Embed Size (px)
Citation preview

NOACPraneel Kumar


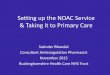
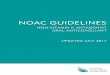
Fibrinogen Fibrin
Common Pathway
Thrombin
Xa
Prothrombin
Clot
Xa
BlockerApixaban
Rivaroxaban
Dabigatran
New Oral Agents

Dabigatran(Pradexa)
• Bioavalibility – 3-7% ( do not open,break,chew or crush capsule)
• Half life – 12 -17 hrs
• Elimination – 80% renal clearance
• Metabolism – minimal ( not a substrate,inhibitor or inducer of CYP 450 enzymes)
• Contraindicated in patient with Cr clearance <30ml/min and reduced dose is recommened with Cr clearance of 30 -50

RE – LY Trial
• Biggest Dabigatran trial - 18113 patient
• Dabigatran vs Warfarin in Patients with AF ( non valvular)
• Publised in NEJM on Sept,2009
• Randomised to 110mg BD Pradexa,150mg BD Pradexa and warfarin with INR goal of 2-3
• Primary effective outcome- stroke or systemic embolism
• Primary safety outcome – major bleeding
• Median follow up of 2 years

Primary Effective Outcome
• Lower dose was non inferior to warfarin with regard to stoke or systemic embolism
• Lower dose showed less major bleeding ( 3.36% for warfarin and 2.71% for 110mg Pradexa)
• 150mg Prdexa- lower rate on stroke or systemic embolism compared to warfarin ( 1.11% vs 1.69%)
• Similar rate of bleeding – intercarnial bleed more common with warfarin and GI bleed with Pradexa 150mg
• High incidence of Dyspepsia with Pradexa (20% discontinued study due to this)

Rivaroxaban (Xarelto)
• Bioavailbility – 80-100% ( dependent on food )
• Half life – 5-9hrs
• Elimination – 30-40% renal clearance unchanged
• Metabolism – via CYP 450 and 3AF
• Contra indicated in patients with Cr Clearance of < 15ml/min

ROCKET AF study
• Publised in NEJM on September,2011
• Rivarxaban vs warfarin in non valvular AF
• RCT – 14,264 patient randomized to receive 20mg of Rivoraxaban or warfarin
• Primary efficacy end point – stroke or other systemic embolism
• Primary safety End point – major or non major clinically relevant bleeding

Primary Efficacy Outcome
• Significant reduction in the primary end point of stroke or systemic embolism
• 1.7% per year in rivaroxaban compared to 2.15 % per year in those treated with warfarin

Primary safety end Point
• Similar rates of bleeding and adverse events compared to warfarin
• Rivaroxaban - Less ICH bleeding but increased GI bleeding
• No dyspepsia symptoms

Apixaban ( Eliquis)
• Bioavailability – 50%
• Half life -12hrs
• Elimination – 25-30% renal clearance
• Metabolism – Via CYP 450 and CYP3A4

ARISTOTLE Study
• Publised in NEJM on sept 2011
• Apixaban 5mg Bd vs warfarin ( INR 2-3 ) with AF
• Primary outcome – stroke or other systemic embolism
• Primary safety outcome – major or non major clinically relevant bleeding

Primary outcome
• Apixaban compared to warfarin significantly decreased risk of stroke and systemic embolism by 21% ( p=0.01) therefore non inferior and superior
• Significantly reduced mortality by 11% ( p=0.047)

Primary safety outcome
• Reduced major bleeding by 31% ( p<0.001)
• Decreased in ICH bleeding
• No increase in GI bleeding

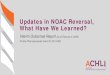
Recommendation for neuraxial anaesthesia


Managing the Bleed
• Scarce literature for how to manage bleed
• Currently no reversal agent