Embed Size (px)
Citation preview
MUSCULOSKELET
AL TRAUMA
OVERVIEW
Fractures
Dislocations
Soft tissue injury
FRACTURES
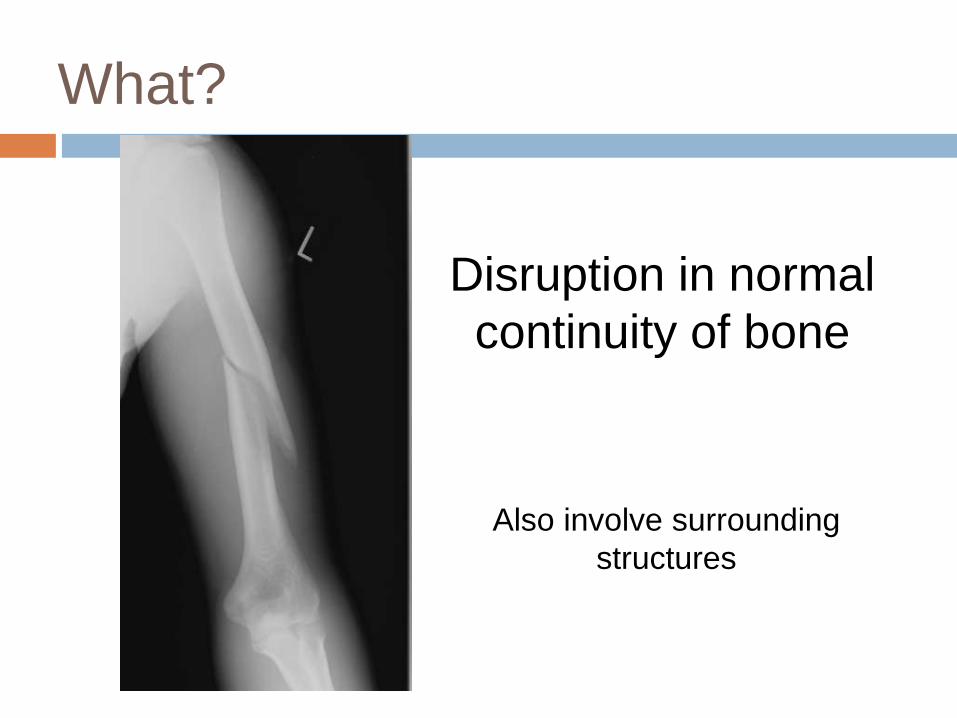
What?
Disruption in normal
continuity of bone
Also involve surrounding
structures
Pathophysiology
d/t mechanical overload
More stress than bone can absorb
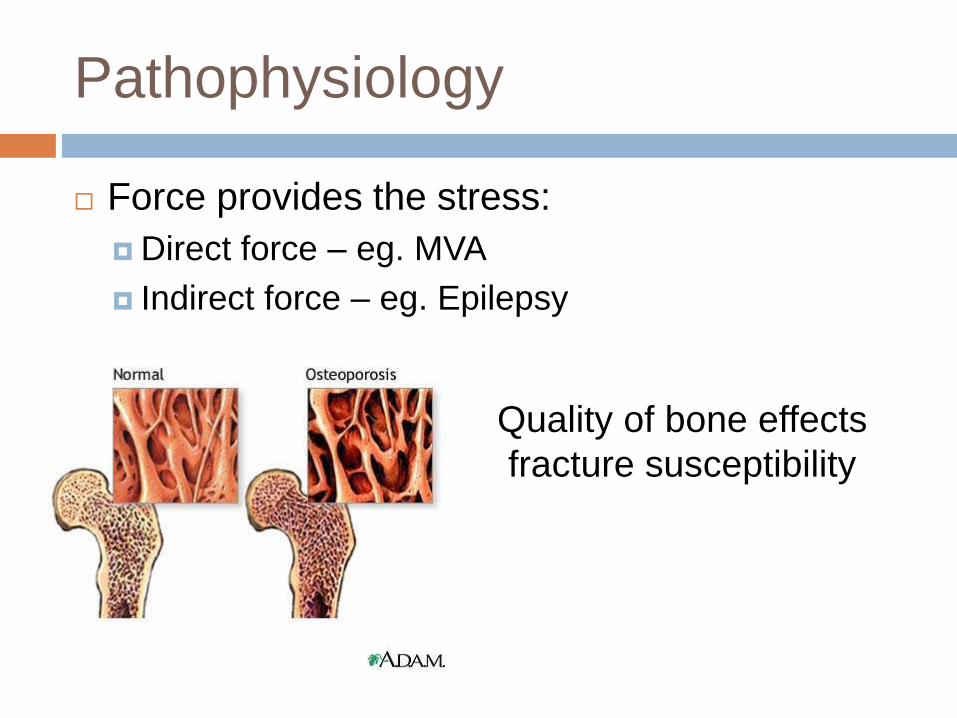
Pathophysiology
Force provides the stress:
Direct force – eg. MVA
Indirect force – eg. Epilepsy
Quality of bone effects
fracture susceptibility
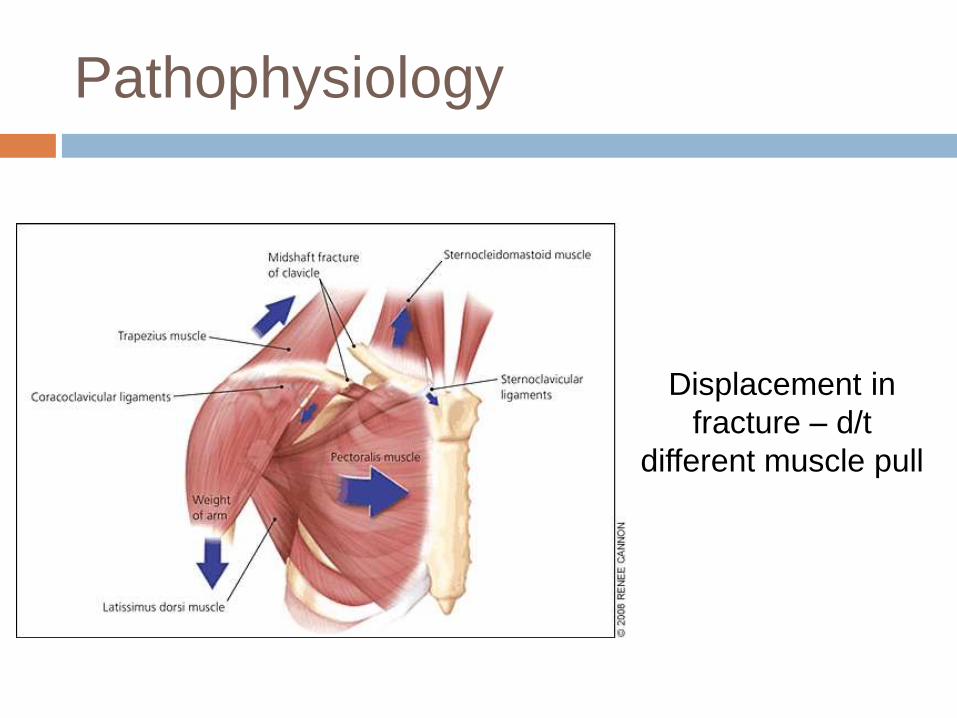
Pathophysiology
Displacement in
fracture – d/t
different muscle pull
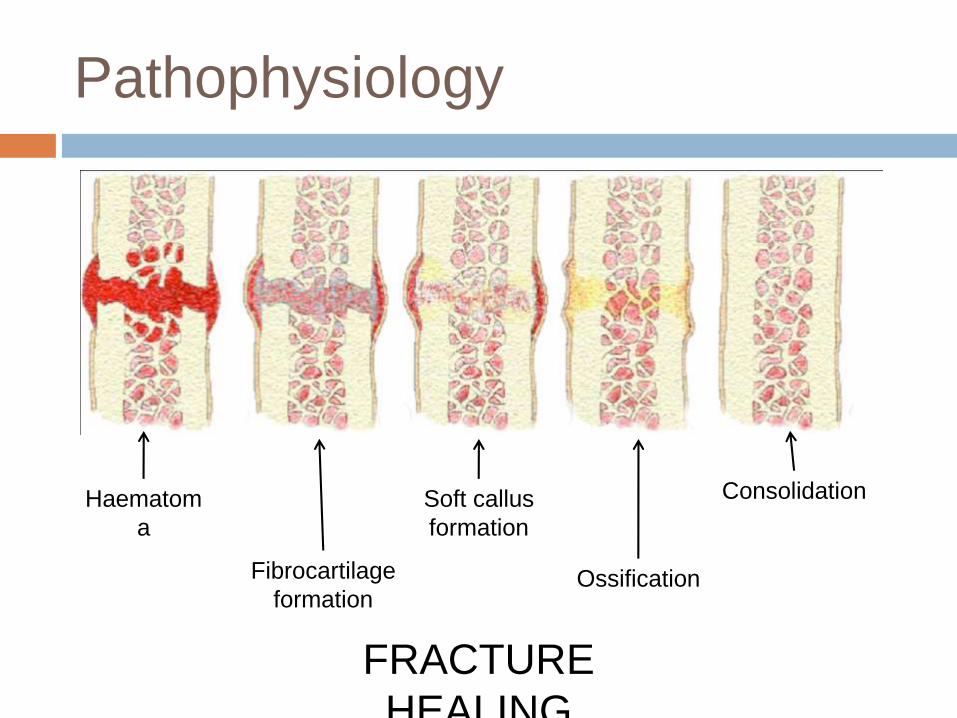
Pathophysiology
Haematom
a
Fibrocartilage
formation
Soft callus
formation
Ossification
Consolidation
FRACTURE
HEALING
Manifestations, assessment &
diagnosis
History :
usually trauma
- MVA
- fall

Manifestations, assessment &
diagnosis
Physical
examination:
• tenderness
• swelling
• deformity
• shock
• neurovascular
involvement
Manifestations, assessment &
diagnosis
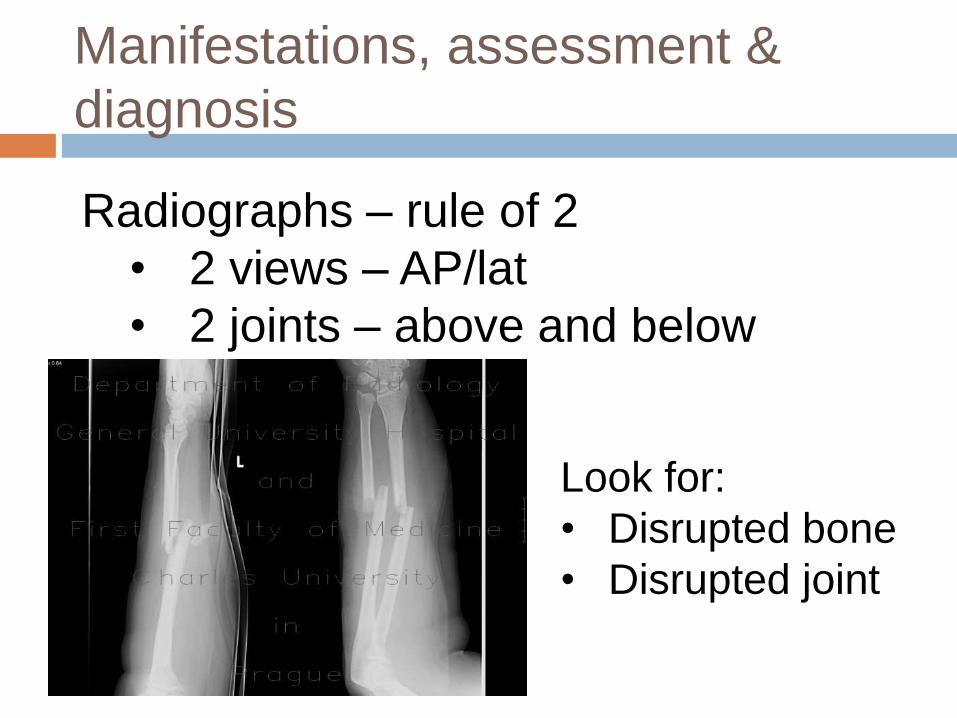
Radiographs – rule of 2
• 2 views – AP/lat
• 2 joints – above and below
Look for:
• Disrupted bone
• Disrupted joint
Manifestations, assessment &
diagnosis
Diagnosis is obvious esp. with h/o MVA or fall
Fracture classification extensive:
e.g: Open fracture (Gustilo))Grade I – wound <1cm, minimal
contamination
Grade II – wound >1cm, moderate contmination
Grade III – wound >1cm with extensive soft tissue damage and high degree contamination
Clinical management
Thorough initial management
Reduction and stabilization of fracture
Monitoring of complications
Remobilization and rehabilitation
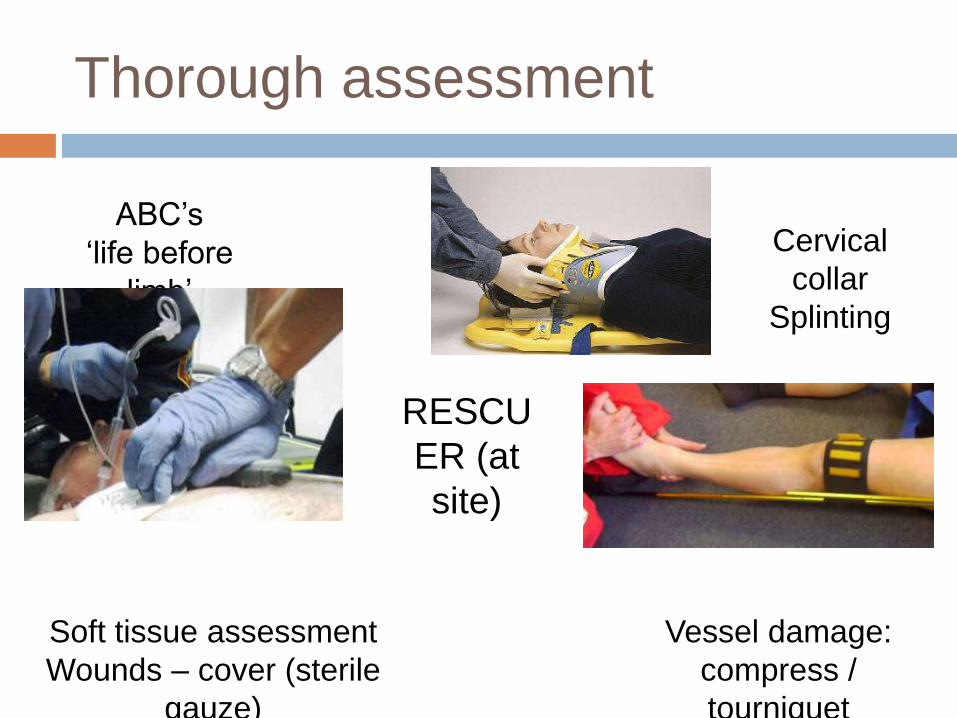
Thorough assessment
RESCU
ER (at
site)
ABC’s
‘life before
limb’
Cervical
collar
Splinting
Soft tissue assessment
Wounds – cover (sterile
gauze)
Vessel damage:
compress /
tourniquet
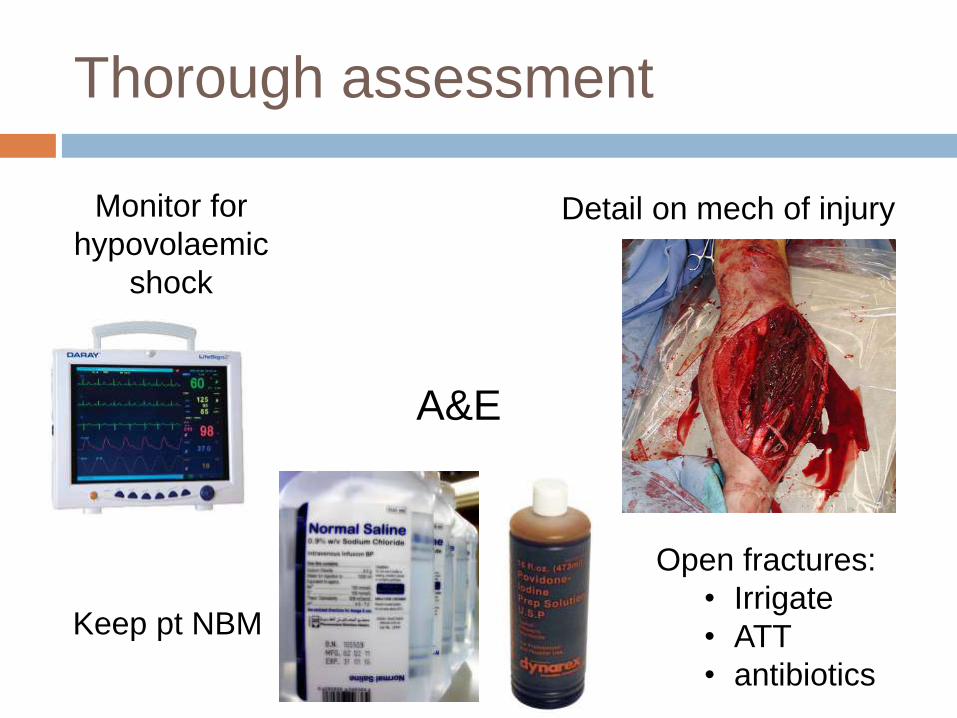
Thorough assessment
A&E
Monitor for
hypovolaemic
shock
Detail on mech of injury
Open fractures:
• Irrigate
• ATT
• antibiotics
Keep pt NBM
Reduction & stabilization
AIM:
Restore alignment
Restore position
Restore length
HOW?
Closed manipulative reduction (CMR)
Open reduction and internal fixation (ORIF)
External fixation (ext-fix)
Traction
Reduction & stabilization - CMR
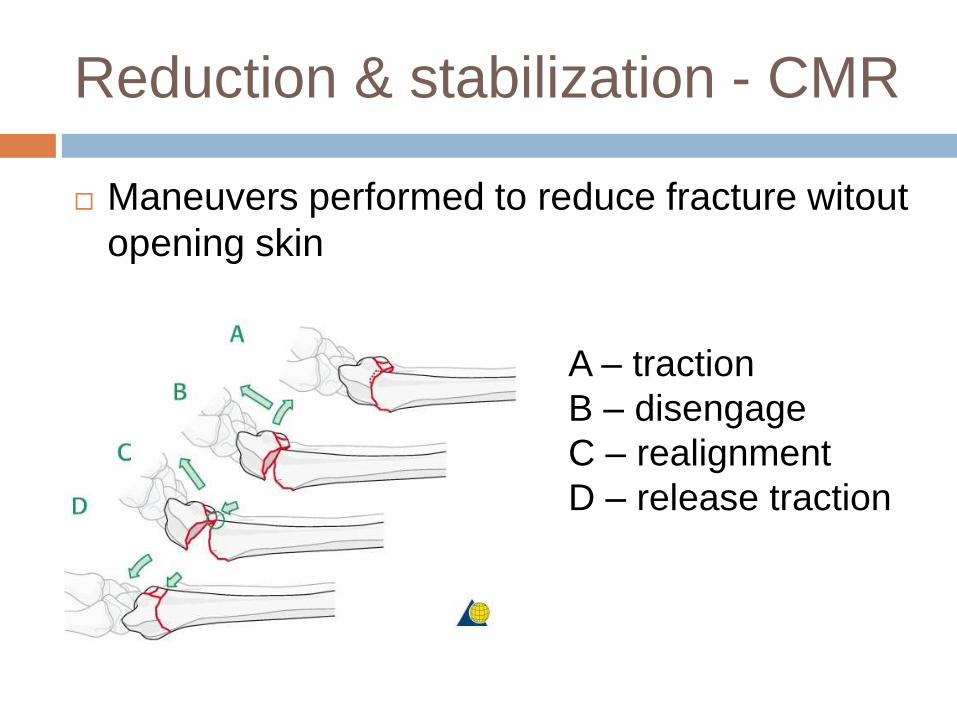
Maneuvers performed to reduce fracture witout
opening skin
A – traction
B – disengage
C – realignment
D – release traction

Reduction & stabilization - CMR
Reduction held with cast
Plaster of Paris (POP) Fibreglass cast
Reduction & stabilization - ORIF
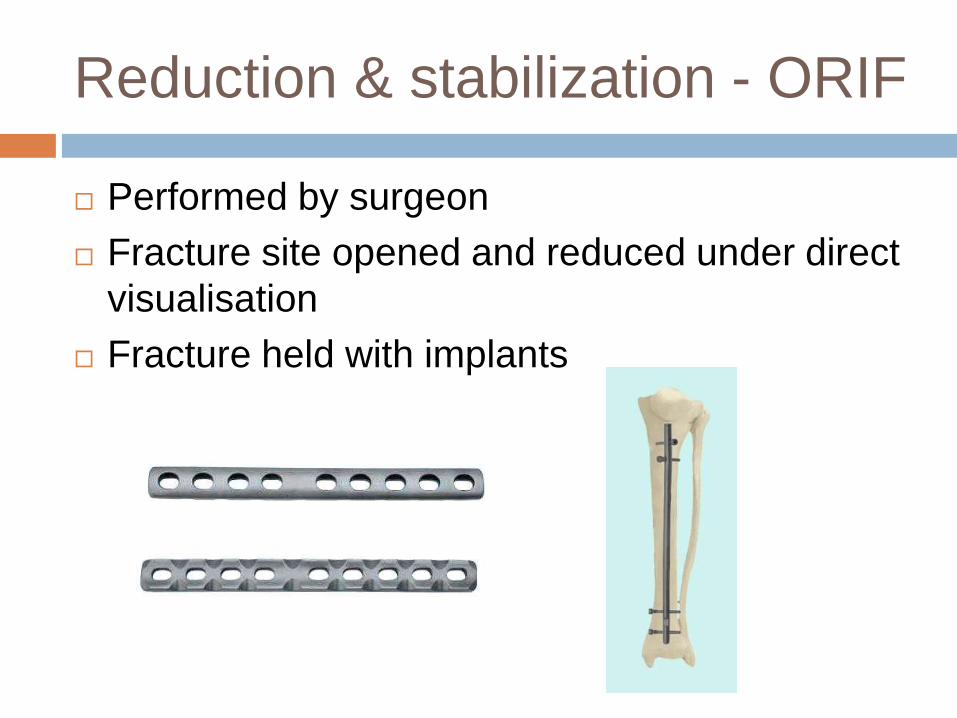
Performed by surgeon
Fracture site opened and reduced under direct
visualisation
Fracture held with implants
Reduction & stabilization – ext-
fix
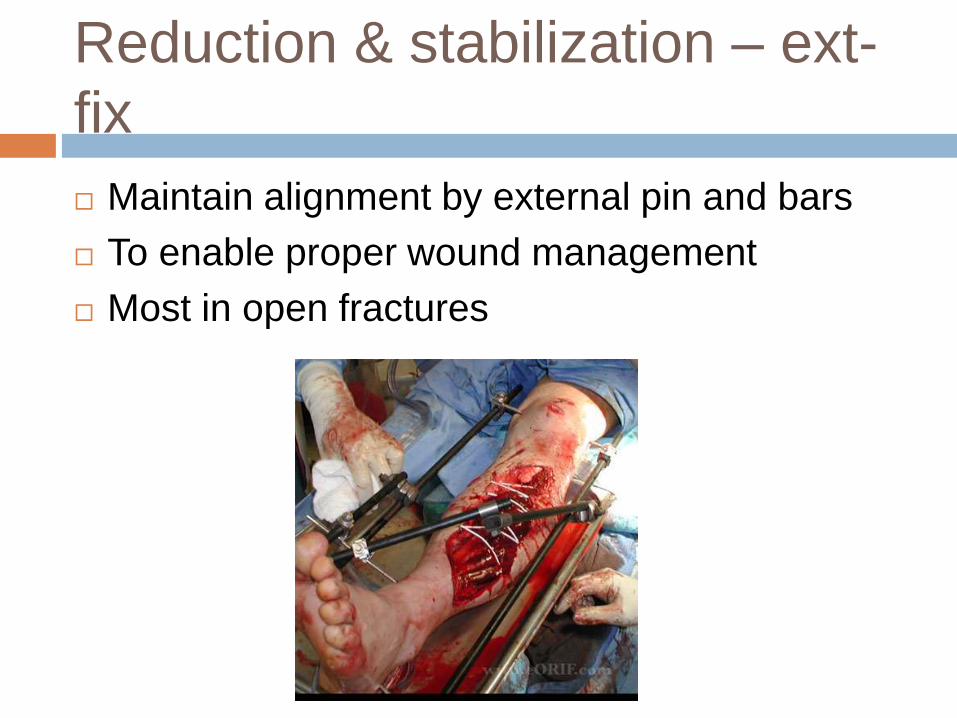
Maintain alignment by external pin and bars
To enable proper wound management
Most in open fractures
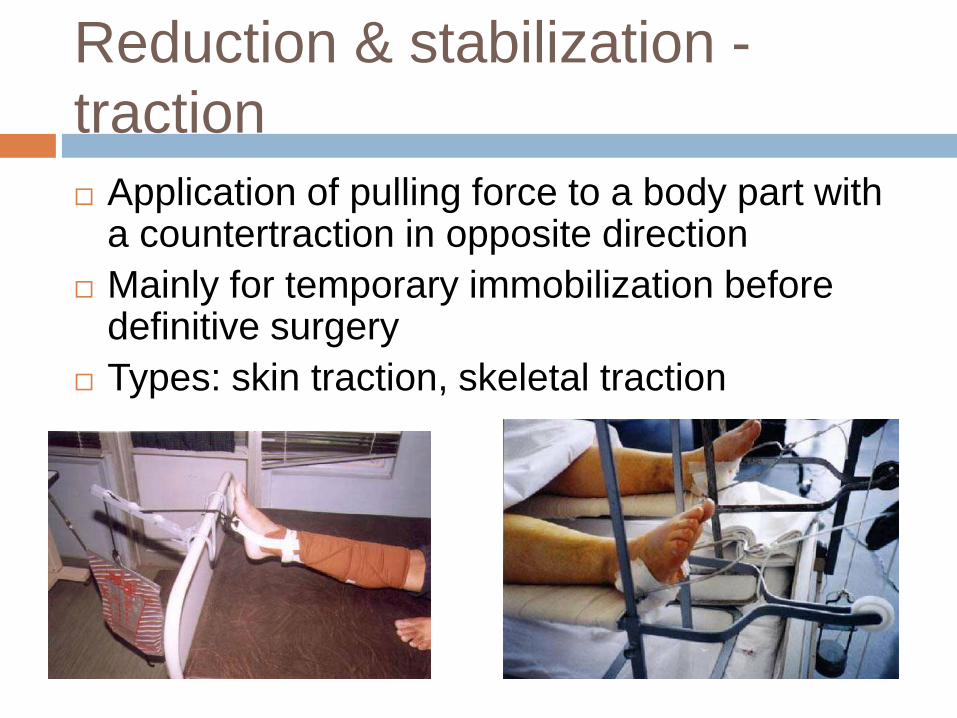
Reduction & stabilization -
traction
Application of pulling force to a body part with a countertraction in opposite direction
Mainly for temporary immobilization before definitive surgery
Types: skin traction, skeletal traction
to look out for….
Complications
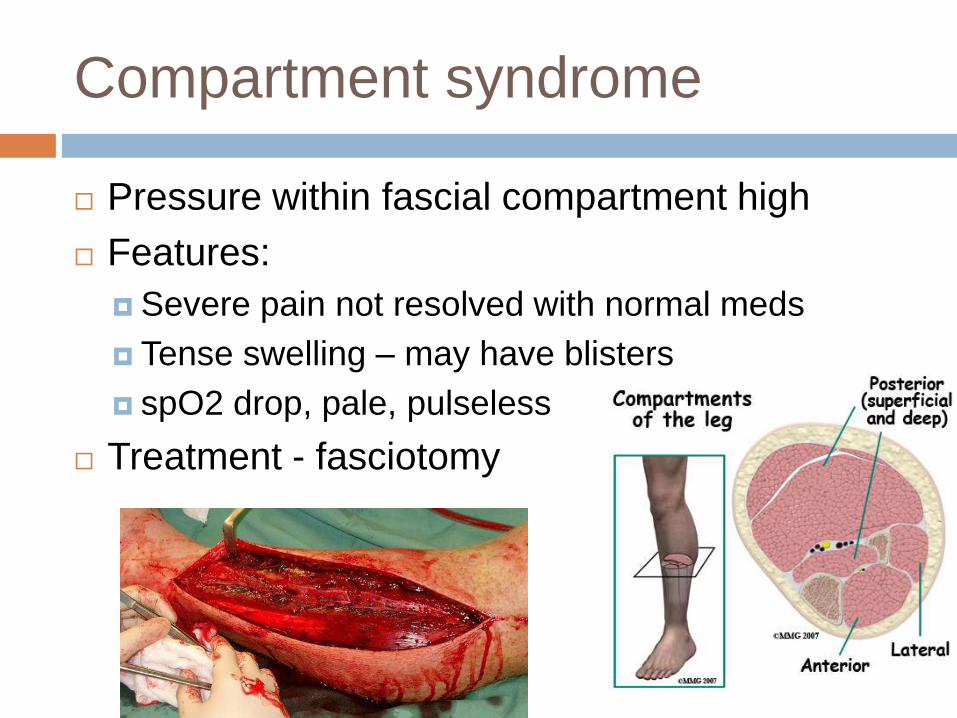
Compartment syndrome
Pressure within fascial compartment high
Features:
Severe pain not resolved with normal meds
Tense swelling – may have blisters
spO2 drop, pale, pulseless
Treatment - fasciotomy
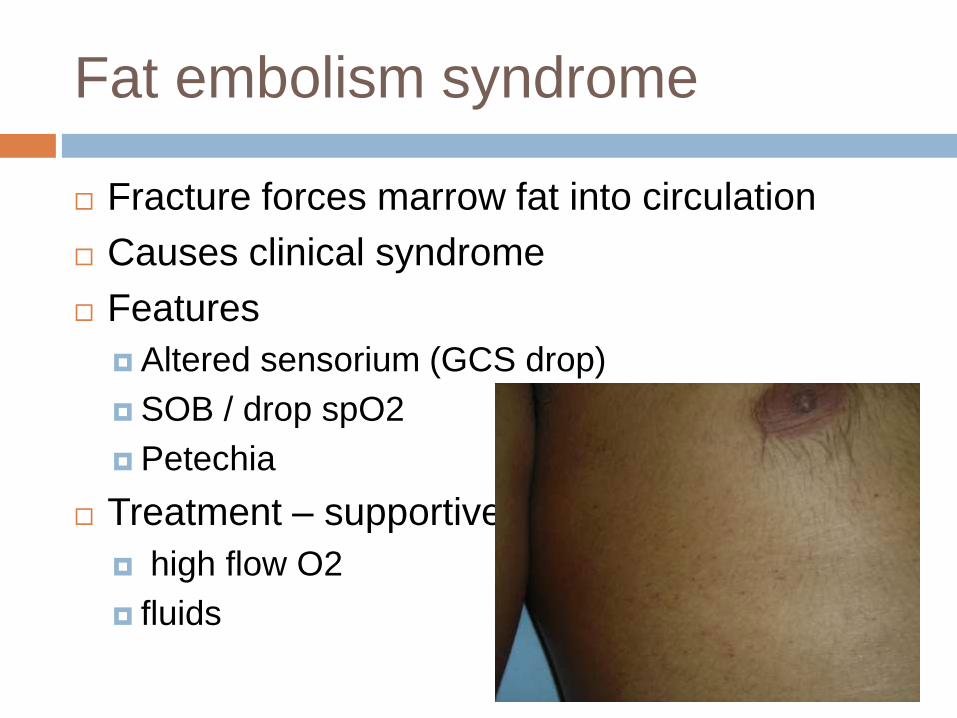
Fat embolism syndrome
Fracture forces marrow fat into circulation
Causes clinical syndrome
Features
Altered sensorium (GCS drop)
SOB / drop spO2
Petechia
Treatment – supportive
high flow O2
fluids
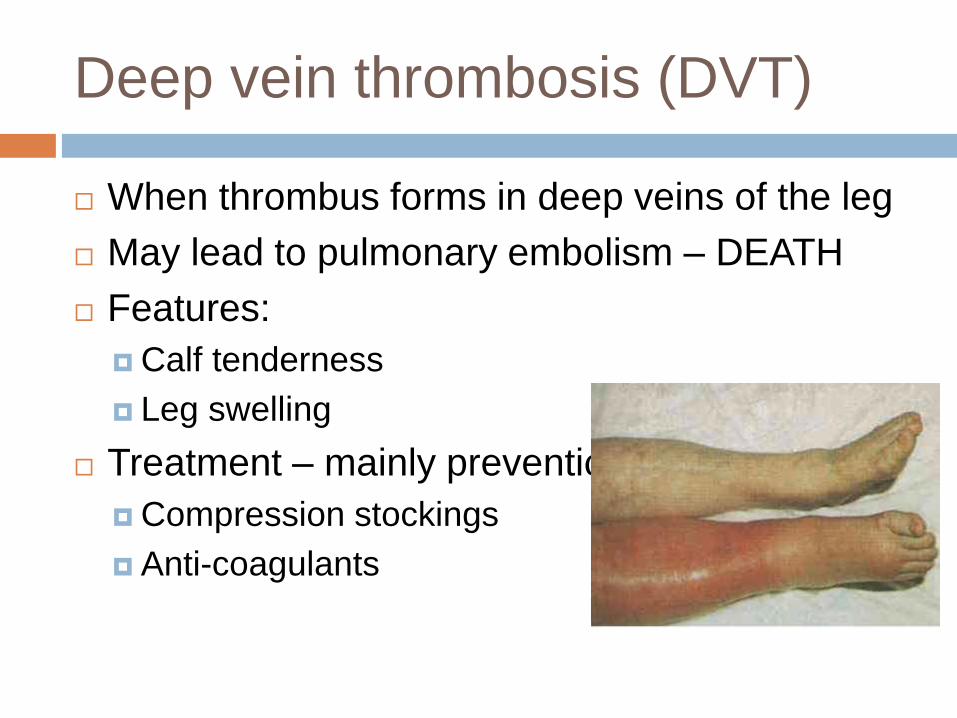
Deep vein thrombosis (DVT)
When thrombus forms in deep veins of the leg
May lead to pulmonary embolism – DEATH
Features:
Calf tenderness
Leg swelling
Treatment – mainly prevention
Compression stockings
Anti-coagulants
DISLOCATIONS
Pathophysiology
Occurs when the normal joint articulation is
disrupted
Usually due to trauma / sports injury
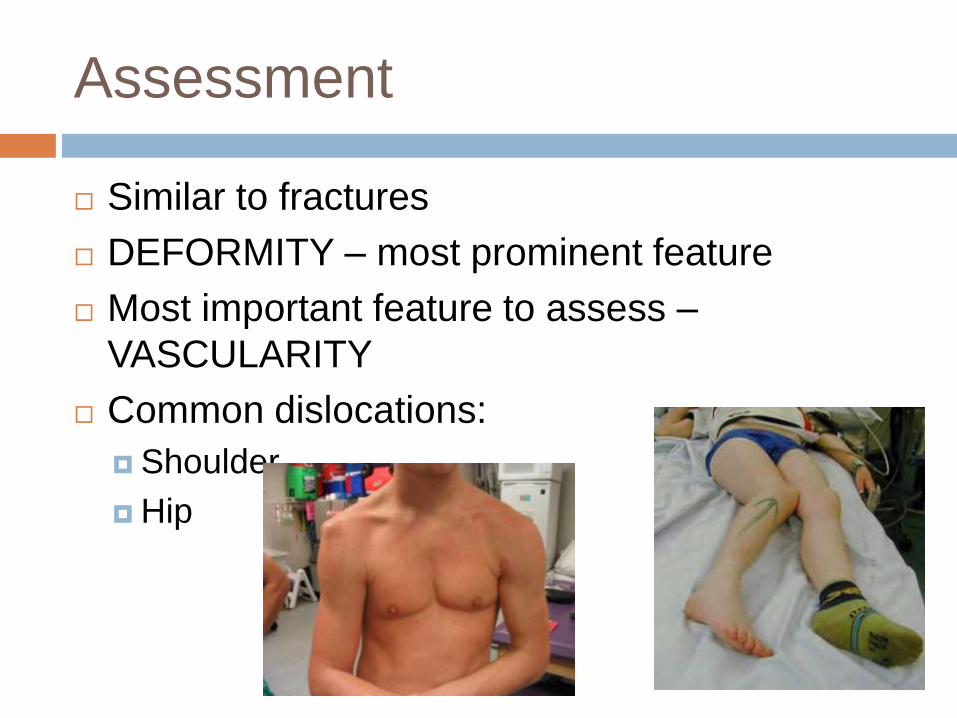
Assessment
Similar to fractures
DEFORMITY – most prominent feature
Most important feature to assess –
VASCULARITY
Common dislocations:
Shoulder
Hip
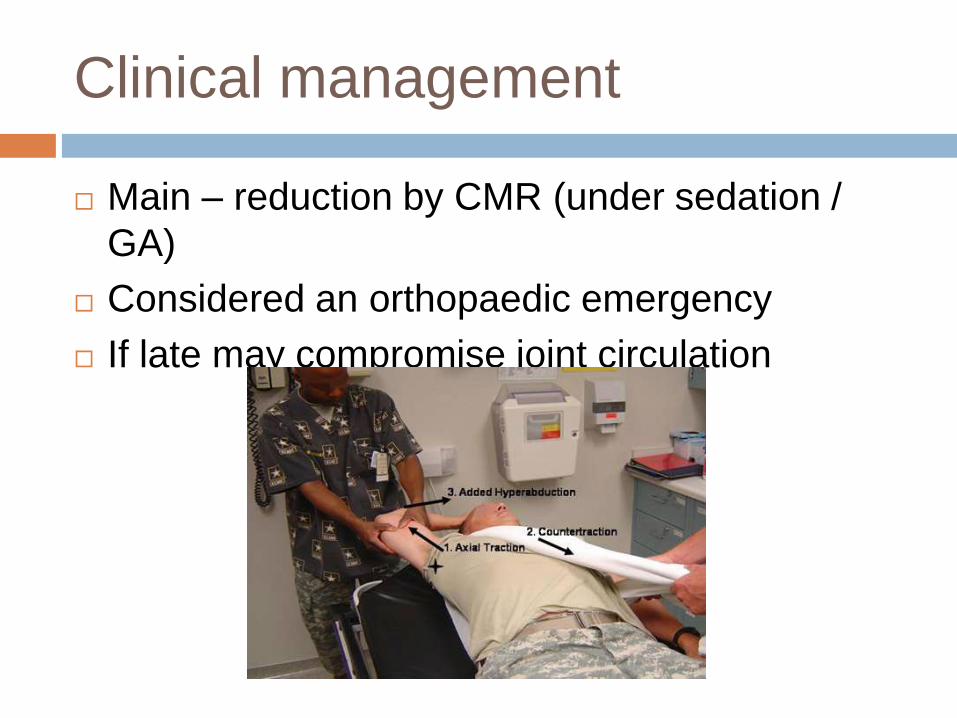
Clinical management
Main – reduction by CMR (under sedation /
GA)
Considered an orthopaedic emergency
If late may compromise joint circulation
SOFT TISSUE INJURIES
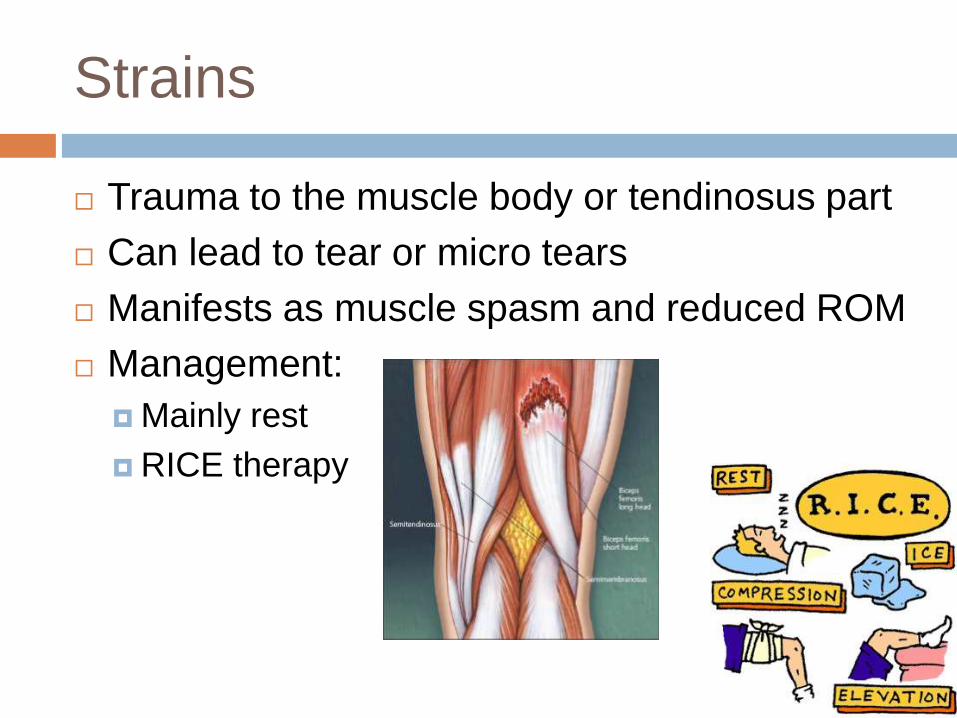
Strains
Trauma to the muscle body or tendinosus part
Can lead to tear or micro tears
Manifests as muscle spasm and reduced ROM
Management:
Mainly rest
RICE therapy
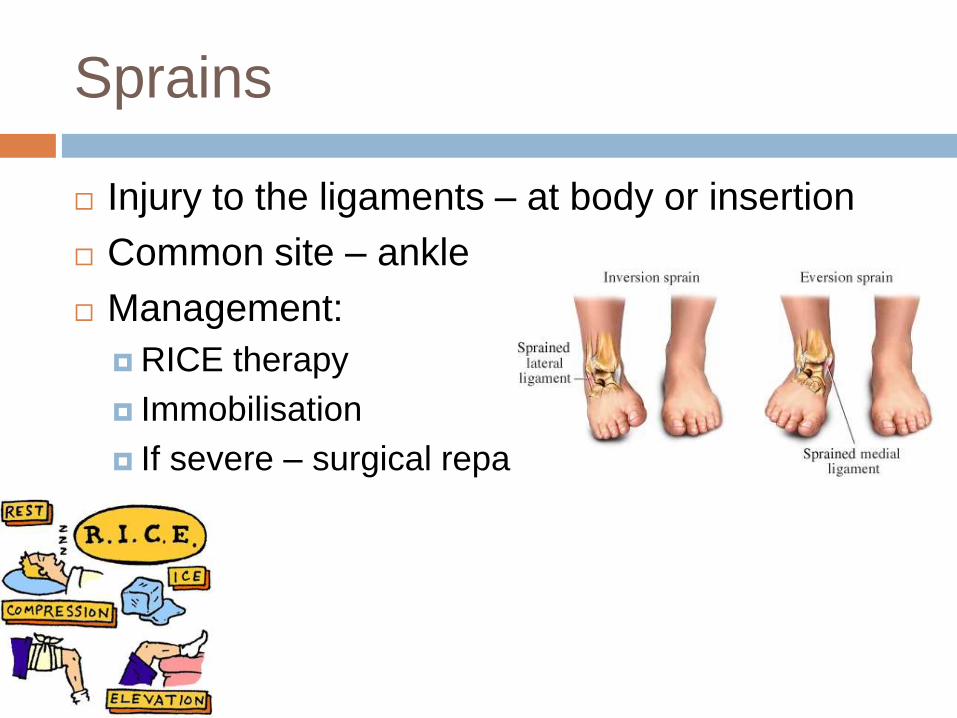
Sprains
Injury to the ligaments – at body or insertion
Common site – ankle
Management:
RICE therapy
Immobilisation
If severe – surgical repair

Questions?
THANK YOU…