Embed Size (px)
Citation preview

Iron Deficiency
Presenter :Purushottam Singh

Objectives•Introduction•Sources and Functions of Iron•Causes of Iron Deficiency•Effects of Iron Deficiency•Lab Findings in Iron Deficiency•Treatment of Iron Deficiency

Why a matter of concern? Anemia prevalence in Nepal In children under 5 years of age : In 1998 – 78% In 2011 – 46% Among these about 70% are under 2 years of age. In women of reproductive age group : In 1998 – 67% In 2011 – 35% Among these about 48% were pregnant women. (source: Annual health report 2011/012)

•Majority of cases are due to deficiency of IRON.• Can be prevented. So, What do they need?

Functions
1. O2 carrier – Haemoglobin Myoglobin
2. Energy production- Cytochromes (P450), Kreb’s cycle enzymes 3. Immunity- Peroxidases, Catalases

Iron is an essential trace element.
Sources Meat, fish, green leafy vegetables, cereals, pulses. Mother’s milk is a poor source.

Recommended dietary allowance (RDA)• Infants(upto 12 months)- 79 micro grams/kg• Children(1 to 3yrs)- 12mg• Children (4 to 9 yrs)- 22mg• 10 to12 yrs - 34mg(boys) 19mg(girls)• 13 to 15 yrs - 41mg(boys) 28mg(girls)• 16 to 18 yrs - 50 mg(boys) 30mg(girls)
Source: Essential Pediatrics – O.P. Ghai

Causes Of Iron Deficiency In Infants-• Low birth weight ( preterm)• Early cord clamping ( as much as 80-100ml of
blood may remain in placenta)• If there’s hemorrhage from the cord, placenta• Later: poor intake( malnutrition), parasitic
infestation• Cow’s milk – poor source and allergy may cause
occult g.i bleeding

In ChildrenDecreased intake - Malnutrition, poor source food
Decreased iron absorption
- High conc. of phytates, ca salts and rich fiber diet - Celiac disease and malabsorption syndrome - Achlorhydria

Increased iron demand- Premature and LBW infants-grow rapidly
Error of iron metabolism - congenital transferrin def ( iron not utilised for
erythropoiesis but is stored in tissues.)
Increased iron loss -Hookworm infestation -Gastrointestinal bleeding - Haemorrhage -Ulcerative colitis - dysentry

Effects of iron deficiencyFeatures of anemia:
• Pallor• Easily fatigued, breathlessness• Frequent infections
• Nails – thin brittle and flat, Koilonychia
• Pica
• Spleen enlargment (15% cases)
• Severe anaemia – cardiac enlargement, systolic and even diastolic flow murmurs, congestive cardiac failure

Reduced weight gain and growth velocityLow endurance, decreased work capabilityPoor attentiveness, poor memoryPoor academic performanceReduced leucocyte defence capacity

Lab Investigation
• Blood hemoglobin level
- will be decreased than normal range.
Male - <13 mg/dl Female - <12 mg/dl

Red cell Indices Normal range Anemia•Mean cell Volume(fl) 82-96 •Mean cell hb (pg) 27-33•Mean cell hb conc.(gm/dl) 33-37•Red cell distribution width(%) 11.5-14.5 Provides an estimate of the size differences in RBCs. Low RDW – RBCs are uniform in size High RDW – marked variation in size of RBCs
RDW = SD of RBC volume x 100 mean cell voume

•Peripheral Smear -Microcytic hypochromic anemia, decreased/normal reticulocyte count
•Plasma ferritin – decreased (<15 mcg/L)
•Serum Iron – reduced ( <30mcg/dL)
•TIBC – increased ( >350 mcg/dL)
•Transferrin saturation- markedly reduced ( <15%)

Mentzer IndexUsed to differentiate iron deficiency anemia from beta thalassemia. Mentzer index = MCV/RBC count in millions If, >13 – iron deficiency anemia is more likely <13 – beta thalassemia is more likely

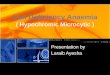
PERIPHERAL BLOOD SMEAR
Severe iron-deficiency anemia. Microcytic and hypochromic red cells smaller than the nucleus of a lymphocyte associated with marked variation in size(anisocytosis) and shape (poikilocytosis).
Normal

TREATMENT• Underlying cause to be treated.• Oral Iron therapy
• Commercially available preparations• Anhydrous ferrous sulphate(37%)• Exsiccated ferrous sulphate(30%)• Ferrous fumarate(33%)• Ferrous succinate(23%)
3-6mg of elemental iron/ kg body weight orally in three divided doses
-continued for at least 3 to 6 mths to replenish iron stores.

Parenteral iron:Iron requirements are calculated from the equation:
• 2.3 x body wt(kg) x (15- observed hb in g/dl) + 500mg( for repleting iron stores)
• Given in divided doses 1-3 mg in 150ml normal saline over 30-90min.
Blood transfusion: Considered in emergency- urgent surgery, hemorrhage,severe anaemia with congestive cardiac failure.

Prevention• Deworming• change in dietary habits• wearing shoes
• National Nutrition Program Goal is to reduce prevalence of anemia among children to less than 40% by 2017. 1)Iron tablet supplementation to pregnant and breastfeeding. 2)Multiple micronutrient powder distribution to children. 3)Deworming tablets distribution bi-annually to children.


SUMMARY• Iron is essential for ……..
• What will happen, if deficient?
• Who are at more risks?
• What do we do? Prevention and Treatment

References• Essential Pediatrics- O.P.Ghai 8th edition
• Pathologic Basis of Disease- Robbins and Cotran 8th edition
• Harper’s Biochmistry 25th edition