Embed Size (px)
Citation preview

Migraine & types
Migraine and headache same?
• The term migraine is originated from Greek word
“hemicrania” meaning “one side of the head”.
• Migraine headache as an episodic neurovascular
phenomenon is characterized by recurrent attacks
of unilateral headache while headache is
recognized as the most well-known symptom of
migraine
Silberstein, S.D. (2004). Migraine. Lancet, Vol.363, No., pp.381-391
Migraine• Migraine has been regarded as a vascular disorder
because of the throbbing nature of the pain.
• Characterized by pulsating headache, usually restricted
to one side (unilateral), which comes in attacks lasting
4-48 hours
• Mostly associated with nausea, vomiting, sensitivity to
light and sound, vertigo, loose motions and other
symptoms.
Worldwide burden Migraine affects 18% of women and 6% of men in
the United States, and has an estimated worldwide
prevalence of about 10%.
For both men and women, the prevalence of migraine
rises throughout early adult life and falls after midlife.
In girls and women, the rate almost triples between
age 10 and 30 years.
Clin J Pain 2009;25:446–452
Causes• Family history of migraine headaches (70-80%)
• Medications (birth control pills, vasodilators)
• Fatigue or emotional stress
• Specific foods or alcohol & caffeine
• Exertion
• Lack of sleep
• Noise, light, diet
Clin J Pain 2009;25:446–452
Types of migraine
• Common migraine(without aura)
• Classical migraine(with aura)
• Mild (1/month, upto 8 hr)
• Moderate (> 1/ month, intense, 6-24 hr, nausea, vomiting
associated)
• Severe (2-3/month, severe throbbing, 12-48 hr, vertigo,
vomiting associated)
Classical migraine• Migraine with aura (ophthalmic, hemiplegic migraine) is defined
as a recurrent disorder involving headache attacks appearing
gradually over 5-20 minutes and lasting for less than 60 minutes.
• The aura encompasses focal neurological symptoms that precede
or accompany at the onset of migraine attacks.
• Aura can involve reversible visual and sensory symptoms
and speech weakness.
International Classification of Headache Disorders II. (2004). Cephalalgia, Vol.24, Sup.1, pp.1-160
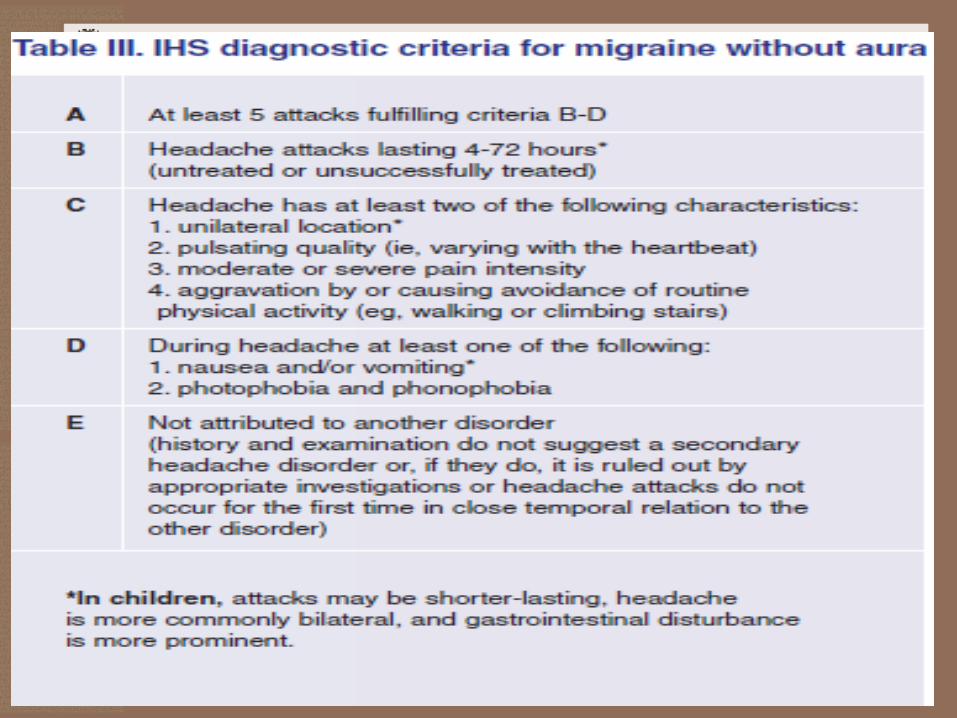
Common migraine• Migraine without aura (hemicrania simplex, common migraine) is a specific
neurological disorder characterized by unilateral, pulsating quality, aggravation
on movement, and moderate to severe headache, nausea and photophobia.
• Most migraineurs suffer from this subtype of migraine, and there are
higher frequency and more severe attacks in comparison with migraine
with aura.
• Owing to strong relationship between migraine without aura with menstrual
cycle, the menstrual migraine (i.e. pure menstrual migraine and menstrually-
related migraine) is categorized in this subtype.International Classification of Headache Disorders II. (2004). Cephalalgia, Vol.24, Sup.1, pp.1-160
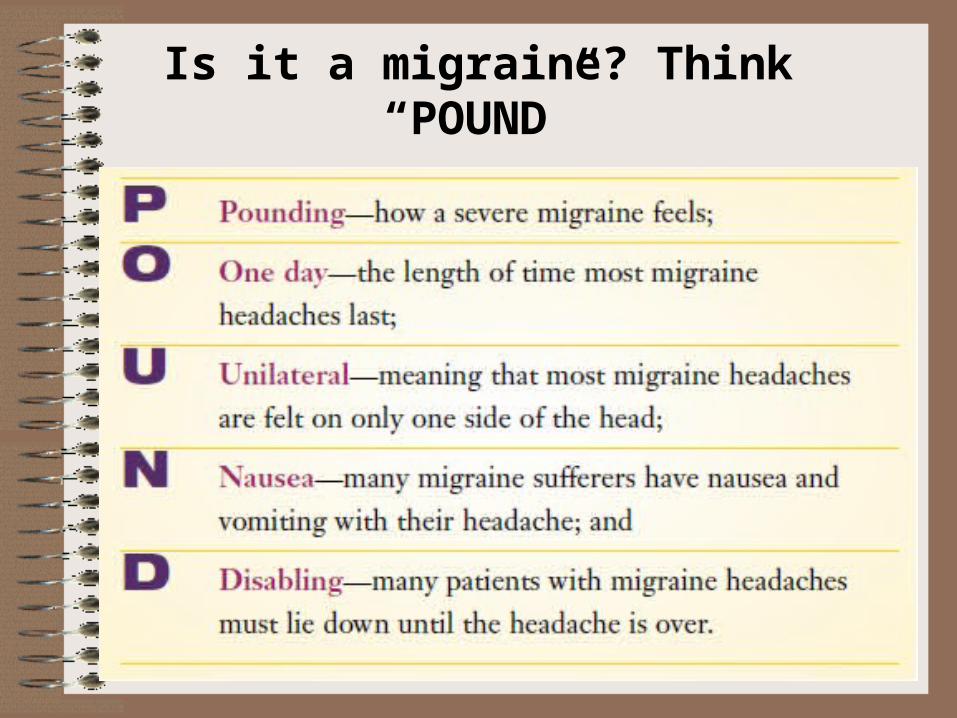
Is it a migraine? Think “POUND”
Pathophysiology • The frequency with which migraine attacks occur may
vary from once in a lifetime to almost daily.
• Attacks are initiated when internal or environmental
triggers are of sufficient intensity to activate a series of
events which culminate in the generation of a migraine
headache.
Pathophysiology• In susceptible individuals, the trigeminovascular
neurons release neurotransmitters, such as calcitonin
generelated peptide(CGRP) and substance P, when
headache triggers are encountered.
• This leads to vasodilation, mast cell degranuation,
increased vascular permeability and meningeal
edema, resulting in neurogenic inflammation.
• Involvement of the neurotransmitter 5-HT
• Dopaminergic stimulationClin J Pain 2009;25:446–452

The role of foods and supplementsin migraine
• Skipped meals and fasting were reported migraine
triggers in over 56% in a population-based study and
40% to 57% in subspeciality clinic-based studies
• The mechanism by which fasting and skipping meals
triggers headaches may be related to alterations in
serotonin and norepinephrine in brainstem
pathways or the release of stress hormones such as
cortisol.
Clin J Pain 2009;25:446–452
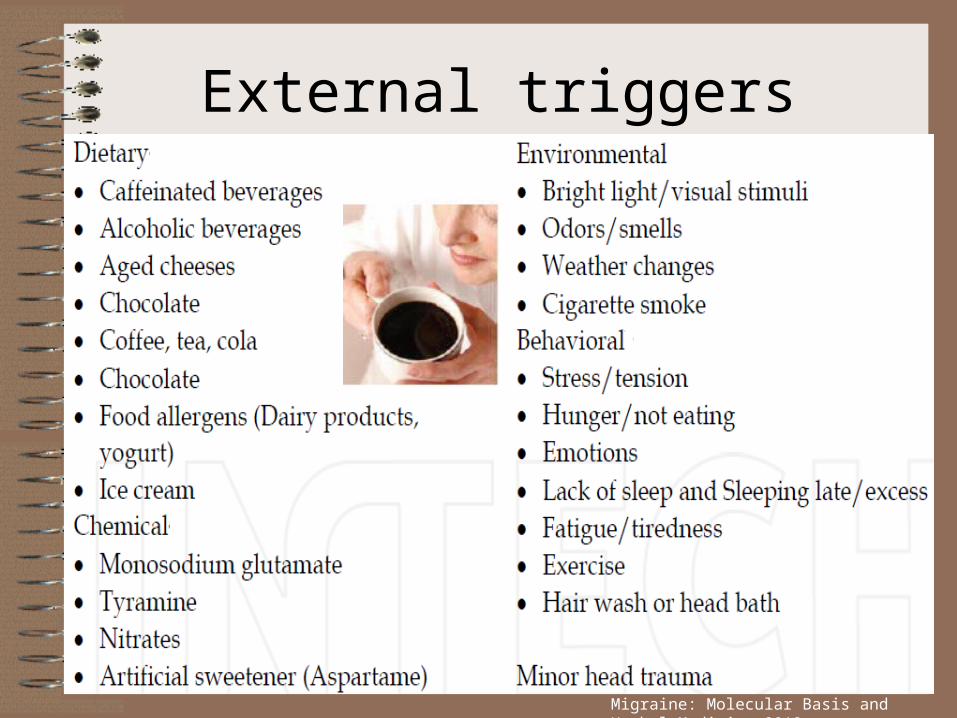
External triggers
Migraine: Molecular Basis and Herbal Medicine 2012

Internal triggers• The most common internal triggers are sex hormones
(neurosteroids and ovarian steroids).
• The key stages of reproduction including first
menstruation, pregnancy and menopause are
associated with frequency or severity of migraine.
• Interestingly only attacks of migraine without aura occur
during the perimenstrual time period and attacks of
migraine with aura happen equally during the menstrual
cycle. Migraine: Molecular Basis and Herbal Medicine 2012
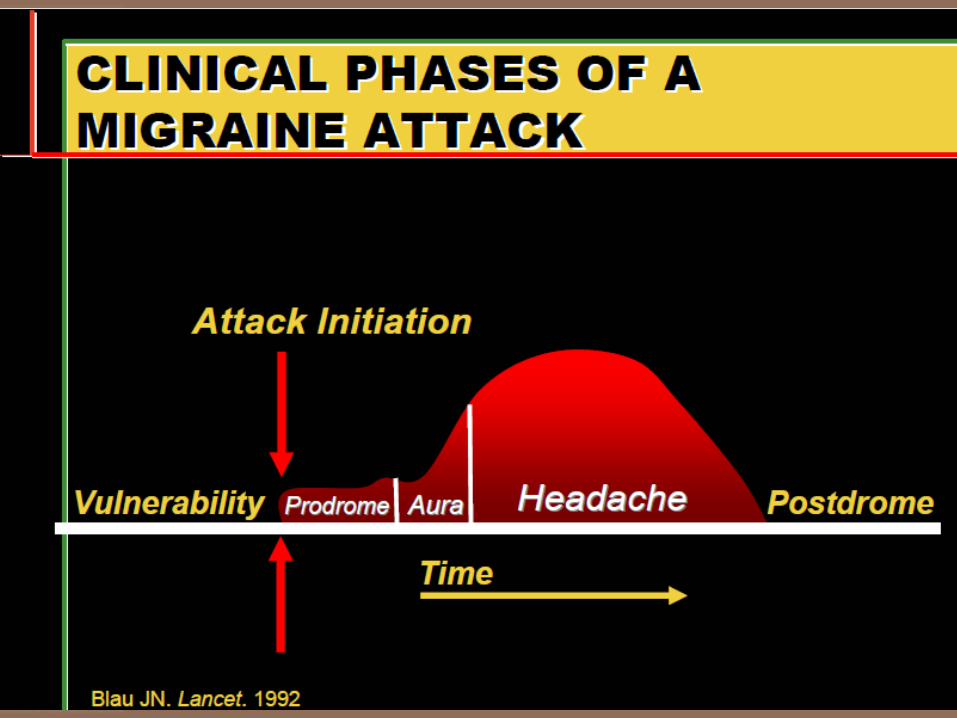

Prodrome & aura phase• Many migraineurs experience vague vegetative or affective
symptoms as much as 24 hours prior to the onset of a
migraine attack. This phase is called the prodrome
• The aura phase consists of focal neurological symptoms
that persist up to one hour.
• Symptoms may include visual, sensory, or language
disturbance as well as symptoms localizing to the
brainstem.
Typical headache & resolution phase
• Within an hour of resolution of the aura symptoms, the
typical migraine headache usually appears with its
unilateral throbbing pain and associated nausea,
vomiting, photophobia, or phonophobia.
• Without treatment, the headache may persist for up to
72 hours before ending in a resolution phase often
characterized by deep sleep.
Management of migraineThe management of migraine begins with an explanation of certain things to the
patient:
• Migraine is an inherited tendency to cerebral dysfunction, and cannot be cured
• Migraine can be modified and controlled by lifestyle adjustment and the use of
medicines
• Migraine is neither life threatening nor associated with serious illness. however
migraine can and often does make life a misery
• Migraine management takes time and co-operation when information, such as
that from a headache diary, has to be collected.
Intern Med J 2003; 33: 436–442
Medications• Abortive Medications
– Analgesics with caffeine (PCM,acetaminophen, aspirin
and caffeine).
– Analgesics with caffeine and barbiturates
– Non steroidal antiinflammatory drugs (NSAIDs) such
as ibuprofen,naproxen sodium.
– Triptans (suma,riza,nara,algo,zolmi-5HT1B/1D agonist)
– Antiemetics (domperidone)
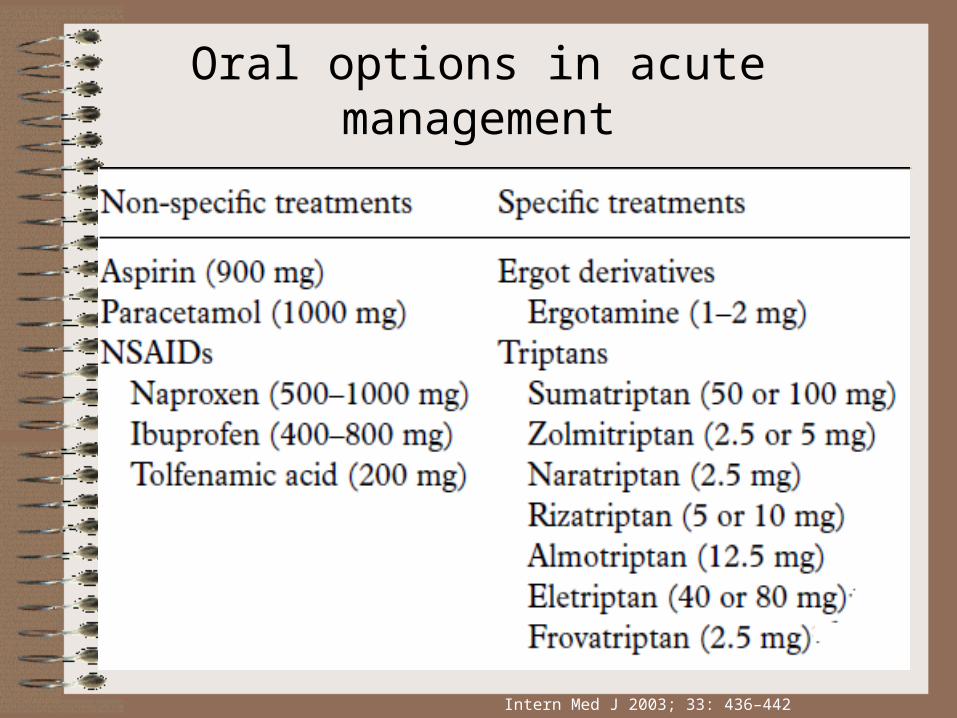
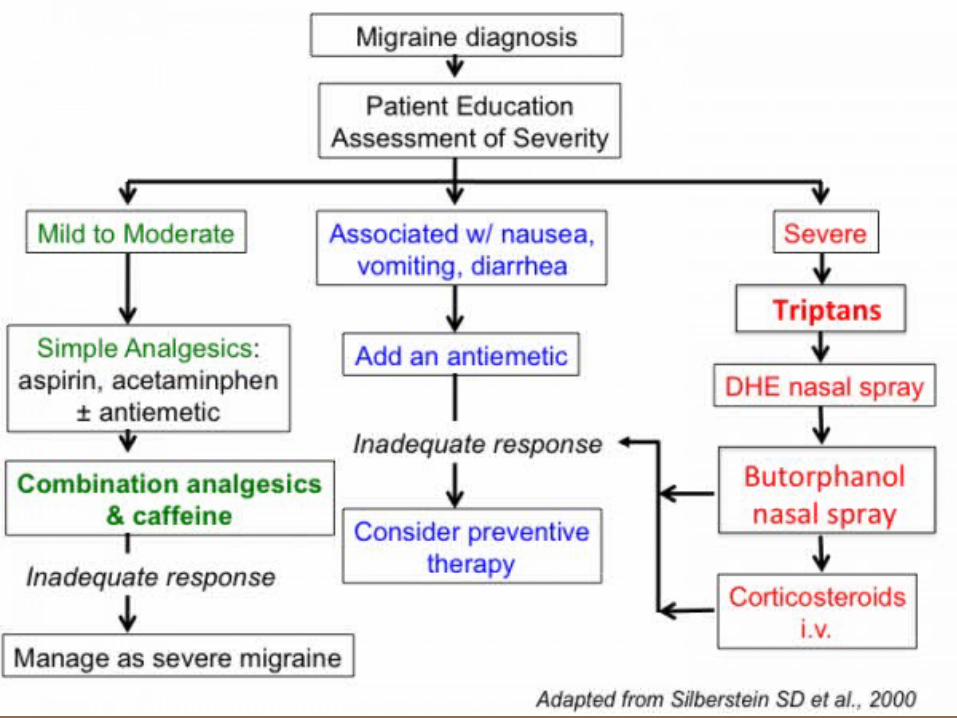
Oral options in acute management
Intern Med J 2003; 33: 436–442

Comparison of available triptans
Annals of Indian Academy of Neurology, August 2012, Vol 15, Supplement 1
Medications• Preventive Medications
– Beta blockers (propranolol, timolol maleate, and
metoprolol. )
– Calcium-channel blockers (diltiazem, nifedipine).
– Antidepressants (fluoxetine, paroxetine,sertraline).
– Anticonvulsants (valproic acid or divalproex sodium).
– NSAIDs (ketoprofen, naproxen sodium).

Preventative therapy for migraine
Annals of Indian Academy of Neurology, August 2012, Vol 15, Supplement 1

General Principles of Preventive Treatment
• Start with a low dose and increase slowly
• Use an adequate trial of 2 to 3 months
• Avoid medication interactions/contraindications
• Monitor with calendar or diary
• Monitor for medication overuse
• Consider comorbid conditions
• Consider preventive medication combinations in refractory
patients
• Taper when headaches are controlledContinuum Lifelong Learning Neurol 2012;18(4):764–782.

THANK YOU