Embed Size (px)
Citation preview
Official Publication of Dr. DY Patil Vidyapeeth Society, Pune
Volume 9 / Issue 4 / July-August 2016
ISSN: 0975-2870
Medical Journal of
Dr.DY Patil University
www.mjdrdypu.org
Medical Journal of D
r. D.Y. P
atil Un
iversity • Volum
e 9 • Issue 4 • July-A
ug
ust 2016 • P
ages 427-***
spine6.5
© 2016 Medical Journal of Dr. D.Y. Patil University | Published by Wolters Kluwer - Medknow 541
Introduction
Pulmonary arteriovenous (PAV) fistulae are an abnormal communication between the pulmonary artery and vein at intrapulmonary level. Although these lesions are not a common clinical problem, sometimes, they may present like cyanotic heart diseases. The etiology of this disease is usually congenital; however, they may be acquired in certain conditions, such as mitral stenosis, schistosomiasis, tuberculosis, trauma, and metastatic thyroid carcinoma. Some patients have hereditary hemorrhagic telangiectasia (HHT) also known as Rendu‑Osler‑Weber syndrome; however, in our case after a meticulous search, no cause was identified.
Case Report
We are presenting a rare case of a 14‑year‑old female admitted to our hospital with complaints of having cyanosis, dyspnea at rest, palpitation, orthopnea, and two episodes of hemoptysis. She had history from 1 year,
Pulmonary arteriovenous fistula mimicking as acyanotic heart disease with shunt reversalKeshri Singh Yadav, Balvir Singh, Mridul ChaturvediDepartment of Medicine, S.N. Medical College, Agra, Uttar Pradesh, India
ABSTRACTPulmonaryarteriovenousmalformations(PAVMs)orpulmonaryarteriovenous(PAV)fistulaarerelativelyrarepulmonaryvasculardisorders. Although most of the patients are asymptomatic,PAVMscancausedyspnea,clubbing,andcentralcyanosisandisan importantdifferentialdiagnosisofcommoncardiopulmonaryproblems,suchashypoxemiaandcongenitalheartdiseaseswithreversalofshunt.ThereisastrongassociationbetweenPAVMandhereditaryhemorrhagictelangiectasia.Chestradiography,contrastechocardiography,andcontrastenhancedcomputed tomographyareimportantinitialdiagnostictools,butpulmonaryangiographyisthegoldstandard.Therapeuticoptionsincludeangiographiccoilembolizationorballoonocclusionandsurgicalexcision.
Keywords:Hereditaryhemorrhagictelangiectasia,pulmonaryarteriovenousmalformations,acyanoticheartdisease,pulmonaryangiography
Access this article online
Quick Response Code:Website:
www.mjdrdypu.org
DOI:
10.4103/0975-2870.186077
Case Report
without any significant past or family history. There was no history of cough with expectoration, squatting, fever. There was no pallor, icterus, lymphadenopathy, or oronasal telangiectasia.
On general examination, she had central as well as peripheral cyanosis [Figure 1], clubbing of Grade 2 [Figure 2], bilateral pedal edema, blood pressure 112/52 mm Hg, pulse rate 146/min, regular, respiratory rate 24/min, and body mass index 16.8 kg/m2. On auscultation, there was bilateral diffuse wheeze present. In cardiovascular system examination, apex was in the left 5th intercostal space in midclavicular line. A grade 2 pansystolic murmur was present in the left parasternal area. The chest X‑ray film revealed cardiomegaly, with right ventricular hypertrophy type apex.
On blood examination, Hb 16.5 g/dl; total leukocyte count 11150/mm3; platelet count 4.5 lacs/mm3; aspartate
Address for correspondence: Dr. Keshri Singh Yadav, Department of Medicine, S.N. Medical College, Agra - 282 002, Uttar Pradesh, India. E-mail: [email protected]
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.
For reprints contact: [email protected]
How to cite this article: Yadav KS, Singh B, Chaturvedi M. Pulmonary arteriovenous fistula mimicking as acyanotic heart disease with shunt reversal. Med J DY Patil Univ 2016;9:541-3.

Yadav, et al.: PAV fistula mimicking as acyanotic heart disease with shunt reversal
542 Medical Journal of Dr. D.Y. Patil University | July-August 2016 | Vol 9 | Issue 4
aminotransferase 69.0 U/L; alanine aminotransferase 120 U/L; serum bilirubin 1.2 mg/dl; serum creatinine 1.2 mg/dl; blood urea 49 mg/dl; sodium 136 mEq/L; potassium 3.3 mEq/L; HIV, hepatitis B, and hepatitis C were nonreactive. Urine examination was within normal limit. Sputum acid‑fast Bacilli smears and blood culture were negative.
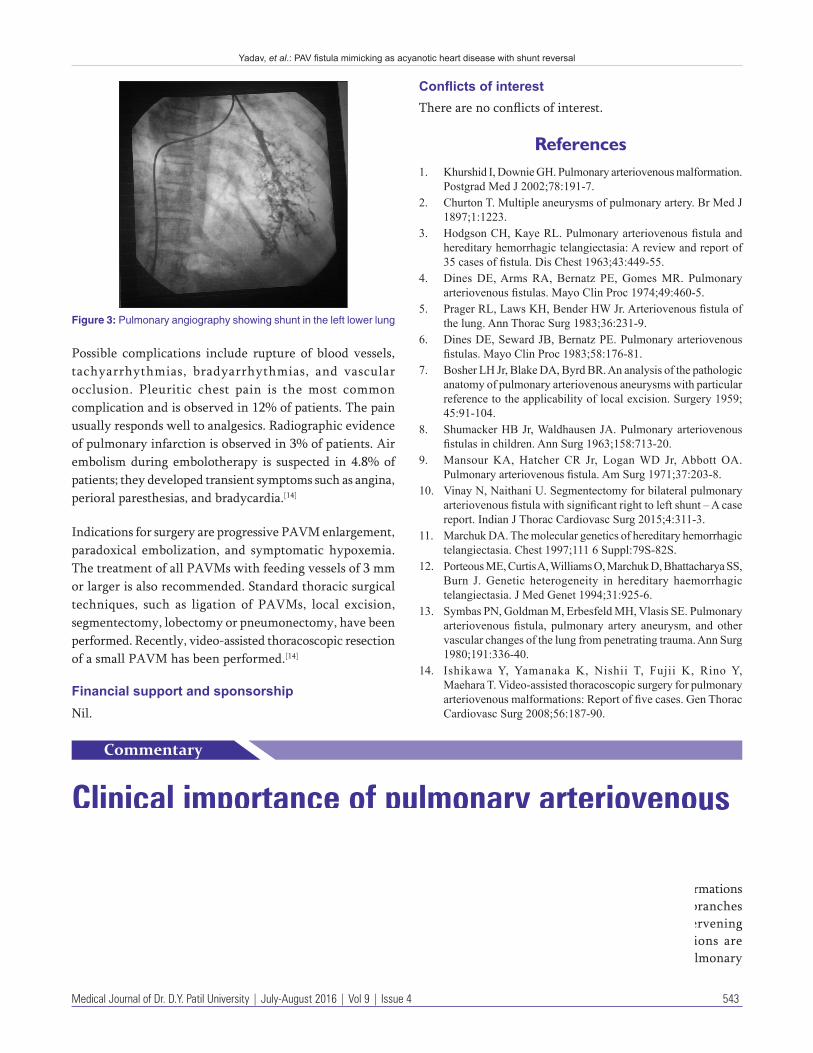
Echocardiography showed normal left ventricular dimension with normal wall motion contractility and systolic function with dilated coronary sinus; however, after putting contrast, it appears in the left atrium after 4‑6 beats suggesting shunting beyond the cardiac level with no evidence of dissection, normal pulmonary artery pressure with mild tricuspid regurgitation. Patient had undergone pulmonary angiography which revealed left lower lobe PAV fistula [Figure 3].
After confirmation of diagnosis, the patient was sent to higher center for coil embolization and patient is not alright after treatment. The prognosis of patients with HHT is not as good as for those without HHT. For patients without HHT, surgery to remove the abnormal vessels usually has good outcome and the condition is not likely to return.
Discussion
Although pulmonary arteriovenous malformation (PAVM) is considered an unusual rare lesion,[1] cases have been reported as early as 1897 by Churton.[2] The diagnosis of PAVM is a very challenging to physicians. PAVMs are direct shunts between the smaller pulmonary arteries and veins. These are lesions in the vasculature that allow blood to bypass the capillary system, flowing from the high‑pressure system to low pressure system, i.e., arteries to the
veins. The lesions are mostly congenital in nature and are caused by failure of differentiation of the embryonic vascular plexus. The incidence of PAVMs is 2‑3/100,000 population[3] with slightly female dominance. The male:female ratio varies from 1:1.5 to 1.8 in several series.[4] The age at first presentation varies from newborn period to 70 years, but the majority of the cases are diagnosed in the first three decades.[5,6]
They may be single or multiple and the incidence of single PAVM varies from 42.0% to 74.0%.[7,8] Most solitary PAVMs are seen in bilateral lower lobes, the left lower lobe being the most common location, followed by right lower lobe, left upper lobe, right middle lobe, and right upper lobe.[7,8] The majority of multiple PAVMs are also confined to bilateral lower lobes; the incidence of bilateral PAVMs ranges from 8.0% to 20.0%.[9] More than 80% of PAVMs are congenital,[4,7] the remaining being acquired. The acquired PAVMs are very rare and are caused by chest trauma, surgery, cirrhosis of liver, metastatic carcinoma, and infections. They may present with complications such as cerebral embolism or brain abscess.[10‑13] The incidence of PAVMs apparently varies according to the specific gene alterations.[11] The genetic etiological linkages to HHT are located on chromosome 9 (9q 33‑34 or OWR‑1) in some families and on chromosome 12 (12q or OWR‑2) in others.[11]
Embolization therapy is the treatment of choice and indicated in patients with multiple or bilateral PAVMs or in patients who are poor surgical candidates.
Postcatheterization precautions include hemorrhage, vascular disruption after balloon dilation, pain, nausea, vomiting, and arterial or venous obstruction from thrombosis or spasm.
Figure 1: Central cyanosis Figure 2: Fingers showing clubbing
Yadav, et al.: PAV fistula mimicking as acyanotic heart disease with shunt reversal
Medical Journal of Dr. D.Y. Patil University | July-August 2016 | Vol 9 | Issue 4 543
Possible complications include rupture of blood vessels, tachyarrhythmias, bradyarrhythmias, and vascular occlusion. Pleuritic chest pain is the most common complication and is observed in 12% of patients. The pain usually responds well to analgesics. Radiographic evidence of pulmonary infarction is observed in 3% of patients. Air embolism during embolotherapy is suspected in 4.8% of patients; they developed transient symptoms such as angina, perioral paresthesias, and bradycardia.[14]
Indications for surgery are progressive PAVM enlargement, paradoxical embolization, and symptomatic hypoxemia. The treatment of all PAVMs with feeding vessels of 3 mm or larger is also recommended. Standard thoracic surgical techniques, such as ligation of PAVMs, local excision, segmentectomy, lobectomy or pneumonectomy, have been performed. Recently, video‑assisted thoracoscopic resection of a small PAVM has been performed.[14]
Financial support and sponsorshipNil.
Conflicts of interestThere are no conflicts of interest.
References1. KhurshidI,DownieGH.Pulmonaryarteriovenousmalformation.
PostgradMedJ2002;78:191‑7.2. ChurtonT.Multipleaneurysmsofpulmonaryartery.BrMedJ
1897;1:1223.3. HodgsonCH,KayeRL.Pulmonaryarteriovenousfistulaand
hereditaryhemorrhagictelangiectasia:Areviewandreportof35casesoffistula.DisChest1963;43:449‑55.
4. DinesDE,ArmsRA,Bernatz PE,GomesMR. Pulmonaryarteriovenousfistulas.MayoClinProc1974;49:460‑5.
5. PragerRL,LawsKH,BenderHWJr.Arteriovenousfistulaofthelung.AnnThoracSurg1983;36:231‑9.
6. DinesDE,SewardJB,BernatzPE.Pulmonaryarteriovenousfistulas.MayoClinProc1983;58:176‑81.
7. BosherLHJr,BlakeDA,ByrdBR.Ananalysisofthepathologicanatomyofpulmonaryarteriovenousaneurysmswithparticularreferencetotheapplicabilityoflocalexcision.Surgery1959;45:91‑104.
8. ShumackerHBJr,WaldhausenJA.Pulmonaryarteriovenousfistulasinchildren.AnnSurg1963;158:713‑20.
9. MansourKA,Hatcher CR Jr, LoganWD Jr,Abbott OA.Pulmonaryarteriovenousfistula.AmSurg1971;37:203‑8.
10. VinayN,NaithaniU.Segmentectomyforbilateralpulmonaryarteriovenousfistulawithsignificantrighttoleftshunt–Acasereport.IndianJThoracCardiovascSurg2015;4:311‑3.
11. MarchukDA.Themoleculargeneticsofhereditaryhemorrhagictelangiectasia.Chest1997;1116Suppl:79S‑82S.
12. PorteousME,CurtisA,WilliamsO,MarchukD,BhattacharyaSS,Burn J.Genetic heterogeneity in hereditary haemorrhagictelangiectasia.JMedGenet1994;31:925‑6.
13. SymbasPN,GoldmanM,ErbesfeldMH,VlasisSE.Pulmonaryarteriovenousfistula, pulmonary artery aneurysm, andothervascularchangesofthelungfrompenetratingtrauma.AnnSurg1980;191:336‑40.
14. IshikawaY, Yamanaka K, Nishii T, Fujii K, RinoY,MaeharaT.Video‑assistedthoracoscopicsurgeryforpulmonaryarteriovenousmalformations:Reportoffivecases.GenThoracCardiovascSurg2008;56:187‑90.
Figure 3: Pulmonary angiography showing shunt in the left lower lung
Clinical importance of pulmonary arteriovenous malformations
Commentary
Hereditary hemorrhagic telangiectasia (HHT), also known as Rendu Osler Weber disease, is an inherited multisystem disorder of the vascular system characterized by recurrent epistaxis and mucosal telangiectasias.[1,2] Pulmonary artery malformations (PAVMs) are common findings and observed
in about 20% of patients with HHT.[1] These malformations are direct fistulous connections between the branches of pulmonary artery and vein without an intervening capillary bed. Furthermore, these malformations are known as pulmonary arteriovenous fistulas, pulmonary




















![INSTITUT DE PHYSIQUE DU GLOBE DE PARIS | Terre - Planètes ...jdy/Publis/Dyment_JGR_93.pdf · and Ramprasad [1989, p. 399] considered that "the pos- has strong implications on the](https://img.pdfslide.net/doc/110x75/5f2349df00b3bc6f05632130/institut-de-physique-du-globe-de-paris-terre-plantes-jdypublisdymentjgr93pdf.jpg)