิ่มยาขยายหลอดลมเมื่อยังบรรเทาอาการหอบเหนื่อยไดไมเพียงพอ
ปรับเพิ่มยา ICSเมื่อมีการกำเริบบอย หรือยังมีอาการหอบ

Component 3: Rehabilitation and Health Promotion

Rehabilitation for COPD Patientsการฟนฟูสมรรถภาพปอด
เพิ่มความทนทาน
ตอการออกกำลังกาย
PulmonaryRehabilitation
ลดโอกาส
การเสียชีวิต
เสริมประสิทธิภาพของ
การรักษาดวย ICS/LABAทำใหสุขภาพจิตดีขึ้น
คลายความกังวล
ทำใหคุณภาพชีวิตดาน
ภาวะสุขภาพดีขึ้นทำใหกำลังกลามเนื้อแขนขาดีขึ้น
ลดจำนวนและวันใน
การเขารักษาในโรงพยาบาล
ฟนตัวจากอาการ
กำเริบของโรคไดเร็วขึ้น

Tuberculosis

Tuberculosis
20 * Diagnostics for tuberculosis: global demand and market potential *
1CHAPTER
WHO’s Global TB Monitoring and
Surveillance Project experts esti-
mate the total number of cases to
be 8.8 million (3.9 million sputum
smear-positives) (2).
In 2003, 4.1 million cases (1.9 mil-
lion sputum smear-positive) were
notified to public health officials
around the globe. Seven million of
the estimated 8.8 million cases are
concentrated in 22 high-burden
countries of the developing world
(Figure 2). If recent trends should
continue for the rest of this decade,
the projected global number of
new cases will increase to 10 mil-
lion cases in 2015 (3).
Exposure to TB
Subclinical "latent" infection
"active" TB disease
Sputumsmear
positive
Sputumsmear
negative
Drugsensitive
Drugresistant
Pulmonary
Smearpositive
Smearnegative
Drugsensitive
Drugresistant
Extrapulmonary
Fig
ur
e 1 TUBERCULOSIS CLASSIFICATION SCHEME
Fig
ur
e 2 THE ESTIMATED GLOBAL BURDEN OF TUBERCULOSIS
CUMMULATIVEINCIDENCE (%)
20%
35%
43%
47%
51%
54%
57%60%62%64%67%68%
70%72%73%
74%75%76%77%78%79%
80%
100%
ESTIMATEDINCIDENCE
1,788,0431,334,066
627,047362,819360,767278,392251,685241,537236,885195,207194,627160,688
144,942
137,260
110,319
106,20189,351
86,130
85,015
84,546
79,656
71,830
8,810,040
COUNTRY
IndiaChinaIndonesiaNigeriaBangladeshPakistanEthiopiaSouth AfricaPhilippinesKenyaDR CongoRussianFederationViet NamUR TanzaniaBrazilUgandaThailandMozambiqueZimbabweMyanmarAfghanistanCambodia GlobalEstimated TB Cases
Sou
rce:
refe
ren
ce 2
.More people die from TB than from any other curable infectious disease.
Every day 25,000 people develop active TB and 5,000 die of the disease.
WHO. Global tuberculosis control: surveillance, planning, financing: WHO report 2005. Geneva: WHO, 2005.
Poverty
Congregation
HIV pandemic

Tuberculosis-HIV Coinfection
* Diagnostics for tuberculosis: global demand and market potential * 53
resistant, it is estimated that over
400,000 people fall ill with MDR-TB
each year, and that over 50 million
people are latently infected with
MDR strains of TB (7). The regional
distribution of MDR-TB is illustrat-
ed in Figure 4. Two thirds of MDR-
TB cases occur in just three
countries, China, India and the
Russian Federation.
Another serious threat underlying
the need for improved diagnostics
is the HIV pandemic, which greatly
increases susceptibility to TB infec-
tion and disease, and decreases the
effectiveness of conventional diag-
nostic approaches. Globally, 12% of
new adult cases of TB are HIV co-
infected, but the burden of dual dis-
ease is concentrated in Africa and
in some regions in Asia (see Figure
5), where the collision between HIV
and high prevalence of latent TB
infection (50-90%) has sparked a
dramatic rise (3-10 fold in some
countries) in active TB cases.
In summary, tuberculosis is a glob-
al epidemic concentrated in the
developing world, in close associa-
tion with poverty and, increasingly,
HIV. Testing for tuberculosis
remains common in industrialized
countries, where immigrants make
up a large and growing fraction of
all cases. MDR-TB and HIV are both
substantial threats to TB control,
and have prompted significant
increases in expenditure on TB
diagnosis and treatment in devel-
oped countries since the mid-
1980s, when TB was declared to be
in the elimination phase in the
United States.
Global availabilityof TB laboratoryservices
Little information has been accessi-
ble on the availability of TB diag-
nostic services in developing
countries or the volume of testing.
To this end, we carried out a global
survey of TB laboratory services.
Surveys were distributed to 207
WHO Member States to gather
information on the number of pub-
lic and private laboratory facilities
performing sputum smear
microscopy, mycobacterial culture
and drug susceptibility testing
(DST). Information was also col-
lected on the volume of testing in
the public sector. Each survey of
the 116 survey responses was
screened and respondents were
contacted directly to explain errors
and/or unexpected information.
Raw data on the number of testing
centres for TB microscopy, culture
and DST are shown in Table 1.
Fig
ur
e 5 PREVALENT ADULT TB CASES COINFECTED WITH HIV, 2004
Sou
rce:
refe
ren
ce 3
.
Dye C, Watt CJ, Bleed DM et al. Journal of American Medical Association 2005; 293:2767-75.

The Gap between Estimated and Notified Cases
Estimated TB cases 8.8 Million
Health facility
TB casesDiagnostic
tests
Recorded & reported
4.1 Million cases reported
Detected but not notified private sector
military prisons
⊕⊖
WHO. Global tuberculosis control: surveillance, planning, financing: WHO report 2005. Geneva: WHO, 2005.

Multidrug-resistant and Extensively drug-resistant TB
Multidrug-resistant (MDR) TB Resistance against at least
rifampicin and isoniazid
Extensively drug-resistant (XDR) TB MDR-TB PLUS
Resistance to any fluoroquinolones AND
≥1 injectable second-line agents
O’Grady J, Maeurer M, Mwaba P et al. Current Opinion in Pulmonary Medicine 2011, 17; 134-141.
Copyright © Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
(ethionamide, prothionamide, cycloserine, terizidone,para-aminosalicylic acid, clofazimine, amoxicillin-clavula-nate, clarithromycin, linezolid) is not recommended [12].Automated liquid culture systems are currently recom-mended by the WHO as the ‘gold standard’ for second-lineDST [12,13!!,14]. In this review, we describe the pheno-typic and genotypic methods currently available for thediagnosis of drug-resistant forms of M. tuberculosis anddiscuss future prospects for TB diagnostics.
Definitions of drug-resistant tuberculosisMDR-TB is defined as resistance to the two key first-lineanti-TB drugs, INH and RIF. XDR-TB is defined as TBcaused by strains of M. tuberculosis resistant to at leastINH and RIF (i.e. MDR-TB), plus any fluoroquinoloneand at least one of three injectable drugs used in anti-TBtreatment, capreomycin, kanamycin or amikacin [7!!,8!!].
Phenotypic drug susceptibility testingCulture-based or phenotypic DST methods are accurateand inexpensive but are disadvantaged by relying on thegrowth on M. tuberculosis, rendering them time consuming[15]. Phenotypic DST methods are performed on solid orliquid media as direct or indirect tests. Direct methods
are those used directly on patient samples where a setof drug-containing and drug-free media is inoculateddirectly with a patient specimen. Indirect DST involvesinoculation of drug-containing media with a pure culturegrown from the original patient specimen [12]. Commer-cial automated liquid culture DST methods have arelatively short turnaround time (because of sensitiveautomation and M. tuberculosis’s relatively faster growthin liquid compared with solid media) and are highlyaccurate but are expensive and require specialist equip-ment [16!]. The WHO considered evidence for theaccuracy and role of a number of noncommercial cul-ture-based methods that utilize widely available andinexpensive laboratory equipment and supplies andrecommended selected methods as interim measureswhile capacity for automated culture DST and/or geno-typic DST are being developed [1!!,17!!,18]. Microscopicobservation drug susceptibility (MODS) [17!!,19–21] andcolorimetric redox indicator (CRI) [22,23] methods and thenitrate reductase assay (NRA) [15,24!!,25] received WHOapproval [17!!]. Such methods have similar accuracy tocommercial liquid culture systems and could be imple-mented in high-burden, low-income settings with mini-mum cost; however, these tests require extensive operatortraining, standardization and quality assurance beforeimplementation [1!!].
136 Infectious diseases
Figure 2 Estimated percentage of multiple drug resistant tuberculosis among new tuberculosis cases, 2008a
, 0 to <3; , 3 to <6; , 6 to <12; , 12 to <18; , "18; ‘, no data available; , subnational data only. Reproduced withpermission from [2].

AFB stain Myc Culture
Drug susceptibility
Chest radiography CT scan
History Chronic productive cough*
Sputum production* Prolonged low grade fever
Night sweats Weight loss
Physical examination Bronchial breath sound
Crepitation Digital clubbing
Establishing Tuberculosis: Pulmonary TB
Imaging
Additional test(s)
Clinical features suggestive for tuberculosis
Microbiology

Sputum Microscopy for Acid-fast Bacilli
Friedrich Carl Adolf Neelsen (1854-1898)
Franz Ziehl (1857-1926)
Neelsen-Ziehl (Acid fast bacilli) Staining
Acid-fast bacilli appear pink in a contrasting methylene blue background

Light Emitting Diode (LED) Fluorescence Microscopy
Same (or slightly more) sensitivity
Cheaper and longer life duration of bulb (10,000 hr)
Cheaper microscopy
A dark room is not required
WHO recommended to use LED fluorescence microscope as a standard technique
WHO. Fluorescent light-emitting diode (LED) microscopy for diagnosis of tuberculosis: policy statement. Geneva: WHO 2011.

Radiographic Patterns of Tuberculosis
Reticulonodular infiltration
Miliary pattern lymphatic/interstitial spread
Cavitation
Bronchiectatic change
Bronchoalveolar pattern bronchial-alveolar spread

Diagnostic Algorithm: Clinically-suggestive
Patient with clinical features suggestive for pulmonary tuberculosis
Sputum examination for acid-fast bacilli Chest radiograph
AFB - positive CXR - compatible with TB
AFB - negative CXR - compatible with TB
AFB - negative CXR - incompatible with TB
Sputum culture and drug susceptibility testing for mycobacteria Treatment for pulmonary tuberculosis
Look for alternative diagnosis
แนวทางเวชปฏิบัติการรักษาวัณโรคในผู้ใหญ่ พ.ศ. 2556 (ฉบับร่าง). สำนักวัณโรค กรมควบคุมโรค สมาคมอุรเวชช์แห่งประเทศไทย

Diagnostic Algorithm: Radiographically-suggestive
Asymptomatic patient withradiographically suggestive tuberculosis
Sputum examination for acid-fast bacilli Review previous chest radiograph
AFB - positive CXR - compatible with TB
AFB - negative CXR - unavailable
AFB - negative CXR - unchanged
Sputum culture and drug susceptibility testing for mycobacteria Treatment for pulmonary tuberculosis
Re-evaluation and repeat CXR in 3 months
AFB - negative CXR - active TB
AFB - negative CXR - old lesion
แนวทางเวชปฏิบัติการรักษาวัณโรคในผู้ใหญ่ พ.ศ. 2556 (ฉบับร่าง). สำนักวัณโรค กรมควบคุมโรค สมาคมอุรเวชช์แห่งประเทศไทย

Mycobacterial Culture
Minion J, et al. The Lancet Infectious Disease. 2010; 10 (10): 688-698.Richter E, et al. Exper Rev Resp Med. 2009; 3 (5): 497-510.
Conventional TB culture
system
Rapid colorimetric drug susceptibility test
20-30 days
Liquid culture-based technique
Mycobacterial growth indicator tube (MGIT)
7-10 days

Treatment Regimen for Pulmonary Tuberculosis
1 2 3 4 5 6 7 8
Isoniazid Rifampin
Pyrazinamide Ethambutol
Isoniazid Rifampin
Isoniazid Rifampin
Pyrazinamide Ethambutol
Streptomycin
Isoniazid Rifampin
Pyrazinamide Ethambutol
Isoniazid Rifampin
Ethambutol
Months of treatment
“New case”
“Retreatment”

Antituberculosis Drug: Dosage
Isoniazid (4-8 mkd)
Rifampin (8-12 mkd)
Pyrazinamide (20-30 mkd)
Ethambutol (15-20 mkd)
Streptomycin (15 mkd)
Body weight
(kg)
35-40 300 450 1000 600 500
41-50 300 450 1250 800 750
50-70 300 600 1500 1000 750-1000
mkd = mg/kg/day

3 weeks 6 weeks
Sputum AFB
Chest x-ray
Response Monitoring in New Case Pulmonary TB: M+
Start 1 2 3 4 5 6
Sputum AFB
Sputum AFB
Chest x-ray
if positive
Sputum culture for TB
if positive
Chest radiograph
2 months 2 months
IRZE IR
Chest radiograph
if positive “failure”
Sputum AFB
Sputum Culture for TB*
Chest radiograph

“High Risk” of Drug-resistance TB
History of close contact to a patient with MDR-TB
Return after default of >2 months
Relapse pulmonary TB
Treatment failure (smear positive at 5th month)
Special population (immigrants, prisoners, HIV infected persons)

Sputum AFB
Chest radiograph
Response Monitoring in New Case Pulmonary TB: M-
Start 1 2 3 4 5 6
Re-evaluate
Look for other cause
Chest radiograph
2 months 2 months
IRZE IR
4 weeks 5 weeks
Chest radiograph
if not improved/progressive

Antituberculosis Drug Side Effects: Minor
Isoniazid Rifampin Pyrazinamide Ethambutol Streptomycin
Nausea/vomiting/pain ☑ ☑ ☑
Joint pain ☑ ☑
Numbness ☑
Sedative ☑
Flu-like symptomps ☑
Anti TB drug can be continued; supportive treatment is usually adequate

Antituberculosis Drug Side Effects: Major
Isoniazid Rifampin Pyrazinamide Ethambutol Streptomycin
Skin rash ☑ ☑ ☑ ☑ ☑
Confusion ☑ ☑ ☑ ☑
Hepatitis/Jaundice ☑ ☑ ☑
Renal dysfunction ☑ ☑
Thrombocytopenia ☑
Nystagmus/vertigo ☑
Visual disturbance ☑

Antituberculosis Drug Side Effects: Minor
Isoniazid Rifampin Pyrazinamide Ethambutol Streptomycin
Nausea/vomiting/pain ☑ ☑ ☑
Joint pain ☑ ☑
Numbness ☑
Sedative ☑
Flu-like symptomps ☑
Anti TB drug can be continued; supportive treatment is usually adequate

Response Monitoring in Re-treatment Pulmonary TB
2 1 month
Start 1 2 3 4 5 6
Sputum AFB
Sputum AFB
Chest x-ray
Sputum culture for TB
Sputum AFB
Chest radiograph
2 months 2 months
IRZES IRE
Chest radiograph
if positive “failure”
Sputum AFB
Sputum Culture for TB
Chest radiograph
7 8
3 wks2 2
IRZE
1 month
if positive
Sputum culture for TB
if positive

Treatment After Interruption
Interruption occurred during intensive phase of treatment
Duration of interruption
Duration of interruption
≥80%
Continue treatment
until complete
แนวทางเวชปฏิบัติการรักษาวัณโรคในผู้ใหญ่ พ.ศ. 2556 (ฉบับร่าง). สำนักวัณโรค กรมควบคุมโรค สมาคมอุรเวชช์แห่งประเทศไทย
yes no
Total treatment received
<80%<14 days ≥14 days
Continue treatment
until complete
Start over
<3 months≥3 months

Treatment for Extrapulmonary Tuberculosis
Treatment duration (months)
Lymph node 6-9
Pleura 6
Pericardium 6
Meninges and tuberculoma ≥12
Bone and joint 9-12
Urinary tract 6
Disseminated depends on the organ(s) involved

Community-acquired Pneumonia

The Disease Triangle
Host Pathogen
Environment

Airway-Lung Defense Mechanisms
Mucociliary clearance Bronchospasm Cellular/
chemical immunity
Coughing Sneezing
Mechanical barriers

Transmission and Pathogenesis
3
2
5
4
Inhalation of aerosols Aspiration of oropharyngeal secretions
Hematogenous spread
Reactivation of latent infection
Mycoplasma pneumoniae Chlamydophila pneumoniae
Legionella pneumophila Chlamydophila psittaci
Streptococcus pneumoniae Haemophilus influenzae Gram-negative bacilli
Anaerobes
Mycobacterium tuberculosis Pneumocystis jiroveci
Staphylococcus aureus Extrapulmonary bacteremias
1Direct contact & Droplets
Rhinovirus Adenovirus
Influenza virus

Community-acquired Pneumonia: Common Pathogens
Bacteria Aerobic gram-positive cocci
Aerobic gram-negative bacilli Anaerobic bacteria
“Atypical” pathogen Mycoplasma pneumoniae Legionella pneumophila
Chlamydophila pneumoniae
Viruses RSV
Adenovirus Influenza virus

Pathogen-related Severity
Outpatients (Mild) Non-ICU inpatients ICU (Severe)
S pneumoniae S pneumoniae S pneumonia
M pneumoniae M pneumoniae Legionella spp.
H influenzae C pneumoniae H influenzae
C pneumoniae H influenzae Gram-negative bacilli
Respiratory viruses Legionella spp. S aureus
Aspiration respiratory viruses P aeruginosa
File T M. Lancet 2003; 362:1991-2001.

Host Defense-modifying Conditions
Diabetes
Gram negative bacilli Melioidosis
Mucormycosis Aspergillus spp.
Candida spp.
Alcoholics Liver disease
Gram negative bacilli Anaerobes
Chronic lung disease
Gram negative bacilli P. aeruginosa Nocardia spp.
Aspergillus spp.
AIDS
Pneumocystis jirovecii Toxoplasma spp.
Rhodococcus spp. Histoplasma spp.
C. neoformans Penicillium marneffii

Diagnosis of Pneumonia
Clinical features of pneumonia
Imaging
History Fever
Cough Dyspnea
Chest pain
Physical examination Decreased lung expansion
Dullness on percussion Vocal resonance
Crepitation Tachypnea Cyanosis
New or Presumed new opacity (infiltrates) on
chest radiograph
Host responses
Tissue injuries
Airspace filling/consolidation Interstitial/reticular opacity

Pathologic-Radiographic Patterns
Inter- and intralobular septal thickening
Alveolar space filling with preserved air in bronchi
“Interstitial “Alveolar

Radiographic Patterns
Alveolar filling pattern Interstitial pattern

C U R B - 65Confusion BUN
>7 mmol/L (20 mg/dL)
Respiratory rate
≥30 bpm
Blood pressure SBP <90 mmHg DBP ≤60 mmHg
Age

CURB-65 Score and MortalityM
orta
lity
(%)
0
20
40
60
80
100
Total CURB-65 Scores0 1 2 3 4 5
1 29 15
40
57Total CURB scores:
0-1 Outpatient setting 2 Inpatient setting ≥3 ICU management
Lim WS, van der Eerden MM, Laing R, et al. Thorax 2003; 58:377–82.

Diagnostic Workups
Microbiology workups
Clinical Status workups
Sputum Gram stain
Culture for bacteria
Blood Hemoculture
BUN, CrCBC Arterial Blood Gas

Principles of Empirical Therapy
Confirmation of infection
Defining location of infection
Common pathogen(s)
Host factors
Environmental factors
Infected or suspected organ(s)
Bacteria Virus
fungus
Alternative diagnosis of
noninfectious disease?
AIDS Cirrhosis Diabetes
CKD Alcoholics
Community Hospital

Recommended Empirical Antibiotics: OPD
Previously healthy; No previous ATB use within 3 months
A Macrolide (Roxithromycin, Clarithromycin, Azithromycin)
Doxycycline
Presence of Comorbidities (chronic heart, lung, renal or liver disease, DM,
alcoholism, malignancy, aplenia, immunosuppressed) Previous ATB use within 3 months
A respiratory fluoroquinolone (Levofloxacin, Gemifloxacin, Moxifloxacin)
A beta-lactam (Amoxicillin-clavulanate, Cefdinir, Cefspan) PLUS a macrolide
Incidence of DRSP >25%
A respiratory fluoroquinolone
Mandell L A, Wunderink R G, Anzueto A, et al. CID 2007; 44:S27–72.

Recommended Empirical Antibiotics: IPD & ICU
ICU treatment
A beta-lactam (cefotaxime, ceftriaxone, or ampicillin-sulbactam) PLUS azithromycin or a respiratory FQ
Pseudomonas infection suspected
An antipneumococcal, antipseudomonal beta-lactam (piperacillin-tazobactam, cefipime, imipenem, meropenem)
PLUS either Ciprofloxacin or Levofloxacin
The above beta-lactam PLUS antipneumococcal fluoroquinolone PLUS an aminoglycoside
MRSA suspected
Add Vancomycin or linezolid
Non-ICU treatment
A respiratory floroquinolone IV A beta-lactam PLUS a macrolide IV
Mandell L A, Wunderink R G, Anzueto A, et al. CID 2007; 44:S27–72.

Supportive Treatment
Respiratory & Hemodynamic support
Drainage & Airway clearance
Chest physical therapy
Postural drainage
Coughing/huffing
Symptomatic treatment
Mucolytic/expectorants
Antipyrexia
Bronchodilators
Oxygen support: Oxygen cannula
Oxygen mask
Ventilatory support: Noninvasive
Invasive
Hemodynamic support: Noninvasive
Invasive

Treatment Modification in Host Defense Abnormalities
Diabetes
Gram negative bacilli Melioidosis
Mucormycosis Aspergillus spp.
Candida spp.
Alcoholics Liver disease
Gram negative bacilli Anaerobes
Chronic lung disease
Gram negative bacilli P. aeruginosa Nocardia spp.
Aspergillus spp.
AIDS
Pneumocystis jirovecii Toxoplasma spp.
Rhodococcus spp. Histoplasma spp.
C. neoformans Penicillium marneffii
Ceftazidime Meropenem
Amphotericin B Voriconazole
Amoxicillin-clavulanate Ceftazidime Cotrimoxazole
Cotrimoxazole Levofloxacin
Amphotericin B Itraconazole

Complications of Pneumonia
Acute respiratory failure ARDS
Pleural effusion Empyema
Lung abscess Sepsis Septic shock

Pleural Effusion

Pleural Cavity and Pleural Fluid
History of close contact to a patient with MDR-TB
Return after default of >2 months
Relapse pulmonary TB
Treatment failure (smear positive at 5th month)
Special population (immigrants, prisoners, HIV infected persons)

Pleural Effusion: Pathophysiology
Increased pleural fluid production
Decreased pleural fluid reabsorption
High hydrostaticCongestive heart failure
hepatic hydrothorax
Low oncoticCirrhosis
Hypoalbuminemia Nephrotic syndrome
Permeability/LeakagePneumonia
Inflammatory diseases Chylothorax
Lymphatic obstruction
Malignant Effusion
Pleural ThickeningComplicated parapneumonic
effusion Asbestosis
Trapped lung Rheumatoid pleurisy (late)

Diagnosis of Pleural Effusion: Chest Radiograph
Upright film: blunt costophrenic angle
fluid in fissures
Decubitus film: fluid shift to dependent area
of the lung
Supine film: fluid distributed along posterior plane
“Filter effect”

Diagnosis of Pleural Effusion: Ultrasonography
Effusion without fibrin formation Effusion with fibrin formation

Diagnosis of Pleural Effusion: CT scan
Effusion without loculation Effusion with loculation

Pleural Fluid Analysis
Specific biochemical tests
Additional test(s)
Initial biochemical tests
Protein LDH
Glucose
ADA Cholesterol Triglyceride
pH
Cytology Pathology
Tumor/inflammatory markers

Pleural Fluid Analysis: Transudate VS Exudate
Modified Light’s Criteria
Exudate Transudate
Fluid protein/serum protein ratio
>0.5 <0.5
Pleural fluid LDH
>200 IU/L or >2/3 upper limit
of normal
<200 IU/L or <2/3 upper limit
of normal
Fluid LDH/serum LDH ratio >0.6 <0.6
Additional Criteria
Exudate Transudate
Pleural fluid protein >3 g/dL <3 g/dL
Pleural fluid cholesterol >45 mg/dL <45 mg/dL
Fluid cholesterol/serum cholesterol ratio
>0.3 <0.3
Albumin gradient ≤1.2 g/dL >1.2 g/dL

Pleural Fluid Analysis: Cell Count and Differentials
Neutrophil predominated
exudates
Acute bacterial pneumonia Acute pulmonary embolism
Acute pancreatitis Rheumatoid pleurisy (acute) Tuberculous effusion (acute)
Lymphocyte- predominated
exudates
Tuberculous effusion Chylothorax Lymphoma
Rheumatoid pleurisy (chronic) Sarcoidosis
Uremic pleuritis Post surgery
Eosinophil- predominated
exudates
Pneumothorax Hemothorax
Benign asbestos Pulmonary embolism
Parasitic disease Fungal disease
Lymphoma Churg-Strauss syndrome

Pleural Fluid Analysis: Other Special Tests
Diseases Diagnostic pleural fluid tests
Empyema Present of microbial or positive culture
Malignancy Positive cytology
Lupus pleuritis Positive LE cells
Tuberculous pleural effusion Positive AFB stain, ADA >40 IU/L
Esophageal rupture Salivary amylase, pH <6.0
Chylothorax Triglyceride >110 mg/dL; positive chylomicrons
Cholesterol effusion Cholesterol >300 mg/dL; Cholesterol/triglyceride ratio >1.0, cholesterol chrystals

Pleural Fluid Analysis: Other Special Tests
Diseases Diagnostic pleural fluid tests
Hemothorax Hematocrit of pleural effusion/blood ratio >0.5
Rheumatoid pleurisy Characteristic cytology; pH <7.0, glucose <30 mg/dL, LDH >1,000 IU/L
Peritoneal dialysis Protein <1.0 g/dL, glucose >300 mg/dL
Urinothorax Creatinine of pleural fluid/serum ratio >1.0

Parapneumonic Effusion

Clinico-pathological Stage in Pleural Effusion
Exudative phase Fibropurulent phase Organizing stage
Parenchymal inflammation with neutrophilic migration
Release of IL-6, IL-8, TNF-α
Increased vascular permeability
Fluid moves into pleural space
Secondary bacterial invasioninto pleural space
Depression of intrapleural fibrinolytic activity
Fibrin formation and loculation of intrapleural fluid
Release of platelet-derived growth factors (PDGF) and transforming growth factor (TGF-β)
Proliferation of fibroblasts
Pleural scarring

Pleural Fluid Characteristics
Simple parapneumonic effusion
Complicated parapneumonic effusion Empyema
Appearance Maybe turbid Maybe cloudy Pus
Biochemical Markers
pH >7.30 LDH elevated (F/P >0.6)
Protein elevated (F/P >0.5) Glucose >60 mg/dL
pH <7.20 LDH >1000 IU/L
Glucose <35-40 mg/dLn/a
Cell differentials Neutrophil (usually <10,000/µL)
Neutrophil (usually >10,000/µL n/a
Gram stain negative negative positive
Culture negative maybe positive maybe positive

Bacteriology of Pleural Fluid Cultures
6%15%
16%
17%47%Streptococci Staphylococci
Aerobic Gram negatives
AnaerobesOthers
E. coli Klebsiella spp. P. aeruginosa
Enterobacter spp.
S. pneumoniae S. milleri
S. pyogenes
S. aureus MRSA

Management of Parapneumonic Effusion
Confirmation of pleural effusion: Chest radiograph, ultrasonography or CT
pH <7.20 LDH > 1,000 IU/L
Glucose <35 mg/dL Positive Gram stain
Positive culture
Frank pus
Thoracentesis: for pH, LDH, glucose, Gram stain, culture
Drainage
pH >7.30 LDH <1,000 IU/L
Glucose >60 mg/dL Negative microbiology
Fluid amount >1/2 hemithorax Observe
yes no

Sepsis and Septic Shock

T h e n e w e ngl a nd j o u r na l o f m e dic i n e
n engl j med 369;9 nejm.org august 29, 2013844
antiinflammatory phenotype that promotes tis-sue repair, and regulatory T cells and myeloid-derived suppressor cells further reduce inflam-mation. In addition, neural mechanisms can inhibit inflammation.35 In the so-called neuroin-flammatory reflex, sensory input is relayed through the afferent vagus nerve to the brain stem, from which the efferent vagus nerve acti-vates the splenic nerve in the celiac plexus, re-sulting in norepinephrine release in the spleen and acetylcholine secretion by a subset of CD4+
T cells. The acetylcholine release targets α7 cho-linergic receptors on macrophages, suppressing the release of proinflammatory cytokines.36 In animal models of sepsis,35 disruption of this neural-based system by vagotomy increases sus-ceptibility to endotoxin shock, whereas stimula-tion of the efferent vagus nerve or α7 cholinergic receptors attenuates systemic inflammation.
Patients who survive early sepsis but remain dependent on intensive care have evidence of im-munosuppression, in part reflected by reduced
1
Drazen
8/29/13
8/09/13
AUTHOR PLEASE NOTE:Figure has been redrawn and type has been reset
Please check carefully
AuthorFig #
Title
ME
DEArtist
Issue date
COLOR FIGURE
Draft 6Angus
Knoper
Hos
t–pa
thog
en in
tera
ctio
n
Proinflammatory response Excessive inflammation causing collateral damage (tissue injury)
Antiinflammatory response
Pathogen factors
Host factors
EnvironmentGeneticsAgeOther illnessesMedications
Load VirulencePathogen-associated molecular patterns
Immunosuppression with enhanced susceptibility to secondary infections
CytokinesProteasesReactive oxygen species Complement products
Perpetuation of inflammation
Coagulation proteases
Damage-associatedmolecular patterns
Leukocyte activation
Neuroendocrine regulation Impaired functionof immune cells
Inhibition of proinflammatory gene transcription
Complement activation Coagulation activation Necrotic cell death
NLRs
RLRs
TLRs
CLRs
Vagus nerve
Apoptosis of T, B, and dendritic cells
Antiinflammatory cytokinesSoluble cytokine receptorsNegative regulators of TLR signalingEpigenetic regulation
Brain
Celiacganglion
Liver,intestine
Norepinephrine
Acetylcholine
Spleen
Adrenalgland
Inhibition of proinflammatorycytokine production
CatecholaminesCortisol
Hypothalamic–pituitary–
adrenal axis
Expansion of regulatory T and myeloid suppressor cells
Impaired phagocytosis
Endosome
Host cell
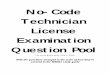
Figure 1. The Host Response in Severe Sepsis.
The host response to sepsis is characterized by both proinflammatory responses (top of panel, in red) and antiinflammatory immunosup-pressive responses (bottom of panel, in blue). The direction, extent, and duration of these reactions are determined by both host factors (e.g., genetic characteristics, age, coexisting illnesses, and medications) and pathogen factors (e.g., microbial load and virulence). In-flammatory responses are initiated by interaction between pathogen-associated molecular patterns expressed by pathogens and pattern-recognition receptors expressed by host cells at the cell surface (toll-like receptors [TLRs] and C-type lectin receptors [CLRs]), in the endosome (TLRs), or in the cytoplasm (retinoic acid inducible gene 1–like receptors [RLRs] and nucleotide-binding oligomerization domain–like receptors [NLRs]). The consequence of exaggerated inflammation is collateral tissue damage and necrotic cell death, which results in the release of damage-associated molecular patterns, so-called danger molecules that perpetuate inflammation at least in part by acting on the same pattern-recognition receptors that are triggered by pathogens.
The New England Journal of Medicine Downloaded from nejm.org on April 23, 2015. For personal use only. No other uses without permission.
Copyright © 2013 Massachusetts Medical Society. All rights reserved.

critical care medicine
n engl j med 369;9 nejm.org august 29, 2013 845
expression of HLA-DR on myeloid cells.37 These patients frequently have ongoing infectious foci, despite antimicrobial therapy, or reactivation of latent viral infection.38,39 Multiple studies have documented reduced responsiveness of blood leukocytes to pathogens in patients with sep-sis,30 findings that were recently corroborated by postmortem studies revealing strong functional impairments of splenocytes obtained from pa-
tients who had died of sepsis in the ICU.37 Be-sides the spleen, the lungs also showed evidence of immunosuppression; both organs had en-hanced expression of ligands for T-cell inhibi-tory receptors on parenchymal cells.37 Enhanced apoptosis, especially of B cells, CD4+ T cells, and follicular dendritic cells, has been implicat-ed in sepsis-associated immunosuppression and death.40,41 Epigenetic regulation of gene expres-
2
Drazen
8/29/13
7/24/13
AUTHOR PLEASE NOTE:Figure has been redrawn and type has been reset
Please check carefully
AuthorFig #
Title
ME
DEArtist
Issue date
COLOR FIGURE
Draft 6Angus
Knoper
Mic
roci
rcul
atio
nTi
ssue
Release of mitochondrial
contents
Mitochondrialdysfunction
Increased coagulation Decreased anticoagulation
Monocyte
Neutrophil
NETs with trapped
platelets
Tissuefactor
↓ Antithrombin
Endothelial cell↓Tissue
factor pathway inhibitor ↓ TM ↓ Endothelial
protein C receptor
↓ Protein C
↓ Activatedprotein C
↓ Activated protein Cand ↑ thrombin
↓Fibrinolysis↑ PAI-1
Thrombosis
Tissue hypoperfusionLoss of
barrier function
↓Tissue oxygenation
Organ failure
↑PAR1
S1P3 S1P1
↑ S1P3 and ↓ S1P1
↑ Angiopoietin 2
↓ VE cadherin and↓Tight junctions
Cell shrinkageand cell death
Capillary leak and interstitial
edema
Vasodilatation
↓ Blood pressure
↓ Red-cell deformability
Thrombus
Tissue hypoperfusion Loss of barrier function
Figure 2. Organ Failure in Severe Sepsis and Dysfunction of the Vascular Endothelium and Mitochondria.
Sepsis is associated with microvascular thrombosis caused by concurrent activation of coagulation (mediated by tissue factor) and im-pairment of anticoagulant mechanisms as a consequence of reduced activity of endogenous anticoagulant pathways (mediated by acti-vated protein C, antithrombin, and tissue factor pathway inhibitor), plus impaired fibrinolysis owing to enhanced release of plasminogen activator inhibitor type 1 (PAI-1). The capacity to generate activated protein C is impaired at least in part by reduced expression of two endothelial receptors: thrombomodulin (TM) and the endothelial protein C receptor. Thrombus formation is further facilitated by neu-trophil extracellular traps (NETs) released from dying neutrophils. Thrombus formation results in tissue hypoperfusion, which is aggra-vated by vasodilatation, hypotension, and reduced red-cell deformability. Tissue oxygenation is further impaired by the loss of barrier function of the endothelium owing to a loss of function of vascular endothelial (VE) cadherin, alterations in endothelial cell-to-cell tight junctions, high levels of angiopoietin 2, and a disturbed balance between sphingosine-1 phosphate receptor 1 (S1P1) and S1P3 within the vascular wall, which is at least in part due to preferential induction of S1P3 through protease activated receptor 1 (PAR1) as a result of a reduced ratio of activated protein C to thrombin. Oxygen use is impaired at the subcellular level because of damage to mitochondria from oxidative stress.
The New England Journal of Medicine Downloaded from nejm.org on April 23, 2015. For personal use only. No other uses without permission.
Copyright © 2013 Massachusetts Medical Society. All rights reserved.

Management of Sepsis
Component 2: Resuscitation &
Hemodynamic monitoring
Component 1: Diagnosis &
Severity assessment
Component 3: Sepsis workup &
Sepsis control
Component 4: Respiratory &
Metabolic support
Management of
Sepsis

Component 1: Diagnosis &
Severity assessment
Management of
Sepsis

Infectious VS Noninfectious Causes of Fever
Causes of FeverCauses of Fever
Infectious Noninfectious
Central Nervous System MeningitisEncephalitis
Cerebral infarction/hemorrhageSeizure
Respiratory system PneumoniaEmpyemaSinusitis
Deep vein thrombosisAtelectasisPulmonary embolism
Gastrointestinal/Hepatobiliary system Intra-abdominal abscessCholecystitis/cholangitisPeritonitis
GI hemorrhagePancreatitisIschemic colitis
Genitourinary system CystitisPyelonephritis
Skin, soft tissue, bones and joints CellulitisWound infectionSeptic arthritis
ThrombophlebitisGout/pseudogoutVasculitis

Definition
Infection Bacteremia Septicemia Sepsis
Sepsis induced
hypotension
Severe sepsis Septic shock
Presence of microbial invasion
Presence of microbes or toxin in blood
Infection PLUS SIRS
SIRS PLUS
hypotension, fluid
responsive
SIRS PLUS
≥2 organ dysfunction
severe sepsis PLUS
hypotension, fluid
irresponsive

Assessment of Severity: APACHE II Score

Assessment of Severity: APACHE II Score

Component 2: Resuscitation &
Hemodynamic monitoring
Management of
Sepsis

Early Goal-Directed Therapy (EGDT) for Septic Shock

Central Venous Pressure Measurement: Noninvasive
Phlebostatic axis

Central Venous Pressure Measurement: Invasive
Venesection“Cutdown”
Internal Jugular vein cathether
Subclavian vein catheter
Pulmonary arterycatheter
“Swan-Ganz”
Venesection “cutdown”
Internal jugular vein catheter
Subclavian vein catheter
Pulmonary artery (Swan-Ganz)
catheter

Fluid Resuscitation: Types of Solution
Crystalloid ColloidCrystalloid ColloidCrystalloid Colloid

Importance of Fluid Resuscitation
ภาวะปกติ ภาวะติดเชื้อรุนแรง ภาวะติดเชื้อรุนแรงNormal Severe Infection
Vasodilatation
Decreased vascular tension
Fluid resuscitation
Restoration of vascular tension

Fluid Resuscitation: Fluid Challenge Testing
Time CVP (cmH2O) Fluid challenge
Initial reading <15 200 mL in 15 min
≥15 50-100 mL in 15 min
During fluid challenge increase >5 cmH2O Stop and wait
Following fluid challenge increase >3 cmH2O wait
≤3 cmH2O Repeat

Fluid Resuscitation: Target
Central venous pressure (CVP) 12-15 cmH2OAND
Mean arterial pressure (MAP) ≥65 mmHg
Mean arterial pressure = [Systolic blood pressure (SBP) + 2 x Diastolic blood pressure]
3Mean arterial pressure = [Systolic blood pressure (SBP) + 2 x (Diastolic blood pressure (DBP)]
3

Vasopressor Therapy in Patients with Sepsis
Dopamine5-20 µg/kg/min
Norepinephrine0.1 µg/min
Dopamine +
Norepinephrine
+Epinephrine

Resuscitation of Microcirculation Level: Rationale
O2
CO2
Delivery
Consumption

Oxygen Delivery to Tissues
Inspired oxygen
Lung Heart pump Blood content
Oxygen delivery = 10 x Cardiac output x [(1.39 x Hb x SaO2) + (PaO2 x 0.0031)]
Pump Lung OxygenBloodcontent
Lung Heart pump Blood content
Oxygen delivery = 10 x Cardiac output x [(1.39 x Hb x SaO2) + (PaO2 x 0.0031)]
Pump Blood content
Lung Oxygen

Maximizing Oxygen Delivery to Tissues: Oxygen & Lungs
Oxygen TherapyMechanical Ventilatory
SupportOxygen Therapy
Mechanical Ventilatory
SupportOxygen therapy
Mechanical ventilatory support

Maximizing Oxygen Delivery to Tissues: Cardiac Output
Inotropic drugsincrease myocardial contractility
Dopamine 5-20 µg/kg/minDobutamine 5-15 µg/kg/min
Inotropic drugs increase myocardial contractility
Dopamine 5-20 µg/kg/min Dobutamine 5-15 µg/kg/min

Maximizing Oxygen Delivery to Tissues: Blood Content
Inotropic drugsincrease myocardial contractility
Dopamine 5-20 µg/kg/minDobutamine 5-15 µg/kg/min
Red cell transfusion increase Hb-O2 binding capacity
Keep Hct 30%


Component 3: Sepsis workup &
Sepsis control
Management of
Sepsis

Microbiological Studies in Sepsis Workup
Direct identification Culture system
Gram stain AFB stain Fluid/secretion Blood

Primary Source of Infection
Respiratory system Pneumonia
Lung abscess Empyema thoracis
Deep neck infection
KUB system Acute pyelonephritis
Acute cystitis
GU system Tubo-ovarian abscess
Pelvic infection
Skin & Soft tissue Cellulitis
Necrotizing fasciitis
GI system Acute cholangitis
Acute cholecystitis Peritonitis
CNS system Acute meningitis Acute cerebritis
Acute meningoencephalitis

Septic Workup Procedures and Specimen Collection
Lumbar puncture Thoracentesis Paracentesis ArthrocentesisLumbar puncture Thoracentesis Paracentesis Arthrocentesis

Blood Collection for Hemoculture
Catheter/device Peripheral veinCatheter/device Peripheral vein

Principles of Empirical Therapy
Confirmation of infection
Defining location of infection
Common pathogen(s)
Host factors
Environmental factors
Infected or suspected organ(s)
Bacteria Virus
fungus
Alternative diagnosis of
noninfectious disease?
AIDS Cirrhosis Diabetes
CKD Alcoholics
Community or
Hospital

Recommended Antimicrobial Therapy: Community-acquired
Infected/Suspected Organ
Respiratory Intra-abdominal Skin & soft tissue Urinary tract CNS
Common pathogens
S. pneumoniae H. influenzae
Legionella spp. C. pneumoniae
E. coli B. fragilis
S. pyogenes S. aureus
Polymicrobials
E. coli Klebsiella spp.
Proteus spp. Enterococci
S. pneumoniae N. meningitidis
L. monocytogenes H. influenzae
Recommended therapy
Ceftriaxone or cefotaxime
PLUS azithromycin
Ceftriaxone PLUS
metronidazole
Cloxacillin/Vancomycin
OR Amoxicillin-Clavulanate
Ciprofloxacin or Levofloxacin
OR Amoxycillin-clavulanate
Ceftrixone or cefipime
PLUS Ampicillin
Vancomycin

Recommended Antimicrobial Therapy: Hospital-acquired
Infected/Suspected Organ
Respiratory Intra-abdominal Skin & soft tissue Urinary tract CNS
Common pathogens
K. pneumoniae P. aeruginosa A. baumanii
MRSA
E. coli Klebsiella spp. P. aeruginosa Anaerobes
Candida spp.
S. pyogenes S. aureus
Polymicrobials
E. coli Klebsiella spp.
Proteus spp. Enterococci
S. pneumoniae N. meningitidis
L. monocytogenes H. influenzae
Recommended therapy
Imipenem Meropenem PLUS colistin
PLUS vancomycin
Imipenem Meropenem
PLUS aminoglycosides
Imipenem Meropenem
Cefipime PLUS vancomycin
Imipenem Meropenem
Cefipime PLUS vancomycin
Cefipime PLUS vancomycin
Adapted from: Simon D, Trenholme G. Crit Care Clin. 2000;16:215-230.

Host Defense-modifying Conditions
Diabetes
Gram negative bacilli Melioidosis
Mucormycosis Aspergillus spp.
Candida spp.
Alcoholics Liver disease
Gram negative bacilli Anaerobes
Chronic lung disease
Gram negative bacilli P. aeruginosa Nocardia spp.
Aspergillus spp.
AIDS
Pneumocystis jirovecii Toxoplasma spp.
Rhodococcus spp. Histoplasma spp.
C. neoformans Penicillium marneffii

Speed is Life!

Antimicrobial Therapy Delay and Mortality
Kumar A, Robers D, Wood K E, et al. Crit Care Med 2006; 34:1589-1596.
0
0.25
0.5
0.75
1
0 0.5 1 2 3 4 5 6 9 12 24 >36
Fraction of patients receiving therapyFraction of surviving patients
Time laps from recognition to the first dose of antimicrobials
Fraction of Patients
Kumar A, Robers D, Wood K E, et al. Crit Care Med 2006; 34:1589-1596.

“We recommend that intravenous antibiotic therapy be started as early as possible and
within the first hour
of recognition of septic shock and severe sepsis without septic shock.”
Surviving Sepsis Campaign: International guidelines for management of severe sepsis and septic shock: 2008

Surgical Control of Infection
Drainage Remove

Component 4: Respiratory &
Metabolic support
Management of
Sepsis

Mechanical ventilatory
support
Sedation Analgesia
Stress ulcer prophylaxis
Transfusion therapy
DVT prophylaxis
Renal replacement
Glucose control

Thank You


















![Online Internal Examination - CC3 [Mauryan & Gupta Empire]](https://img.pdfslide.net/doc/110x75/629596b279fe5a53bc3845e9/online-internal-examination-cc3-mauryan-amp-gupta-empire.jpg)








