Embed Size (px)
Citation preview

Mini Atlas Series®
GASTROINTESTINALSURGERY

Mini Atlas Series®
GASTROINTESTINALSURGERY
S Devaji Rao MS, MNAMS, FICSTeaching Faculty, National Board of Examinations
Senior Consultant in General SurgerySurgical Gastroenterology and Surgical Oncology
St. Isabel’s Hospital and Chennai Meenakshi MultispecialityHospital, Mylapore
Harvey Multispeciality Hospital, Alwarpet,Chennai, India
®
JAYPEE BROTHERS MEDICAL PUBLISHERS (P) LTDNew Delhi • Ahmedabad • Bengaluru • Chennai • Hyderabad
Kochi • Kolkata • Lucknow • Mumbai • NagpurSt Louis (USA)

Published byJitendar P VijJaypee Brothers Medical Publishers (P) Ltd
Corporate Office4838/24 Ansari Road, Daryaganj, New Delhi-110002, India, Phone: +91-11-43574357
Registered OfficeB-3 EMCA House, 23/23B Ansari Road, Daryaganj, New Delhi-110002, IndiaPhones: +91-11-23272143, +91-11-23272703, +91-11-23282021, +91-11-23245672Rel: +91-11-32558559, Fax: +91-11-23276490, +91-11-23245683e-mail: [email protected], Website: www.jaypeebrothers.com
Branches 2/B, Akruti Society, Jodhpur Gam Road Satellite
Ahmedabad 380 015, Phones: +91-079-26926233, Rel: +91-079-32988717Fax: +91-079-26927094, e-mail: [email protected]
202 Batavia Chambers, 8 Kumara Krupa Road, Kumara Park EastBengaluru 560 001, Phones: +91-80-22285971, +91-80-22382956, Rel: +91-80-32714073Fax: +91-80-22281761, e-mail: [email protected]
282 IIIrd Floor, Khaleel Shirazi Estate, Fountain Plaza, Pantheon RoadChennai 600 008, Phones: +91-44-28193265, +91-44-28194897, Rel: +91-44-32972089Fax: +91-44-28193231, e-mail: [email protected]
4-2-1067/1-3, 1st Floor, Balaji Building, Ramkote Cross RoadHyderabad 500 095, Phones: +91-40-66610020, +91-40-24758498, Rel:+91-40-32940929Fax:+91-40-24758499, e-mail: [email protected]
No. 41/3098, B & B1, Kuruvi Building, St. Vincent RoadKochi 682 018, Kerala, Phones: 0484-4036109, +91-0484-2395739, +91-0484-2395740e-mail: [email protected]
1-A Indian Mirror Street, Wellington SquareKolkata 700 013, Phones: +91-33-22451926, +91-33-22276404, +91-33-22276415Rel: +91-33-32901926, Fax: +91-33-22456075, e-mail: [email protected]
Lekhraj Market III, B-2, Sector-4, Faizabad Road, Indira NagarLucknow 226 016, Phones: +91-522-3040553, +91-522-3040554e-mail: [email protected]
106 Amit Industrial Estate, 61 Dr SS Rao Road, Near MGM Hospital, ParelMumbai 400 012, Phones: +91-22-24124863, +91-22-24104532, Rel: +91-22-32926896Fax: +91-22-24160828, e-mail: [email protected]
“KAMALPUSHPA” 38, Reshimbag, Opp. Mohota Science College, Umred RoadNagpur 440 009 (MS), Phones: Rel: 3245220, Fax: 0712-2704275e-mail: [email protected]
USA Office1745, Pheasant Run Drive, Maryland Heights (Missouri), MO 63043, USA, Ph: 001-636-6279734e-mail: [email protected], [email protected]
Mini Atlas Series® Gastrointestinal Surgery© 2009, Jaypee Brothers Medical Publishers
All rights reserved. No part of this publication and DVD ROM should be reproduced, stored in a retrievalsystem, or transmitted in any form or by any means: electronic, mechanical, photocopying, recording, orotherwise, without the prior written permission of the author and the publisher.
This book has been published in good faith that the material provided by author is original. Every effort is madeto ensure accuracy of material, but the publisher, printer and author will not be held responsible for anyinadvertent error(s). In case of any dispute, all legal matters are to be settled under Delhi jurisdiction only.
First Edition : 2009
ISBN 978-81-8448-486-1
Typeset at JPBMP typesetting unitPrinted at Ajanta Press

Dedicatedto
My parentsMrs S Uma Bai and Dr D Siva Rao
andall my teachers


Preface
This concise book presents in-depth information of varioussurgical procedures and their complications, eachsupported by well-drawn illustrations and photographs.Many voluminous books are available which describe thesurgical procedures in detail, but rarely we see bookshighlighting the complications in a cogent and orderlymanner. Few describe them but with illustrations only andnot with supportive colour photographs. A student learnshis best, only when photographs and drawings areprovided together.
This manual should benefit not only the students ofsurgery but also all the surgeons, as every surgeon towhatever specialty he belongs to, may end up managingthe gastrointestinal tract.
If a surgeon is familiar with complications, and theirexpected days of occurrence, he or she can handle thembefore it gets complicated further. This also helps inperforming the procedures carefully averting seriouscomplications. In this book, the surgical procedures areshown in points with supportive illustrations, making themlook very simple and understandable. The student should

(viii)
understand that the procedures are not so simple as projectedin the book, but it highlights the basic principles. The studentshould also refer to operative surgery books and manualsfor details. A colour photograph manual GastrointestinalSurgery Made Easy authored by me is a good complement forthis book, which deals with the operative procedures, stepby step.
It is hoped that this carry-on-hand atlas will be of greathelp to all surgeons who deal with the gastrointestinal tract,by intention or accident.
S Devaji Rao
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY

Acknowledgements
The motivating stimulus to make this manual is fromShri Jitendar P Vij, CEO, Jaypee Brothers Medical PublishersPvt. Ltd., to whom I express my very sincere thanks. Theoffer was readily accepted by me due to the exposure andteaching I have had during my career and more so, the colourphotographs which I have collected in large numbers. Wherecolour photographs cannot support, illustrative drawingsare the only solution, and at this juncture, my very sincerethanks goes to my daughter Dr Kirthana Rao, who has putall her precious time in drawing them.
My special thanks goes to my teachers who haveimparted the knowledge, which I am able to share with mycolleagues.
I express my sincere gratitude to my colleagues,Dr A Chandrasekar Rao, Dr J Vijayan, Dr Mani Veeraghavanand Dr R Surendran for allowing me to use theirphotographs.
My family members, especially my wife, Kalpana, whohas been patient enough during my preparation of thismanual, which has stolen all my free time. My special thanksto her and my daughters for their extreme tolerance.


Contents
1. Gastrointestinal Staplers ............................................. 12. Vagotomy ....................................................................... 53. Esophageal Resection ................................................. 214. Gastrectomy and Gastrostomy .................................. 395. Small Bowel Resection ............................................. 1376. Ileostomy .................................................................... 1717. Appendicectomy ....................................................... 2078. Large Bowel Resection ............................................. 2299. Colostomy .................................................................. 255
10. Abdominoperineal Resection .................................. 28111. Anterior Resection ....................................................30112. Surgery of Liver ......................................................... 31113. Surgery of Gallbladder ............................................. 33314. Surgery of Pancreas .................................................. 36715. Surgery of Spleen ...................................................... 397
Index .................................................................................... 413
Mini Atlas Series®
GASTROINTESTINALSURGERY



(2)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
INTRALUMINAL STAPLERS
Intraluminal staplers (Fig. 1.1) apply titanium staples in adouble staggered circular pattern. As the instrument isfired, staples are driven through the enclosed tissue andformed against the anvil; at the same time, a circular bladeadvances to cut a uniform stoma between the intestines tobe anastomosed:
They can be applied for the following anastomosis:• End to end• End to side.
Various sizes are available to permit proper matchingof instrument diameter and organ lumen. They aredesigned to allow adjustment of closed staple height –from 1 to 2.5 mm, to compensate for various tissuethicknesses.
Fig. 1.1: Intraluminal stapler

(3)
CHAPTER 1: GASTROINTESTINAL STAPLERS
LINEAR STAPLERS
Linear staplers (Fig. 1.2) apply a double staggered row oftitanium staples to approximate internal tissues.
Various sizes are available for a variety of applicationsthroughout the alimentary tract.
Fig. 1.2: Linear stapler

(4)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
Fig. 1.3: Linear cutter
LINEAR CUTTER
Linear cutter (Fig. 1.3) applies two double staggered rowsof titanium staples while simultaneously dividing the tissuebetween the rows. Staple cartridges can be reloaded in theinstrument.


(6)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
HISTORY
• 1922—Truncal vagotomy for patients with ulcer diseaseby Latarjet
• 1940—Truncal vagotomy and hemigastrectomy byFarmer and Smithwick
• 1950—Various forms of vagotomy by Harkin’s group• 1960—Highly selective vagotomy by Johnston
(Fig. 2.1A), Terrence Kennedy (Fig. 2.1B), Goligher andAmdrup.
Fig. 2.1A: Johnston Fig. 2.1B: Terrence Kennedy

(7)
CHAPTER 2: VAGOTOMY
VARIETIES OF VAGOTOMIESThere are a variety of vagotomies (Fig. 2.2). They are:• Truncal vagotomy (1)• Selective vagotomy (2)• Highly selective vagotomy (3).
Fig. 2.2: Varieties of vagotomy

(8)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
INDICATIONS
• Increased acid secretion and ulcer disease (Fig. 2.3).
Fig. 2.3: Endoscopy—Chronic duodenal ulcer

(9)
CHAPTER 2: VAGOTOMY
INCISION
Upper midline (Fig. 2.4).
Fig. 2.4: Upper midline incision

(10)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
SURGICAL TECHNIQUESurgical technique of vagotomies (Fig. 2.5)1. Anterior vagotomy — identified by direct vision and
cut (1)2. Posterior vagotomy — identified by feel and cut by
direct vision (2).
Fig. 2.5: Surgical technique of vagotomies

(11)
CHAPTER 2: VAGOTOMY
NECROSIS OF LESSER CURVE (POST-VAGOTOMY)
Definition
Avascular necrosis of lesser curve of stomach.
Pathogenesis
• Exact cause is not known• Possibly inadvertent instrument injury to lesser curve
vessels.
Day of Occurrence
2nd to 3rd postoperative day.
Clinical Presentation
• Sudden upper abdominal pain• Marked tenderness and rigidity in the upper abdomen• Shock like picture.
Investigations
CT Scan and gastroscopy (Fig. 2.6) may be useful.

(12)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
Management
Resection of necrotic area and gastroenteric anastomosis.
Fig. 2.6: Esophagoscopy necrosis of lasser curve

(13)
CHAPTER 2: VAGOTOMY
ACHALASIA (POST-VAGOTOMY)
Definition
Spasm of lower esophageal sphincter.
Pathogenesis
Exact cause is not known.
Day of Occurrence
Early postoperative period.
Clinical Presentation
Difficulty in swallowing.
Investigations
• Endoscopy (Fig. 2.7) is informative• Mamometry may be useful.

(14)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
Management
No treatment is required as the recovery is spontaneous.
Fig. 2.7: Esophagoscopy—Achalasia showing retained fluid

(15)
CHAPTER 2: VAGOTOMY
POST-VAGOTOMY DIARRHEA
DefinitionLoose stools after vagotomy.
PathogenesisPathogenesis is complex (Fig. 2.8).
Fig. 2.8: Pathogenesis of post-vegotomy diarrhea

(16)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
Day of Occurrence
Months or years after vagotomy.
Clinical Presentation
Loose stools passed many times in a day.
Investigations
No specific investigation is required.
Management
Medical
• Low carbohydrate and low milk diet• Postprandial positioning of patient• Bowel binders and antispasmodics.
Surgical
• Interpositioning of antiperistaltic jejunal segment (onlywhen stools passed > 20/day).

(17)
CHAPTER 2: VAGOTOMY
REFLUX ESOPHAGITIS AND STRICTURE
Definition
Gastroesophageal reflux of gastric contents.
Pathogenesis
Injury to right crural sling fibers during esophagealmobilization.
Day of Occurrence
Days/months/years after vagotomy.
Clinical Presentation
• Upper abdominal dyspepsia• Retrosternal burning• Eructations• Chest pain.
Investigations
• Barium meal in Trendelenburg position• Endsocopy (Fig. 2.9)• Esophageal manometry• Radionuclide scan.

(18)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
Management
• H2 blockers/Proton pump inhibitors• Gastrokinetics• Dilatation for strictures.
Fig. 2.9: Esophagoscopy — Severe esophagitis

(19)
CHAPTER 2: VAGOTOMY
DYSTONY OF GALLBLADDER ANDCHOLELITHIASIS
Definition
Development of stones in the gallbladder.
Pathogenesis
Division of hepatic vagi reduce the gallbladder tone, whichproduces stasis of bile leading to gallstones.
Day of Occurrence
Months after vagotomy.
Clinical Presentation
• Upper abdominal dyspepsia• Right hypochondrial pain• Vomiting.
Investigations
• US is diagnostic in many cases• Radionuclide scan is useful in dystony of gallbladder.

(20)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
Management
Cholecystectomy for calculous cholecystitis (Fig. 2.10).
Fig. 2.10: Multiple gallstones


(22)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
HISTORY
• 1871 – Resection of cervical esophagus by Billroth(Fig. 3.1)
• 1913 – Tranhiatal esophagectomy by Denk• 1915 – Resection of thoracic esophagus for cancer by
Torek
Fig. 3.1: Christian Albert Theodor Billroth (1819 -1894)

(23)
CHAPTER 3: ESOPHAGEAL RESECTION
• 1933 – Thoracic resection with primary esophagogastricanastomosis by Ohsawa
• 1933 – Transhiatal resection with skin tube as aoesophago gastric conduit by Grey Turner
• 1938 – Transthoracic esophageal resection andreconstruction by Adams and Phemister
• 1978 – Transthoracic resection and reconstruction withdecreased morbidity and mortality by Orringer andSloan.

(24)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
ESOPHAGEAL RESECTIONS (FIG. 3.2)• Transhiatal esophagectomy• Three hole esophagectomy• Right posterolateral esophagectomy• Left thoracotomy approach.
Fig. 3.2: Approaches for esophagectomy

(25)
CHAPTER 3: ESOPHAGEAL RESECTION
RECONSTRUCTIONS AFTER RESECTIONS
• Cervical gastroesophagostomy (Stapled or handsewn)• Ivor Lewis approach (Esophagogastrostomy in the apex
of right chest)• Colonic interposition (Fig. 3.3).
Fig. 3.3: Reconstruction

(26)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
INDICATIONS
• Benign strictures of esophagus (Fig. 3.4A)• Malignancy of oesophagus (Fig. 3.4B)
Figs 3.4A and B: Barium swallow — (A) Corrosive stricture(B) Esophageal malignancy mid third

(27)
CHAPTER 3: ESOPHAGEAL RESECTION
SURGICAL TECHNIQUE
This consists of three phases (Fig. 3.5).
Abdominal Dissection• Upper midline abdominal incision• Mobilization of stomach based on the right
gastroepiploic and right gastric arteries (1)
Fig. 3.5: Surgical technique

(28)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
• Enlargement of esophageal hiatus• With downward traction on the esophagus, it is
mobilized by finger dissection• Kocher’s maneuver and pyloroplasty are necessary.
Cervical Dissection
• Left cervical incision along the anteromedial border ofsternomastoid
• Reflection of thyroid medially, sternomastoid andcarotid sheath laterally
• Blunt dissection using finger to separate the esophagusfrom the prevertebral fascia, with upward traction.The fingers from top and bottom should meet and completeness
of mobilization assessed.
Transection of Esophagus
• Transection of cervical esophagus with staples (2)• Gastroesophageal transection done with gastric tube
formation with staples (3).
Reconstruction
• Stomach is passed through esophageal bed• Esophagogastric anastomosis done in the neck (4 and
5).

(29)
CHAPTER 3: ESOPHAGEAL RESECTION
ANASTOMOTIC LEAK (POSTESOPHAGECTOMY)
Definition
Leak from anastomosis of esophagus with stomach,jejunum or colon.
Pathogenesis
Disruption of anastomosis.
Day of Occurrence
2nd to 3rd postoperative day.
Clinical Presentation
• Fever• Difficulty in breathing• Chest pain.
Investigations
• X-ray chest will show pleural collection.• Gastrograffin swallow (Fig. 3.6) may demonstrate a
leak.

(30)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
Management
Minor leak — chest drainage, delay oral intakeMajor leak — resection of necrotic part, esophagostomy andfeeding jejunostomy.
Fig. 3.6: Gastrograffin swallow — Leaking dye in anastomotic line

(31)
CHAPTER 3: ESOPHAGEAL RESECTION
DYSPHAGIA (POSTESOPHAGOENTEROSTOMY)
Definition
Difficulty in swallowing.
Pathogenesis
Edema of anastomotic area.
Day of Occurrence
2nd to 5th postoperative day.
Clinical Presentation
Difficulty in swallowing.
Investigations
• No special investigation is usually necessary• Esophagoscopy (Fig. 3.7) may be useful in later stages.

(32)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
Management
As edema subsides, it will recover.
Fig. 3.7: Esophagoscopy edema and inflammation of esophago-jejunal anastomosis

(33)
CHAPTER 3: ESOPHAGEAL RESECTION
HOARSENESS OF VOICE(POSTESOPHAGEAL SURGERY)
Definition
Change in voice.
Pathogenesis
Traction to the recurrent laryngeal nerves.
Day of Occurrence
Early postoperative period.
Clinical Presentation
Change in voice tone.
Investigations
Direct laryngoscopy (Figs 3.8A and B).
Management
Recover in due course of time.

(34)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
Fig. 3.8A: Direct laryngoscopy to assess recurrentlaryngeal nerve injury

(35)
CHAPTER 3: ESOPHAGEAL RESECTION
Fig. 3.8B: Vocal cord plasy

(36)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
PERSISTENT DYSPHAGIA(POSTESOPHAGEAL SURGERY)
Definition
Persistence of difficulty in swallowing.
Pathogenesis
• Local recurrence of malignancy• Anastomotic stricture.
Day of Occurrence
Months after surgery.
Clinical Presentation
Difficulty in swallowing.
Investigations
Endoscopy (Fig. 3.9) is diagnostic.

(37)
CHAPTER 3: ESOPHAGEAL RESECTION
Management
• Benign stricture — dilatation• Malignant stricture — surgery.
Fig. 3.9: Esophagoscopy—Malignant stricture


(40)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
HISTORY
• 1881 – First successful pylorectomy for benign ulcerdisease by Rydgier
• 1881 – First successful pylorectomy for malignancy byBillroth (Fig. 4.1)
• 1884 – First gastroenterostomy for benign ulcer diseaseby Rydgier
• 1885 – Reconstructive procedures after gastrectomydescribed by Billroth and his students
• 1914 – Posterior gastroenterostomy by Eugen Polya andReichel.
Fig. 4.1: Christian Theodor Billroth (1819-1894)

(41)
CHAPTER 4: GASTRECTOMY AND GASTROSTOMY
VARIETIES OF SURGERIES OF STOMACH ANDDUODENUM
• Gastrostomy (connect stomach to the exterior) (Fig. 4.2)
Fig. 4.2: Gastrostomy

(42)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
• Gastrectomy (excision of stomach) (Fig. 4.3)– Upper partial (excision of upper half of stomach)– Lower partial (excision of lower half of stomach)– Subtotal (excision of lower 2/3 or ¾ of stomach)– Total (excision of whole of stomach)
Fig. 4.3: Varieties of gastrectomies

(43)
CHAPTER 4: GASTRECTOMY AND GASTROSTOMY
• Gastrotomy (opening and closing the stomach)• Gastrojejunostomy (joining stomach and jejunum side
to side) (Fig. 4.4)• Pyloroplasty (relaxing procedure of pyloric sphincter)
(Fig. 4.5).
Fig. 4.4: Gastrojejunostomy and pyloroplasty

(44)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
INDICATIONS
• Ulcer disease and its complications• Gastric and duodenal malignancies (Figs 4.5 and 4.6)
Fig. 4.5: Partial gastrectomy for malignancy

(45)
CHAPTER 4: GASTRECTOMY AND GASTROSTOMY
Fig. 4.6: Total gastrectomy for malignancy

(46)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
INCISIONS
Upper midline (most popular) (Fig. 4.7).
Note: It has the advantage of:• Ease• Speed• Versatility• Allows access to stomach and duodenum• Easily extendable when needed.
Fig. 4.7: Upper midline incision

(47)
CHAPTER 4: GASTRECTOMY AND GASTROSTOMY
SURGICAL TECHNIQUE
• Good exposure of abdomen (Fig. 4.8)• Step 1 — Division of gastrohepatic ligament and entry
into and inspection of lesser sac
Fig. 4.8: Surgical procedure

(48)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
• Step 2 — Mobilization of greater curvature and markingthe line of resection on the stomach
• Step 3 — Division of left gastroepiploic vessels at themarked place
• Step 4 — Division of right gastroepiploic vessels at itsorigin from gastroduodenal artery
• Step 5 — Division of right gastric vessels• Step 6 — Division and closure of duodenum• Step 7 — Division of left gastric artery• Step 8 — Transection of stomach• Establishment of pathway by reconstruction (Fig. 4.9).

(49)
CHAPTER 4: GASTRECTOMY AND GASTROSTOMY
RECONSTRUCTION AFTER GASTRECTOMIESAfter removal of stomach, the continuity is established inmany ways (Fig. 4.9). They are:• After esophagogastrectomy, esophagogastrostomy or
esophago colostomy
Fig. 4.9: Mehtods of reconstructions after gastrectomy

(50)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
• After partial gastrectomy, end-to-end gastro-duodenostomy (Billroth I) or end-to-side gastro-jejunostomy (Billroth II)
• After subtotal gastrectomy, end-to-side gastro-jejunostomy (Billroth II)
• After total gastrectomy, end-to-side or end-to-endesophago-jejunostomy (Roux-en-Y).Whether it is removal of part of oesophagus or stomach
or to perform a side-to-side anastomosis, hand sewntechnique or stapler technique can be adopted.

(51)
CHAPTER 4: GASTRECTOMY AND GASTROSTOMY
EARLY INTRAGASTRIC HEMORRHAGE(POST-GASTRECTOMY)
Definition
Bleeding in the stomach within 48 to 72 hours after surgery.
Pathogenesis
• Bleeding from the anastomotic line• Small bleeding ulcer in the proximal gastric pouch.
Day of Occurrence
2nd to 3rd postoperative day.
Clinical Presentation
Bleeding in the nasogastric tube within 48 hours aftersurgery (Fig. 4.10).
InvestigationsNothing specific is needed.
ManagementMedical
• Ice cold saline lavage• Blood transfusions.

(52)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
Surgical
• Opening of gastric pouch above the gastroenterostomysite, evacuation of blood clots and saline irrigation
• ‘‘Figure of 8’’ stitch applied over the bleeding vessel.
Fig. 4.10: Early intragastric hemorrhage

(53)
CHAPTER 4: GASTRECTOMY AND GASTROSTOMY
DELAYED INTRAGASTRIC HEMORRHAGE(POST-GASTRECTOMY)
DefinitionBleeding in the stomach beyond 48 to 72 hours after surgery.
Pathogenesis• Bleeding from the duodenal ulcer deliberately left
behind• Bleeding from the ulcer inadequately undersewn
during the original operation.
Day of Occurrence5th to 7th postoperative day.
Clinical PresentationHematemesis and melena.
InvestigationsGastroduodenoscopy (Fig. 4.11) is informative.
ManagementMedical• Ice cold saline lavage• Blood transfusions.

(54)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
Surgical
• If the original operation is gastrojejunostomy:– Bleeding ulcer if present during original surgery in
the postbulbar duodenum, anterior duodenotomyis done and ulcer oversewn (Horsley’s slit) (Fig. 4.12).
Fig. 4.11: Late intragastric hemorrhage

(55)
CHAPTER 4: GASTRECTOMY AND GASTROSTOMY
– If the gastric chyme is to be prevented to traversethe duodenum, Billroth II reconstruction may bedone
Fig. 4.12: Horsley's slit and oversewing of ulcer

(56)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
• If the original operation is Billroth I reconstruction, itmay be revised to Billroth II or Roux-en-Yreconstruction
• If the original operation is Billroth II reconstruction,Roux-en-Y reconstruction may be done with Horsley’sslit (Fig 4.12)
• If the original operation is Billroth or Roux-en-Yreconstruction, the duodenal stump is reopened, thebleeding ulcer is transfixed and the duodenum may beclosed or a catheter duodenostomy performed
• If the original operation is pyloroplasty, antrum canbe resected with the ulcer, and reconstruction may bedone either in Billroth I, or II or Roux-en-Y fashions.

(57)
CHAPTER 4: GASTRECTOMY AND GASTROSTOMY
EXTRAGASTRIC HEMORRHAGE(POST-GASTRECTOMY)
Definition
Bleeding from sources outside the stomach (Fig 4.13).
Fig. 4.13: Extragastric hemorrhage

(58)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
Pathogenesis
• Laceration of spleen• Injury to liver by retractors• Injury to vasa brevia• Hemorrhage from pancreatic bed• Improperly secured vessel in the greater or lesser
omentum• Hemorrhage from right gastric artery and right
gastroepiploic vessels• Bleeding from the site of vagotomy or subdiaphrag-
matic vessels.
Day of Occurrence
2nd to 4th postoperative day.
Clinical Presentation
Symptoms
• General malaise.
Signs
• Tachycardia• Hypotension• Moist and clammy skin

(59)
CHAPTER 4: GASTRECTOMY AND GASTROSTOMY
• Blood in the drainage tube• Clear nasogastric aspirate.
Investigations
• Hematocrit• US or CT for collections of blood.
Management
Medical
• Blood transfusions.
Surgical
• Exploratory laparotomy if the patient does not improve• Identification of bleeding point and suturing.

(60)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
DUODENAL STUMP LEAK (BILLROTH ANASTOMOSIS)
DefinitionLeakage of duodenal contents into the peritoneal cavityfollowing Billroth II anastomosis.
Pathogenesis• Severely diseased and scarred duodenal bulb• Tissue necrosis of duodenal stump by suturing• Postoperative pancreatitis• Poor nutritional state• Localized infection and sepsis.
Day of Occurrence2nd and 5th postoperative day.
Clinical Presentation• Severe abdominal pain• Fever• Shock like syndrome.
Signs• Shock like picture• Bile in the drain.
InvestigationsCT with oral contrast.

(61)
CHAPTER 4: GASTRECTOMY AND GASTROSTOMY
Management• Adequate drainage• Nil by mouth• Nasogastric aspiration• Feeding jejunostomy to maintain nutrition• Lateral duodenostomy (Fig 4.14).
Fig. 4.14: Lateral duodenostomy for duodenal stump leakage

(62)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
GASTRODUODENOSTOMY(BILLROTH I ANASTOMOSIS) LEAK
DefinitionLeakage of duodenal contents into the peritoneal cavityafter Billroth I anastomosis.
PathogenesisSeverely diseased and scarred duodenum.
Day of Occurrence2nd and 5th postoperative day
Clinical Presentation• Subtle symptoms• Moderate degree of abdominal pain• Fever• Bile in the drain.
Investigations• Gastrograffin study• Contrast enhanced CT scan.
ManagementMedical• Nil by mouth

(63)
CHAPTER 4: GASTRECTOMY AND GASTROSTOMY
• Nasogastric aspiration• Supportive therapy.
Surgical• Small leaks – Omental patch application• Large leaks – Conversion to Billroth II or Roux-en-Y
reconstruction, (Fig. 4.15) supplemented by feedingjejunostomy.
• Lateral duodenostomy may be useful.
Fig. 4.15: Gastroduodenostomy leak

(64)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
GASTROJEJUNOSTOMY LEAK
DefinitionLeakage of gastric contents into the peritoneal cavity after:• Side-to-side gastrojejunostomy• End-to-side gastrojejunostomy.
Pathogenesis• Increased tension on the anastomotic line• Necrosis due to jeopardized blood supply.
Day of Occurrence2nd and 5th postoperative day.
Clinical Presentation• Subtle symptoms• Moderate degree of abdominal pain• Fever• Bile stained fluid in the drain.
Investigations• Gastrograffin study• Contrast enhanced CT scan.
ManagementMedical• Nil by mouth

(65)
CHAPTER 4: GASTRECTOMY AND GASTROSTOMY
• Nasogastric aspiration• Supportive therapy.
Surgical• Small leaks — Omental patch application• Large leaks
– Conversion of Gastrojejunostomy to Billroth IIanastomosis
– Billroth II to miniresection and Billroth II or Roux-en-Y reconstruction (Fig. 4.16), supplemented byfeeding jejunostomy.
Fig. 4.16: Miniresection of stomach with Roux-en-Y reconstruction

(66)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
PYLOROPLASTY LEAK
Definition
Leakage of gastric contents into the peritoneal cavity afterpyloroplasty (Fig. 4.17).
Fig. 4.17: Pyloroplasty leak

(67)
CHAPTER 4: GASTRECTOMY AND GASTROSTOMY
Pathogenesis• Edema and inflammatory reaction at pyloroplasty site.
Day of Occurrence2nd and 5th postoperative day.
Clinical Presentation• Subtle symptoms• Moderate degree of abdominal pain• Fever• Bile stained fluid in the drain.
Investigations• Gastrograffin study• Contrast enhanced CT scan
ManagementMedical• Nil by mouth• Nasogastric aspiration• Supportive therapy.
Surgical• Small leaks — Omental patch application and
gastrojejunostomy• Large leaks — Conversion to Billroth II or Roux-en-Y
reconstruction, supplemented by feeding jejunostomy.

(68)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
GASTRIC REMNANT NECROSIS(POST-GASTRECTOMY)
Definition
Necrosis of remnant of stomach.
Pathogenesis
Ischemia due to ligation of left gastric artery at its base.
Day of Occurrence
2nd to 4th postoperative day.
Clinical Presentation
• Severe abdominal pain• Fever• Shock like picture.• Dark brown fluid in the drain
Investigations
• Endoscopy• CT scan.

(69)
CHAPTER 4: GASTRECTOMY AND GASTROSTOMY
Management
Always Surgical
• Small viable proximal gastric remnant — Roux-en-Yside-to-side gastrojejunostomy (Fig. 4.18).
Fig. 4.18: Side-to-side Roux-en-Y gastrojejunostomy

(70)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
• Questionably viable entire gastric remnant — totalgastrectomy and esophagojejunostomy (Roux-en-Y)(Fig. 4.19).
Fig. 4.19: Esophagojejunostomy (Roux-en-Y)

(71)
CHAPTER 4: GASTRECTOMY AND GASTROSTOMY
• Necrosis extends to lower end of esophagus — cervicalesophagostomy + feeding jejunostomy, and colonicinterpositioning at a later date (Fig. 4.20).
Fig. 4.20: Cervical esophagostomy, jejunojejunostomy withfeeding jejunostomy

(72)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
STOMAL OBSTRUCTION (POST-GASTRECTOMY)
Definition
Obstruction of gastroduodenostomy or gastrojejunostomystoma (Fig. 4.21).
Fig. 4.21: Stomal obstruction

(73)
CHAPTER 4: GASTRECTOMY AND GASTROSTOMY
Pathogenesis
• Stomal edema• Improper surgical technique• Extensive duodenal disease• Postoperative suture line leakage• Anastomotic leakage• Acute pancreatitis• Inflammatory adhesions• Inflamed omentum.
Day of Occurrence
2nd to 4th postoperative day.
Clinical Presentation
• Excessive nasogastric aspiration
In patients whose nasogastric tube has been removed:• Abdominal discomfort and distension• Nausea and vomiting.
Investigations
After 2 weeks:• Gastrograffin study• Endoscopy.

(74)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
Management
Medical
In patients with nasogastric tube:• Maintenance of nasogastric suction• Correction of volume• Correction of electrolytesIn patients whose nasogastric tube has been removed:• Reinsertion of nasogastric tube• Correction of volume and electrolytes.
Surgical
• After Billroth I anastomosis — Dismantle gastroduode-nostomy and convert to Billroth II or Roux-en-Yreconstruction
• After Billroth II anastomosis– Kinking and adhesions — Release and feeding
jejunostomy– Herniation of loops — Reduction and preventive
measures– Non viable herniated loops — Resection and Roux-
en-Y reconstruction.

(75)
CHAPTER 4: GASTRECTOMY AND GASTROSTOMY
ACUTE AFFERENT LOOP OBSTRUCTION(POST-GASTRECTOMY)
Definition
Obstruction of afferent loop in Billroth II anastomosis.
Pathogenesis
• Twist of afferent loop (Fig. 4.22A)• Volvulus of afferent loop• Internal herniation• Jejunogastric intussusception• Kink at gastrojejunostomy site.
Day of Occurrence
2nd to 4th postoperative day.
Clinical Presentation
• Severe upper abdominal pain• Tenderness upper abdomen• Upper abdominal distension• Tachycardia• Shock like picture.

(76)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
Fig. 4.22A: Torsion of afferent loop

(77)
CHAPTER 4: GASTRECTOMY AND GASTROSTOMY
Fig. 4.22B: Gastrograffin study — Afferent loop obstruction
Investigations• Gastrograffin meal (Fig. 4.22B)• CT scan• Plain X-ray may show distended afferent loop.

(78)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
Fig. 4.23: Shortening of afferent loop and end-to-end anastomosis
Management
Exploration and treatment according to pathology:• In not seriously ill patients – if loop is kinked — shortening
of loop and end-to-end anastomosis (Fig. 4.23) or Roux-en-Y reconstruction.

(79)
CHAPTER 4: GASTRECTOMY AND GASTROSTOMY
Fig. 4.24: Simple entero-enterostomy (Duodenojejunostomy)
• In seriously ill patients– Viable but distended afferent loop — simple entero-
enterostomy (Fig. 4.24)– If the loop is gangrenous — resection of afferent loop
and Roux-en-Y reconstruction– If there is complete necrosis of afferent loop—
pancreatoduodenectomy.

(80)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
EFFERENT LOOP OBSTRUCTION(POST-GASTRECTOMY)
Definition
Obstruction of efferent loop after Billroth II anastomosis.
Pathogenesis
• Short afferent loop• Long afferent loop which may herniated behind the
efferent loop.
Day of Occurrence
4th to 7th postoperative day.
Clinical Presentation
• Nausea and vomiting• Upper abdominal pain• Epigastric fullness.
Investigations
• Gastrograffin study• CT abdomen.

(81)
CHAPTER 4: GASTRECTOMY AND GASTROSTOMY
Management
Exploration and treatment according to pathology:• If the afferent loop is long – division of afferent loop
and Roux-en-Y reconstruction (Fig. 4.25)• If efferent loop is gangrenous — excision of gangrenous
segment, division of afferent loop with end-to-endanastomosis (Fig. 4.26A) or Roux-en-Y reconstruction(Fig. 4.26B).
Fig. 4.25: Division of afferent loop and Roux-en-Y reconstruction

(82)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
Fig. 4.26A: Excision of gangrenous efferent loop and end-to-endanastomosis
Fig. 4.26B: Excision of efferent loop with Roux-en-Y reconstruction

(83)
CHAPTER 4: GASTRECTOMY AND GASTROSTOMY
INTRA-ABDOMINAL ABSCESS(POST-GASTRECTOMY)
Definition
Collection of pus in the abdominal cavity.
Pathogenesis• Spillage of intestinal contents during surgery• Anastomotic leaks• Incomplete resolution of generalized peritonitis.
Day of Occurrence1 week after surgery.
Clinical Presentation• General malaise• Fever of varying grades• Abdominal pain.
InvestigationsUS and CT are diagnostic.
Management• Small abscess — long-term broad spectrum antibiotics• Therapeutic aspiration under US or CT guidance
(Fig. 4.27).

(84)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
• Open drainage if it is inaccessible for closed aspirationor thick pus which cannot be aspirated (Fig. 4.28).
Fig. 4.27: Aspiration of intra-abdominal abscess
Fig. 4.28: Drainage of intraperitoneal abscess by laparotomy

(85)
CHAPTER 4: GASTRECTOMY AND GASTROSTOMY
POSTOPERATIVE PANCREATITIS(POST-GASTRECTOMY)
DefinitionAcute inflammation of pancreatic parenchyma.
Pathogenesis• Operative trauma to head of pancreas• Extensive dissection of supracolic compartment• Injury to pancreatic ductal system.
Day of Occurrence
3rd to 7th postoperative day.
Clinical Presentation• Restlessness• Acute upper abdominal pain• Fever• Upper abdominal tenderness• Seriously ill.
Investigations• Leucocytosis• Increased serum amylase, lipase, GGT• CT or MRI will show inflamed pancreas (Fig. 4.29).

(86)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
ManagementMedical• Nasogastric suction• Fluid and electrolyte management• Antibiotics• Somatostatin and its analogues.
Surgical• Necrosectomy• Drainage of pancreatic abscess• Cystogastrostomy for pseudocyst.
Fig. 4.29: CT - Enlarged and edematous pancreas —Acute pancreatitis

(87)
CHAPTER 4: GASTRECTOMY AND GASTROSTOMY
INADEVERTENT GASTROILEOSTOMY
Definition
Anastomosis of stomach and ileum (Fig. 4.30).
Pathogenesis
• Surgery done in extreme haste under unfavorableconditions
• Inexperienced surgeon.
Fig. 4.30: Inadvertent gastroileostomy

(88)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
Day of Occurrence
3rd to 7th postoperative days.
Clinical Presentation
• Foul belching• Profuse diarrhea• Electrolyte disturbances• Rapid weight loss• Malnutrition• Cachexia.
InvestigationsGastrograffin study will demonstrate the gastroileostomy.
ManagementMedical
Total parenteral nutrition.
Surgical• Simple gastroileostomy—vagotomy, antrectomy and
Billroth II anastomosis• Gastroileostomy (Billroth II fashion)—undo the
anastomosis, revision to Billroth II gastrojejunostomyor Roux-en-Y reconstruction.

(89)
CHAPTER 4: GASTRECTOMY AND GASTROSTOMY
ALKALINE REFLUX GASTRITIS(POST-GASTRECTOMY)
Definition
Gastritis caused by reflux of alkaline duodenal contents.
Pathogenesis
Reflux of duodenal contents (bile and pancreatic juice).
Day of Occurrence
1 week after surgery.
Clinical Presentation
• Burning sensation in epigastrium• Epigastric pain• Pain worsens on food intake• Bilious vomiting• Weight loss and anemia.
Investigations
• Gastroscopy — reflux of bile into the stomach, biopsy –gastritis picture (Fig. 4.31A)
• Scintigraphy — demonstrates reflux (Fig. 4.31B).

(90)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
Fig. 4.31A: Gastroscopy—Reflux of bile into stomach

(91)
CHAPTER 4: GASTRECTOMY AND GASTROSTOMY
Management
Medical
• H2 blockers or PPIs• Gastrokinetics.
Surgical• Billroth I or II anastomosis to be converted into Roux-
en-Y reconstruction.
Fig. 4.31B: Scintiscan — Gastroesophageal reflux

(92)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
EARLY DUMPING SYNDROME(POST-GASTRECTOMY)
Definition
Gastrointestinal and vasomotor symptoms occurringwithin 10 to 40 minutes of food intake.
Pathogenesis
• Theory I: Sudden entry of large amounts of carbohydraterich fluid in the small bowel causes fluid shift fromintravascular space to bowel lumen causing vasomotorand gastrointestinal symptoms
• Theory II: Vasoactive intestinal hormones (serotonin,gastric inhibitory polypeptide and neurotensin) causevasomotor symptoms.
Day of OccurrenceFew weeks after surgery.
Clinical PresentationGastrointestinal Symptoms
• Abdominal fullness• Crampy abdominal pain• Nausea

(93)
CHAPTER 4: GASTRECTOMY AND GASTROSTOMY
• Vomiting• Explosive diarrhea.
Vasomotor Symptoms
• Diaphoresis• Weakness• Dizziness• Flushing and palpitations.
Investigations
No specific investigation is necessary.
Management
Medical
• Changes in dietary habits• Consumption of low carbohydrate food• Restriction of extra salt.

(94)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
Surgical
• Henley’s operation: Interpositioning of jejunum betweenthe gastric remnant and duodenum (Fig. 4.32).
Fig. 4.32: Henley's operation

(95)
CHAPTER 4: GASTRECTOMY AND GASTROSTOMY
• Poth’s operation: Interpositioning of two separate isolatedjejunal segments (one isoperistaltic and the other anteperistaltic) between the gastric remnant and duodenum(Fig. 4.33).
Fig. 4.33: Poth's operation

(96)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
• Triple limb pouch operations: Three plicated jejunalsegments converted into a single receptacle betweenthe gastric remnant and duodenum or fashioned into aRoux-en-Y limb (Figs 4.34A and B)
Fig. 4.34A: Triple limb pouch

(97)
CHAPTER 4: GASTRECTOMY AND GASTROSTOMY
Fig. 4.34B: Triple limb Roux-en-Y

(98)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
Fig. 4.35: Reversed interposition
• Reversed interpositioning of jejunum: Interpositioning ofsingle reversed jejunal segment between the gastricremnant and duodenum (Fig. 4.35)

(99)
CHAPTER 4: GASTRECTOMY AND GASTROSTOMY
Fig. 4.36: Terrence Kennedy operation
• Terrence Kennedy operation: Roux-en-Y reconstructionwith interpositioning of 8 to 10 cm of reversed jejunalsegment between the gastric remnant and Roux-en-Y(Fig. 4.36).

(100)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
LATE DUMPING (POST-GASTRECTOMY)
DefinitionVasomotor symptoms occurring 20 minutes after food intake.
Pathogenesis (Fig. 4.37)• Loss of proximal receptive relaxation due to vagotomy• Loss of gastric capacity due to gastric resection• Loss of control of emptying due to pyloric ablation• Loss of duodenal feedback inhibition of gastric emptying.
Day of occurrenceMonths and years after surgery.
Clinical PresentationVasomotor symptoms• Sweating• Weakness• Palpitations• Dizziness• Flushing during postprandial period.
Gastrointestinal Symptoms – absentInvestigationsNo specific investigation is useful.

(101)
CHAPTER 4: GASTRECTOMY AND GASTROSTOMY
ManagementMedical• Frequent small quantities of food intake• Food less in carbohydrates and rich in protein.
SurgicalProcedures described in early dumping may be chosen inselect cases, but requirement is extremely rare.
Fig. 4.37: Late dumping pathogenesis

(102)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
WEIGHT LOSS (POST-GASTRECTOMY)
Definition
Loss of weight following gastric resections.
Pathogenesis (Fig. 4.38)• Stasis in long afferent loop (Billroth II)• Impaired fat absorption• Ineffective mixing of food and pancreatic juice
(pancreaticocibal asynchrony).
Day of OccurrenceMonths or years after surgery.
Clinical Presentation• Excessive weight loss• Fatigue• Pallor.
InvestigationsDecreased hematocrit.
ManagementMedical• Diet modification

(103)
CHAPTER 4: GASTRECTOMY AND GASTROSTOMY
• Consumption of balanced diet• Pancreatic enzymes.
SurgicalConversion of Billroth II to Billroth I or Roux-en-Y.
Fig. 4.38: Weight loss pathogenesis

(104)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
ANEMIA (POST-GASTRECTOMY)
Definition
Anemia could be iron deficiency or megaloblastic anemia.
Pathogenesis (Fig. 4.39)
• Decreased food intake• Decreased small bowel transit time leading to decreased
iron uptake• B12 deficiency.
Day of Occurrence
Months or years after surgery.
Clinical Presentation
• General malaise.
Investigations
• Serum iron levels are lowered in iron deficiency anemia• Serum B12 levels are lowered in megaloblastic anemia.
Management
• Iron supplements.

(105)
CHAPTER 4: GASTRECTOMY AND GASTROSTOMY
• Supplements of Vitamin B12 and folate (Inj. Cyanoco-balamin with folate tablets).
Fig. 4.39: Anemia pathogenesis

(106)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
CHRONIC GASTRIC ATONY (POST-GASTRECTOMY)
Definition
Decreased tone of gastric remnant.
Pathogenesis (Fig. 4.40)
• Gastric vagal denervation leads to loss of toniccontractions of stomach
• Delayed gastric emptying leads to gastric atony.
Day of Occurrence
Months or years after surgery.
Clinical Presentation
• Fullness and pain in epigastrium• Postprandial fullness• Nausea and vomiting.
Investigations
• Gastrograffin study• Endoscopy• Scintigraphy.

(107)
CHAPTER 4: GASTRECTOMY AND GASTROSTOMY
Management
Medical
Prokinetic drugs.
Surgical
• Vagotomy pyloroplasty — convert to antrectomy• Billroth I or Billroth II — convert to near total
gastrectomy and Roux-en-Y anastomosis.
Fig. 4.40: Gastric atony pathogenesis

(108)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
GASTRIC STASIS AND BEZOAR FORMATION(POST-GASTRECTOMY)
Definition
Bezoars are balls of undigested material:• Hair — trichobezoars• Vegetable matter — phytobezoar• Combined — trichophytobezoar.
Pathogenesis
• Vagotomy causes antral denervation resulting ininadequate drainage and gastric stasis
• Narrowing of gastroduodenostomy stoma (Billroth I)caused gastric stasis
• Gastrojejunostomy (Billroth II) ulcers can cause gastricstasis
• Jejunogastric intussusception after Billroth II can causegastric stasis.
Gastric stasis ultimately causes stagnation of material inthe gastric remnant causing bezoars.
Day of Occurrence
Months or years after surgery.

(109)
CHAPTER 4: GASTRECTOMY AND GASTROSTOMY
Clinical Presentation
• Upper abdominal pain• Abdominal distension• Vomiting.
Investigations
• Plain X-rays and contrast studies are useful• Ultrasonography is useful• Endoscopy is diagnostic (Fig. 4.41A).
Fig. 4.41A: Endoscopy — Phytobezoar

(110)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
Management
Medical
• Oral administration of gastroenterase or papain todigest the fibers
• Low fiber diet prevents a bezoar• Gastrokinetics increase the gastric emptying.
Surgical
• Small bezoars are removed by endoscope• Large bezoars need open surgical removal (Fig. 4.41B).
Fig. 4.41B: Removal trichobezoar by laparotomy

(111)
CHAPTER 4: GASTRECTOMY AND GASTROSTOMY
SMALL GASTRIC REMNANT SYNDROME(POST-GASTRECTOMY)
Definition
Complex of symptoms caused by small gastric remnant.
Pathogenesis
Small gastric remnant leads to loss of reservoir function.
Day of Occurrence
Months or years after surgery.
Clinical Presentation
• Upper abdominal fullness• Epigastric distress• Weight loss• Nutritional imbalances.
Investigations
Gastrograffin study shows gastric hurry.

(112)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
Management
Medical
• Small feeds• Enzyme supplements• Supplements of iron, vitamins for deficiencies• Antispasmodics to reduce pain and gastric motility.
Surgical
• Hunt Lawrence pouch operation (Fig. 4.42)• Tanner’s 19 reservoir operation (Fig. 4.43).
Fig. 4.42: Hunt Lawrence pouch

(113)
CHAPTER 4: GASTRECTOMY AND GASTROSTOMY
Fig. 4.43: Tanner’s 19 veservoir operation

(114)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
ROUX STASIS SYNDROME (POST-GASTRECTOMY)
DefinitionChronic postgastrectomy atony in patients who haveundergone Roux-en-Y gastroenterostomy as primaryreconstruction.
Pathogenesis• Exact pathology is not clear• Suggested theories are:
– Length of Roux limb seems to have direct correlationwith transit time
– Transection of jejunum prevents the pace setterpotential which delay the transit time
– Truncal vagotomy reduces the transit time.
Day of OccurrenceMonths or years after surgery.
Clinical Presentation• Epigastric fullness• Abdominal pain• Nausea• Vomiting• Malnutrition and weight loss.

(115)
CHAPTER 4: GASTRECTOMY AND GASTROSTOMY
Investigations
• Contrast radiography• Isotope studies• Endoscopy to rule out mechanical causes.
Management
Medical
Seldom useful.
Surgical
• Completion gastrectomy with adjustment of Roux limbto 40 cm
• Uncut Roux gastroenterostomy is useful to prevent thiscomplication (Fig. 4.44).

(116)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
Fig. 4.44: Uncut Roux operation

(117)
CHAPTER 4: GASTRECTOMY AND GASTROSTOMY
GASTRIC REMNANT CARCINOMA(POST-GASTRECTOMY)
Definition
Malignancy in the gastric remnant.
Pathogenesis
• Pathology is not clear• Suggested cause: Reflux of duodenal contents produce
deconjugation of bile salts in the presence of gastrichypoacidity.
Day of Occurrence
Years after surgery.
Clinical Presentation
• Loss of appetite and weight• Nausea• Upper abdominal pain.
Investigations
Gastroscopy is diagnostic (Fig. 4.45).

(118)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
Management
• Radical excision of gastric remnant with lymph nodedissection
• Adjuvant chemotherapy.
Fig. 4.45: Gastric remnant carcinoma

(119)
CHAPTER 4: GASTRECTOMY AND GASTROSTOMY
RECURRENT ULCER (POST-GASTRECTOMY)DefinitionUlcer in the gastric remnant.
Pathogenesis• Incomplete vagotomy• Retained antrum after Billroth II reconstruction• G cell hyperplasia• Gastrinoma• Multiple endocrine neoplasia• Long afferent loop• Ulcerogenic drugs• Gastric stasis.
Day of OccurrenceYears after surgery.
Clinical PresentationUpper abdominal pain relieved by food intake.
InvestigationsGastroscopy is diagnostic (Fig. 4.46).
ManagementMedicalPPIs or H2 blockers.

(120)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
SurgicalSurgery depends on the original operation:• Vagotomy and gastrojejunostomy — completion
vagotomy• Gastrectomy (Billroth I or II) — resection of additional
gastric tissue and Billroth II reconstruction• Vagotomy and antrectomy — resection of additional
gastric tissue and Billroth II reconstruction.Note:• Proximal gastric vagotomy is converted into truncal
vagotomy• Incomplete truncal vagotomy is converted into
complete truncal vagotomy.
Fig. 4.46: Gastroscopy — Anastomotic ulcer

(121)
CHAPTER 4: GASTRECTOMY AND GASTROSTOMY
GASTROJEJUNOCOLIC FISTULA(POST-GASTRECTOMY)
Definition
Communication between anastomosis (Gastrojejunostomyof Billroth II) and transverse colon.
Pathogenesis
Anastomotic leak may lead to abscess which may openinto adjacent colon to form a fistula (Fig. 4.47).
Fig. 4.47: Gastrojejunocolic fistula

(122)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
Day of OccurrenceMonths or years after surgery.
Clinical Presentation• Abdominal pain• Weight loss• Malnutrition• Diarrhea• Fecal belching.
InvestigationsBarium enema (Fig. 4.48) is useful in localizing the fistula.
Management
Vagotomy, distal gastrectomy with colon resectionincluding the fistula. Reconstruction is done by Billroth IIor Roux-en-Y reconstruction.

(123)
CHAPTER 4: GASTRECTOMY AND GASTROSTOMY
Fig. 4.48: Barium enema — Gastrojejunocolic fistula

(124)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
CHRONIC AFFERENT LOOP OBSTRUCTION(POST-GASTRECTOMY)
Definition
Longstanding mild obstruction of afferent loop.
Pathogenesis (Fig. 4.49)
• Long afferent loop with stasis• Volvulus or kink of long afferent loop.
Day of Occurrence
Months years after surgery.
Clinical Presentation
• Post prandial upper abdominal pain• Pain relieved by vomiting.
Investigations
• Endoscopy is useful• CECT is useful.

(125)
CHAPTER 4: GASTRECTOMY AND GASTROSTOMY
Management
Conversion of Billroth II to Billroth I or Roux-en-Yreconstruction.
Fig. 4.49: Chronic afferent loop obstruction

(126)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
CHRONIC EFFERENT LOOP OBSTRUCTION(POST-GASTRECTOMY)
Definition
Chronic obstruction of efferent loop.
Pathogenesis (Figs 4.50A and B)
• Partial or total obstruction of efferent loop• Adhesions• Internal herniation.
Day of Occurrence
Months or years after surgery.
Clinical Presentation
• Upper abdominal pain• Distension of abdomen• Vomiting (sometimes bilious).
Investigations
• Endoscopy• CECT abdomen.

(127)
CHAPTER 4: GASTRECTOMY AND GASTROSTOMY
Management
• Exploratory laparotomy• Adhesion release• Conversion of Billroth II to Roux-en-Y may be needed
rarely.
Figs 4.50A and B: Efferent loop obstruction (A) Adhesions(B) Internal herniation

(128)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
INTERNAL HERNIA (POST-GASTRECTOMY)
Definition
Herniation of small bowel between intestinal loops.
Pathogenesis
Herniation of loop of jejunum through (Fig 4.51):• A potential space in antecolic gastrojejunostomy• Two potential spaces in retrocolic gastrojejnunostomy.
Fig. 4.51: Internal herniation of jejunum

(129)
CHAPTER 4: GASTRECTOMY AND GASTROSTOMY
Day of Occurrence
Months or years after surgery.
Clinical Presentation
Acute proximal small bowel obstruction.
Investigations
• Barium meal followthrough• Upper GI endoscopy.
Management
Reduction of herniated loop, and resection if bowel isgangrenous.

(130)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
JEJUNOGASTRIC INTUSSUSCEPTION(POST-GASTRECTOMY)
Definition
Intussusception of jejunum into stomach through GJ stoma.
Pathogenesis
Reversed peristalsis of jejunum into the GJ stoma.
Day of Occurrence
Months or years after surgery.
Clinical Presentation
• Upper abdominal pain• Nausea and vomiting• Palpable firm mass in the upper abdomen.
Investigations
• Barium meal study• Upper GI endoscopy (Fig. 4.52).

(131)
CHAPTER 4: GASTRECTOMY AND GASTROSTOMY
Management
• Reduction of herniated jejunum and anchoring to theparietes
• If the bowel is non-viable, resection is required.
Fig. 4.52: Gastroscopy — Jejunogastric intussusception

(132)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
GASTROSTOMY
SURGICAL PROCEDURE
• Incision — upper midline• Picking up of anterior wall of stomach with Babcock
forceps (Fig. 4.53)• Stab wound in the anterior wall• Insertion of Malecot’s catheter• Fixing of catheter with absorbable suture• Fixing of stomach to parietal peritoneum.
Fig. 4.53: Gastrostomy surgery

(133)
CHAPTER 4: GASTRECTOMY AND GASTROSTOMY
INTRAPERITONEAL LEAK AFTER GASTROSTOMY
Definition
Leak of gastric contents into the peritoneal cavity (Fig. 4.54).
Fig. 4.54: Intraperitoneal leak

(134)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
Pathogenesis
Improper fixation of gastrostomy stomach to the parietalperitoneum.
Day of Occurrence
Early postoperative period.
Clinical Presentation
• Fever• Abdominal pain.
Investigations
US or CT will reveal the leak and perigastric collection.
Management
Laparotomy and proper fixation of stomach to parietalperitoneum.

(135)
CHAPTER 4: GASTRECTOMY AND GASTROSTOMY
EXCORIATION AND INFECTION AROUNDGASTROSTOMY STOMA
Definition
Excoriation and damage of skin around the stoma.
Pathogenesis
Regurgitation of acidic gastric contents around the tubeon to the skin.
Day of Occurrence
Anytime after surgery.
Clinical Presentation
Pain and seropurulent discharge around the stoma(Fig. 4.55).
Investigations
No special investigation is required.

(136)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
Management
• Local skin care around the tube• Antibiotics• Replacement of gastrostomy tube.
Fig. 4.55: Discharge and excoriation around gastrostomy stoma


(138)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
HISTORY
• 1920 – Discovery of non-crushing intestinal twin clampsfor resection by Lane (Fig. 5.1).
Fig. 5.1: Sir William Arbuthnot Lane (1856-1943)

(139)
CHAPTER 5: SMALL BOWEL RESECTION
INDICATIONS• Obstructive lesions (strictures, tumors, intussusception)
(Figs 5.2A and B)• Strangulations with non-viable bowel.
Fig. 5.2A: Ileo ileal intussusception
Fig. 5.2B: Lipoma the cause of ileo ileal intussusception

(140)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
INCISION
• Midline (most popular) (Fig. 5.3).Note: It has the advantage of:• Ease• Speed• Versatility• Allows access to all quadrants• Easily extendable when needed.
Fig. 5.3: Midline incision

(141)
CHAPTER 5: SMALL BOWEL RESECTION
VARIETIES OF SURGERIES OF SMALL BOWEL
Varieties of small bowel surgeries (Fig. 5.4) are:• Resection and establishment of continuity (hand sewn
or stapled anastomosis)• Bypass procedures (hand sewn or stapled anastomosis)
without resections• Diversion procedures (ileostomies).
Fig. 5.4: Varieties of surgeries

(142)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
TYPES OF SMALL BOWEL ANASTOMOSIS
The types of small bowel anastomosis (Fig. 5.5) are:• End-to-end• End-to-side• Side-to-side.
Fig. 5.5: Types of small bowel anastomoses

(143)
CHAPTER 5: SMALL BOWEL RESECTION
SURGICAL TECHNIQUE
Hand Sewn Technique (Fig. 5.6)
Step 1 : Marking the lines of resection and control of vesselsin the mestentery.
Fig. 5.6: Surgical technique

(144)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
Step 2 : Division of bowel at marked places betweenclamps.
Step 3 : Anastomosis to establish continuity.
• Double layer anastomosis– Posterior outer row first (seromuscular) with non-
absorbable material– Posterior inner row next (running full thickness) with
absorbable material– Anterior inner row in continuity from the posterior
inner row– Anterior outer row last (seromuscular) with non-
absorbable material.Note:• Inverting anastomosis causes serosa to serosa
apposition• Inversion of mucosa reestablishes integrity of lumen
preventing leakage.

(145)
CHAPTER 5: SMALL BOWEL RESECTION
END-TO-END ANASTOMOSIS (STAPLED)
Method of stapled end-to-end anastomosis (Fig. 5.7)• Bowel is cleared about 1 cm from the cut margin• Gun is introduced into the proximal gut through
enterotomy• Proximal and distal ends each require a purse string
suture• The purse string sutures are snugged down over the
instrument ends (Fig. 5.7A)
Fig. 5.7A: End-to-end anastomosis (Staped technique)

(146)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
• Anvil and head are brought together• Firing is done for application of staplers• The screw mechanism is unwound for a quarter of turn
to release the bowel• After removal of instrument, doughnuts (Fig. 5.7B) are
checked for integrity• Enterotomy is closed with sutures or a linear stapler.
Fig. 5.7B: Doughnuts

(147)
CHAPTER 5: SMALL BOWEL RESECTION
END-TO-SIDE ANASTOMOSIS (STAPLED)
Method of stapled end-to-side anastomosis (Fig. 5.8)• The gun is introduced in the bowel to have end
anastomosis (enterotomy)
Fig. 5.8: End-to-side anastomosis (Stapled technique)

(148)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
• Purse string suture is made and snugged down overthe anvil
• A small incision is made in the bowel to have sideanastomosis
• The head assembly is introduced through the openingand held
• Anvil and head are brought together• Firing is done for application of staplers• The screw mechanism is unwound for a quarter of turn
to release the bowel• After removal of instrument, doughnuts are checked
for integrity• Enterotomy is closed with sutures or a linear stapler.

(149)
CHAPTER 5: SMALL BOWEL RESECTION
SIDE-TO-SIDE ANASTOMOSIS (STAPLED)
The method of stapled side-to-side anastomosis (Fig. 5.9)• Liner cutter is used for this anastomosis• The two guts which are to be anastomosed are laid
together side by side
Fig. 5.9: Side-to-side anastomosis (Stapled technique)

(150)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
• Small holes are made in each tube for introduction ofstapler jaws
• The forks are introduced through these enterotomies• The forks are locked together• Stapler is activated, so that the anastomosis is made
with stapling• The forks are separated and removed• The enterotomy openings are closed with sutures or a
linear stapler.

(151)
CHAPTER 5: SMALL BOWEL RESECTION
ANASTOMOTIC LEAKAGE(INTESTINAL ANASTOMOSIS)
Definition
• Leakage of intestinal contents through the anastomoticline.
Pathogenesis
• Inadequate bowel preparation• Poor blood supply to both ends of bowel• Tension on the anastomosis
Day of Occurrence
2nd to 5th postoperative day.
Clinical Presentation
• Abdominal pain• Fever• Leakage of intestinal contents through the drain
(Fig. 5.10).
InvestigationsNo special investigation is necessary.

(152)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
Management• Nil by mouth• Intravenous fluids• Intravenous broad spectrum antibiotics• Replacement of fluids, calories and electrolytes• Minor leaks heal, larger leaks take a longer time• If fistula is formed, it may heal over a period of time• Some may require surgery, after 6 to 12 weeks.
Fig. 5.10: Anastomotic leakage

(153)
CHAPTER 5: SMALL BOWEL RESECTION
HEMORRHAGE (INTESTINAL ANASTOMOSIS)
Definition
• Bleeding from the anastomotic line (Fig. 5.11).
Fig. 5.11: Hemorrhage

(154)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
Pathogenesis
• Bleeding from a marginal vessel due to improperapplication of staplers or hemostatic full thicknesssutures.
Clinical Presentation
Bleeding per rectum or melena.
Reason
Improper application of staplers.
Day of Occurrence
2nd to 3rd postoperative day.
Investigations
No specific investigation is necessary, as the bleeding isusually minor.
Management
Majority of bleeding stops without treatment.

(155)
CHAPTER 5: SMALL BOWEL RESECTION
INTRA-ABDOMINAL ABSCESS(POST INTESTINAL ANASTOMOSIS)
Definition
Collection of pus in the peritoneal cavity (Fig. 5.12).
Pathogenesis
Spillage of bowel contents into the peritoneal cavity,leading to abscess formation.
Fig. 5.12: Intra-abdominal abscesses

(156)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
Clinical Presentation
• General malaise• Hyperpyrexia of varying grades• Insignificant clinical examination.
Day of Occurrence
7th to 10th postoperative days.
Investigations
Ultrasonography and CT are useful in localizing abscess.
Management
Medical
• Small abscesses resolve with antibiotics.
Surgical
• Drainage of abscess under US or CT guidance (seeFig. 4.27)
• Open drainage if abscess is large and pus is thick(see Fig. 4.28).

(157)
CHAPTER 5: SMALL BOWEL RESECTION
ANASTOMOTIC STRICTURE(INTESTINAL ANASTOMOSIS)
Definition
• Narrowing of lumen of anastomotic area (Fig. 5.13).
Fig. 5.13: Stricture

(158)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
Pathogenesis
• Healing of a circular anastomosis results in a stricture.
Day of Occurrence
Months or years after surgery.
Clinical Presentation
• Constipation• Abdominal pain• Vomiting• Abdominal distension.
Investigations
Contrast studies may be useful.
Management
• Small bowel strictures are bypassed or resectionanastomosis done.
Note:• Strictures following stapler usage is rare, if the correct
size is chosen.

(159)
CHAPTER 5: SMALL BOWEL RESECTION
ADHESIONS (INTESTINAL SURGERY)
Definition
Adherence of bowels between themselves or with theparietes (Fig. 5.14).
Pathogenesis
• Postoperative fibrinous adhesions result from thehealing of local inflammatory processes in the operatedarea
Fig. 5.14: Intra-abdominal adhesions

(160)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
• Resolved infections of peritoneum can causeadhesions.
Clinical Presentation
• Recurrent attacks of abdominal pain• Vomiting• Constipation• Abdominal distension.
Days of Occurrence
Months–years after surgery.
Investigations
X-rays of abdomen will show distended bowel.
Management
Medical
• Nil by mouth• Intravenous fluids and electrolytes.
Surgical
• If medical management fails, adhesiolysis by open orlaparoscopic methods.

(161)
CHAPTER 5: SMALL BOWEL RESECTION
INTERNAL FISTULAE (INTESTINAL ANASTOMOSIS)
Definition
Communication between anastomotic line of small bowelwith adjacent hollow viscera (Fig. 5.15).
Fig. 5.15: Internal fistulae

(162)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
Pathogenesis
• Anastomotic leak leads to collection of pus which inturn erode into the adjacent viscera
• Inflammatory bowel disease.
Clinical Presentation
• Generally asymptomatic• Recurrent urinary tract infections can occur in
vesicoenteric fistulae.
Days of Occurrence
Months after surgery.
Investigations
Contrast studies are useful.
Management
• Entero-enteric fistulae do not require any treatment• Vesico-enteric fistulae require excision.

(163)
CHAPTER 5: SMALL BOWEL RESECTION
EXTERNAL FISTULAE(INTESTINAL RESECTION)
DefinitionLeakage of intestinal contents through fistulae to the exterior.
Pathogenesis• Anastomotic leak leads to collection of pus which in
turn drains through the drainage tube• Intentional external drainage of collection of pus from
the anastomotic leak• Inflammatory bowel disease.
Clinical Presentation• Has had a turbulent postoperative period• Discharging wound in the postoperative period• Fluid and electrolyte disturbances• Skin excoriation around the fistulous opening
(Fig. 5.16A)• Fever• Malnutrition, especially if large segments are lost during
surgery.
Days of OccurrenceMonths after surgery.

(164)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
Investigations• Oral administration of non-absorbable marker (charcoal
or congo red)• Fistulogram (Fig. 5.16B)• US, CT with contrast or isotope scanning are useful.
ManagementMedical• Total parenteral nutritionMost lateral fistulae heal spontaneously
Fig. 5.16A: Multiple enterocutaneous fistulae

(165)
CHAPTER 5: SMALL BOWEL RESECTION
Surgical
Excision of fistulaIndicated when there is:• Evidence of obstruction• Active disease• Interruption of bowel continuity• Closure not occurred by 6 weeks.
Fig. 5.16B: Fistulogram — Ileocutaneous fistula

(166)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
NUTRITIONAL DEFICIENCIES
DefinitionDeficiency of nutritional factors secondary to surgery.
Pathogenesis (Fig. 5.17)• Stagnation of intestinal contents• Stricture
Fig. 5.17: Nutritional deficiencies pathogenesis

(167)
CHAPTER 5: SMALL BOWEL RESECTION
• Stenosis• Fistulae• Blind pouch formation• Diverticulae.
Clinical Presentation• Diarrhea• Steatorrhea• Anemia• Weight loss• Abdominal pain• Multiple vitamin deficiency symptoms.
Days of OccurrenceMonths or years after surgery.
Investigations• Variety of laboratory investigations may be required.
ManagementMedical
• Supplement of deficient factors.
Surgical• Stenosis, stricture and diverticulae need surgical excision.

(168)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
SHORT BOWEL SYNDROME
Definition
Symptom complex caused by short loop of bowel.
Pathogenesis (Fig. 5.18)
Results due to massive resections of small bowel:• Vit B12 deficiency (Resection of terminal ileum)• Water and electrolyte disturbances (resection of large
segment of ileum)• Fat malabsorption (resection of large segment of ileum).
Clinical Presentation
Severe emaciation.
Days of Occurrence
Months after surgery.
Investigations
Variety of laboratory investigations.

(169)
CHAPTER 5: SMALL BOWEL RESECTION
Management
• Fat restriction• Drugs to slow intestinal motility• Oral bile salts• Intravenous hyperalimentation.
Fig. 5.18: Short bowel syndrome — Pathogenesis


(172)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
HISTORY• 1879 – First recorded ileostomy by Baum• 1941 – Skin graft on the serosal surface of projecting
ileum by Dragstedt• 1951 - Projecting 5 cm of ileum and allowing to granulate
by Warren and McKittrick• 1952 – Projecting ileum covered by pedicle of skin from
abdominal wall• 1952 – Immediate suture of bowel to skin by Butler• 1952 – Turning back of ileum to the skin of abdomen by
Brooke (Fig. 6.1)• 1953 – Removal of serosa and muscular coats before
suturing by Turnbull.
Fig. 6.1: Bryan Nicholas Brooke (1915-1998)

(173)
CHAPTER 6: ILEOSTOMY
TYPES OF ILEOSTOMY
There are three types of ileostomy (Fig. 6.2A). They are:1. End ilesotomy2. Loop ileostomy3. Loop end ileostomy.
Fig. 6.2A: Types and indications

(174)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
INDICATIONS FOR ILEOSTOMY
End Ileostomy
• After completion of total colectomy or proctocolectomy(Fig. 6.2B)
• As a temporary procedure in inflammatory boweldisease
• While constructing an ileal conduit for urinarydiversion.
Fig. 6.2B: Total colectomy for multiple polyposis coli

(175)
CHAPTER 6: ILEOSTOMY
Loop Ileostomy
• Above an ileal pouch anal anastomosis fordefunctioning
• Above a continent ileal reservoir• Proximal to enterocutaneous fistula• As an alternative to colostomy when it is difficult.
Loop end Ileostomy
• As a primary procedure for the definitive stoma of ilealurinary conduits.

(176)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
SURGICAL PROCEDURESurgical procedure of end ileostomy (Fig. 6.3):• A circular opening of 2 cm is made in the abdominal
wall at the site of ileostomy (1)• A loop of small intestine or terminal ileum is selected• The small intestine is brought out through the opening (2)• The bowel is fixed to the parietal peritoneum to prevent
recession.• The free end of the bowel is inverted and sutured to border
of abdominal opening with absorbable material (3).
Fig. 6.3: Surgical procedure

(177)
CHAPTER 6: ILEOSTOMY
HEMORRHAGE FROM ILEOSTOMY
Definition
Bleeding from the ileostomy (Fig. 6.4).
Fig. 6.4: Hemorrhage

(178)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
Pathogenesis
Bleeding from the mucosal vessels over the ileostomy.
Day of Occurrence
2nd to 3rd postoperative day.
Clinical Presentation
Blood staining of the ileostomy ouput.
Investigations
No special investigation is necessary.
Management
Application of adrenaline soaked gauze.

(179)
CHAPTER 6: ILEOSTOMY
MUCOSAL SLOUGH OF ILEOSTOMY
Definition
Sloughing of mucosa of ileostomy (Fig. 6.5A).
Fig. 6.5A: Mucosal slough of ileostomy

(180)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
Pathogenesis
Avascular necrosis due to tight appliance flange.
Day of Occurrence
2nd to 3rd postoperative day.
Clinical Presentation
Sloughed ulcer area on the ileostomy.
Investigations
No special investigation is necessary.
Management
Medical
• If the flange of the appliance is tight, it needs to bechanged
• Minor slough needs no treatment.

(181)
CHAPTER 6: ILEOSTOMY
Fig. 6.5B: Excision of mucosal slough
Surgical
• If the sloughing is patchy, excision (Fig. 6.5B) is done• If it is circumferential, revision surgery is required.

(182)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
PARASTOMAL SKIN IRRITATION
Definition
Irritation of skin around the ileostomy stoma (Fig. 6.6).
Fig. 6.6: Parastomal skin irritation

(183)
CHAPTER 6: ILEOSTOMY
Pathogenesis
• Allergy to pouch adhesives• Allergy to adhesive tapes• Candidiasis• Follliculitis• Trauma due to frequent pouch changes• Eczema.
Day of Occurrence
3rd to 5th postoperative day.
Clinical Presentation
Erythematous or ulcerative skin around the stoma,sometimes bleeding.
Investigations
No special investigation is necessary.
Management
• Treatment of dermatological lesion• Modification of appliance.

(184)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
PARAILEOSTOMY ULCERATION
Definition
Ulceration around the ileostomy.
Pathogenesis• Causes of skin irritation• Neglected cases of irritation may lead to ulceration.
Day of Occurrence
3rd to 7th postoperative day.
Clinical Presentation
Ulcerations around the ileostomy (Fig. 6.7).
Investigations
Evaluation of diabetes is required.
Management
• Local skin care• Debridement of slough over the ulcers• Non-seal, nonadhesive appliance is useful• Conventional pouch may be used till the ulcer heals.

(185)
CHAPTER 6: ILEOSTOMY
Fig. 6.7: Paraileostomy ulceration

(186)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
ILEOSTOMY OBSTRUCTION
DefinitionObstruction of ileostomy.
Pathogenesis• Edema of stoma• Adhesions• Volvulus• Entrapment of ileum in the fascial closure• Food bolus obstruction.
Day of Occurrence
Early postoperative period.
Clinical Presentation
• Edematpis ileostomy stoma (Fig. 6.8)• Abdominal pain• Vomiting• Abdominal distension• Diminution of ileostomy output.
InvestigationsPlain X-ray may show air fluid levels.

(187)
CHAPTER 6: ILEOSTOMY
ManagementMedical
Irrigation of ileostomy, till returns are clear.
SurgicalIf mechanical obstruction is identified, laparotomy maybe required.
Fig. 6.8: Ileostomy obstruction

(188)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
STENOSIS OF ILEOSTOMY
Definition
Narrowing of ileostomy stoma (Fig. 6.9A).
Fig. 6.9A: Stenosis of ileostomy

(189)
CHAPTER 6: ILEOSTOMY
Pathogenesis
• Healing of circular ulceration of mucocutaneousjunction
• Tight opening in the abdominal wall while creating thestoma.
Day of Occurrence
Months after surgery.
Clinical Presentation
Small ileostomy stoma.
Investigations
No special investigation is necessary.
Management
Medical
Dilatation with fingers or metal dilators (Fig. 6.9B).
Surgical
Local repair (mobilization of terminal ileum andrefashioning) (Fig. 6.9C).

(190)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
Fig. 6.9B: Dilatation of stenosis of ileostomy with (I) Finger (II) Dilator
Fig. 6.9C: Operative treatment of ileostomy stenosis

(191)
CHAPTER 6: ILEOSTOMY
RECESSION OF ILEOSTOMY
Definition
Pulling in of the ileostomy (Fig. 6.10A).
Pathogenesis• Too large opening in the abdominal wall• Inadequate fixation of ileum at the fascial plane.
Fig. 6.10A: Recession of ileostomy

(192)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
Day of OccurrenceMonths after surgery.
Clinical Presentation• Soiling of peristomal skin• Skin changes may be evident• Stoma appears pulled into the abdomen.
InvestigationsNo special investigation is necessary.
ManagementLocal repair (mobilization of terminal ileum andrefashioning) (Fig. 6.10B).
Fig. 6.10B: Operative treatment of ileostomy recession

(193)
CHAPTER 6: ILEOSTOMY
PROLAPSE OF ILEOSTOMY
Definition
Prolapse of ileostomy more common with loop ileostomy(Fig. 6.11A).
Pathogenesis
Long loop of small bowel fashioned outside the skin forcreation of ileostomy.
Fig. 6.11A: Prolapse of (I) End ileostomy (II) Loop ileostomy

(194)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
Day of OccurrenceMonths after surgery.
Clinical Presentation• Stoma appears very much above the surface of skin• Mucosa may get ulcerated recurrently, caused by the
appliance.
InvestigationsNo special investigation is necessary.
ManagementLocal repair (detachment of mucocutaneous junction,reduction of everted stoma, amputation of excess lengthand refashioning) (Fig. 6.11B).
Fig. 6.11B: Operative treatment of ileostomy prolapse

(195)
CHAPTER 6: ILEOSTOMY
PARASTOMAL HERNIA
Definition
Herniation of intra-abdominal contents anywhere aroundthe stoma (Fig. 6.12A).
Pathogenesis
• Opening in the abdominal wall very large• Patulous abdominal wall.
Fig. 6.12A: Paraileostomy hernia

(196)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
Day of Occurrence
Months after surgery.
Clinical Presentation
Swelling in the parastomal regionAbdominal or local pain, if obstruction occurs.
Investigations
No special investigation is necessary.
Management
• Local repair (detachment of stoma, with the help ofincision hernial sac is identified, reduced andrefashioning of stoma) (Fig. 6.12B)
• Skin may be closed by ‘Mercedes repair’ (Fig. 6.12C).
Fig. 6.12B: Operative repair of parastomal hernia

(197)
CHAPTER 6: ILEOSTOMY
Fig. 6.12C: Mercedes repair of parastomal hernia

(198)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
EXCESSIVE LENGTH OF ILEOSTOMY STOMA
Definition
Long length of ileum above the skin surface, common afterend ileostomy.
Pathogenesis
Fashioning of long length of ileum above the skin surface.
Day of Occurrence
Months after surgery.
Clinical Presentation
• Long overhanging length of ileum• May ulcerate due to appliance.
Investigations
No special investigation is necessary.

(199)
CHAPTER 6: ILEOSTOMY
Management
Local repair (detachment of mucocutaneous junction,reduction of everted stoma, amputation of excess lengthand refashioning) (Fig. 6.13).
Fig. 6.13: Operative treatment of excessive length of ileostomy

(200)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
PARASTOMAL ABSCESS
Definition
Abscesses in the area around the ileostomy (Fig. 6.14).
Fig. 6.14: Parastomal abscess

(201)
CHAPTER 6: ILEOSTOMY
Pathogenesis
• Mucocutaneous suture line breaks• Infection of hematoma.
Day of Occurrence
Months after surgery.
Clinical Presentation
Painful swellings around the stoma.
Investigations
• No special investigation is necessary• Diabetes may have to be evaluated.
Management
Drainage of abscess.

(202)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
ILEOTOMY FISTULA
Definition
Fistulous opening anywhere around the ileostomy.
Pathogenesis
Suturing of bowel wall to the rectus fascia by deeper full-thickness stitch.
Day of Occurrence
Months after surgery.
Clinical Presentation
Leakage of purulent material anywhere around theileostomy.
Investigations
Fistulogram may be useful.
Management
• If the fistulous opening is close to stoma, no treatmentis required

(203)
CHAPTER 6: ILEOSTOMY
• If the fistulous opening is far from the stoma, theappliance may be made to include the fistula in theappliance.
• If the fistulous opening is very far from the stoma, andcannot be included in the appliance, bistulectomy(Fig. 6.15) is the the treatment of choice.
Fig. 6.15: Operative treatment of paraileostomy fistula

(204)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
PARAILEOSTOMY GRANULOMA
Definition
Reddish swelling around the ileostomy (Fig. 6.16).
Fig. 6.16: Parastomal granuloma

(205)
CHAPTER 6: ILEOSTOMY
Pathogenesis
• Long standing skin irritation• Neglected cases of irritation may lead to ulceration and
granuloma.
Day of Occurrence
Months after surgery.
Clinical Presentation
Painful reddish swellings around the ileostomy.
Investigations
• Evaluation of diabetes is required• Dermatological causes have to be assessed.
Management
• Excision of granuloma.


(208)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
HISTORY
• 1736 – First appendicectomy by Caludius Amyand• 1848 – Drainage of appendix abscess by Hancock• 1887 – Appendicectomy for gangrenous appendix by
Tait• 1889 – Muscle splitting incision for appendicectomy by
McBurney (Fig. 7.1)• 1977 – First laparoscopic appendicectomy by DeKok.
Fig. 7.1: Charles McBurney

(209)
CHAPTER 7: APPENDICECTOMY
INDICATIONS
• Acute appendicitis (Fig. 7.2 A)• Chronic appendicitis (Fig. 7.2 B)• Tumors of appendix.
Fig. 7.2A: Acute suppurative appendicitis (note the pus in the cup)

(210)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
Fig. 7.2B: Appendix with fecoliths

(211)
CHAPTER 7: APPENDICECTOMY
INCISIONS
Incision for appendicectomy (Fig. 7.3)• McBurney’s incision (Most popular)• Lanz incision• Right lower paramedian incision.
Fig. 7.3: Incisions for appendicectomy

(212)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
SURGICAL TECHNIQUE
Surgical technique of appendicectomy (Fig. 7.4)
Position: Supine
• Identifying the appendix• Appendix is picked-up with the fingers
Fig. 7.4: Appendicectomy surgery

(213)
CHAPTER 7: APPENDICECTOMY
• Appendix is held with Babcock’s forceps upwards• Appendicular artery identified in the mesoappendix• Appendicular artery divided between ligatures (1)• Appendix is crushed at its base• Clamp applied at the crushed site, and advanced
distally• Ligature applied at the crushed site with absorbable
material• Appendix is divided between the suture and the clamp,
and removed (2)• Purse string sutured on the cecum and appendicular
stump buried (3).

(214)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
HEMORRHAGE FROM APPENDICULAR STUMP
Definition
Bleeding in the abdominal cavity (Fig. 7.5).
Fig. 7.5: Hemorrhage

(215)
CHAPTER 7: APPENDICECTOMY
Pathogenesis
• Leakage of blood from the appendicular stump• Slipped ligature of the appendicular artery.
Day of Occurrence
2nd to 3rd postoperative day.
Clinical Presentation
• Severe lower abdominal pain• Guarding in right iliac fossa.
Investigations
US and CT may be contributory.
Management
Exploration of abdomen and ligation of mesoappendix.

(216)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
PARALYTIC ILEUS
Definition
Delayed recovery of intestinal movements.
Pathogenesis
• Peritonitis• Electrolyte disturbances (hypokalemia).
Day of Occurrence
2nd to 5th postoperative day.
Clinical Presentation
• Vomiting• Abdominal distension• Constipation.
Investigations
X-ray abdomen (Fig. 7.6) shows distended loops of smallbowel (Step ladder pattern).

(217)
CHAPTER 7: APPENDICECTOMY
Management
• Correction of electrolytes• Nasogastric aspiration.
Fig. 7.6: X-ray — Step ladder pattern of paralytic ileus

(218)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
WOUND INFECTION AFTER APPENDICECTOMY
Definition
Infection of operative wound, may vary from mild to floridinfection.
Pathogenesis
• Spillage of infected appendicular contents• Extension of infection from appendix to abdominal
wall.
Day of Occurrence
2nd to 5th postoperative day.
Clinical Presentation
• Fever• Discharge from wound (Fig. 7.7)• Pain in the wound.
Investigations
Pus culture to identify the incriminating organisms.

(219)
CHAPTER 7: APPENDICECTOMY
Management
• Drainage of collection of abscess• Appropriate antibiotics• Wound care.
Fig. 7.7: Wound infection (appendicectomy)

(220)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
PELVIC/PARACOLIC ABSCESS
Definition
Collection of pus in the region adjacent to cecum or pelviccavity.
Pathogenesis
• Spillage of appendicular contents• Incomplete resolution of generalized peritonitis.
Day of Occurrence
5th to 7th postoperative day.
Clinical Presentation
• Abdominal pain• High grade fever• Constipation.
Investigations
US and CT (Fig. 7.8) are diagnostic.

(221)
CHAPTER 7: APPENDICECTOMY
Management
• Drainage under US or CT guidance or open method• Appropriate antibiotics.
Fig. 7.8: CT — Paracolic abscess

(222)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
RUPTURE OF STUMP AND APPENDICOCUTANEOUS
Definition
Dehiscence of appendicular stump.
Pathogenesis• Sloughing of appendicular stump• Administration of enema in the postoperative period• Fistula may form spontaneously or after surgical
drainage.
Day of Occurrence
3rd to 5th postoperative day.
Clinical Presentation
• Right lower quadrant pain• Vomiting• Tenderness at the operated area• Constipation• Discharging fistula (Fig. 7.9).
Investigations
• US may be useful in localizing abscess• Fistulogram is useful.

(223)
CHAPTER 7: APPENDICECTOMY
Management
Medical
• Antibiotics• Drainage of collection (appendicocutaneous fistula may
result).
Surgical
• Cecostomy will prevent further spillage• Fistula has to be excised.
Fig. 7.9: Appendicocutaneous fistula

(224)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
HERNIA (POST-APPENDICECTOMY)
Definition
Prolapse of intestines at the appendicectomy scar.
Pathogenesis
Weakness of muscles due to:• Postoperative infection• Chronic cough• Chronic sneeze• Chronic constipation.
Day of Occurrence
Late postoperative period.
Clinical Presentation
• Swelling of the abdomen around the operated area(Fig. 7.10)
• Pain if obstruction occurs.
Investigations
No special investigation is necessary.

(225)
CHAPTER 7: APPENDICECTOMY
Management
Surgical repair with a mesh.
Fig. 7.10: Ventral hernia (post appendicectomy)

(226)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
INTESTINAL OBSTRUCTION
Definition
Mechanical obstruction of small bowel.
Pathogenesis
Postoperative adhesions in the ileocecal area.
Day of Occurrence
Months or years after surgery.
Clinical Presentation
• Recurrent attacks of abdominal pain• Associated vomiting and constipation.
Investigations• Plain X-ray (Fig. 7.11) may be useful• Contrast studies are useful• Laparoscopy is diagnostic.
ManagementMedicalConservative management.

(227)
CHAPTER 7: APPENDICECTOMY
Fig. 7.11: X-ray abdomen: Multiple air fluid levels ofsmall bowel obstruction
Surgical
Release of adhesions (laparoscopic or open).


(230)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
HISTORY
• 1823 – First successful resection for colonic growth byReybard of Lyons
• Extraperitoneal resection of colon:– 1894 – Exteriorization and delayed excision of
sigmoid by Bloch– 1895 and 1912 – Exteriorization and simultaneous
excision of sigmoid by Paul (Fig. 8.1)– 1894 – Exteriorization and delayed excision of
sigmoid by Miculicz
Fig. 8.1: Frank Thomas Paul (1851-1941)

(231)
CHAPTER 8: LARGE BOWEL RESECTION
– 1926 – Modification of Paul’s technique (byapplication of crushing clamps) by Rankin
– 1931 – Extraperitoneal resection of right colon andsplenic flexure by Devine
• Intraperitoneal resection with ‘aseptic anastomosis’– 1898 – Halstead– 1900 – O’Hara– 1921 – Shoemaker– 1928 – Pringle– 1940 – Wangensteen– 1950 – Monro
• Intraperitoneal resection of left colon afterdefunctioning transverse colostomy– 1931, 1935, 1938 – Devine
• Intraperitoneal resection with intestinal antisepsis– 1953 – Lloyd Davies, Morgan and Goligher– 1963 to 1967 – Nonabsorbable antibiotics and
irrigants by Gabriel, Hummel, Altemeier and Hill,Mckittrick and Naunton Morgan
– 1959 to 1968 – Tyson, Wangensteen and Gilbertsen,Grant and Barbara, Black)
• 1990 - First laparoscopic colonic resection (righthemicolectomy) by Moises Jacobs.

(232)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
VARIETIES OF SURGERIES OF COLON AND RECTUMVarieties of colon and rectum surgeries (Fig. 8.2)• Resection and establishment of continuity (hand sewn
or stapled anastomosis)• Bypass procedures (hand sewn or stapled anastomosis)
without resections.
Fig. 8.2: Varieties of colon and rectum surgeries

(233)
CHAPTER 8: LARGE BOWEL RESECTION
• Types of anastomosis (Fig. 8.3):– End-to-end– End-to-side– Side-to-side.
• Hand sewn anastomosis can be made in:– Single layer– Double layer.
Fig. 8.3: Types of anastomosis

(234)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
INDICATIONS
• Bleeding lesions (Figs 8.4A and B)• Obstructive lesions (strictures, tumors, intussusception)
(Figs 8.4C and D)• Strangulations with nonviable bowel.
Fig. 8.4A: Benign colonic polyp

(235)
CHAPTER 8: LARGE BOWEL RESECTION
Fig. 8.4B: Colonic polyp with dysplasia

(236)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
Fig. 8.4C: Malignancy of colon

(237)
CHAPTER 8: LARGE BOWEL RESECTION
Fig. 8.4D: Intussusception

(238)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
INCISIONS
• Midline (most popular) (Fig. 8.5)• Left paramedian for left colon• Right paramedian for right colon.
Note: Midline incision has the advantage of:• Ease• Speed• Versatility• Allows access to all quadrants• Easily extendable when needed.
Fig. 8.5: Midline incision

(239)
CHAPTER 8: LARGE BOWEL RESECTION
SURGICAL TECHNIQUE
Hand Sewn Technique (Fig. 8.6)
• Adequate mobilization• Marking the lines of resection
Fig. 8.6: Resection of colon

(240)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
• Vascular control (division of vessels betweenligatures) (1)
• Division of bowel• Anastomosis of the bowel ends (single or double
layer) (2)• Single layer anastomosis (3)
– Alignment of bowel ends– Application of full thickness sutures (outside in and
inside out)– Knotting on the outside
• Double layer anastomosis (3)– Posterior outer row first (seromuscular) with non-
absorbable material– Posterior inner row next (running full thickness) with
absorbable material– Anterior inner row in continuity from the posterior
inner row– Anterior outer row last (seromuscular) with non-
absorbable material.Note:• Inverting anastomosis causes serosa to serosa
apposition• Inversion of mucosa reestablishes integrity of lumen
preventing leakage.

(241)
CHAPTER 8: LARGE BOWEL RESECTION
WOUND INFECTION AFTER COLONIC SURGERY
Definition
Infection of laparotomy wound.
Pathogenesis
Handling of colon and soilage of the wound.
Day of Occurrence
2nd to 5th postoperative day.
Clinical Presentation
Discharge from the laparotomy wound (Fig. 8.7).
Relevant Investigation
Culture of discharge to isolate the incriminatingorganism.

(242)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
Management
• Broad spectrum antibiotics• Local wound care.
Fig. 8.7: Wound infection

(243)
CHAPTER 8: LARGE BOWEL RESECTION
ANASTOMOTIC LEAKAGE AFTER COLONICSURGERY
Definition
• Leakage of intestinal contents through the anastomoticline.
Pathogenesis
• Inadequate bowel preparation• Poor blood supply to both ends of bowel• Tension on the anastomosis.
Day of Occurrence
2nd to 5th postoperative day.
Clinical Presentation
• Abdominal pain• Fever• Leakage of intestinal contents through the drain.
Investigations
No special investigation is necessary.

(244)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
Management• Nil by mouth• Intravenous fluids• Intravenous broad spectrum antibiotics• Replacement of fluids, calories and electrolytes• Minor leaks heal, larger leaks require surgery (Fig. 8.8)• If fistula is formed, it may heal over a period of time• Some may require surgery, after 6 to 12 weeks for fistula.
Fig. 8.8: Anastomotic leakage producing fecal peritonitis

(245)
CHAPTER 8: LARGE BOWEL RESECTION
ANASTOMOTIC STRICTURE AFTER COLONICANASTOMOSIS
Definition
• Narrowing of lumen of anastomotic area (Fig. 8.9).
Fig. 8.9: Anastomotic stricture

(246)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
Pathogenesis
• Healing of a circular anastomosis results in a stricture.
Day of Occurrence
Months or years after surgery.
Clinical Presentation
• Constipation• Abdominal pain• Vomiting• Abdominal distension.
Investigations
Contrast studies may be useful.
Management
• Small bowel strictures are bypassed or resectionanastomosis done.
Note:Strictures following stapler usage is rare, if the correct sizeis chosen.

(247)
CHAPTER 8: LARGE BOWEL RESECTION
ADHESIONS AFTER COLONIC SURGERY
Definition
Adherence of bowels between themselves or with theparietes (Fig. 8.10).
Pathogenesis• Postoperative fibrinous adhesions result from the healing
of local inflammatory processes in the operated area• Resolved infections of peritoneum can cause adhesions.
Fig. 8.10: Adhesions between intestinal loops (black arrows) and toparietes (yellow arrow)

(248)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
Days of Occurrence
Months–years after surgery.
Clinical Presentation
• Recurrent attacks of abdominal pain• Vomiting• Constipation• Abdominal distension.
Investigations
X-rays of abdomen will show distended bowel.
Management
Medical
• Nil by mouth• Intravenous fluids and electrolytes.
Surgical
• If medical management fails, adhesiolysis by open orlaparoscopic methods.

(249)
CHAPTER 8: LARGE BOWEL RESECTION
EXTERNAL URINARY FISTULAE AFTERCOLONIC SURGERY
Definition
Fistulous communication between the ureter and exterior.
Pathogenesis
• Inadvertent clamping, cutting or damage to the ureter.
Days of Occurrence
Months after surgery.
Clinical Presentation
• Discharge of straw-colored clear fluid through drain.
Investigations
Contrast studies are useful.

(250)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
Management
• Ureteric fistulae due to:– Partial injury: Ureteric catheterization and
spontaneous healing– Complete injury: Resection and anastomosis (uretero
ureterostomy, uretero neocystoscomy) (Fig. 8.11).
Fig. 8.11: Operations of repair in ureteric injuries

(251)
CHAPTER 8: LARGE BOWEL RESECTION
EXTERNAL COLONIC FISTULAE
Definition
Leakage of colonic contents through a fistulae to theexterior.
Pathogenesis
• Anastomotic leak lead to collection of pus which in turndrain through the drainage tube
• Intentional external drainage of collection of pus fromthe anastomotic leak.
Days of Occurrence
Months after surgery.
Clinical Presentation
• Has had a turbulent postoperative period• Discharging wound in the postoperative period• Fluid and electrolyte disturbances• Skin excoriation around the fistulous opening (Fig. 8.12)• Fever.

(252)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
Investigations
• Oral administration of non-absorbable marker (charcoalor congo red)
• Fistulogram• US, CT with contrast or isotope scanning are useful.
Fig. 8.12: External colonic fistula

(253)
CHAPTER 8: LARGE BOWEL RESECTION
Management
Most lateral fistulae heal spontaneously.
Surgical
Excision of fistulaIndicated when there is:• Evidence of obstruction• Active disease• Interruption of bowel continuity• Closure not occurred by 6 weeks.


(256)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
HISTORY
• 1793 – First successful inguinal colostomy by Duret• 1797 – First transverse colostomy by Fine• 1808 – Colostomy by lumbar approach by Hendrik
Callisen• 1817 – Colostomy for imperforate anus by George Freer• 1820 – Colostomy with skin complications by Ping• 1839 – Lumbar colostomy by Amussat (Fig. 9.1)• 1931, 1935, 1938 – Defunctioning transverse colostomy
by Devine.
Fig. 9.1: Jean Zulema Amussat (1796-1856)

(257)
CHAPTER 9: COLOSTOMY
TYPES OF COLOSTOMY
There are four types of colostomy (Fig. 9.2). They are:1. Loop colostomy (C)2. Double barreled colostomy (A)
Fig. 9.2: Types of colostomy

(258)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
3. Divided colostomy (B)4. Terminal colostomy (D).
Indications for Loop Colostomy• As a temporary or palliative procedure in obstructed
colonic malignancies.
Indications for Double Barreled Colostomy
• Proximal to colocutaneous fistula• As an alternative to loop colostomy.
Indication for Divided Colostomy
• As a primary procedure for the definitive stoma.
Indication for Teminal Colostomy
• As a part of abdominoperineal resection for cancer oflower rectum (Fig. 9.3).

(259)
CHAPTER 9: COLOSTOMY
Fig. 9.3: Carcinoma lower rectum

(260)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
SURGICAL PROCEDURE
Terminal Colostomy (Fig. 9.4A)• A circular opening of 2 cm is made in the abdominal
wall at the site of colostomy (1)• The sigmoid colon is brought out through the
opening (2)• The bowel is fixed to the parietal peritoneum to prevent
recession
Fig. 9.4A: Surgical procedure of terminal colostomy

(261)
CHAPTER 9: COLOSTOMY
• The free end of the bowel is inverted and sutured to borderof abdominal opening with absorbable material (3).
Loop Colostomy (Fig. 9.4B)• Incision in the right upper abdomen• A loop of transverse colon is picked-up• Colon is fixed to parietes• Colon is opened with diathermy• Everting mucocutaneous suturing done with
absorbable material.
Fig. 9.4B: Surgical procedure of loop colostomy

(262)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
LOSS OF VIABILITY OF COLOSTOMY
Definition
Viability of the colostomy becomes questionable.
Pathogenesis
• Inadequate blood supply• Opening in the abdominal wall smaller than the colonic
diameter.
Day of Occurrence
2nd to 3rd postoperative day.
Clinical Presentation
Blackening or darkening of colostomy (Fig. 9.5).
Investigations
No special investigation is necessary.

(263)
CHAPTER 9: COLOSTOMY
Management
• Release of tight compressive dressings if necessary• If darkening does not improve, and extend downwards,
the wound should be reopened and refashioned.
Fig. 9.5: Loss of viability

(264)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
PERICOLOSTOMY SKIN DAMAGE
Definition
Irritation of skin around the colostomy stoma.
Pathogenesis
• Infection of mucocutaneous junction due to fecalcontamination.
Day of Occurrence
3rd to 5th postoperative day.
Clinical Presentation
Erythematous or ulcerative skin around the stoma,sometimes bleeding (Figs 9.6A and B).
Investigations
No special investigation is necessary.
Management• Antibiotics• Local dressings.

(265)
CHAPTER 9: COLOSTOMY
Fig. 9.6B: Excoriation of skin around transverse colostomy
Fig. 9.6A: Skin damage around end colostomy

(266)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
SEPARATION OF COLOSTOMY
DefinitionSeparation of mucocutaneous junction.
PathogenesisNon-healing of infected mucocutaneous junction.
Fig. 9.7A: Separation of end colostomy

(267)
CHAPTER 9: COLOSTOMY
Day of Occurrence3rd to 5th postoperative day.
Clinical PresentationUlcerated mucocutaneous junction (Figs 9.7A and B).
InvestigationsNo special investigation is necessary.
Treatment• Antibiotics• Local care dressings.
Fig. 9.7B: Ulceration and separation of colostomy

(268)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
STRICTURE AND RETRACTION OF COLOSTOMY
DefinitionInward pulling of narrowed colostomy.
Pathogenesis• Healing of circular ulceration of mucocutaneous
junction• Tight opening in the abdominal wall while creating the
stoma.
Fig. 9.8A: Stricture of colostomy

(269)
CHAPTER 9: COLOSTOMY
Day of Occurrence
Months after surgery.
Clinical Presentation
Retracted colostomy (Fig. 9.8A).
Investigations
No special investigation is necessary.
Management
Reconstruction with a formal laparotomy (Fig. 9.8B).
Fig. 9.8B: Surgical treatment of colostomy stricture

(270)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
STENOSIS OF COLOSTOMY
Definition
Narrowing of colostomy stoma.
Pathogenesis
• Healing of circular ulceration of mucocutaneousjunction
• Non-suturing of mucocutaneous junction duringsurgery
• Inadequate mucocutaneous approximation.
Day of Occurrence
Months after surgery.
Clinical Presentation
Constipation and passing small diameter fecal matter(Fig. 9.9A).
Investigations
No special investigation is necessary.

(271)
CHAPTER 9: COLOSTOMY
Fig. 9.9A: Stenosis of colostomy
Fig. 9.9B: Finger dilatation of stenosis of colostomy

(272)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
Management
Medical
Dilatation with finger (Fig. 9.9B) or metal dilator.
Surgical
Local repair (mobilization of colostomy and refashioning)(Fig. 9.9C).
Fig. 9.9C: Operative repair of stenosis of colostomy

(273)
CHAPTER 9: COLOSTOMY
PROLAPSE OF COLOSTOMY
Definition
Prolapse of colostomy, which is more common with loopcolostomy (Fig. 9.10A).
Fig. 9.10A: Prolapse of loop colostomy

(274)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
Pathogenesis
Construction of colostomy when the colon is dilated, andthe diameter of colon and the opening in the abdominalwall get mismatched.
Day of Occurrence
Months after surgery.
Clinical Presentation
• Stoma appears very much above the surface of skin• Mucosa may get ulcerated recurrently, caused by the
appliance.
Investigations
No special investigation is necessary.
Management
Local repair (detachment of mucocutaneous junction,reduction of everted stoma, amputation of excess lengthand refashioning) (Figs 9.10 B and C).

(275)
CHAPTER 9: COLOSTOMY
Fig. 9.10B: Operative repair of loop colostomy
Fig. 9.10C: Operative repair of end colostomy

(276)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
PARACOLOSTOMY HERNIA
Definition
Herniation of intra-abdominal contents anywhere aroundthe stoma.
Pathogenesis• Opening in the abdominal wall very large• Patulous abdominal wall.
Day of OccurrenceMonths after surgery.
Clinical Presentation• Swelling in the parastomal region (Fig. 9.11A)• Abdominal or local pain, if obstruction occurs.
Investigations
No special investigation is necessary.
Management
• Local repair (detachment of stoma, with the helpincision hernial sac is identified, reduced andrefashioned) (Fig. 9.11B).

(277)
CHAPTER 9: COLOSTOMY
Fig. 9.11B: Operative repair of paracolostomy hernia
Fig. 9.11A: Paracolostomy hernia

(278)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
Fig. 9.12: Colostomy perforation
COLOSTOMY PERFORATION
DefinitionPerforation of colostomy (Fig. 9.12).
PathogenesisCareless intubation during irrigation or contrast studies,which may cause peritonitis due to fecal contamination.

(279)
CHAPTER 9: COLOSTOMY
Day of Occurrence
Months after surgery.
Clinical Presentation
• Severe abdominal pain• Signs of localized peritonitis.
Investigations
• US and CT can localize collections• Endoscopy may show the perforation.
Management
Laparotomy and reconstruction of colostomy.


(282)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
HISTORY
• 1884 – First combined abdominoperineal excision ofrectum by Czerny (Fig. 10.1A)
• 1908 – Popularization of combined abdominoperinealresection by Ernest Miles
• 1920 – Two stage perineoabdominal excision by GreyTurner
• 1934 – Single stage perineoabdominal excision byGabriel
• 1934 – Synchronous combined abdominoperinealoperation by Heidelberg
Fig. 10.1A: Vincenz Czerny (1842-1916)

(283)
CHAPTER 10: ABDOMINOPERINEAL RESECTION
• 1937 – Popularization of synchronous combinedabdominoperineal operation by Devine
• 1939 – Synchronous combined abdominoperinealoperation in Lithotomy – Trendelenburg (Fig. 10.1B)position by Lloyd – Davies
• 1960 – Two team, simultaneous abdominoperinealresection by Rhoads.
Fig. 10.1B: Friedrich Trendelenburg

(284)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
INDICATION
• Malignancies of distal rectum or anus (Fig. 10.2).
Fig. 10.2: Specimen of carcinoma lower rectum

(285)
CHAPTER 10: ABDOMINOPERINEAL RESECTION
INCISION
• Lower midline (most convenient) (Fig. 10.3)• Lower left paramedian.Note: It has the advantage of:• Ease• Speed• Versatility• Allows access deep into pelvis• Easily extendable when needed• Site for colostomy is marked well in advance in sitting
position.
Fig. 10.3: Left lower paramedian incision with site marked for colostomy

(286)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
SURGICAL TECHNIQUE
Position of patient.
Lithotomy Trendelenburg Position
• Abdominal dissection (Fig. 10.4)– Lower midline incision– Release of sigmoid colon (1)– Identification and preservation of left ureter– Release of sigmoid colon from the right side (2)– Both incisions are joined anteriorly in the rectovesical
or rectouterine pouch– Rectum dissected and separated from the urinary
bladder and prostate (3)– Rectum is separated fully in the presacral space as
far down as possible (4)– Rectum separated fully on both the lateral sides
dividing lateral ligaments containing the middlerectal vessels
– Inferior mesenteric vessels flush ligated (5).• Perineal dissection
– Elliptical incision around the anus– Rectum is separated on all sides and dissection
carried proximally to meet the abdominal surgeon(6 and 7).

(287)
CHAPTER 10: ABDOMINOPERINEAL RESECTION
• Completion of operation– The separated rectum is removed from the perineal
wound– Terminal colostomy created (8).
Fig. 10.4: Surgical procedure

(288)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
HEMORRHAGE AND SHOCK AFTER AP RESECTION
Definition
Bleeding from the pelvis through the drain in the perinealwound (Fig. 10.5).
Fig. 10.5: Hemorrhage

(289)
CHAPTER 10: ABDOMINOPERINEAL RESECTION
Pathogenesis
Ooze from the pelvic cavity.
Day of Occurrence
2nd to 3rd postoperative day.
Clinical Presentation
• Tachycardia and hypotension• Signs of shock• Blood in the drain.
Investigations
Hematocrit to assess the blood loss.
Management
• Blood transfusions• Re-exploration if bleeding persists and requires large
transfusions.

(290)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
RUPTURE OF PELVIC PERITONEUM
DefinitionPartial or complete giving way of pelvic peritoneum(Fig. 10.6).
Pathogenesis• Inadequate approximation of pelvic peritoneum• Giving way of sutures approximating the pelvic
peritoneum.
Fig. 10.6: Rupture of pelvic peritoneum

(291)
CHAPTER 10: ABDOMINOPERINEAL RESECTION
Day of Occurrence
3rd to 10th postoperative days.
Clinical Presentation
• Severe abdominal pain• Bowel may be visible through the perineal wound.
Investigations
• No special investigation is necessary• Rarely ultrasound may be useful.
Management
• Surgery by abdominal route:– Bowel is released and pulled into abdomen and the
floor repaired (primarily or with a graft or mesh)– Gangrenous bowel needs to be resected.

(292)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
INFECTION OF PERINEAL WOUND AFTER APRESECTION
DefinitionInfection of perineal wound.
PathogenesisInadvertent opening of anorectum and spillage of contents.
Day of Occurrence
3rd to 10th postoperative day.
Clinical Presentation
• Pain in perineal wound• Discharge from perineal wound (Fig. 10.7).
Investigations
Culture of discharge to identify incriminating organism.
Management
• Broad spectrum antibiotics• Secondary suturing, if required.

(293)
CHAPTER 10: ABDOMINOPERINEAL RESECTION
Fig. 10.7: Infection of perineal wound

(294)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
STENOSIS OF PERINEAL SCAR AFTER APRESECTION
Definition
Narrowing of perineal scar.
Pathogenesis
Results after management of perineal wound by openregime.
Day of Occurrence
Months after surgery.
Clinical Presentation
• Pain in the perineal scar• Depression in the perineal sear (Fig. 10.8).
Investigations
No special investigation is necessary.
Management
• Scar release and stretching the skin is useful• Any collection below the scar needs to be drained.

(295)
CHAPTER 10: ABDOMINOPERINEAL RESECTION
Fig. 10.8: Stenosis of perineal scar

(296)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
PERINEAL HERNIA
DefinitionHernia of the perineal region.
PathogenesisWeakness of pelvic floor after extensive resections.
Day of OccurrenceMonths/years after surgery.
Fig. 10.9A: Perineal hernia through rent in pelvic peritoneum

(297)
CHAPTER 10: ABDOMINOPERINEAL RESECTION
Clinical PresentationBulge in the perineum (Fig. 10.9A and B).
InvestigationsCT may be useful.
ManagementPerineal repair with mesh is necessary.
Fig. 10.9B: Perineal hernia (Diagramatic representation)

(298)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
INTERNAL HERNIATION
Definition
Herniation of small bowel in the paracolic region.
PathogenesisHerniation of small bowel lateral to the terminal colon usedto form colostomy (Fig. 10.10).
Fig. 10.10: Internal herniation of small intestine

(299)
CHAPTER 10: ABDOMINOPERINEAL RESECTION
Day of Occurrence
Months after surgery.
Clinical Presentation
• Pain the left side of abdomen• Distention of abdomen• Vomiting• Fullness of the paracolostomy areas.
Investigations
• Colostogram is useful• CT abdomen is useful.
Management
Always Surgical
• Herniated small bowel requires to be reduced throughlaparotomy
• Non-viable bowel needs resection.

(301)
CHAPTER 11: ANTERIOR RESECTION

(302)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
HISTORY
• 1910 – Resection of rectosigmoid by abdominalapproach by Balfour
• 1934 – Resection of rectosigmoid by abdominalapproach with restoration of continuity by telescopicand tube technique by Lockhart Mummery (Fig. 11.1)
• 1963 – Resection of rectosigmoid by abdominalapproach with restoration with special mechanicaldevices by Hallenbeck, Judd and David
• 1965 – Very low colorectal anastomosis without sutureafter anterior resection by Brummelkamp
• 1945 – Mayo clinic operation by CF Dixon, CW Mayoand others of Mayo clinic.
Fig. 11.1: JP Lockhart Mummery

(303)
CHAPTER 11: ANTERIOR RESECTION
INDICATIONS
• Malignancies of mid and distal rectum (Fig. 11.2).
Fig. 11.2: Colorectal specimen containing a rectal tumor

(304)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
INCISIONS
• Lower midline (most convenient) [Fig. 11.3(a)]• Left lower paramedian [Fig. 11.3(b)].
Fig. 11.3: Incisions

(305)
CHAPTER 11: ANTERIOR RESECTION
SURGICAL TECHNIQUE
• Position of patient– Lithotomy Trendelenburg position
• Abdominal dissection– Lower midline incision– Release of sigmoid, descending colon beyond splenic
flexure– Identification and preservation of left ureter– Release of sigmoid colon from the right side– Both incisions are joined anteriorly in the rectovesical
or rectouterine pouch– Rectum dissected and separated from the urinary
bladder and prostate– Rectum is separated full in the presacral space as far
down as possible– Rectum separated fully on both the lateral sides
dividing lateral ligaments containing the middlerectal vessels
– Inferior mesenteric vessels flush ligated– Rectum stapled and transected low (using linear
stapler)– Colon transected at mid sigmoid level.
• Stapler anastomosis– Circular stapler introduced into the distal rectal
stump through the anus (Fig. 11.4A).

(306)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
– Anvil is introduced into the proximal colon(Fig. 11.4B)
– Proximal and distal guts are approximated(Fig. 11.4C)
Fig. 11.4 A: Insertion of stapler in the rectal stump

(307)
CHAPTER 11: ANTERIOR RESECTION
Fig. 11.4 B: Anvil in the proximal colon

(308)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
Fig. 11.4 C: Colon and rectum approximation
– The gun is fired to throw the staples (Fig. 11.4D)– Stapler is opened a little and gut released– Stapler is removed

(309)
CHAPTER 11: ANTERIOR RESECTION
Fig. 11.4 D: Firining of gun for anastomosis

(310)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
• Testing the integrity of anastomosis– Checking the doughnuts (Fig. 11.5)– By filling the pelvis with saline and injecting air in
the bowel and check for the air leak– By filling the rectum with dilute povidone iodine
solution and check for the solution leak.
Fig. 11.5: Doughnuts


(312)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
HISTORY
• 1716 – First surgical removal of a portion of liver by Berta• 1870 – Resection of lacerated portion of liver by Bruns• 1886 – Excision of solid tumor by Lius• 1890 – First resection of liver for tumor by Tiffany• 1910 – Near total right lobectomy by Wendel• 1952 – Anatomic hepatic lobectomy by Lortat-Jacob and
Robert• 1953 – Major hepatic resection by Quattlebaum• 1956 – Right hepatic lobectomy by finger fracture
technique (digitoclasia) by Fineberg• 1963 – Hepatic resection by digitoclasia with occlusion
of portal pedicle by Ton That Tung (Fig. 12.1).
Fig. 12.1: Ton That Tung

(313)
CHAPTER 12: SURGERY OF LIVER
VARIETIES OF HEPATIC RESECTIONSVerieties of hepatic resections (Fig. 12.2) are:• Right and left lobectomy (resection along the main portal
fissure, separating the right and left lobes of liver)• Right extended lobectomy or Trisegmentectomy (resection
of the entire right lobe, medial segment of left lobe, liver
Fig. 12.2: Varieties of hepatic resections

(314)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
substance to the right of falciform ligament andligamentum teres
• Left lateral segmentectomy (removal of segments II andIII to the left of falciform ligament and the ligamentumteres
• Unisegmentectomy (removal of single segment)*• Plurisegmentectomy (removal of two or more segments
at one time)• Wedge resection (removal of small segment of liver)
*Note:• Removal of segment I is impractical, as it requires
removal of segments II and III• Removal of segments II and III individually, has no
practical value• Removal of segment IV refers to removal of quadrate
lobe• Removal of segment VI is rarely indicated• Removal of segment VIII is very difficult, as it is
connected with intrahepatic inferior vena cava andsegment I.

(315)
CHAPTER 12: SURGERY OF LIVER
INDICATIONS
• Parasitic cysts (Figs 12.3A and B)• Non parasitic cysts
Figs 12.3A and B: (A) Hydatid cyst, (B) US—Simple cyst

(316)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
• Granulomas• Neoplasms• Primary (Benign and Malignant) (Fig. 12.3C)• Metastatic• Trauma
Fig. 12.3C: Hepatocellular carcinoma

(317)
CHAPTER 12: SURGERY OF LIVER
INCISIONS
Incisions for hepatic surgery (Fig. 12.4)• Roof Top incision (1)• Hockey stick incision (sternal or costal extensions if
necessary) (2).
Fig. 12.4: Hepatectomy incisions

(318)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
SURGICAL TECHNIQUE
Principles
• Adequate mobilization of liver to be resected(transection of ligamentous attachments)
• Temporary control of blood supply to the liver (byvascular tapes or clamps) (Fig. 12.5A) or permanent(ligatures and transections)
• Compression of blood vessels within the liverparenchyma (digital compression or hemoclips)
Fig. 12.5A: Pringle maneuver

(319)
CHAPTER 12: SURGERY OF LIVER
• Transection of liver parenchyma (digitoclasia,ultrasonic dissection)
• Control of bleeding from raw surface of liver (Gelfoam,oxidized cellulose, thrombin paste or powder, Argonbeam coagulation).
Steps
• Mobilization– Ligamentum teres is transected, cut end is held with
clamp for traction [(1) in Fig. 12.5B]– Anterior and posterior leaflets of coronary ligaments
are divided• Control of blood supply
– Hepatoduodenal dissection- Cystic artery and ducts are divided before
hepatoduodenal dissection [(2) in Fig 12.5B]- Identification of right hepatic artery and control
with vascular tape- Identification of right branch of portal vein and
control with vascular tape [(3) in Fig 12.5B]- Right hepatic duct is doubly ligated and divided
[(3) in Fig 12.5B]- Right hepatic artery and right branch of portal
vein are divided between ligatures [(3) in Fig12.5B].

(320)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
– Control of venous drainage- Main right hepatic vein is identified, clamped,
transected, the hepatic side is ligated, the cavalside is sutured with prolene [(4) in Fig 12.5B]
• Transection of liver parenchyma– Done with digitoclysis or ultrasonic dissector [(5) in
Fig. 12.5B]– Vessels encountered during transection are clamped
with hemoclips and divided.
Fig. 12.5B: Surgical technique

(321)
CHAPTER 12: SURGERY OF LIVER
• Specimen is removed• Raw surface bleeding may be controlled by
– Adequate diathermy and hemastatic agents– Approximation of anterior and posterior parts of Glisson’s
capsule (Fig. 12.5C)• Drains are required in the subphrenic space.
Fig. 12.5C: Methods to control bleeding from raw area of liver

(322)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
HYPERBILIRUBINEMIA
Definition
Yellowish discoloration of sclerae and skin.
Pathogenesis
• Direct damage to liver parenchyma• Hypovolemia• Reduced hepatic blood flow• Infection.
Day of Occurrence
2nd to 5th postoperative day.
Clinical Presentation
Yellowish discoloration of sclerae (Fig. 12.6) and skin.
Investigations
Serum bilirubin values are elevated.

(323)
CHAPTER 12: SURGERY OF LIVER
Management
• Resolve spontaneously• Broad spectrum antibiotics• Biliary enteric anastomosis if there is mechanical
obstruction.
Fig. 12.6: Yellowish discoloration of sclera (hyperbilirubinemia)

(324)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
PERSISTENT BILE LEAKAGE/BILIARY FISTULA
Definition
Leakage of bile from the surface of residual liver.
Pathogenesis
• Inadvertent bile duct injury• Insufficient or slipped ligature of bile duct• Peritoneal absorption of bile causes jaundice• Bile causes chemical peritonitis.
Day of Occurrence
3rd to 5th postoperative day.
Clinical Presentation
• Drainage of bile through the drain or skin (Fig. 12.7)• Yellowish discoloration of sclerae and skin (jaundice)• Severe abdominal pain (peritonitis).
Investigations
• Serum bilirubin levels may be elevated• CT scan may show localized collections of bile• MRCP can demonstrate the site of the fistula• Isotope scan is useful in locating the site of fistula.

(325)
CHAPTER 12: SURGERY OF LIVER
Management• Most bile leaks heal spontaneously if there is no distal
obstruction• Wide spectrum antibiotics• Biliary enteric anastomosis is required if there is
irremovable distal obstruction.
Fig. 12.7: External biliary fistula

(326)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
SUBPHRENIC ABSCESS
Definition
Collection of pus in the subphrenic spaces (Fig. 12.8).
Pathogenesis
Infection of collected blood in the operative area.
Fig. 12.8: Subphrenic abscesses

(327)
CHAPTER 12: SURGERY OF LIVER
Day of Occurrence
7th to 10th postoperative day.
Clinical Presentation
• General malaise• Hyperpyrexia of varying grades• Insignificant clinical examination.
Investigations
Ultrasonography and CT are useful in localizing abscess.
Management
Medical
• Small abscesses resolve with antibiotics.
Surgical
• Drainage of abscess under US or CT guidance• Open drainage if large and pus is thick.

(328)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
STRICTURE OF BILE DUCTS
Definition
Narrowing of bile ducts.
Reason
Inadvertent injury to bile ducts unrecognized during firstsurgery.
Day of Occurrence
Months or years after surgery.
Clinical Presentation
Yellowish discoloration of sclerae and skin.
Investigations
• Ultrasonography and CT are useful• ERCP (Fig. 12.9A) to delineate the obstruction and also
to stent• MRCP (Fig. 12.9B) or PTC will show the level of
obstruction.

(329)
CHAPTER 12: SURGERY OF LIVER
Fig. 12.9A: ERCP — Benign stricture of CBD

(330)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
Management
• ERCP sphincterotomy and stenting• Nasobiliary drainage if the stricture is passable• Percutaneous transhepatic drainage if the stricture is
not passable• Biliary enteric anastomosis if the stricture is not passable
but resectable.
Fig. 12.9B: MRCP — Benign stricture of CBD

(331)
CHAPTER 12: SURGERY OF LIVER
RECURRENCE OF MALIGNANCY
Definition
Recurrence of malignancy in the residual liver (Fig. 12.10).
Pathogenesis
• Residual tumor due to insufficient clearance• Microscopic disease during primary surgery.
Fig. 12.10: CT — Recurrent hepatocellular carcinoma

(332)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
Day of Occurrence
Months or years after surgery.
Clinical Presentation
• General malaise• Loss of appetite and weight• Abdominal pain• Abdominal distension• Jaundice.
Investigations
Ultrasonography and CT abdomen are useful.
Management
• Palliative—intra-arterial embolisation, intra arterialantimitotic drugs
• Surgical—resection if the tumor is solitary.


(334)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
HISTORY
• 1733 – Removal of gallstone and drainage of gallbladderby Jean-Louis Petit
• 1878 – First cholecystectomy by Marion Simms• 1878 – First successful cholecystostomy by Theodor
Kocher (Fig. 13.1A)• 1882 - First successful cholecystectomy by Carl Johann
August Langenbuch (Fig. 13.1B)• 1893 – First choledocholithotomy by Ludwig
Courvoisier (Fig. 13.1C)• 1987 – First human laparoscopic cholecystectomy by
Mouret.
Fig. 13.1B: CarlLangenbuch
Fig. 13.1C: LudwigCourvoisier (1843-1918)
Fig. 13.1A: TheodorKocher

(335)
CHAPTER 13: SURGERY OF GALLBLADDER
INDICATIONS FOR CHOLECYSTECTOMY
• Chronic calculous cholecystitis (Fig. 13.2A)• Acute calculous cholecystitis
Fig. 13.2A: Faceted gallstones in edematous gallbladder

(336)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
• Acalculous cholecystitis (Fig. 13.2B)• Empyema of gallbladder• Emphysematous cholecystitis
Fig. 13.2B: Acalculous cholecystitis

(337)
CHAPTER 13: SURGERY OF GALLBLADDER
• Gallbladder perforation• Gallbladder malignancy (Fig. 13.2C).
Note: Indications for laparoscopic cholecystectomy areanalogous to open cholecystectomy, and the decision toconvert to open technique should be made prior to acomplication.
Fig. 13.2C: Gallbladder malignancy with faceted gallstones

(338)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
SURGICAL TECHNIQUE
Open Cholecystectomy (Figs 13.3A and B)
Incisions
• Midline (1)• Right upper paramedian (2)• Right subcostal (Kocher’s) (3).
Fig. 13.3A: Incisions for cholecystectomy

(339)
CHAPTER 13: SURGERY OF GALLBLADDER
Fig. 13.3B: Kocher's incision for cholecystectomy

(340)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
Surgical Procedure (Fig. 13.4)
• Retraction to visualize the structures of hepatoduodenalligament– A deep retractor to retract the costal margin– The assistant’s right hand to retract the stomach to
the left stretching the ligament– The assistant’s left hand to retract the duodenun
downwards stretching the ligament
Fig. 13.4: Open cholecystectomy

(341)
CHAPTER 13: SURGERY OF GALLBLADDER
– Fundus and the Hartmann’s pouch of the gallbladderare retracted laterally to open the angle between thecystic duct and the common bile duct
– A sponge is placed in the Morrison’s pouch beneaththe free edge of the ligament which will raise thestructures towards the surgeon.
• The peritoneal reflection over the angle between thecystic duct and the common bile duct is snipped anddissected, to expose the cystic duct
• The cystic artery is identified within the triangle of Calot(space between the cystic duct and hepatic duct), doublyligated and divided (1)
• The cystic duct is divided between ligatures, leaving asmall stump (2)
• Gallbladder is dissected from its bed by blunt fingerdissection (3)
• Hemostasis established by cautery.
Laparoscopic Cholecystectomy (Figs 13.5A and B)
• Imaging instruments, diathermy devices, suctionapparatus and instrument tables are arranged in acomfortable manner
• Patient in supine position with lateral tilt• Four entry ports (Fig. 13.5A)
– Camera port at the umbilicus

(342)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
– Working port at the epigastrium– Right subcostal port– Right lateral port
• Carbon dioxide pneumoperitoneum created (12-15 mmHg)
Fig. 13.5A: Ports for laparoscopic cholecystectomy

(343)
CHAPTER 13: SURGERY OF GALLBLADDER
• Trocars inserted at the specified sites• Dissection started at the infundibulum (Fig. 13.5B)• Cystic artery divided between clips• Cystic duct divided between clips• Gallbladder dissected out of its bed• Gallbladder removed through epigastric port• Hemostasis established.
Fig. 13.5B: Laparoscopic cholecystectomy in progress

(344)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
BILIARY PERITONITIS
Definition
Infection of peritoneal cavity by bile (Fig. 13.6).
Fig. 13.6: Biliary peritonitis

(345)
CHAPTER 13: SURGERY OF GALLBLADDER
Pathogenesis
Leak of infected bile or superadded infection to the leakedbile, during surgery or perforated gallbladder.
Day of Occurrence
2nd to 5th postoperative day.
Clinical Presentation
High grade fever, severe pain in the right upper abdomen.
Investigations
Leukocytosis and raised sedimentation rate.
Management
Higher grade broader spectrum antibiotics, to cover grampositive organisms (3rd and 4th generation cephalospor-ins), gram negative organisms (aminoglycosides) andanaerobes (metronidazole).
Prevention
Prophylactic antibiotics, proper irrigation and suction ofsubhepatic area.

(346)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
HEMATOMA
Definition
Hematoma formation near the gallbladder bed (Fig. 13.7).
Fig. 13.7: Hematoma

(347)
CHAPTER 13: SURGERY OF GALLBLADDER
Pathogenesis
Slipped ligature of cystic artery or ooze from gallbladderbed.
Day of Occurrence
2nd to 5th postoperative day.
Clinical Presentation
Low grade fever, pain in the right upper abdomen.
Investigations
Ultrasonography or CT is useful.
Management
• Small collections resolve• Large collections obstructing the CBD, need aspiration
under US or CT guidance or open drainage.
Prevention
Application of double ligatures or double clips to the cysticartery proximally.

(348)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
BILE COLLECTION (BILEOMA)
Definition
Collection of bile in the gallbladder bed.
Pathogenesis
• Slipped ligature of cystic duct or ooze from gallbladderbed
• Sloughing of ligature of cystic duct• Surgical error• Anomalies of ductal system• Surgery on gangrenous gallbladder.
Clinical Presentation
Low grade fever, severe pain right upper abdomen.
Day of Occurrence
2nd to 5th postoperative day.
Investigations
Ultrasonography or CT is useful.

(349)
CHAPTER 13: SURGERY OF GALLBLADDER
Management
• Small collections resolve• Large collections obstructing the CBD, need aspiration
under US or CT guidance or open drainage (Fig. 13.8).
Prevention
Double ligature or clipping of cystic duct, proper irrigationand suction, understanding the anatomy.
Fig. 13.8: Drainage of bileoma

(350)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
SUBHEPATIC ABSCESS
Definition
Collection of pus in the peritoneal cavity (Fig. 13.9).
Fig. 13.9: Abscess

(351)
CHAPTER 13: SURGERY OF GALLBLADDER
Pathogenesis
• Infection of collected bile or blood or both• Collection of infected bile.
Day of Occurrence
2nd to 5th postoperative day.
Clinical Presentation
• High grade fever• Severe pain right upper abdomen• Severe tenderness right hypochondrium.
Investigations
Ultrasonography or CT is useful.
Management
• Small collections resolve• Large collections obstructing the CBD, need aspiration
under US or CT guidance or open drainage.
Prevention
Prophylactic antibiotics.

(352)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
EXTERNAL BILIARY FISTULA
Definition
Leakage of bile through a fistulous tract between the biliarytract and exterior.
Pathogenesis
• Spontaneous leakage of bile or bileoma to the exterior• Surgical drainage of bileoma• Distal obstruction of CBD (stone or malignancy).
Day of Occurrence
7th to 10th postoperative day.
Clinical presentation
• High grade fever• Discharge of bile from wound or drain site (Fig. 13.10A)• Signs of electrolyte imbalance.
Investigations
• US will demonstrate dilated biliary radicles• CT and MRI may demonstrate the pathology at the distal
CBD

(353)
CHAPTER 13: SURGERY OF GALLBLADDER
• Fistulography or MR fistulography may demonstrate thepathology at the distal CBD
• MRCP (Fig. 13.10B) is useful• PTC is useful when the ductal system is dilated• Isotope studies apart from the origin of fistulous tract
gives the index of liver function and biliary secretion.
Fig. 13.10A: External biliary fistula

(354)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
Management
Medical
• Correction of electrolyte and fluid imbalance• Correction of malnutrition• Control of skin excoriation• Control of intra-abdominal infection.
Surgical
• Relief of obstruction of CBD (ERCP sphincterotomy andbasketing of stone) (Fig. 13.10C)
Fig. 13.10B: MRCP—Stricture lower CBD

(355)
CHAPTER 13: SURGERY OF GALLBLADDER
• Total disruption of CBD warrants fistulo-jejunostomyor choledocho-jejunostomy
• Malignancy requires pancreato-duodenectomy.
Fig. 13.10C: Sphincterotomy

(356)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
CYSTIC DUCT STONE
Definition
Retained stone in the cystic duct remnant (Fig. 13.11).
Fig. 13.11: Cystic duct stone

(357)
CHAPTER 13: SURGERY OF GALLBLADDER
Pathogenesis
Unidentified stone retained in the cystic duct remnant(between the ligature and the junction of cystic duct andCBD).
Day of Occurrence
Months after surgery.
Clinical Presentation
• Usually asymptomatic• May present with upper abdominal pain.
Investigations
US or CT is diagnostic.
Management
• If asymptomatic, no treatment is required• If symptomatic, the stone may have to be removed.

(358)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
RETAINED CBD STONES
DefinitionStones in the common bile duct after primary gallbladderor bile duct surgery.
Pathogenesis• Overlooked stones in the common bile duct• Retained stones descending from hepatic ducts.
Day of OccurrenceMonths or years after surgery.
Clinical Presentation• Upper abdominal pain• High grade fever• Obstructive jaundice.
Investigations• US shows proximal dilatation of bile ducts• CT may show the obstructing calculus• MRCP shows the obstructing calculus (Fig. 13.12A)• PTC is used when ERCP is non contributory, especially
in dilated ductal system• Per oral mother baby choledochoscopy is contributory.

(359)
CHAPTER 13: SURGERY OF GALLBLADDER
Management
Removal of stone is necessary• Sphincterotomy and basketing (Fig. 13.12B) is curativeWhen the stone is impacted,• ESWL may be used to break the stone, followed by
basketing
Fig. 13.12A: ERCP — Multiple stones in CBD

(360)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
• Extraction using per oral mother baby choledochoscope• Dissolution of stones may be attempted• Choledochotomy is required if endoscopic procedure
fails• Choledocho enterostomy is done for stones impacted
in the lower CBD.
Fig. 13.12B: Basketing of common bile duct stone

(361)
CHAPTER 13: SURGERY OF GALLBLADDER
BENIGN CBD STRICTURE
Definition
Narrowing of common bile duct after surgery.
Pathogenesis
• Injury to the common bile duct• Primary closure of CBD after stone removal.
Day of Occurrence
Months or years after surgery.
Clinical Presentation
• Upper abdominal pain• Obstructive jaundice• Fever.
Investigations
• US and CT show proximal dilatation of bile ducts• MRCP (Fig. 13.13A) shows the stricture• ERCP (Fig. 13.13B) shows the stricture• PTC is used when ERCP is non contributory, especially
in dilated ductal system

(362)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
• Per oral mother baby choledochoscopy is contributory• Isotope studies are useful.
Fig. 13.13A: MRCP — Benign stricture of CBD

(363)
CHAPTER 13: SURGERY OF GALLBLADDER
Management
• Excision of stricture and end to end anastomosis over aT tube
• Choledocho enterostomy is a good alternative• Hepaticodochoenterostomy is required for strictures of
common hepatic duct.
Fig. 13.13B: ERCP — Benign stricture of CBD

(364)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
BILIARY ENTERIC FISTULA
Definition
Communication between the biliary system and intestines.
Pathogenesis
Rupture of pericholedochal abscess into the adjoiningbowel.
Day of Occurrence
Months or years after surgery.
Clinical Presentation
Usually asymptomatic.
Investigations
• X-ray and CT (Fig. 13.14) and useful• MRCP is useful• Barium studies may show the fistula• Isotope studies are diagnostic.

(365)
CHAPTER 13: SURGERY OF GALLBLADDER
Fig. 13.14: X-ray and CT—Air in the biliary system
Management
• Asymptomatic patients require no treatment• Excision of fistula is required in symptomatic patients.


(368)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
HISTORY
• 1899 – Successful resection of periampullary carcinomaby Halsted (Fig. 14.1A)
• 1912 – First successful pancreaticoduodenectomy byKausch
• 1935 – Successful two-stage pancreaticoduodenectomyby Whipple (Fig. 14.1B)
• 1941 – First one-stage pancreaticoduodenectomy byTrimble.
Fig. 14.1A: William Halsted Fig. 14.1B: Whipple

(369)
CHAPTER 14: SURGERY OF PANCREAS
VARIETIES OF PANCREATIC RESECTIONS
Varieties of pancreatic resections (Fig. 14.2) are:• Resection of pancreatic tail• Distal pancreatectomy (includes splenectomy)
Fig. 14.2: Varieties of pancreatic resections

(370)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
• Left pancreatectomy (removal of body and tail)• Pancreatoduodenectomy — Whipple’s operation
(removal of pancreatic head including duodenum,proximal part of jejunum and distal biliary tree)
• Subtotal pancreatectomy (removal of part of head,entire body and tail of pancreas)
• Total pancreatectomy (removal of entire pancreas).

(371)
CHAPTER 14: SURGERY OF PANCREAS
INDICATIONS FOR PANCREATECTOMY
• Inflammation– Necrotising pancreatitis– Chronic pancreatitis with pain
• Trauma• Neoplasms (Figs 14.3A to C)
– Adenocarcinoma (85%)– Cystadenoma (mucinous/serous)
Fig. 14.3A: CT — Malignancy of body and tail of pancreas

(372)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
– Cystadenocarcinoma– Islet cell tumors (neuroendocrine tumors)– Papillary cystic neoplasms
Fig. 14.3B: MRCP — Carcinoma of head of pancreas

(373)
CHAPTER 14: SURGERY OF PANCREAS
– Lymphoma– Acinar cell tumors
• Severe hyperinsulinemic hypoglycemia.
Fig. 14.3C: CT — Pancreatic head malignancy

(374)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
INCISIONS
Incisions for panereatic (Fig. 14.4)• Bilateral subcostal (1)• Long midline. (2)
Fig. 14.4: Incisions for pancreatic surgery

(375)
CHAPTER 14: SURGERY OF PANCREAS
SURGICAL TECHNIQUE OF WHIPPLE’S OPERATIONSurgical procedure (Fig. 14.5A) :• Mobilization of duodenum and head of pancreas, with
identification of superior mesenteric vein• Mobilization of common bile duct and portal vein
(above pancreas)• Cholecystectomy (1) and division of common bile duct (2)• Elevation of neck of pancreas from superior mesenteric
and portal veins
Fig. 14.5A: Surgical technique of Whipple’s operation

(376)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
• Division of stomach or duodenum (if pylorus is to bepreserved) (3)
• Division of neck of pancreas (4)• Dissection of divided pancreas from mesenteric vessels• Mobilization and division of proximal jejunum (5)• Division of mesoduodenum and attachments of
uncinate process to the superior mesenteric artery, andremoval of specimen
• Reconstruction of gastrointestinal continuity (Fig. 14.5B).
Fig. 14.5B: Recenstruction after whipple’s operation

(377)
CHAPTER 14: SURGERY OF PANCREAS
GASTROINTESTINAL HEMORRHAGE(POST-PANCREATECTOMY)
Definition
Bleeding in the stomach (Fig. 14.6).
Fig. 14.6: Gastrointestinal hemorrhage

(378)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
PathogenesisBleeding from:• Anastomotic area• Small bleeding ulcer in the gastric pouch• Erosion of ligated artery following pancreatic leak.
Day of Occurrence1st to 5th postoperative day.
Clinical PresentationBloody nasogastric aspirate.
InvestigationsHematocrit values may fall low.
ManagementMedical
• Ice cold saline• Endoscopic injection of 1:10000 adrenaline• Blood transfusions.
Surgical• Opening of gastric pouch above the anastomosis and
control of bleeding site.

(379)
CHAPTER 14: SURGERY OF PANCREAS
EXTRAGASTRIC HEMORRHAGE(POST-PANCREATECTOMY)
Definition
Bleeding from sources outside stomach (Fig. 14.7).
Fig. 14.7: Extragastric hemorrhage

(380)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
Pathogenesis• Laceration of spleen• Injury to liver by retractors• Injury to vasa brevia• Hemorrhage from pancreatic bed• Improperly secured vessel in the greater and lesser
omentum.
Day of Occurrence1st to 5th postoperative day.
Clinical Presentation• Bloody discharge from the drain in the abdominal cavity• Clear nasogastric aspirate.
Investigations• Hematocrit values may fall low• CT abdomen may be contributory.
ManagementMedical• Blood transfusion.
Surgical• Exploratory laparotomy and correction of cause.

(381)
CHAPTER 14: SURGERY OF PANCREAS
DELAYED GASTRIC EMPTYING(POST-PANCREATECTOMY
Definition
Delay in emptying of stomach in the post-pancreativeperiod.
Pathogenesis (Fig. 14.8)
• Gastric atony due to disruption of gastoduodenal neuralconnection
• Ischemic injury to antropyloric muscle mechanism• Gastric dysrythmias due to intra-abdominal leaks• Gastric atony due to reduced levels of motilin.
Day of Occurrence
3rd to 5th postoperative day.
Clinical PresentationIncreasing nasogastric aspirate lasting for more than 2–3weeks.
InvestigationsUpper GI endoscopy after two weeks to rule out mechanicalobstruction.

(382)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
ManagementMedical• Prolonged patient gastric decompression• Intravenous water and electrolyte substitution• Prokinetic drugs like bethanechol, metoclopramide,
erythromycin derivatives.
Fig. 14.8: Delayed gastric emptying — pathogenesis

(383)
CHAPTER 14: SURGERY OF PANCREAS
BILIARY LEAK (POST-WAIPPLE’S OPERATION)
DefinitionLeakage of bile.
PathogenesisDisruption of biliary enteric anastomosis (Fig. 14.9A).
Fig. 14.9A: Biliary leak

(384)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
Day of Occurrence
3rd to 7th postoperative day.
Clinical Presentation
• Discharge of bile stained fluid through the intra-abdominal drain
• Skin excoriation around the drain (Fig. 14.9B).
Fig. 14.9B: Biliary leak and skin excoriation

(385)
CHAPTER 14: SURGERY OF PANCREAS
Investigations
• Diagnosis is obvious, but isotope scan can demonstratethe leak
• CT is useful in locating localized collections of bile.
Management
Medical
• Most leaks heal spontaneously if there is no distalobstruction.
Surgical
• Localized collections of bile should be drained by USor CT guidance
• Open drainage of collection of bile is rarely necessary.

(386)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
PANCREATIC LEAK
Definition
Leakage of pancreatic secretions (Fig. 14.10).
Fig. 14.10: Pancreatic leak

(387)
CHAPTER 14: SURGERY OF PANCREAS
Pathogenesis
Disruption of pancreatico-enteric anastomosis.
Day of Occurrence
3rd to 7th postoperative day.
Clinical Presentation
• Discharge of clear fluid through the intra-abdominaldrain
• Tachycardia, hyperpyrexia, tachypnea• Excoriation of skin around the drain• Abdominal tenderness.
Investigations
• Leucocytosis• Serum lactate and amylase levels may be elevated.
ManagementMedical
• Replacement of fluids and electrolytes• When the loss is less than 50ml/day, it heals
spontaneously

(388)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
• Antibiotics are needed for large leaks with peritonitis• Total parenteral nutrition is useful in large leaks• May result in a pancreatic fistula.
Surgical
• Percutaneous drainage of localized collections• Laparotomy and peritoneal toileting in peritonitis• Completion pancreatectomy is rarely needed.

(389)
CHAPTER 14: SURGERY OF PANCREAS
CHYLOUS ASCITES (POST-PANCREATECTOMY)
Definition
Leakage of lymph in the peritoneal cavity (Fig. 14.11).
Fig. 14.11: Chylous ascites

(390)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
Pathogenesis
Due to extensive retroperitoneal lymph node dissectionand injury to main lymphatic channels.
Day of Occurrence
10th to 15th postoperative day.
Clinical Presentation
• Yellowish serous or milky discharge (chyle) throughthe intra-abdominal drain
• Amounts to several liters of fluid daily.
Investigations
CT is useful in diagnosing localized collections.
Management
• Ligation of main lymphatic channel may be required ifit does not resolve in a few weeks
• TPN may be required to maintain good nutritionalstatus.

(391)
CHAPTER 14: SURGERY OF PANCREAS
MARGINAL ULCERATIONS
Definition
Ulceration on the anastomotic margin.
Pathogenesis
• Non-performance of vagotomy• Ulcerogenic potential of pancreatectomy.
Day of Occurrence
After 2 weeks.
Clinical Presentation
• Upper abdominal discomfort• Pain abdomen• Hematemesis and melena.
Investigation
Upper GI endoscopy (Fig. 14.12) is diagnostic.

(392)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
Management
Proton pump inhibitors.
Fig. 14.12: Endoscopy — Anastomotic ulcer

(393)
CHAPTER 14: SURGERY OF PANCREAS
OBSTRUCTIVE JAUNDICE (POST AND WHIPPLE’SOPERATION)
Definition
Jaundice due to obstruction in the biliary drainage.
Pathogenesis
• Benign– Stricture of biliary enteric anastomosis
• Malignant– Local recurrence at mesenteric root– Recurrence of malignancy at hilum of liver.
Day of Occurrence
12 weeks after surgery.
Clinical Presentation
Yellowish discoloration of urine, sclera (Fig. 14.13) and skin.
Investigations
• Serum bilirubin levels are high• MRCP will localize the level of obstruction• CT will localize the cause of obstruction.

(394)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
Management
Surgical
• Percutaneous transhepatic drainage and stenting oftumors at hilum of liver
• Second Roux-en-Y reconstruction may relieve jaundice.
Fig. 14.13: Jaundice

(395)
CHAPTER 14: SURGERY OF PANCREAS
ENDOCRINE AND EXOCRINE INSUFFICIENCY
DefinitionDeficiency of endocrine and exocrine components ofpancreatic secretions.
Pathogenesis (Fig. 14.14)
• Removal of endocrine and exocrine tissues as part ofpancreatic resection
• Fibrosis of pancreatic remnant leading to loss of isletcell tissue
• Stenosis at pancreaticojejunostomy site.
Day of Occurrence
18 months after surgery.
Clinical PresentationSevere wasting.
Investigations• Determination of blood sugar levels (endocrine
deficiency)• Determination of enzyme levels in blood and feces
(exocrine deficiency).

(396)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
ManagementMedical• Replacement of insulin• Administration of enzymes rich in lipase, fat-soluble
vitamins, calcium and trace elements.
Fig. 14.14: Endocrine and exocrine deficiency — Pathogenesis


(398)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
HISTORY
• 1549 – First recorded splenectomy by Adriano Zacarello• 1590 – First successful partial splenectomy by Franciscus
Rosetti• 1678 – Partial splenectomy for trauma by Nicolaus
Matthias• 1816 – First splenectomy for trauma by O’Brien• 1895 – First successful repair of lacerated spleen by
Zikoff• 1962 – First successful partial splenectomy for trauma
in modern times by Campos Christo• 1991 – Delaitre (France), Carroll (US), Cushieri (UK) (Fig.
15.1) published reports on laparoscopic splenectomy.
Fig. 15.1: Alfred Cuschieri

(399)
CHAPTER 15: SURGERY OF SPLEEN
VARIETIES OF OPERATIONS OF SPLEEN
Varieties of operations of spleen (Fig. 15.2) are:• Splenectomy• Partial splenectomy• Splenorrhaphy and autotransplantation.
Fig. 15.2: Varieties of operations of spleen

(400)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
INDICATIONS
• Trauma (Fig. 15.3A)– Spontaneous rupture– Physical trauma
• Disorders of hemopoietic system– Idiopathic thrombocytic purpura
• Disorders of lymphoreticular system– Large spleen in lymphoma (Fig. 15.3B)
Fig. 15.3A: CT — Splenic injury with lower rib fracture

(401)
CHAPTER 15: SURGERY OF SPLEEN
Fig. 15.3B: CT — Gross splenomegaly in non-Hodgkin's lymphoma
– Large spleen of hypersplenism• Adjunct procedures
– Extension of malignancy of stomach– A part of upper partial or total gastrectomy
• Splenic abscess (Fig. 15.3C).

(402)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
Fig. 15.3C: CT — Splenic abscesses

(403)
CHAPTER 15: SURGERY OF SPLEEN
INCISIONS
Incisions for splenectomy (Fig. 15.4) are:• Upper midline (1)• Left upper paramedian (2)• Left subcostal (3)• Left hockey-stick (4).
Fig. 15.4: Incisions

(404)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
SURGICAL TECHNIQUESurgical technique of splenectomy (Fig. 15.5) are:• Division of ligamentous attachment (1)
– Splenophrenic ligament– Splenocolic ligament– Splenorenal ligament
• Division of vessels– Transection of short gastric vessels (2)– Ligation and division of splenic artery (3)– Ligation and division of splenic vein (4)
• Removal of spleen.
Fig. 15.5: Surgical technique of splenectomy

(405)
CHAPTER 15: SURGERY OF SPLEEN
POST-SPLENECTOMY BLEEDING
Definition
Bleeding from the operative field (Fig. 15.6).
Fig. 15.6: Bleeding

(406)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
Pathogenesis
Slippage of ligature of short gastric vessels.
Day of Occurrence
2nd to 5th postoperative days.
Clinical Presentation
Bleeding from the drain in the left subphrenic space.
Investigations
Hematocrit values may fall.
Management
Medical
• Blood transfusion.
Surgical
• Exploratory laparotomy and ligation of bleedingvessels.

(407)
CHAPTER 15: SURGERY OF SPLEEN
THROMBOCYTOSIS
Definition
Increase in platelet count.
Pathogenesis
• Elimination of splenic sequestration• Removal of regulatory humoral factor produced by
spleen• Persistent anemia• Altered platelet function.
Day of Occurrence
Late postoperative period.
Clinical Presentation
• Episodes of upper gastrointestinal bleeding(without encephalopathy and ascites).
Investigations
• Platelet count raised above 4,00,000/cmm (Fig. 15.7)• Liver function tests remain normal.

(408)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
Management
• Good hydration• Antiplatelet drugs (acetyl salicylic acid, dipyridamole).
Fig. 15.7: Thrombocytosis

(409)
CHAPTER 15: SURGERY OF SPLEEN
THROMBOSIS OF SPLENIC AND PORTAL VEINS
Definition
Thrombosis of splenic and portal veins (Fig. 15.8).
Fig. 15.8: Thrombosis of portal and splenic veins

(410)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
Pathogenesis
• Combined effect of hypercoagulable state and stasis ofblood in splenic vein stump
• Aberrant coagulation originating in the splenic veinstump and progressing into portal vein.
Day of Occurrence
Late postoperative period.
Clinical Presentation
• Episodes of upper gastrointestinal bleeding(without encephalopathy and ascites).
Investigations• Ultrasonography and contrast enhanced CT of portal
vein and splenic vein• Venous phase of visceral angiography.
Management• Urgent treatment with thrombolytic agents like
heparin, intravenous antibiotics, followed byanticoagulation
• Bowel resection may be needed for bowel infarctionand ischemia.

(411)
CHAPTER 15: SURGERY OF SPLEEN
FULMINANT SEPSIS
Definition
High grade Gram-negative infection after splenectomy.
Pathogenesis
• Lack of splenic macrophages to clear opsonisedmicroorganisms
• Lack of type-specific antibodies.
Day of Occurrence
Late postoperative period.
Clinical Presentation
• High grade pyrexia of abrupt onset (Fig. 15.9)• Rapid deterioratory course• Cardiovascular collapse.
Investigations
• Leucocytosis• Isolation of organism in blood by culture.

(412)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
Management
Intravenous antibiotics.
Fig. 15.9: Post-splenectomy fulminant sepsis—Temperature chart

A
Abdominoperineal resection 281incision 285indication 284surgical technique 286
Achalasia 13clinical presentation 13investigations 13management 14pathogenesis 13
Acute afferent loop obstruction 75clinical presentation 75investigations 77management 78pathogenesis 75
Adhesion 159clinical presentation 160investigations 160management 160pathogenesis 159
Adhesions after colonic surgery247
clinical presentation 248investigations 248pathogenesis 247
Alkaline reflux gastritis 89clinical presentation 89investigations 89management 91pathogenesis 89
Anastomotic leak(postesophagectomy) 29
clinical presentation 29investigations 29management 30pathogenesis 29
Anastomotic leakage (intestinalanastomosis) 151
clinical presentation 151investigations 151management 152pathogenesis 151
Anastomotic leakage after colonicsurgery 243
clinical presentation 243investigations 243management 244pathogenesis 243
Anastomotic stricture 157clinical presentation 158investigations 158management 158pathogenesis 158
Index

(414)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
Anemia 104clinical presentation 104investigations 104management 104pathogenesis 104
Anterior resection 301history 302incisions 304indications 303surgical technique 305
Appendicectomy 207incisions 211indications 209investigations 248surgical technique 212
B
Benign CBD stricture 361clinical presentation 361investigations 361management 363pathogenesis 361
Bile collection (bileoma) 348clinical presentation 348investigations 348management 349pathogenesis 348prevention 349
Biliary enteric fistula 364clinical presentation 364investigations 364
management 365pathogenesis 364
Biliary leak 383clinical presentation 384investigations 385management 385pathogenesis 383
Biliary peritonitis 344clinical presentation 345investigations 345management 345pathogenesis 345prevention 345
C
Chronic afferent loop obstruction124
clinical presentation 124investigations 124management 125pathogenesis 124
Chronic efferent loop obstruction126
clinical presentation 126investigations 126management 127pathogenesis 126
Chronic gastric atony 106clinical presentation 106investigations 106management 107

(415)
INDEX
medical 107surgical 107
pathogenesis 106Chylous ascites 389
clinical presentation 390investigations 390management 390pathogenesis 390
Colostomy 255surgical procedure 260types 257
Colostomy perforation 278clinical presentation 279investigations 279management 279pathogenesis 278
Cystic duct stone 356clinical presentation 357investigations 357management 357pathogenesis 357
D
Delayed gastric emptying 381clinical presentation 381investigations 381management 382pathogenesis 381
Delayed intragastric hemorrhage(post-gastrectomy) 53
clinical presentation 53
investigations 53management 53pathogenesis 53
Duodenal stump leak 60clinical presentation 60investigations 60management 61pathogenesis 60signs 60
Dysphagia 31clinical presentation 31investigations 31management 32pathogenesis 31
Dystony of gallbladder andcholelithiasis 19
clinical presentation 19investigations 19management 20pathogenesis 19
E
Early dumping syndrome 92clinical presentation 92investigations 93management 93pathogenesis 92
Early intragastric hemorrhage(post-gastrectomy) 51
clinical presentation 51investigations 51

(416)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
management 51pathogenesis 51
Efferent loop obstruction 80clinical presentation 80investigations 80management 81pathogenesis 80
Endocrine and exocrineinsufficiency 395
clinical presentation 395investigations 395management 396pathogenesis 395
Esophageal resection 21indications 26reconstructions after resections
25surgical technique 27
abdominal dissection 27cervical dissection 28reconstruction 28
Excessive length of ileostomystoma 198
clinical presentation 198investigations 198management 199pathogenesis 198
Excoriation and infection aroundgastrostomy stoma 135
clinical presentation 135investigations 135management 136pathogenesis 135
External biliary fistula 352clinical presentation 352investigations 352management 354pathogenesis 352
External colonic fistulae 251clinical presentation 251investigations 252management 253pathogenesis 251
External fistulae 163clinical presentation 163investigations 164management 164pathogenesis 163
External urinary fistulae aftercolonic surgery 249
clinical presentation 249investigations 249management 250pathogenesis 249
Extragastric hemorrhage 379clinical presentation 380investigations 380management 380pathogenesis 380
Extragastric hemorrhage (post-gastrectomy) 57
clinical presentation 58investigations 59management 59pathogenesis 58

(417)
INDEX
F
Fulminant sepsis 411clinical presentation 411investigations 411management 412pathogenesis 411
G
Gastrectomy and gastrostomy 39incisions 46indications 44reconstruction after
gastrectomies 49surgical technique 47varieties of surgeries of stomach
and duodenum 41Gastric remnant carcinoma 117
clinical presentation 117investigations 117management 118pathogenesis 117
Gastric remnant necrosis 68clinical presentation 68clinical presentation 73investigations 68investigations 73management 74pathogenesis 73stomal obstruction 72
Gastric stasis and bezoar formation108
clinical presentation 109investigations 109management 110pathogenesis 108
Gastroduodenostomy 62clinical presentation 62investigations 62management 62pathogenesis 62
Gastrointestinal hemorrhage 377clinical presentation 378investigations 378management 378pathogenesis 378
Gastrointestinal staplers 1intraluminal staplers 2linear cutter 4linear staplers 3
Gastrojejunocolic fistula 121clinical presentation 122investigations 122management 122pathogenesis 121
Gastrojejunostomy leak 64clinical presentation 64investigations 64management 64pathogenesis 64

(418)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
H
Hematoma 346clinical presentation 347management 347pathogenesis 347prevention 347
Hemorrhage (intestinalanastomosis) 153
clinical presentation 154investigations 154management 154pathogenesis 154reason 154
Hemorrhage and shock after APresection 288
clinical presentation 289investigations 289management 289pathogenesis 289
Hemorrhage from appendicularstump 214
clinical presentation 215investigations 215management 215pathogenesis 215
Hemorrhage from ileostomy 177clinical presentation 178investigations 178management 178pathogenesis 178
Hernia (post-appendicectomy 224clinical presentation 224investigations 224management 225pathogenesis 224
Hoarseness of voice 33clinical presentation 33investigations 33management 33pathogenesis 33
Hyperbilirubinemia 322clinical presentation 322investigations 322management 323pathogenesis 322
I
Ileostomy 171history 172indications 174
end ileostomy 174loop end ileostomy 175loop ileostomy 175
surgical procedure 176types 173
Ileotomy fistula 202clinical presentation 202investigations 202management 202pathogenesis 202

(419)
INDEX
Ileostomy obstruction 186clinical presentation 186investigations 186management 187pathogenesis 186
Inadvertent gastroileostomy 87clinical presentation 88investigations 88management 88pathogenesis 87
Infection of perineal wound afterAP resection 292
clinical presentation 292investigation 292management 292pathogenesis 292
Internal fistulae 161clinical presentation 162investigations 162management 162pathogenesis 162
Internal hernia 128clinical presentation 129investigations 129management 129pathogenesis 128
Internal herniation 298clinical presentation 299investigations 299management 299pathogenesis 298
Intestinal obstruction 226clinical presentation 226investigations 226
management 226pathogenesis 226
Intra-abdominal abscess 155clinical presentation 156investigations 156management 156pathogenesis 155
Intra-abdominal abscess 83clinical presentation 83investigations 83management 83pathogenesis 83
Intraperitoneal leak aftergastrostomy 133
clinical presentation 134investigations 134management 134pathogenesis 134
JJejunogastric intussusception 130
clinical presentation 130investigations 130management 131pathogenesis 130
KKocher’s incision 339
LLarge bowel resection 229
incisions 238

(420)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
indications 234surgical technique 239
Late dumping 100clinical presentation 100management 101pathogenesis 100
Loss of viability of colostomy 262clinical presentation 262investigations 262management 263pathogenesis 262
M
Marginal ulcerations 391clinical presentation 391investigation 391management 392pathogenesis 391
Mucosal slough of ileostomy 179clinical presentation 180investigations 180management 180pathogenesis 180
N
Necrosis of lesser curve 11clinical presentation 11investigation 11management 12pathogenesis 11
Nutritional deficiencies 166clinical presentation 167investigations 167management 167pathogenesis 166
O
Obstructive jaundice 393clinical presentation 393investigations 393management 394pathogenesis 393
P
Pancreatic leak 386clinical presentation 387investigations 387management 387pathogenesis 387
Paracolostomy hernia 276clinical presentation 276investigations 276management 276pathogenesis 276
Paraileostomy granuloma 204clinical presentation 205investigations 205management 205pathogenesis 205

(421)
INDEX
Paralytic ileus 216clinical presentation 216investigations 216management 217pathogenesis 216
Parastomal abscess 200clinical presentation 201investigations 201management 201pathogenesis 201
Parastomal hernia 195clinical presentation 196investigations 196management 196pathogenesis 195
Parastomal skin irritation 182clinical presentation 183investigations 183management 183pathogenesis 183
Pelvic/paracolic abscess 220investigations 220clinical presentation 220management 221pathogenesis 220
Pericolostomy skin damage 264clinical presentation 264investigations 264management 264pathogenesis 264
Persistent bile leakage/biliaryfistula 324
clinical presentation 324investigations 324management 325pathogenesis 324
Persistent dysphagia 36clinical presentation 36investigations 36management 37pathogenesis 36
Postoperative pancreatiis 85clinical presentation 85investigations 85management 86pathogenesis 85
Post-splenectomy bleeding 405clinical presentation 406investigations 406management 406pathogenesis 406
Post-vagotomy diarrhea 15clinical presentation 16investigations 16management 16pathogenesis 15
Prolapse of colostomy 273clinical presentation 274investigations 274management 274pathogenesis 274
Prolapse of ileostomy 193clinical presentation 194investigations 194

(422)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
management 194pathogenesis 193
Pyloroplasty leak 66pathogenesis 67clinical presentation 67investigations 67management 67
R
Recession of ileostomy 191pathogenesis 191clinical presentation 192investigations 192management 192
Recurrence of malignancy 331pathogenesis 331clinical presentation 332investigations 332management 332
Recurrent ulcer 119pathogenesis 119clinical presentation 119investigations 119management 119
Reflux esophagitis and stricture17
pathogenesis 17clinical presentation 17investigations 17management 18
Retained CBD stones 358pathogenesis 358
clinical presentation 358investigations 358management 359
Roux stasis syndrome 114pathogenesis 114clinical presentation 114investigations 115management 115
Rupture of pelvic peritoneum 290pathogenesis 290clinical presentation 291investigations 291management 291
Rupture of stump andappendicocutaneous 222
pathogenesis 222clinical presentation 222investigations 222management 223
S
Separation of colostomy 266pathogenesis 266clinical presentation 267investigations 267treatment 267
Short bowel syndrome 168pathogenesis 168clinical presentation 168investigations 168management 169

(423)
INDEX
Small bowel resection 137indications 139incisions 140varieties 140types of small bowelanastomosis 142end-to-end anastomosis 145end-to-side anastomosis 147side-to-side anastomosis 149
Small gastric remnant syndrome111
pathogenesis 111clinical presentation 111investigations 111management 112
Stenosis of colostomy 270pathogenesis 270clinical presentation 270investigations 270management 272
Stenosis of ileostomy 188pathogenesis 189clinical presentation 189investigations 189management 189
Stenosis of perineal scar after APresection 294
pathogenesis 294clinical presentation 294investigations 294management 294
Stricture and retraction ofcolostomy 268
pathogenesis 268clinical presentation 269investigations 269management 269
Stricture of bile ducts 328reason 328
clinical presentation 328investigations 328management 330
Subhepatic abscess 350pathogenesis 351clinical presentation 351investigations 351management 351prevention 351
Subphrenic abscess 326pathogenesis 326clinical presentation 327investigations 327management 327
medical 327surgical 327
Surgery of gallbladder 333history 334indications for
cholecystectomy 335surgical technique 338open cholecystectomy 338surgical procedure 340
laparoscopiccholecystectomy 341
Surgery of liver 311history 312

(424)
MINI ATLAS SERIES: GASTROINTESTINAL SURGERY
varieties of hepatic resections313
indications 315incisions 317surgical technique 318
principles 318steps 319
Surgery of pancreas 367history 368varieties of pancreaticresections 369
indications 371incisions 374
Surgery of spleen 397history 398varieties of operations 399
indications 400incisions 403surgical technique 404
TThrombocytosis 407
pathogenesis 407clinical presentation 407investigation 407management 408
Thrombosis of splenic and portalveins 409
pathogenesis 410clinical presentation 410investigations 410investigations 410management 410
V
Vagotomy 5varieties 7
truncal vagotomy 7selective vagotomy 7highly selective vagotomy
7indications 8incision 9surgical technique 10
W
Weight loss (post-gastrectomy)102
clinical presentation 102investigations 102management 102pathogenesis 102
Whipple’s operation 375Wound infection after
appendicectomy 218pathogenesis 218clinical presentation 218investigations 218management 219
Wound infection after colonicsurgery 241
pathogenesis 241clinical presentation 241relevant investigation 241management 242
















![Jaypee Gold Standard Mini Atlas Series Pe-dodontics (2008) [UnitedVRG]](https://img.pdfslide.net/doc/110x75/577cc19d1a28aba7119377c8/jaypee-gold-standard-mini-atlas-series-pe-dodontics-2008-pdf-unitedvrg.jpg)





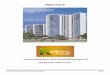


![Jaypee Gold Standard Mini Atlas Series® Embryology (2010) [UnitedVRG]](https://img.pdfslide.net/doc/110x75/5695d4de1a28ab9b02a31b00/jaypee-gold-standard-mini-atlas-series-embryology-2010-pdf-unitedvrg.jpg)

