Embed Size (px)
Citation preview
MDCT in upper gastrointestinal obstruction :
A pictorial review.
JM Tubiana - P Taourel, MD.
Paris - Montpellier FRANCE Hanoi, nov 2015
Learning objectives
v To learn specific causes, epidemiology, physiopathology and MDCT aspect of gastro-duodenal obstruction.
v To discuss the contribution of MDCT in the management of acute gastro-duodenal obstruction, describing and illustrating key CT findings.
v To be aware of CT pitfalls and difficulty diagnosis.
Introduction
v Intestinal obstruction is a very common cause of acute abdomen in emergency department.
v Small bowel obstruction: about 65 to 75% v Large bowel obstruction: 25 to 35%.
v In these cases, accuracy and impact of MDCT with semiologic findings are well known by emergency radiologists.
v Upper intestinal obstruction i.e. gastro-duodenal obstruction: rare (1-2% of all bowel obstruction and poorly managed)
So the aim of this work is to review the specific causes of upper intestinal obstruction, illustrated by some cases with emphasis on MDCT semiological key-findings.
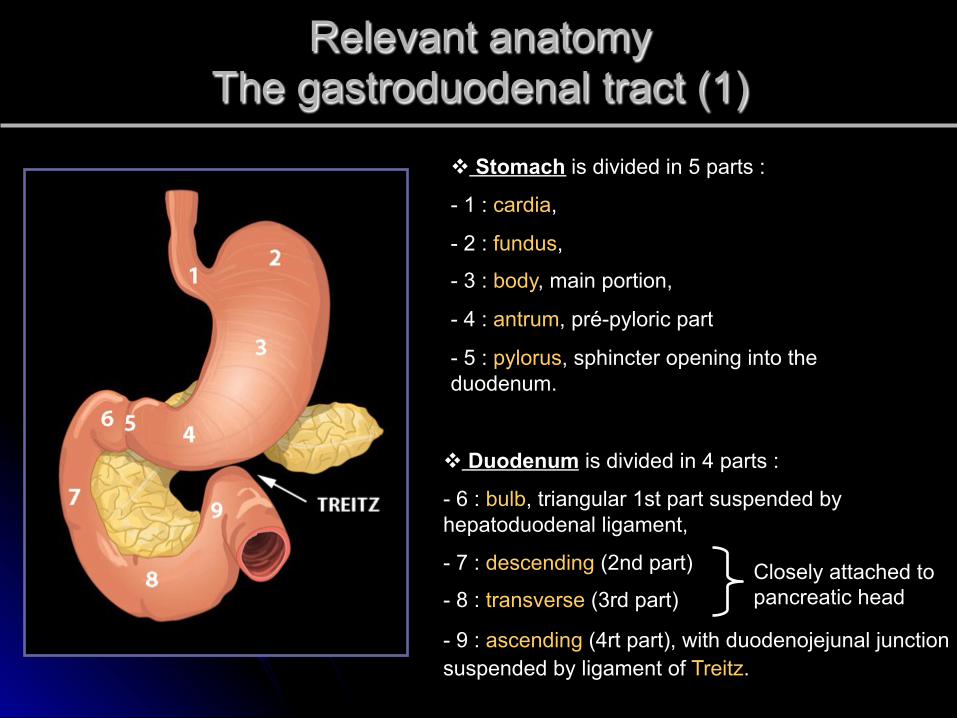
Relevant anatomy The gastroduodenal tract (1)
v Stomach is divided in 5 parts :
- 1 : cardia,
- 2 : fundus,
- 3 : body, main portion,
- 4 : antrum, pré-pyloric part
- 5 : pylorus, sphincter opening into the duodenum.
v Duodenum is divided in 4 parts :
- 6 : bulb, triangular 1st part suspended by hepatoduodenal ligament,
- 7 : descending (2nd part)
- 8 : transverse (3rd part)
- 9 : ascending (4rt part), with duodenojejunal junction suspended by ligament of Treitz.
Closely attached to pancreatic head
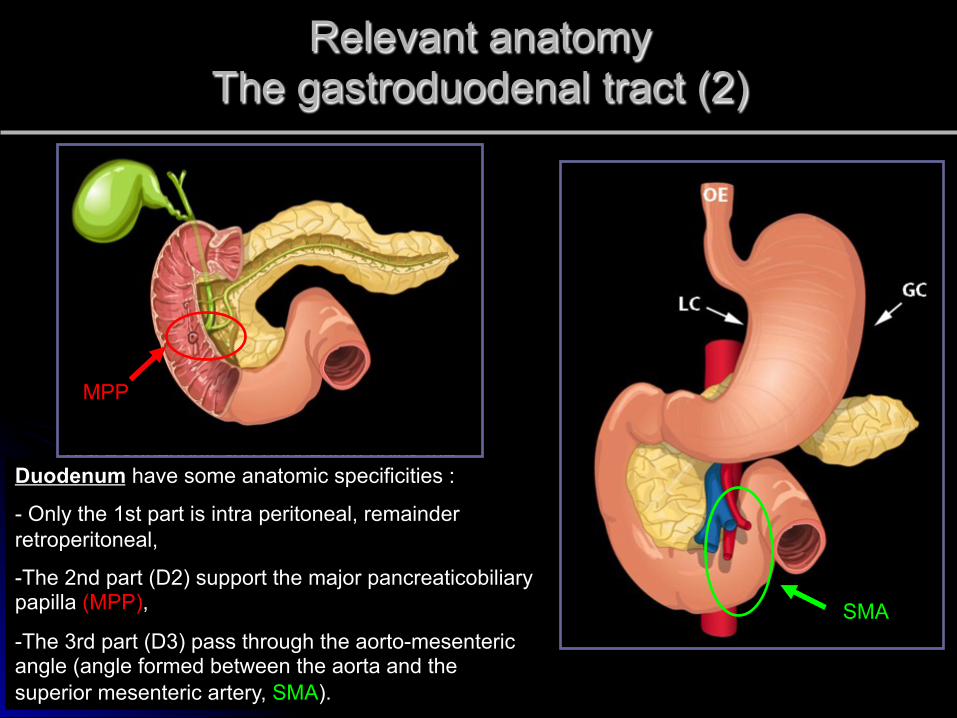
Relevant anatomy The gastroduodenal tract (2)
Stomach is suspended relatively and securely by gastric ligaments :
- gastrohepatic ligament along the lesser curvature (LC),
- gastrocolic and gastro splenic ligaments along the greater curvature (GC)
- gastrophrenic ligament along the posterior aspect of the fundus.
The esophagus (OE) holds the stomach in place superiorly and duodenum holds the stomach inferiorly. Duodenum have some anatomic specificities :
- Only the 1st part is intra peritoneal, remainder retroperitoneal,
- The 2nd part (D2) support the major pancreaticobiliary papilla (MPP),
- The 3rd part (D3) pass through the aorto-mesenteric angle (angle formed between the aorta and the superior mesenteric artery, SMA).
MPP
SMA
Acute gastro-duodenal obstruction versus gastroparesis
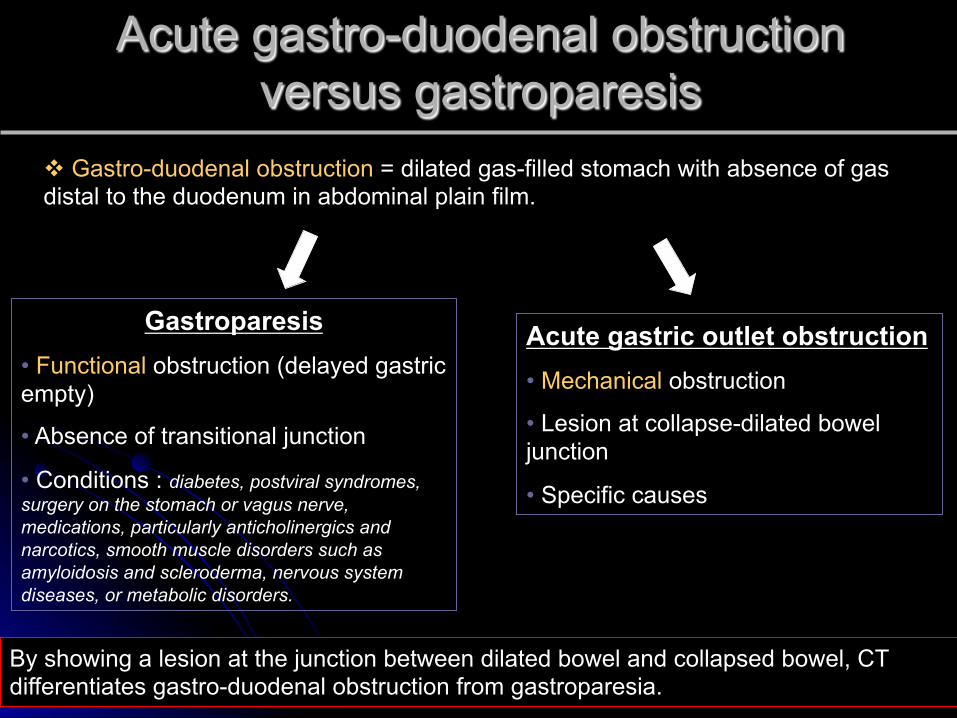
By showing a lesion at the junction between dilated bowel and collapsed bowel, CT differentiates gastro-duodenal obstruction from gastroparesia.
v Gastro-duodenal obstruction = dilated gas-filled stomach with absence of gas distal to the duodenum in abdominal plain film.
Gastroparesis
• Functional obstruction (delayed gastric empty)
• Absence of transitional junction
• Conditions : diabetes, postviral syndromes, surgery on the stomach or vagus nerve, medications, particularly anticholinergics and narcotics, smooth muscle disorders such as amyloidosis and scleroderma, nervous system diseases, or metabolic disorders.
Acute gastric outlet obstruction • Mechanical obstruction
• Lesion at collapse-dilated bowel junction
• Specific causes
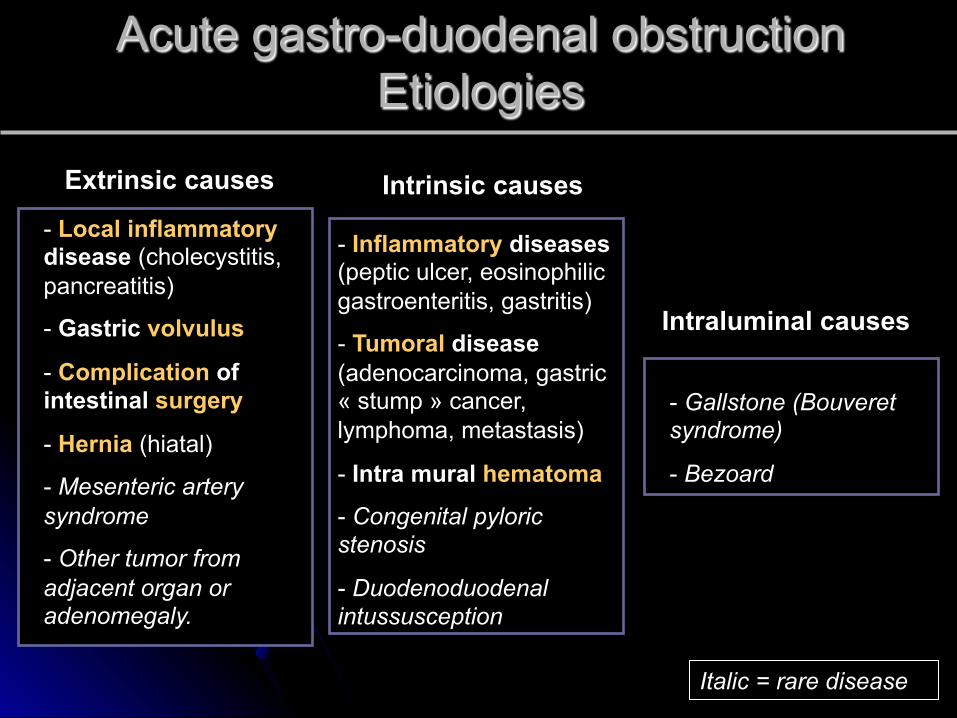
Acute gastro-duodenal obstruction Etiologies
Intrinsic causes Extrinsic causes
Intraluminal causes
- Gallstone (Bouveret syndrome)
- Bezoard
- Inflammatory diseases (peptic ulcer, eosinophilic gastroenteritis, gastritis)
- Tumoral disease (adenocarcinoma, gastric « stump » cancer, lymphoma, metastasis)
- Intra mural hematoma
- Congenital pyloric stenosis
- Duodenoduodenal intussusception
- Local inflammatory disease (cholecystitis, pancreatitis)
- Gastric volvulus
- Complication of intestinal surgery
- Hernia (hiatal)
- Mesenteric artery syndrome
- Other tumor from adjacent organ or adenomegaly.
Italic = rare disease
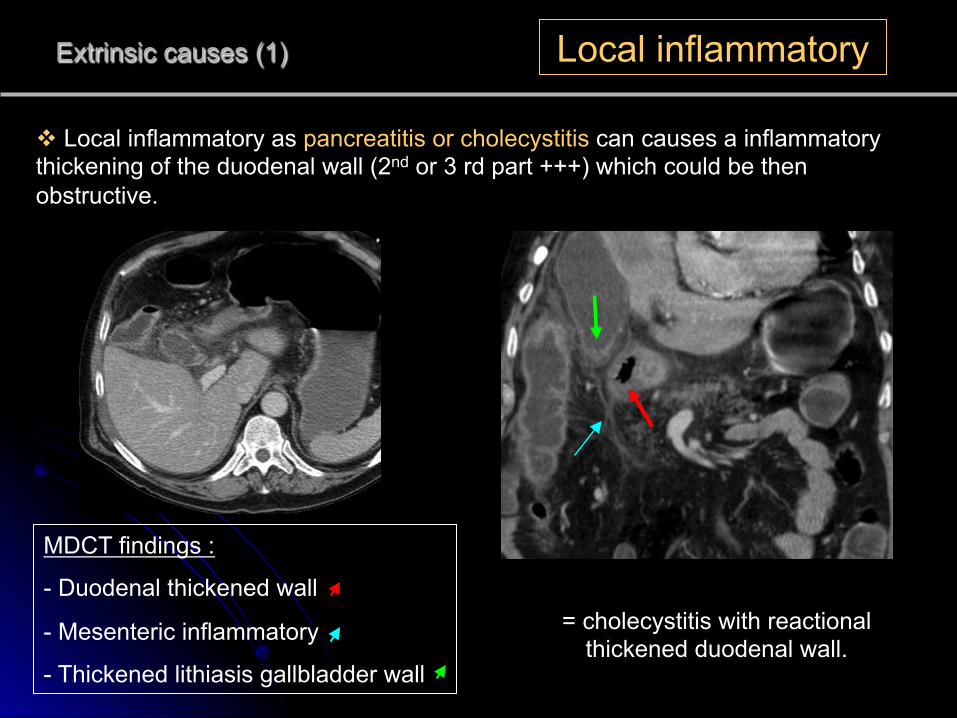
Extrinsic causes (1) Local inflammatory
v Local inflammatory as pancreatitis or cholecystitis can causes a inflammatory thickening of the duodenal wall (2nd or 3 rd part +++) which could be then obstructive.
MDCT findings :
- Duodenal thickened wall
- Mesenteric inflammatory
- Thickened lithiasis gallbladder wall
= cholecystitis with reactional thickened duodenal wall.
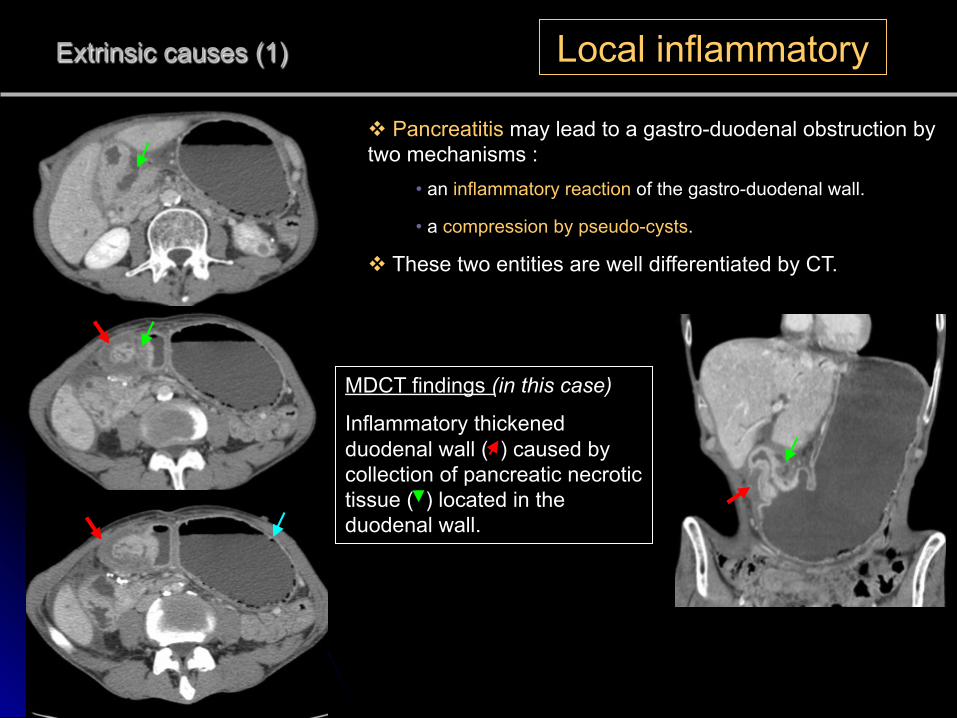
Extrinsic causes (1) Local inflammatory
v Pancreatitis may lead to a gastro-duodenal obstruction by two mechanisms :
• an inflammatory reaction of the gastro-duodenal wall.
• a compression by pseudo-cysts.
v These two entities are well differentiated by CT.
MDCT findings (in this case)
Inflammatory thickened duodenal wall ( ) caused by collection of pancreatic necrotic tissue ( ) located in the duodenal wall.
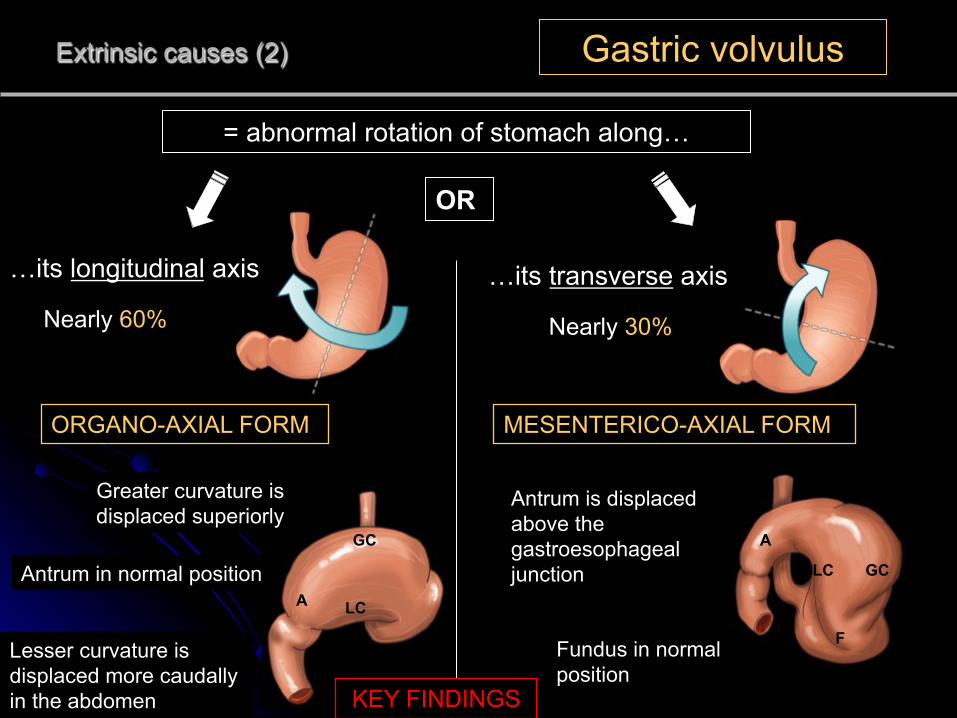
Extrinsic causes (2) Gastric volvulus
= abnormal rotation of stomach along…
…its transverse axis …its longitudinal axis
OR
Nearly 60% Nearly 30%
ORGANO-AXIAL FORM MESENTERICO-AXIAL FORM
A Antrum in normal position
Greater curvature is displaced superiorly
GC
Lesser curvature is displaced more caudally in the abdomen
LC
GC LC
A
Antrum is displaced above the gastroesophageal junction
F Fundus in normal position
KEY FINDINGS
Extrinsic causes (2) Gastric volvulus
v The rotation must be greater than 180° for generate a gastric obstruction.
v It is more commonly secondary (paraoesophagal hiatus hernia, traumatic diaphragmatic hernia, eventration of the diaphragm abdominal bands or adhesion).
v Predominantly in older adults.
v Symptoms = triad of Borchardt 1. severe and sudden gastric pain
2. an episode of vomiting followed by retching without the ability to vomit
3. difficulty or inability to pass a nasogastric tube.
v Treatment : surgical repair in emergency, gastric ischemia risk.
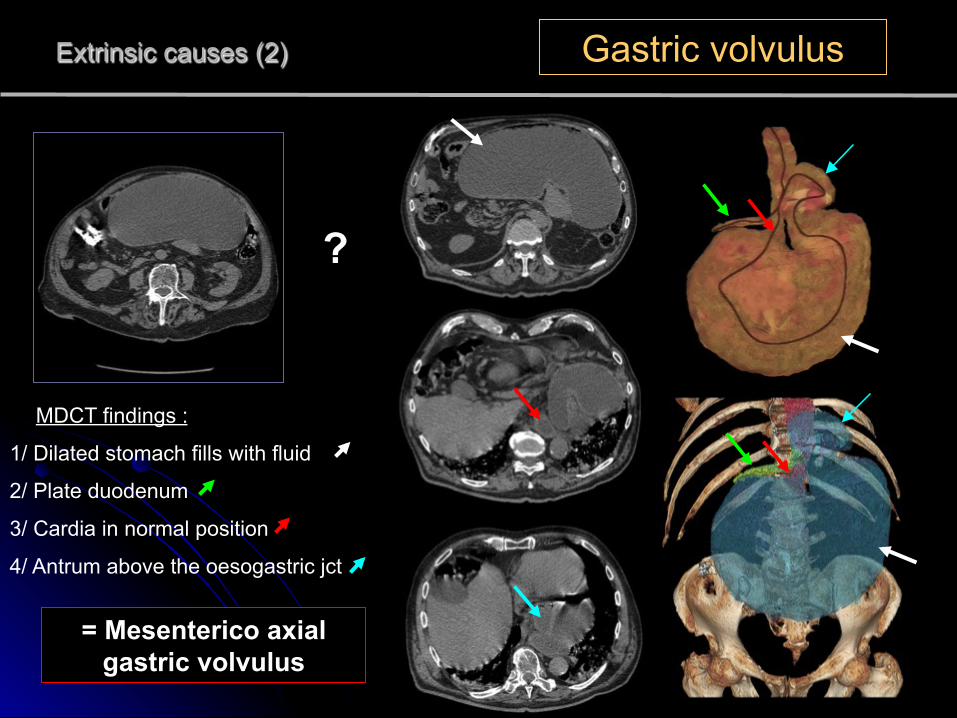
MDCT findings :
Extrinsic causes (2) Gastric volvulus
?
= Mesenterico axial gastric volvulus
1/ Dilated stomach fills with fluid
2/ Plate duodenum
3/ Cardia in normal position
4/ Antrum above the oesogastric jct
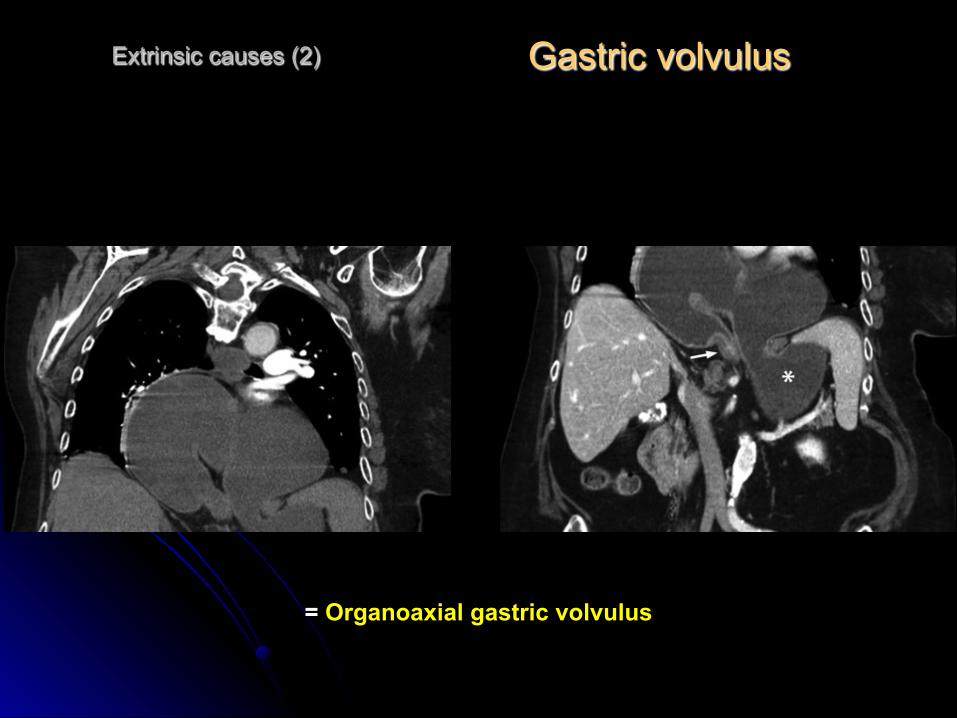
Gastric volvulus
Extrinsic causes (2)
= Organoaxial gastric volvulus
Extrinsic causes (2) Gastric volvulus
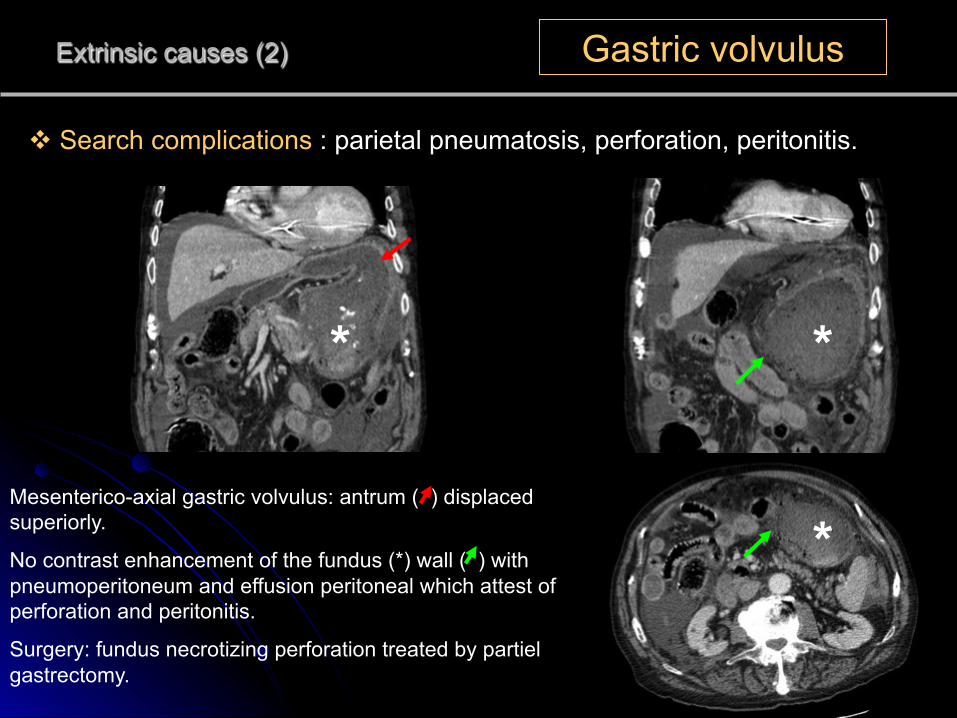
v Search complications : parietal pneumatosis, perforation, peritonitis.
Mesenterico-axial gastric volvulus: antrum ( ) displaced superiorly.
No contrast enhancement of the fundus (*) wall ( ) with pneumoperitoneum and effusion peritoneal which attest of perforation and peritonitis.
Surgery: fundus necrotizing perforation treated by partiel gastrectomy.
* *
*
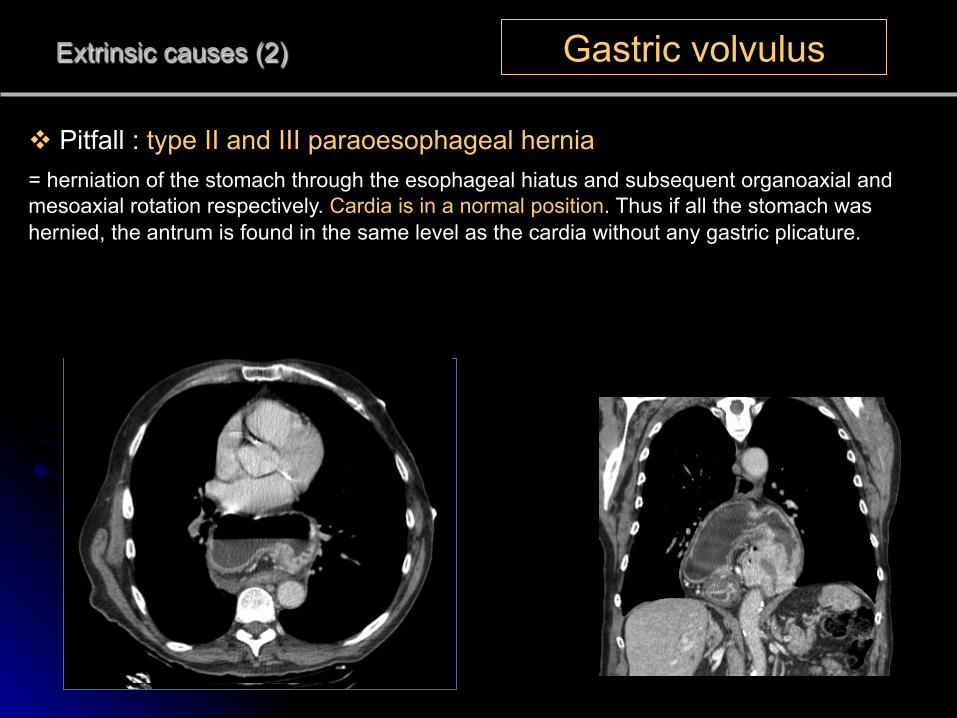
Extrinsic causes (2) Gastric volvulus
v Pitfall : type II and III paraoesophageal hernia = herniation of the stomach through the esophageal hiatus and subsequent organoaxial and mesoaxial rotation respectively. Cardia is in a normal position. Thus if all the stomach was hernied, the antrum is found in the same level as the cardia without any gastric plicature.
Extrinsic causes (3) Surgical complication
v Post operative stenosis: increasing cause of gastric obstruction since the development of bariatric surgery.
v Reported incidence is up to 5%.
v The main localisation of stenosis is in the gastrojejunal anastomosis.
EARLY post operative setting
• severe edema
• overzealous suturing
LATE post operative setting
• fibrotic stenosis
• internal hernias
• adhesions
v Barium oesophagography could be as suggestive as CT.
Extrinsic causes (3) Surgical complication
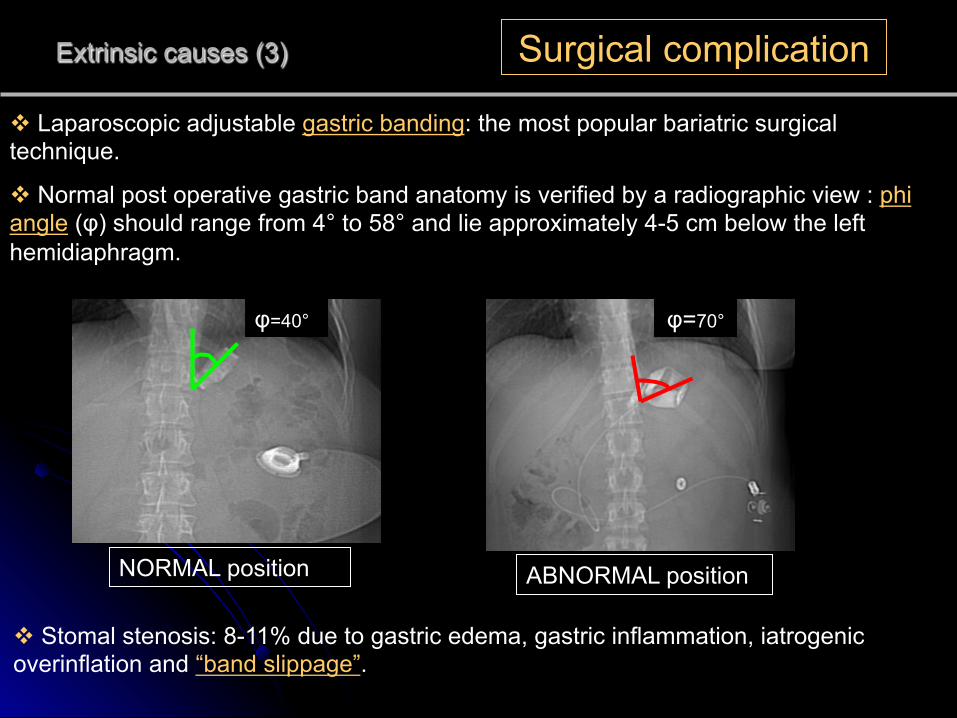
v Laparoscopic adjustable gastric banding: the most popular bariatric surgical technique.
v Normal post operative gastric band anatomy is verified by a radiographic view : phi angle (φ) should range from 4° to 58° and lie approximately 4-5 cm below the left hemidiaphragm.
φ=70° φ=40°
NORMAL position ABNORMAL position
v Stomal stenosis: 8-11% due to gastric edema, gastric inflammation, iatrogenic overinflation and “band slippage”.
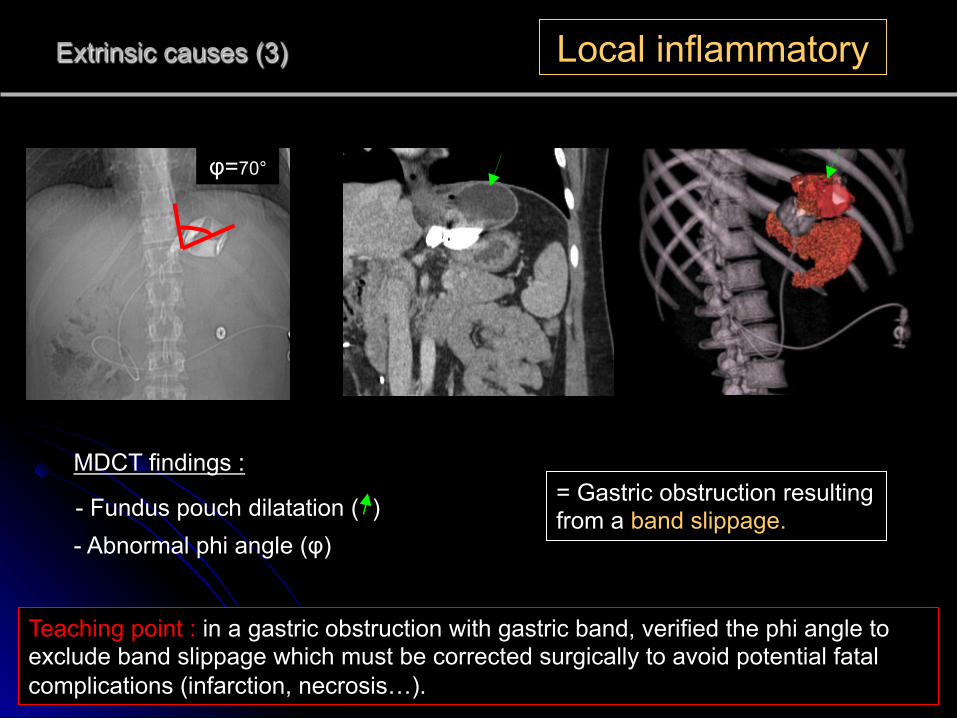
Extrinsic causes (3) Local inflammatory
Teaching point : in a gastric obstruction with gastric band, verified the phi angle to exclude band slippage which must be corrected surgically to avoid potential fatal complications (infarction, necrosis…).
= Gastric obstruction resulting from a band slippage.
MDCT findings :
- Fundus pouch dilatation ( )
φ=70°
- Abnormal phi angle (φ)
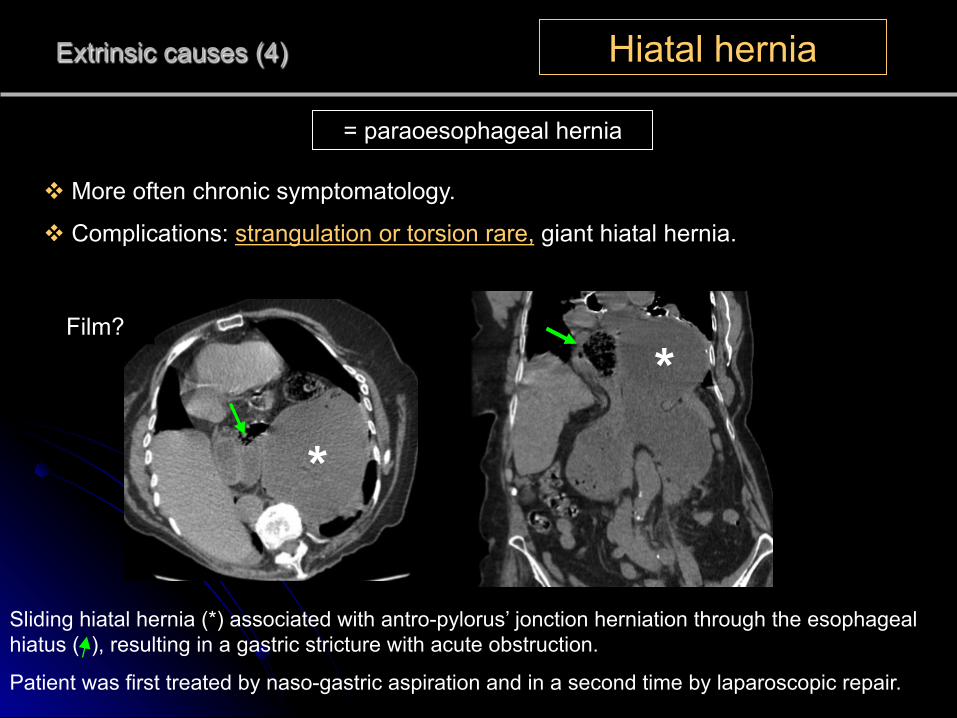
Extrinsic causes (4) Hiatal hernia
v More often chronic symptomatology.
v Complications: strangulation or torsion rare, giant hiatal hernia.
Sliding hiatal hernia (*) associated with antro-pylorus’ jonction herniation through the esophageal hiatus ( ), resulting in a gastric stricture with acute obstruction.
Patient was first treated by naso-gastric aspiration and in a second time by laparoscopic repair.
*
*
= paraoesophageal hernia
Film?
Extrinsic causes (5) Mesenteric artery syndroma
= compression of the 3rd duodenum between superior mesenteric artery and aorta
v 2/3 female, average 41 ans
v Predisposing conditions : • a rapid and dramatic weight loss with decrease in the retroperitoneal and mesenteric fat
• dystonic enervation of the abdominal wall and spinal muscles
• disease or trauma to the spine (spinal traction, lumbar hyperlordosis)
v Symptoms = post prandial epigastric pain, eructation, fullness, voluminous vomiting of partially digested food.
v More often it appears as a chronic condition more than a acute illness.
v Treatment : medical intervention first and sometimes surgical.
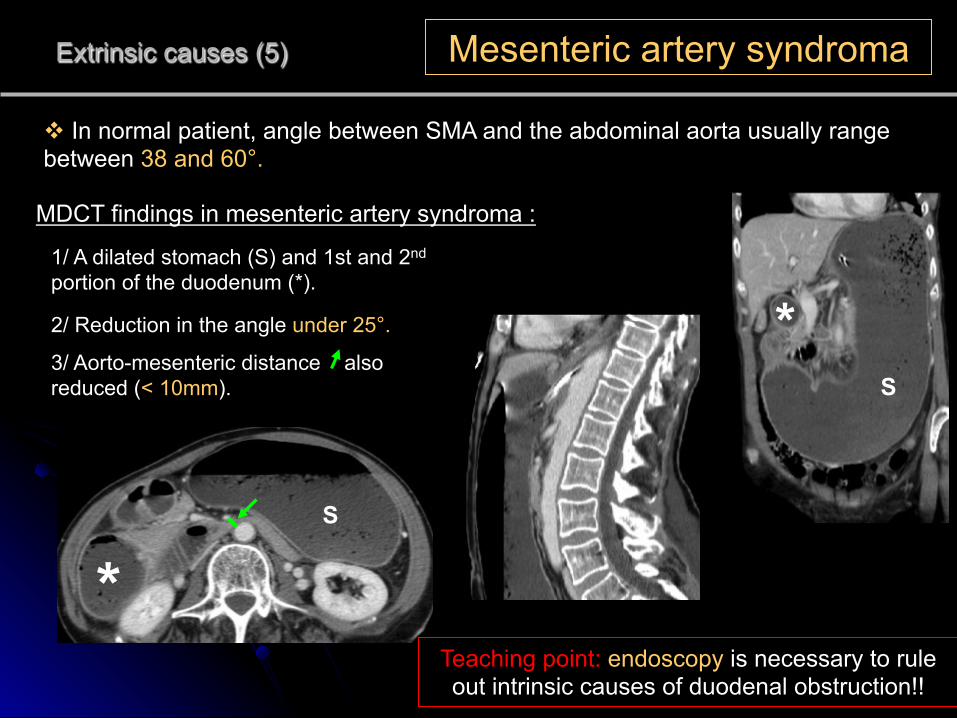
Extrinsic causes (5) Mesenteric artery syndroma
v In normal patient, angle between SMA and the abdominal aorta usually range between 38 and 60°.
MDCT findings in mesenteric artery syndroma :
2/ Reduction in the angle under 25°.
1/ A dilated stomach (S) and 1st and 2nd portion of the duodenum (*).
S
S
*
*3/ Aorto-mesenteric distance also reduced (< 10mm).
Teaching point: endoscopy is necessary to rule out intrinsic causes of duodenal obstruction!!
Extrinsic causes (6) Extrinsic mass
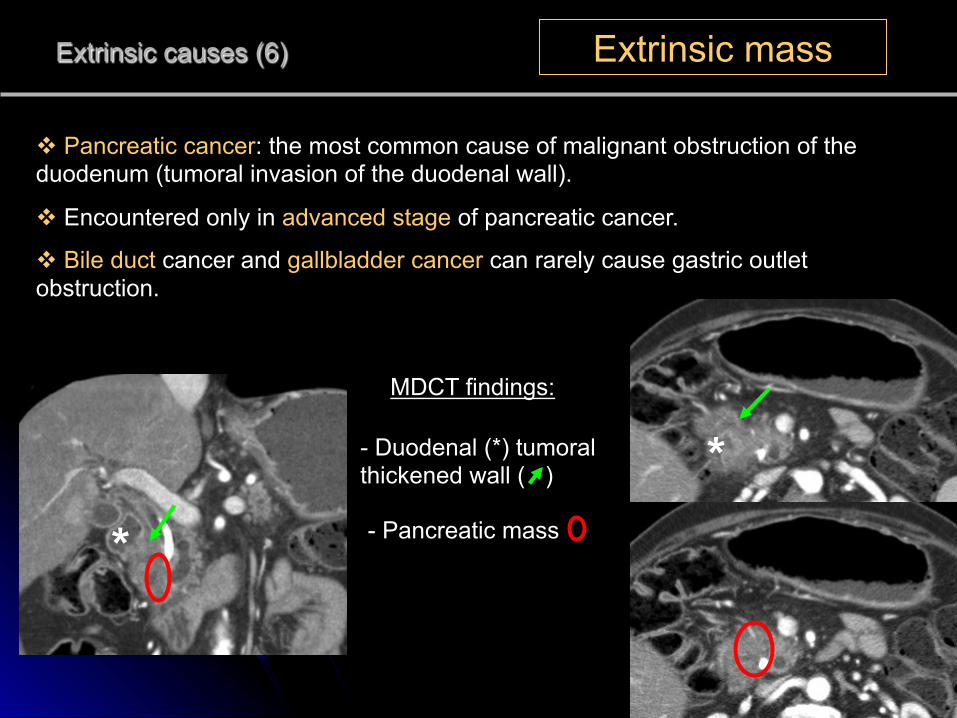
v Pancreatic cancer: the most common cause of malignant obstruction of the duodenum (tumoral invasion of the duodenal wall).
v Encountered only in advanced stage of pancreatic cancer.
v Bile duct cancer and gallbladder cancer can rarely cause gastric outlet obstruction.
MDCT findings:
- Duodenal (*) tumoral thickened wall ( )
- Pancreatic mass *
*
Extrinsic causes (6) Extrinsic mass
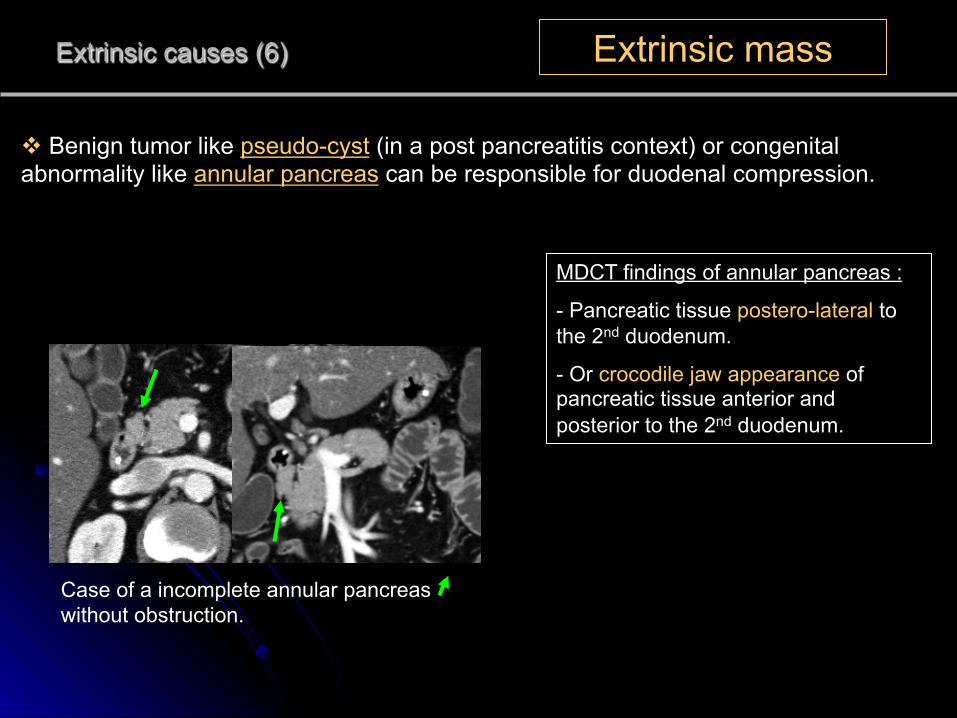
v Benign tumor like pseudo-cyst (in a post pancreatitis context) or congenital abnormality like annular pancreas can be responsible for duodenal compression.
Case of a incomplete annular pancreas without obstruction.
MDCT findings of annular pancreas :
- Pancreatic tissue postero-lateral to the 2nd duodenum.
- Or crocodile jaw appearance of pancreatic tissue anterior and posterior to the 2nd duodenum.
Intrinsic causes (1) Inflammatory disease
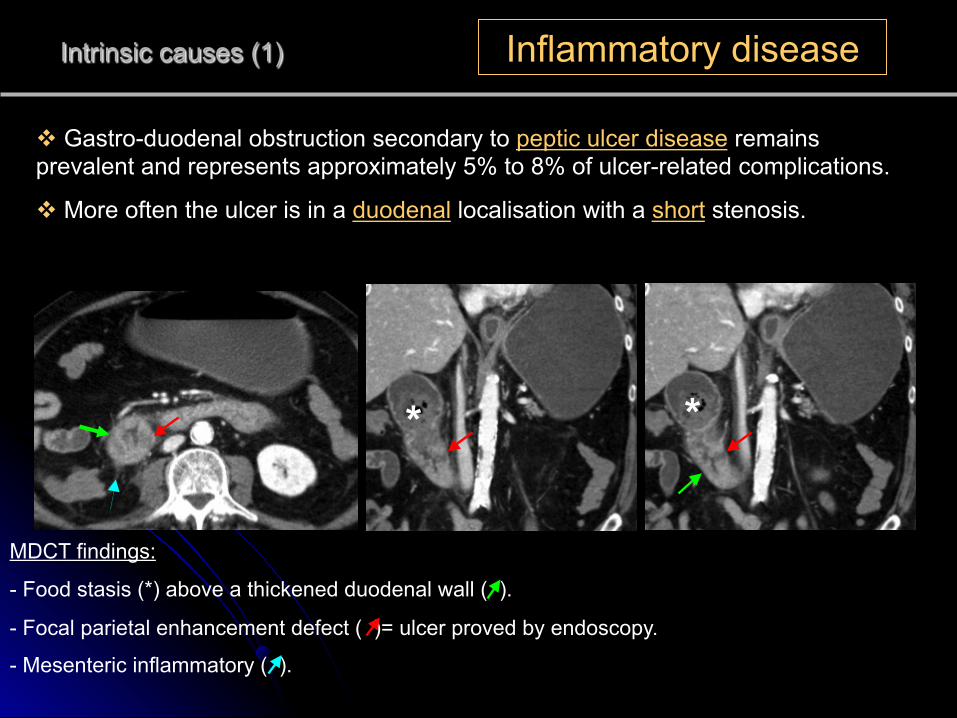
v Gastro-duodenal obstruction secondary to peptic ulcer disease remains prevalent and represents approximately 5% to 8% of ulcer-related complications.
v More often the ulcer is in a duodenal localisation with a short stenosis.
MDCT findings:
- Food stasis (*) above a thickened duodenal wall ( ).
- Focal parietal enhancement defect ( )= ulcer proved by endoscopy.
- Mesenteric inflammatory ( ).
* *
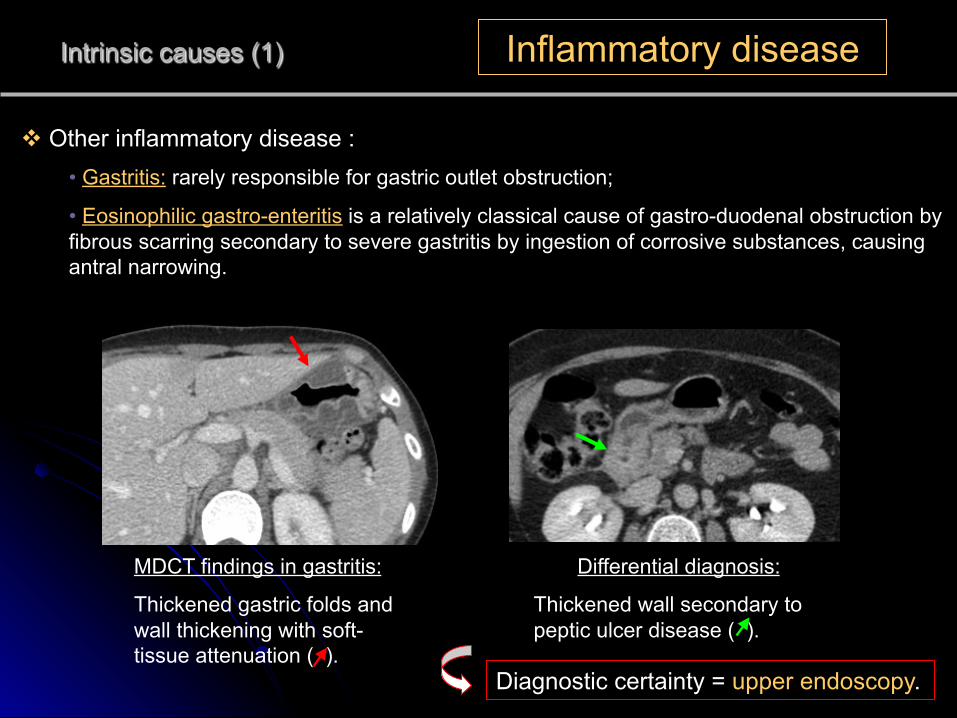
v Other inflammatory disease : • Gastritis: rarely responsible for gastric outlet obstruction;
• Eosinophilic gastro-enteritis is a relatively classical cause of gastro-duodenal obstruction by fibrous scarring secondary to severe gastritis by ingestion of corrosive substances, causing antral narrowing.
Intrinsic causes (1) Inflammatory disease
MDCT findings in gastritis:
Thickened gastric folds and wall thickening with soft-tissue attenuation ( ).
Differential diagnosis:
Thickened wall secondary to peptic ulcer disease ( ).
Diagnostic certainty = upper endoscopy.
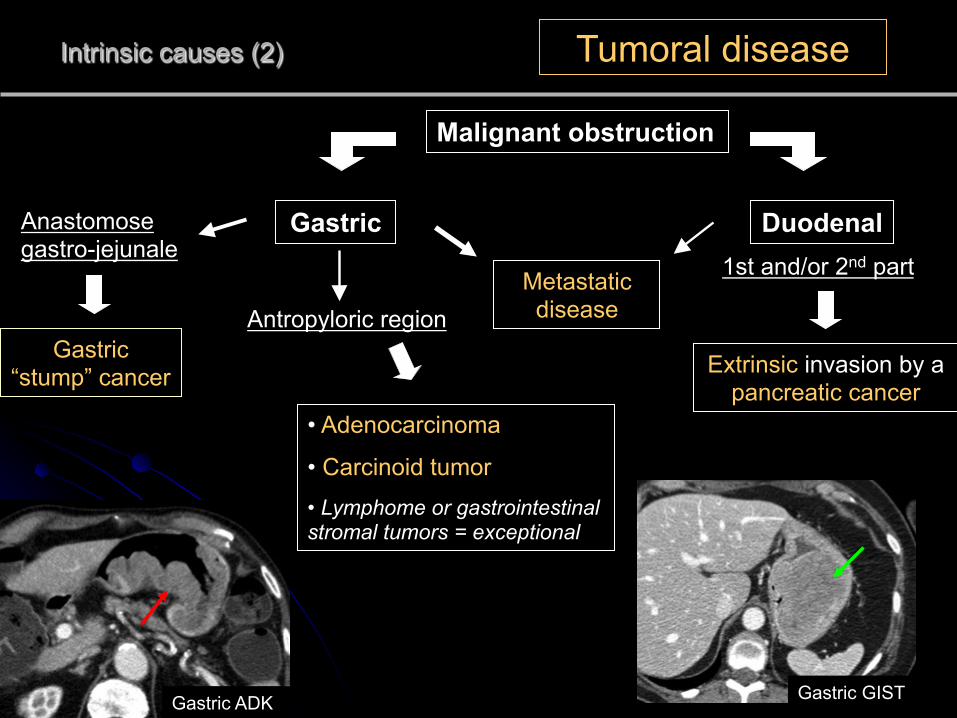
Intrinsic causes (2) Tumoral disease
Malignant obstruction
Gastric Duodenal
Antropyloric region
1st and/or 2nd part
• Adenocarcinoma
• Carcinoid tumor • Lymphome or gastrointestinal stromal tumors = exceptional
Extrinsic invasion by a pancreatic cancer
Metastatic disease
Gastric GIST
Gastric “stump” cancer
Anastomose gastro-jejunale
Gastric ADK
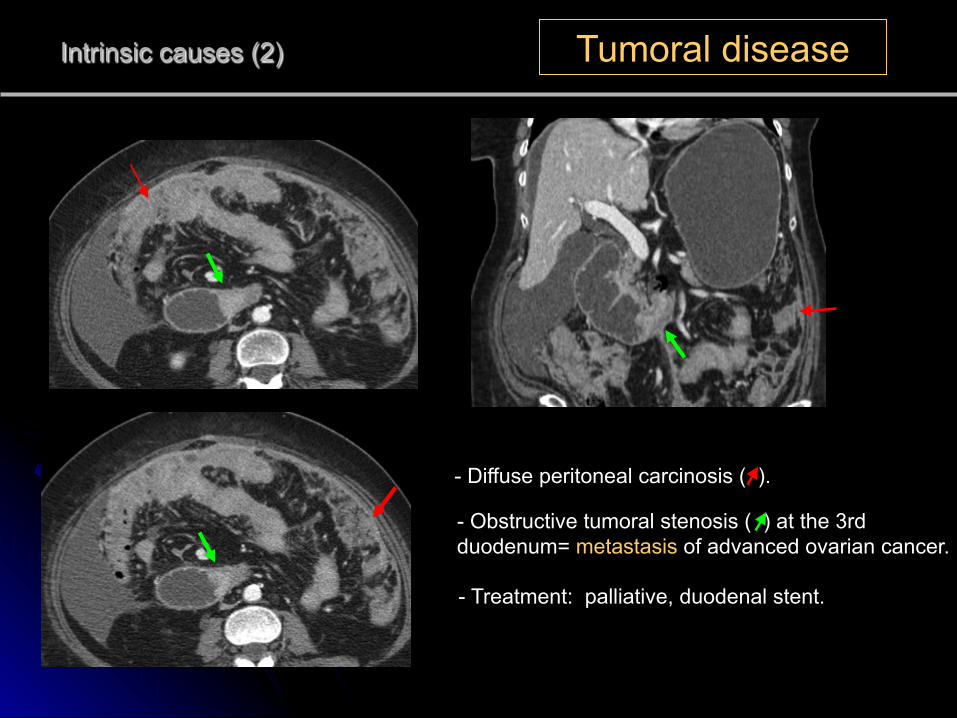
- Diffuse peritoneal carcinosis ( ).
Intrinsic causes (2) Tumoral disease
- Obstructive tumoral stenosis ( ) at the 3rd duodenum= metastasis of advanced ovarian cancer.
- Treatment: palliative, duodenal stent.
Intrinsic causes (3) Intramural hematoma
v Reach essentially the 2nd and 3rd part of the duodenum.
v Most common factors: blunt trauma, anticoagulant therapy, Henoch-Schonlein purpura, and blood dyscrasias.
v Classical in childhood : bike falls with direct abdominal trauma on handlebars/ or child abuse (by epigastric direct blow).
v Resolve spontaneously with conservative treatment, sometimes surgical intervention (endoscopic drainage) is possible if medical treatment failed.
Teaching point : On MDCT, search severity signs and complications as perforation or extravasation of enteric or vascular contrast medium which requires surgery in emergency.
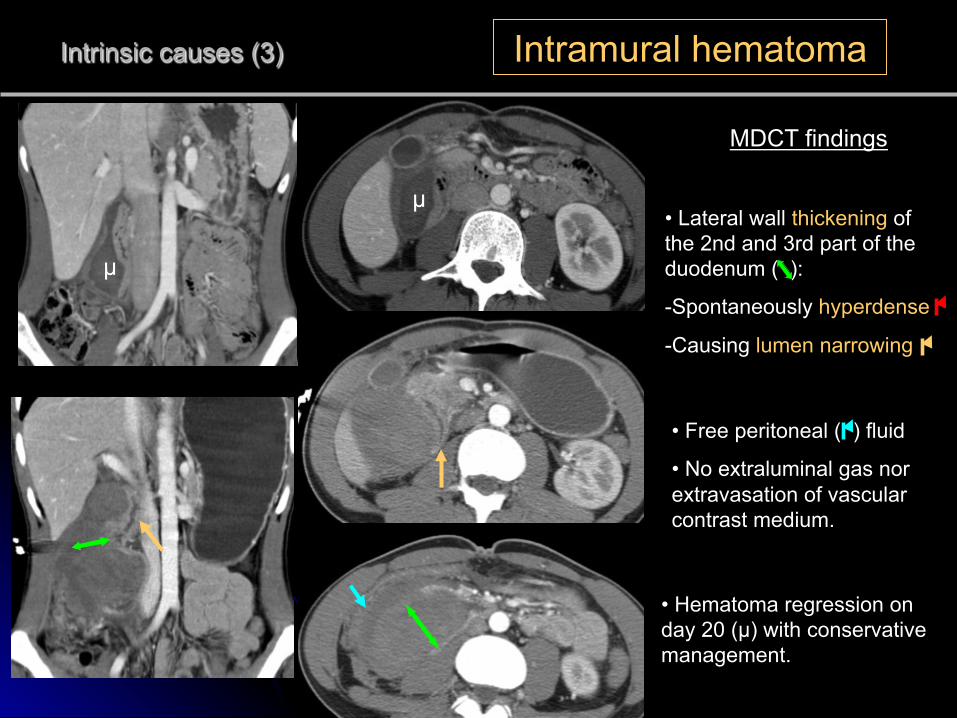
• Free peritoneal ( ) fluid
• No extraluminal gas nor extravasation of vascular contrast medium.
Intrinsic causes (3) Intramural hematoma
MDCT findings
• Lateral wall thickening of the 2nd and 3rd part of the duodenum ( ):
- Spontaneously hyperdense
- Causing lumen narrowing
• Hematoma regression on day 20 (µ) with conservative management.
µ
µ
Intrinsic causes (5) Duodenal intussusception
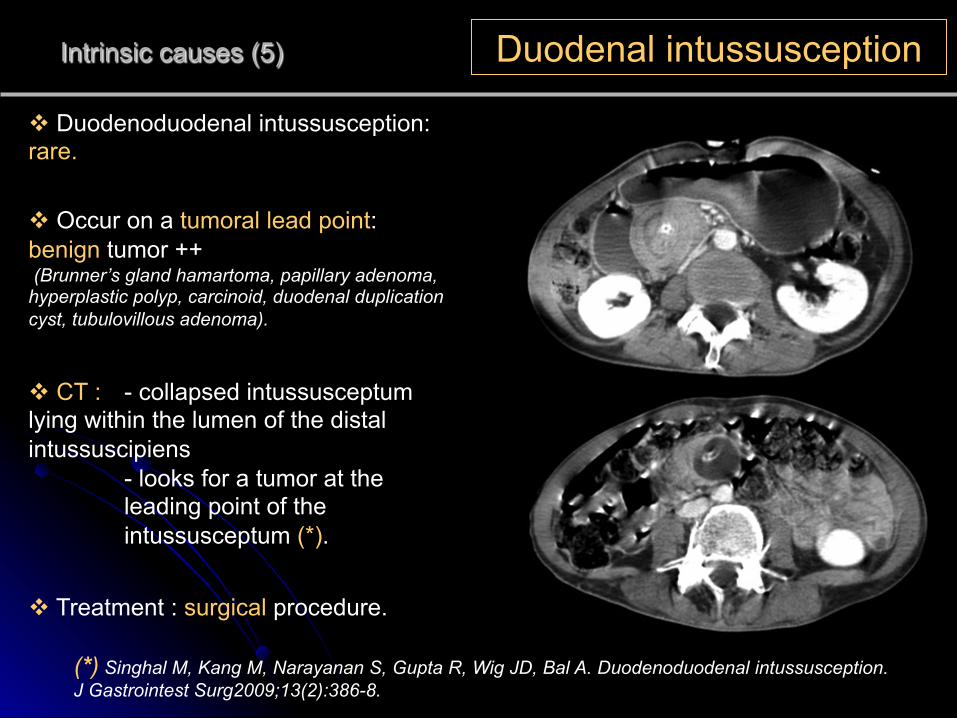
v Duodenoduodenal intussusception: rare.
v Occur on a tumoral lead point: benign tumor ++ (Brunner’s gland hamartoma, papillary adenoma, hyperplastic polyp, carcinoid, duodenal duplication cyst, tubulovillous adenoma).
v CT : - collapsed intussusceptum lying within the lumen of the distal intussuscipiens
- looks for a tumor at the leading point of the intussusceptum (*).
v Treatment : surgical procedure.
(*) Singhal M, Kang M, Narayanan S, Gupta R, Wig JD, Bal A. Duodenoduodenal intussusception. J Gastrointest Surg2009;13(2):386-8.
Intraluminal causes (1) Gallstone
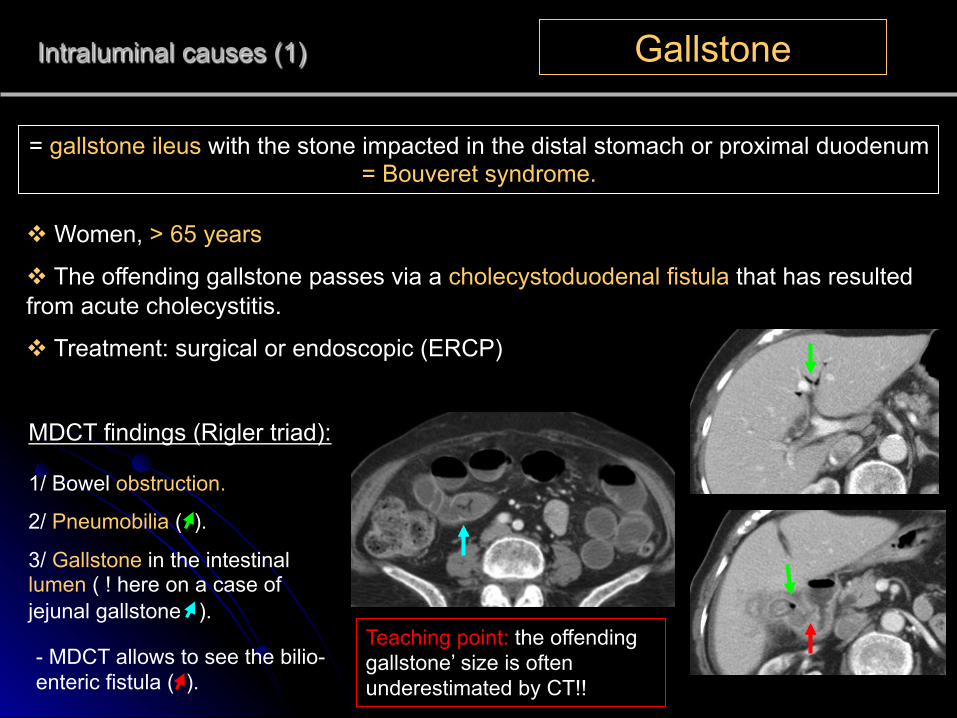
= gallstone ileus with the stone impacted in the distal stomach or proximal duodenum = Bouveret syndrome.
MDCT findings (Rigler triad):
1/ Bowel obstruction.
2/ Pneumobilia ( ).
3/ Gallstone in the intestinal lumen ( ! here on a case of jejunal gallstone ).
v Women, > 65 years
v The offending gallstone passes via a cholecystoduodenal fistula that has resulted from acute cholecystitis.
v Treatment: surgical or endoscopic (ERCP)
- MDCT allows to see the bilio-enteric fistula ( ).
Teaching point: the offending gallstone’ size is often underestimated by CT!!
Extra-Intraluminal causes (2)
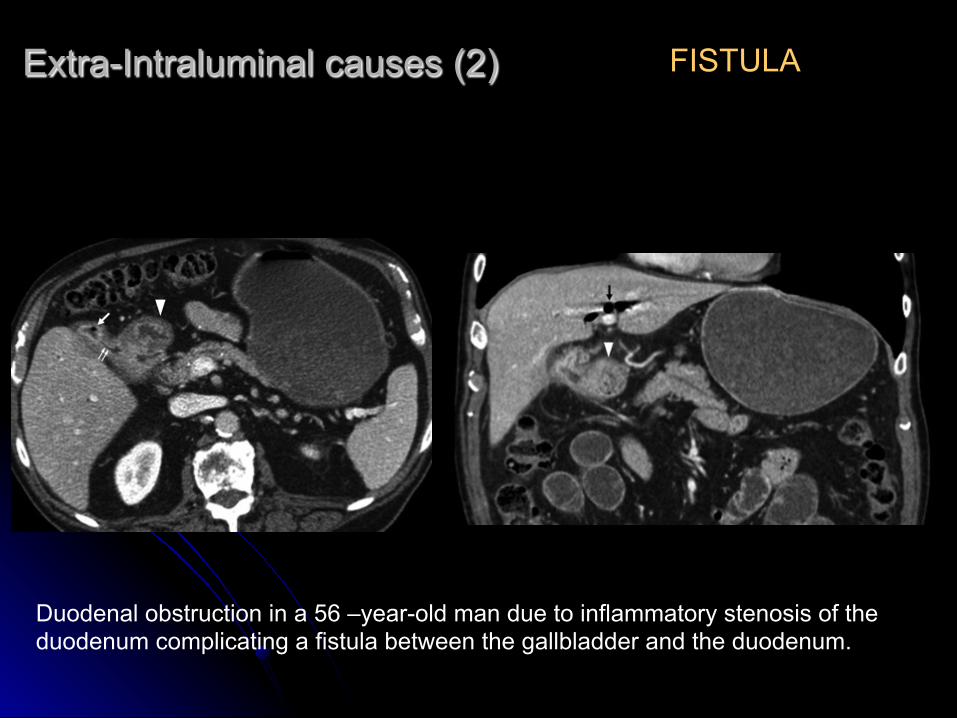
Duodenal obstruction in a 56 –year-old man due to inflammatory stenosis of the duodenum complicating a fistula between the gallbladder and the duodenum.
FISTULA
Intraluminal causes (2) Bezoard
v Mostly more common in the stomach rather than in the duodenum.
2/ Trichobezoard - concretion of hair fibres
- young women with psychiatric disorders (trichotillomania) or children with mental retardation.
1/ Phytobezoard - concretion of poorly digested fruit and vegetable fibres
- gastric surgical history or a gastroparesis.
3/ Pharmacobezoars medication bezoars which adhere when in bulk
(cholestyramine, kayexalate resin, cavafate and antacids)
v Treatment : conservative (chemical substances / mechanical fragmentation) or surgical extraction.
3 types
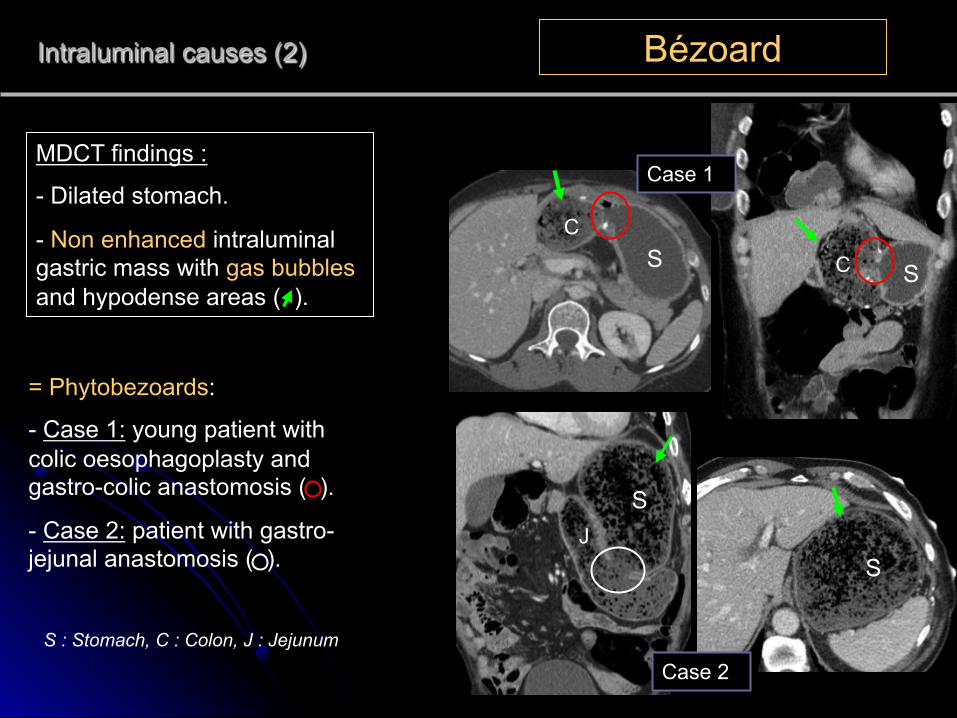
Intraluminal causes (2) Bézoard
MDCT findings :
- Dilated stomach.
- Non enhanced intraluminal gastric mass with gas bubbles and hypodense areas ( ).
Case 1
Case 2
= Phytobezoards:
- Case 1: young patient with colic oesophagoplasty and gastro-colic anastomosis ( ).
- Case 2: patient with gastro-jejunal anastomosis ( ).
S : Stomach, C : Colon, J : Jejunum
S S
S
S
C
C
J
CONCLUSION
v Acute gastro-duodenal obstruction is rare.
v MDCT confirm that is a true obstruction and determine its level, its cause and its severity to allow a good management either medically or surgically.
v Malignant lesion and peptic ulcer disease are the two main causes of gastric outlet obstruction.