Embed Size (px)
DESCRIPTION
Overview presented to group of undergraduate and postgraduate students from UPM on 9 December 2013 in Putrajaya
Citation preview

NCDs in Malaysia:
Issues & Challenges
Feisul Idzwan Mustapha MBBS, MPH, AM(M)Public Health Specialist
Disease Control DivisionMinistry of Health, Malaysia
9 December 2013
Ministry of Health Malaysia

2
Non-Communicable Diseases Section• Headed by a Deputy Director• Consists of three main sectors:
• NCD-Cancer-FCTC• Occupational & Environmental Health• Mental health, Substance Abuse, Violence and Injury Program
(MESVIP)
• Two main functions:• Policy and Program Development for the prevention and control
of NCD in Malaysia• Monitoring and Evaluation

There are Four Major Groups of Non-Communicable Diseases;Four major lifestyles related risk factors
Modifiable causative risk factors
Tobacco use Unhealthy diets
Physical inactivity
Harmful use of alcohol
Noncommunicable diseases
Heart disease and stroke
Diabetes
Cancers
Chronic lung disease
3

NHMS II (1996) NHMS III (2006)
NHMS 20110
5
10
15
20
25
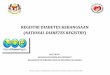
8.3
14.9
20.8
6.5
9.510.7
1.8
5.4
10.1
4.3 4.7 5.3
Prevalence of Diabetes, ≥30 years (1996, 2006 & 2011)
Total diabetesKnownUndiagnosedIFG
Prev
alen
ce (%
)
Source: National Health & Morbidity Surveys (NHMS)
NHMS III (2006) NHMS 20110
5
10
15
20
25
30
35 32.2 32.7
12.8
19.8
Prevalence of Hypertension, ≥18 years (2006 & 2011)
Total HPTKnownUndiagnosed
Prev
alen
ce (%
)
NHMS III (2006) NHMS 20110
5
10
15
20
25
30
35
40
20.6
35.1
8.4
26.6
Prevalence of Hypercholesterolaemia, ≥18 years (2006 & 2011)
Total HCholKnownUndiagnosed
Prev
alen
ce (%
)
4

NHMS II (1996)
NHMS III (2006)
NHMS 20110
5
10
15
20
25
30
35
16.6
29.1 29.4
4.4
14 15.1
Prevalence of Overweight & Obesity, ≥18 years (1996, 2006 & 2011)
OverweightObesity
Prev
alen
ce (%
)
Prevalence of Abdominal Obesity, ≥18 years (2006 & 2011)
18-19 20-24 25-29 30-34 35-39 40-44 45-49 50-54 55-59 60-64 65-69 70-74 75+10
20
30
40
50
60
70
19.6
28.633.6
44.748.0
51.055.7
62.8 63.2 61.4 63.2
56.2
50.4
AGE GROUPS (years)
PREV
ALEN
CE (%
)
NHMS 2006 NHMS 201120
30
40
50
60
30.1
37.1
47.1
54.1
MALES FEMALES
PREV
ALE
NCE
(%)
Prevalence of Abdominal Obesity by age groups (NHMS 2011)
5

Overweight in adults, ASEAN Region, 2010
6Viet
Nam
Cambodia La
o
Myanmar
Indonesia
Philippines
Thail
and
Singa
pore
Malaysi
aJap
an0.0
5.0
10.0
15.0
20.0
25.0
30.0
35.0
40.0
45.0
50.0
MaleFemale
Prev
alen
ce %

Obesity in adults, ASEAN Region, 2010
7Viet
Nam
Cambodia La
o
Myanmar
Indonesia
Philippines
Thail
and
Singa
pore
Malaysi
aJap
an0.0
2.0
4.0
6.0
8.0
10.0
12.0
14.0
16.0
18.0
MaleFemale
Prev
alen
ce %

8
Cambodia
Myanmar
Philippines
Indonesia
Thail
and
Singa
pore
Viet N
am
Malaysi
aJap
an0.0
2.0
4.0
6.0
8.0
10.0
12.0
MaleFemale
Prev
alen
ce %
High Blood Sugars in Adults, ASEAN Region, 2010

Burden of Diabetes in Malaysia: Trends & Projections by 2020 (Adults age 18 years and above)
2006 2007 2008 2009 2010 2011 2012 2013 2014 2015 2016 2017 2018 2019 20200
5
10
15
20
25
0
500,000
1,000,000
1,500,000
2,000,000
2,500,000
3,000,000
3,500,000
4,000,000
4,500,000
5,000,000
Est. population, 2006 Est. population, 2011Prevalence projection, 2006 Prevalence projection, 2011
Year
Prev
alen
ce (%
)
Estim
ated
pop
ulati
on
Current projection
9

UN Secretary-General:NCDs in developing countries are hidden, misunderstood and under-recorded
A rapidly rising epidemic in developed and developing countries…
… with serious socio-economic impacts, particularly in developing countries.
Workable solutions exist to prevent most premature deaths from NCDs and mitigate the negative impact on development.
The way forward: These solutions need to be mainstreamed into socio-economic development programmes and poverty alleviation strategies. 10

11

65th World Health Assembly (May 2012):Decided to adopt a global target of a 25% reduction in premature mortality from NCD by 2025.
66th World Health Assembly (May 2013):Adoption of the Global Action plan for the Prevention and Control of NCDs (2013-2020), including 25 NCD indicators with 9 voluntary global targets.
12

Global Monitoring Framework for NCDsIndicator Targets
1. Premature mortality from NCD 25% relative reduction in risk of dying
2. Harmful use of alcohol 10% relative reduction
3. Physical inactivity 10% relative reduction
4. Salt intake 30% relative reduction in mean population intake
5. Tobacco use 30% relative reduction
6. Hypertension Contain the prevalence
7. Diabetes & obesity Contain the prevalence
8. Drug therapy to prevent heart attacks & strokes
At least 50% of eligible people receive therapy
9. Essential NCD medicines & basic technologies to treat major NCDs
Availability & affordability
Note: Targets for year 2025, against baseline of year 2010. Reporting to the United Nations every five years (next will be in 2015)
13

Overarching principles & approaches in the GAP for NCD
14

National Strategic Plan for Non-Communicable Diseases (NSP-NCD) 2010-2014
• Presented and approved by the Cabinet on 17 December 2010
• Provides the framework for strengthening NCD prevention & control program in Malaysia
• Adopts the “whole-of-government” and “whole-of-society approach”
Seven Strategies:1. Prevention and Promotion
2. Clinical Management
3. Increasing Patient
Compliance
4. Action with NGOs,
Professional Bodies & Other
Stakeholders
5. Monitoring, Research and
Surveillance
6. Capacity Building
7. Policy and Regulatory
interventions
15

Multi-Sectoral Approach: What & Why?• Working together across sectors to improve health and
influence its determinant• Forging new collaborations and partnerships are critical in
making progress in addressing the NCD epidemic.• Partnership occurs at different levels:
• Individuals, families and communities.• Government, communities and NGOs.• Government, development partners (within countries), civil
society and, as appropriate, the private sector.
16

‘Whole-of-Government’ and ‘Whole- of-Society’ approach • ‘Whole-of-Government’ denotes
public service agencies working across portfolio boundaries to achieve a shared goal and an integrated government response to particular issues.
• Responsibility for health and its social determinants rests with the whole society, and health is produced in new ways between society and government.
17

Social Determinants of Health
18

Cost effective interventions to address NCDs
19
Population-based interventions addressing NCD risk factors
Tobacco use
- Excise tax increases - Smoke-free indoor workplaces and public places- Health information and warnings about tobacco - Bans on advertising and promotion
Harmful use of alcohol
- Excise tax increases on alcoholic beverages - Comprehensive restrictions and bans on alcohol
marketing- Restrictions on the availability of retailed alcohol
Unhealthy diet and physical inactivity
- Salt reduction through mass media campaigns and reduced salt content in processed foods
- Replacement of trans-fats with polyunsaturated fats- Public awareness programme about diet and physical
activity
Individual-based interventionsaddressing NCDs in primary care
Cancer - Prevention of liver cancer through hepatitis B immunization
- Prevention of cervical cancer through screening (visual inspection with acetic acid [VIA]) and treatment of pre-cancerous lesions
CVD and diabetes
- Multi-drug therapy (including glycaemic control for diabetes mellitus) for individuals who have had a heart attack or stroke, and to persons at high risk (> 30%) of a cardiovascular event within 10 years
- Providing aspirin to people having an acute heart attack

Tobacco useTobacco use
Harmful use of alcohol
Harmful use of alcohol
• Excise tax increases • Smoke-free indoor workplaces and public places• Health warnings • Bans on advertising and promotion
• Excise tax increases • Smoke-free indoor workplaces and public places• Health warnings • Bans on advertising and promotion
• Excise tax increases on alcoholic beverages • Comprehensive restrictions and bans on alcohol
marketing• Restrictions on the availability of retailed alcohol
• Excise tax increases on alcoholic beverages • Comprehensive restrictions and bans on alcohol
marketing• Restrictions on the availability of retailed alcohol
• Salt reduction through mass media campaigns and reduced salt content in processed foods
• Replacement of trans-fats with polyunsaturated fats
• Public awareness programme about diet and physical activity
• Salt reduction through mass media campaigns and reduced salt content in processed foods
• Replacement of trans-fats with polyunsaturated fats
• Public awareness programme about diet and physical activity
“Healthy” Settings such as Cities, Towns, Schools, Workplaces etc. “Healthy” Settings such as Cities, Towns, Schools, Workplaces etc.
ADVOCACY, HEALTH IMPACT ASSESSMENT HEALTH IN ALL POLICIESADVOCACY, HEALTH IMPACT ASSESSMENT HEALTH IN ALL POLICIES
Interventions & Multi-Sectoral Action
MSA
Unhealthy diet and physical inactivity
Ministries including• Health• Agriculture• Finance•Transport• Trade and Industry• Education• Labour• Urban planning• Justice
Other stakeholders including• Industry• Civil society• NGOs• Academia
MINISTRIES Health, Agriculture, Finance, Transport, Trade and Industry Education, Labour, Urban planning, JusticeOTHER STAKEHOLDERS Civil society, NGOs, Academia, Private sector, Donor, development partners
20

MSA-Entry Points
National multi-ministerial forumNational• Effective only with commitment at the highest level,
need a good driver, Health in All Policies
City/District/Village levelSubnational• More feasible, leverage local government, collective
voice of community, government closer to the community, local ordinances
Tobacco/Alcohol/Physical ActivityRisk factor• Facilitators-activism, pressure groups, champions,
international agreements (FCTC), global reporting, more palpable interventions, common good /common enemy
Inter ministerial
Local Government
Cross sector working groups 21

Current inter-sectoral mechanisms: MOH participation• Cabinet Committee for a Health-Promoting Environment.
• Established under NSP-NCD.• Chaired by the Deputy Prime Minister, members consist of 10
Ministers
• National Council on Food Safety and Nutrition• Established under the National Plan of Action for Nutrition.
• MOH is also a permanent member of various inter-ministerial committees under several ministries e.g.• Ministry of Education;• Ministry of Youth and Sports;• Ministry of Housing & Local Governments;• Ministry of Women, Family and Social Affair. 22

Current inter-sectoral mechanisms
23
Cabinet Committee for A Health Promoting Environment
Main TOR: To determine policies that creates a living environment which supports positive behavioural changes of the population towards healthy eating and active living
Chaired by the Deputy Prime Minister1. Minister of Health2. Minister of Education3. Minister of Information, Communications, Arts & Culture4. Minister of Rural & Regional Development5. Minister of Agriculture and Agro-based Industry6. Minister of Youth & Sports7. Minister of Human Resource8. Minister of Domestic Trade, Co-operatives and Consumerism9. Minister of Housing and Local Governments10. Minister of Women, Family and Social Affairs

Strategy 7 NSP-NCD: Policy & Regulatory Interventions• Main thrust of NSP-NCD• Health promotion and education will increase awareness and
knowledge• However changes in behaviour is strongly influenced by our
living environment
Awareness Knowledge Behavioural Change
Supportive living environment
Health promotion & educations
Policies & regulations24

25

Strategy 7: Policy & Regulatory Interventions, Progress thus far…• Guideline on marketing of foods and non-alcoholic beverages
to children (Self-regulatory, August 2013).• Strengthening implementation of the Framework Convention
for Tobacco Control (FCTC).• Guideline on food and beverages sold in school canteens
(revised guideline, January 2012).• Banning of sale of food & beverages by mobile vendors
outside of school perimeters (2012)• Health-promoting workplaces in the public sector
• Healthy menus during meetings• Healthy vending machines• Healthy cafeterias 26
There is still much that needs to be done….

Lessons learned from the past and current attempts to work with other sectors• Go for the path of least resistance.
• Perhaps less impact, but at least establish the link and develop trust.
• Compromise, find the “middle path”• You cannot force the other sectors to go 100% your way.
• Be creative – think “out-of-the-box”• Use other existing mechanisms not previously used to move the
NCD prevention agenda forward.
• Be sensitive to current global/national trends.• Use any opportunity to move the NCD prevention agenda
forward.27

Meet their primary interest-NCD prevention can be a Co-Benefit
EducationImproved scholastic outcome
Improved health of children
AgricultureImproved
production of fruits and
vegetables
Improved consumption of
f&v in population
IndustriesImproved
productivityLess expenses on sickness of
employees
Healthier people
Urban planning
Beautiful city, more tourists, more money
More physical activity
28

Strategy 5, Research
• What’s new?• Currently developing a research framework for developing and
evaluating behaviour change interventions in combating obesity among Malaysians.
• JOM MAMA – a pre-pregnancy intervention for the future prevention of obesity, diabetes and CVD.
• SEACO Demographic Surveillance Site.• HOPE-4: Hypertension Outcomes Prevention and Evaluation 4;
cluster randomised trial of a model hypertension and CVD risk assessment, detection, treatment and control programme.
29

Challenges for Malaysia
• The main challenge in policy and regulatory interventions remain that they are mostly under the responsibilities of ministries and departments other than Ministry of Health• Ministry of Health needs to take leadership role.• Need to find a win-win solution – “mutuality of interest”.• Economic and “political” consideration remains paramount and
needs to be acknowledged.• The health sector needs to play a strong advocacy role.
30

Summary
• Preventing and controlling NCD is an urgent priority for all countries.
• Most of the drivers of NCDs and their risk factors lie outside the control of the health sector.
• Specific for NCDs:• MSA is required to create enabling environments, so that healthy
choices are the easy choices.• MSA is also required to break the cycle of poverty and NCDs.• The prevention and control of NCDs and their risk factors have a
positive impact not only on health, but also on productivity and economic and social development.
31

Health promotion champions
• Public health personnel are most suited to become health promotion champions• Health knowledge• Clinical skills• Communication skills• Right attitude• Confidence among people• Friendly 32