Embed Size (px)
DESCRIPTION
A short introduction to Stewart's model of acid-base disturbances. Modified from a talk I gave during a fellow's retreat back in 2006 in the beautiful Seven Spring's resort.Will probably get excommunicated by the Nephrology Orthodoxy for endorsing Stewart's "heresy" :) but it is worth it!
Citation preview

New models of acid-basebalance and their application to critical care nephrology
Christos Argyropoulos MD PhDDepartment of Internal Medicine, Renal and Electrolyte Division

Goals of acid-base models
1. Patient Care : diagnosis and treatment of complex acid-base disorders
2. Medical Education: establish the paradigm of acid-base physiology taught in medical curricula
3. Research : Advance understanding of genetic disorders of ion transport in epithelial celss

Qualifications of an acid-base model (formal)
A general acid-base model should provide:1. the classification of the disturbance as
“metabolic” or “respiratory” 2. a mechanistic explanation for the underlying
disturbance 3. a quantitative estimate of the magnitude of
an acid-base disturbance4. the enumeration of the independent
variables that govern the disturbance.

Qualifications of an acid-base model (informal)
A general acid-base model should answer the following questions:
1. Which organ/system is causing the disturbance?
2. How does it cause the disturbance?3. What is the magnitude of the
disturbance4. What should I do to fix this?

“Standard” Model
• Acid = H+ donor, Base = H+ acceptor
• Final pH = function of amount of acid added or removed
• Plasma membranes may be permeable to H+
• Analysis of a single acid – base (HCO3-/CO2) buffer system suffices to understand all disorders
• Magnitude of disorder estimated by the Henderson Hasselbach equation

“Standard” model or modelS ?
• Magnitude of the disorder is used to decide mechanism/type/”dose” of therapy
• Two main approaches to quantification:– The “six” rules of thumb (medicine boards
a.k.a “Boston approach”)– Standard Base Excess and PCO2 (Anesthesia
and Surgical boards aka “Copenhagen” approach)

Six rules of thumb
1. The 1 for 10 Rule for Acute Respiratory Acidosis 2. The 4 for 10 Rule for Chronic Respiratory Acidosis 3. The 2 for 10 Rule for Acute Respiratory Alkalosis 4. The 5 for 10 Rule for a Chronic Respiratory
Alkalosis 5. The One & a Half plus 8 Rule - for a Metabolic
Acidosis 6. The Point Seven plus Twenty Rule - for a
Metabolic Alkalosis

Standard Base Excess
“Amount of acid or base in meqs needed to titrate 1 lt of blood to pH 7.4 at pCO2 of
40mmHg keeping the temperature constant at 37oC”
• Calculated on the basis of modifications of the Van Slyke equation:
SBE = 0.9287 × (HCO3– – 24.4 + 14.83 × [pH – 7.4])• “SBE” = metabolic component, “CO2” =
respiratory component

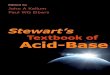
Does the model hold true for all pH values?
The Henderson Hasselbach predicts a linear relation between pH and logPCO2
3
2
[ ]log( ) log( )2
CO
HCOPCO pH
K S
But in vitro in vivo CO2 equilibration studies demonstrate a non-linear relationship between log PCO2 and pH over a wide range of pH

Copyright ©1997 American Physiological Society
Constable, P. D. J Appl Physiol 83: 297-311 1997
No Caption FoundThe curvilinear relationship between pH and log PCO2

Clinical “failures” of the standard model
• The mechanism of hyperchloremic acidosis during NaCl administration and cardio-pulmonary bypass *
• Metabolic alkalosis associated with decreased plasma albumin concentrations **
**J Appl Physiol 84: 1740-1748, 1998
*Anesthesiology. 2000 Nov;93(5):1170-3 Anesthesiology 1999, 90:1265--1270
Critical Care 2002, 6(Suppl 2):2

New models of acid base balance – the Stewart model
• They try to offer explanations for such “extreme” phenomena in human physiology and disease
• Include the “standard” model formulas as special cases
• Grounded on physical chemistry and equilibrium thermodynamic analysis of uni- and multi-compartmental fluidic systems
Can J Physiol Pharmacol 61:1444-1481 1983J Appl Physiol 86:326-334, 1999
J Appl Physiol 95:2333-2344, 2003

Physico-chemical basis of “new” acid basis models
In any physiologic solution, that is at thermodynamic equilibrium the
following laws simultaneously apply to all acid/base pairs:
1. Conservation of mass2. Conservation of charge3. Law of mass action

Acid – base pairs in a physiologic solution
1. Water Dissociation Equilibrium2. Electrical Neutrality Equation3. Weak acid (albumin, phosphate,
sulfate etc) dissociation equilibrium4. Conservation of mass for weak acids5. Bicarbonate ion formation
equilibrium (“standard” model)6. Carbonate ion formation equilibrium

Acid – base pairs in a physiologic solution

The “modified” Henderson Hasselbach equation
Accounting for all these systems simultaneously leads to a modified HH equation:
2 2
[ ] [ ] /( 10 )log
pHtot
CO CO
SID K A KpH pK
S P
Kα : dissociation constant for weak acids
Atot : total concentration of weak acids
SID+ : Strong Ion difference =
[Na+] + [K+] –[Cl-] – [lactate] =
[HCO3-]+[A-]

What does this all mean?
• The bicarbonate acid base system (“standard” HH) is a marker of acid base status (“CXR – pneumonia” concept)
• The three main “independent” variables that control the pH are:
1. PCO2 : controlled by the lungs
2. Atot : controlled by the liver3. SID: kidney, intestine and tissue

What does this all mean?

Dependent v.s. Independent variables in the Stewart model
• The designation of certain variables as independent while others (pH) are dependent is a controversial aspect of the theory
• The theory was developed years before the first epithelial H+ transporter was cloned/identified i.e. biological systems do handle protons directly …

Dependent v.s. Independent variables II
• Equilibrium approaches cannot be used to infer causality relations without a model of the system as exists far from equilibrium (ion transport)
• However equilibrium models render constraints that any quantitative description of the system should obey
• The modified HH is thus a more general version of the Henderson Hasselbach and include the “6-pack” rule of acid base disorders of the “standard” model

Thinking about fluids and RRT in the ICU
Even fluids that do not have any CO2 will have an effect in the pH of body fluids according to the new theory
• After infusion, the fluid administered will equilibrate with plasma, ECF and finally ECF
• In the new “equilibrium” state, the SID and Atot of the ECF will change towards the ones of the infused fluid

Acid – Base Analysis within the “new” paradigm I

Acid – Base Analysis within the “new” paradigm II

Clinical Use of the Stewart Model
• Formulas are more complicated than the standard acid-base approach
• Calculation of the Strong Ion Difference may be accomplished by the formula:
11
2[ ] (1000 2.46 10 /10 )
[ ] (0.123 0.631)
[ ] (0.309 0.469)
pHCOSID P
alb pH
phos pH
Detection of gap acidosis is done by the Strong Ion Gap:2 2[ ] [ ] [ ] [ ] [ ]
[ ] [ ] [ ]
SIG Na K Ca Mg
Cl lactate SID

Thinking about fluids in the ICU
It is the SID value of NS, not the dilution of plasma bicarbonate that causes the “dilutional” acidosis of massive rescuscitation, CPB *
Paradoxically, sodium bicarbonate will have an alkalizing effect only if ventilation is not limited (infusion of “high” SID fluid)
If ventilation is limited, CO2 will rise, and pH will fall after sodium bicarbonate infusion**
*Anesth Analg 2003;96:919-922
**Am. J. Respir. Crit. Care Med., 2000;
161(4): 1149-1153 J Nephrol. 2005 18(3):303-7

Acid – Base and Chloride Transport I
• The “independent” variable of SID may explain the following basic science observations:
1. Excretion of any organic anion will decrease SID (Na+ will accompany the anion)
2. NH4+ excretion will increase SID (Cl- will accompany the cation but Na+ will stay behind)
3. Glimpses of the non-equilibrium model for acid base control might be re-constructed from clinical disorders of ion transport(-ers)

Acid – Base and Chloride Transport II
A hypochloremic metabolic alkalosis is characteristic of the following disorders:
Cystic Fibrosis: due to mutations of CTFR (a chloride channel)
Bartter syndrome: due to mutations of ROMK (potassium channel) /NKCC2 (sodium chloride transporter) /CLCNKB (chloride channel)
Alkalosis is due to :“volume contraction” (standard model) elevated SID (Stewart model)

Internet Resources
• UPMC’s Department of Critical Care pHorum (references and excel based calculator of SIG/SID, modified HH):
http://www.ccm.upmc.edu/education/resources/phorum.html
• The full text of Stewart’s 1983 book is available on the web for free: http://www.acidbase.org/
• A “colorful” introduction at the Anesthetist: http://www.anaesthetist.com/icu/elec/index.htm