Embed Size (px)
Citation preview

Normal organ Biological Effective Dose (Saving kidney, bone marrow and liver)
Safety and toxicity
Azmal/Su/Jamila

BED: Introduction
• Radiobiological model
• Can help predict clinical outcomes when treatment parameters are altered
• base on:
– linear quadratic model
– radiobiological data for patients
• assumes:
– full repair between two fractions
– no proliferation of tumor cells

BED: Definition
Biologically effective dose (of a given schedule) is:
• the total dose required to give the same log cell kill as the schedule being studied,
• at an infinitely low dose-rate or with infinitely small fractions well spaced out;
• with an overall time factor for repopulation during continued irradiation
• for a tissue with a particular α/β ratio only

BED: Formula
BED=nd(1+d/[α/β]) - loge2 (T-Tk)/αTp
• n fractions of
• d Gy are given
• in an overall time of T days
• and tumour repopulation doesn’t start until day Tk
(using k for kick-off, or onset, of the delayed repopulation during fractionated irradiation)
• assuming a constant repopulation rate or cell doubling time Tp up to the end of the RT

α and β
• tissue specific coefficients for radiation damage
• α proportional to dose (one single event is lethal)
• β proportional to dose squared (two sublethalevents required for lethal damage)
• α/β ratio
- repair capacity
- quantifies the sensitivity of a given tissue to changes in fractionation

Dose limiting organ(organ with largest absorbed dose)
• nonmyeloablative radionuclide therapy: red marrow
• 90Y-ibritumomab tiuxetan therapy: liver
• 131I-tositumomab: lung, liver and kidney
• peptide receptor radionuclide therapy (PRRT): red marrow and kidney
• 90Y-glass or resin microsphere: liver and lung
• 11C-docetaxel: liver and gall bladder
• 89Sr, 153Sm, 186/188Re- RP: bone surface, red marrow
• 223 RaCl2 : bone surface

Dose limiting organ(organ with largest absorbed dose)
• nonmyeloablative radionuclide therapy: red marrow
• 90Y-ibritumomab tiuxetan therapy: liver
• 131I-tositumomab: lung, liver and kidney
• peptide receptor radionuclide therapy (PRRT): redmarrow and kidney
• 90Y-glass or resin microsphere: liver and lung
• 11C-docetaxel: liver and gall bladder
• 89Sr, 153Sm, 186/188Re- RP: bone surface, red marrow
• 223 RaCl2 : bone surface

Red marrow
Non specific/?SSRT mediatedUptakeβ or γ range
Mild transient myelotoxicityMyelodysplastic syndrome
Blood basedImage based
2-3 Gy
Indv. dosimetryα emitter

Figure: Penetration of γ-rays, β particles and α particles into bone marrow
Cancer J 2013;19: 71-78

Kidney
Megalin/ cubilinSSRTPinocytosisOrganic anion transporter
Radiation nephropathy: Acute/chronic
PlanarSPECT3D RBD
28 vs 40 Gy<7.4GBq/m2
L-lys & L-arg 25g/25g Fractionation

111In-DTPA-exendin-4
40-50
MBq
Megalin deficient : 20-40 Gy/kidney
Wild type: 70 Gy/kidney
↓Body wt.
↑uri. protein
↑U&C
Histopath
16-19 weeks
Thickening and necrosis of tubular basal lamina Glomerulo-sclerosisMelis et al. J NuclMed. 2010 (51)

Megalin
• 600 kD, member of LDL protein family
• Also known as LRP2
• A multiligand binding receptor
• Expressed in plasma membrane of absorptive epithelial cells: lungs, oviducts, thyroid, parathyroid, eyes & ears
• Present as Megalin/Cubilin complex, a scavenging protein receptor in apical membrane of renal proximal tubular cells.
Megalin
• Facilitates renal re absorption (endocytosis) of peptides, (binding) proteins, hormones, drugs, toxins and enzymes.
• Re absorption of radio-labeled octreotide in mice.
• ↓uptake and ↓renal retention of 111In-SSTR analogue is seen in absence of megalin.

Figure: Abdominal scintigraphy in a patient
after 220MBq 111DTPA-octreotide:
(A) without and (B) with coinfusion of LysArg
Renal activity 52% controlled with LysArg
A B
Eur J Nucl Med (2003) 30:9-15
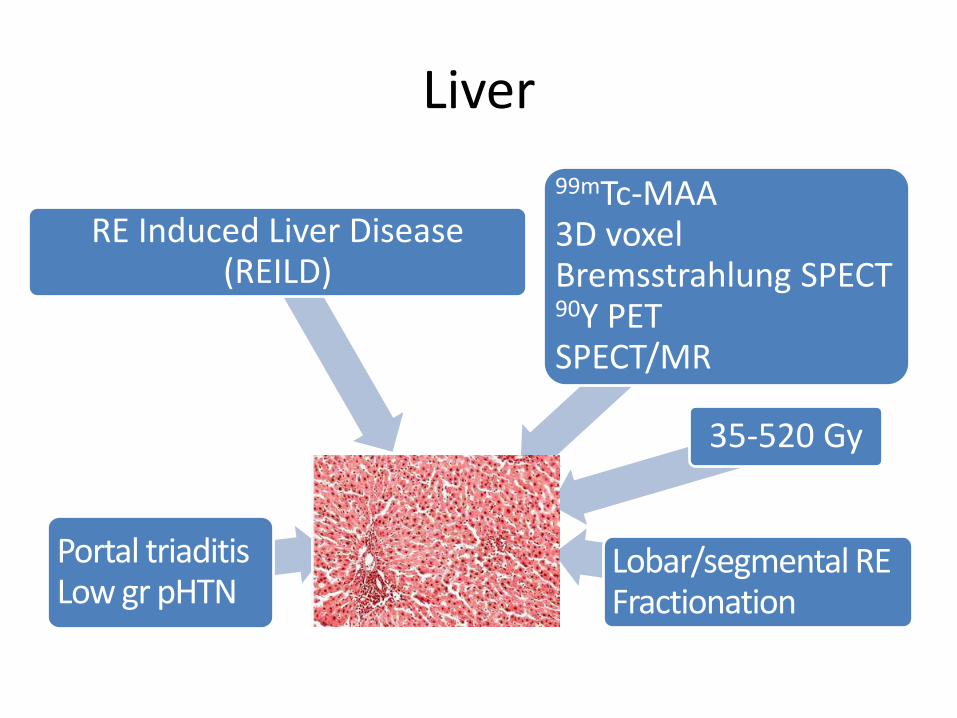
Liver
Portal triaditisLow gr pHTN
RE Induced Liver Disease (REILD)
99mTc-MAA3D voxelBremsstrahlung SPECT90Y PETSPECT/MR
35-520 Gy
Lobar/segmental RE Fractionation

Dose delivered to liver
Figure : Liver absorbed dose and tolerability Front Oncol 2014 4: 210

Lung
β radiation mediated damage
Prog. pul. insuf, Pul. fibrosisRadiation pneumonitis
99mTc-MAA
<20-30 Gy
Multicompartmentalmethod

Dose delivered to lung
Figure : Lung absorbed dose and tolerability Front Oncol 2014 4: 210

Suggested normal limits from literature
RN Disease Max Limit131I DTC, Benign thyroid, NB, BCL 2Gy to blood90Y Liver NET 2Gy to BM
Radiopeptide
NET 28Gy and 40Gy for kidneys
90Y-microspheres
HCC, metastatic liver tumors Variable ?35-520Gy
Zevalin NHL, Follicular lymphoma WB AD 1.3-2.4mGy/MBq
Bexxar NHL. Folliclar lymphoma WB AD 0.65-0.75 Gy

Suggested safety measures from literature
RN Organ safety measures131I, 90Y Bone marrow Individual dose optimization
radiopeptide
Kidney Co administratin of amino acids
90Y-microspheres
Liver Selective placement of catheter to hepatic artery, targeting of least possible number of segments
90Y-microspheres
Lung LS 20%, <20 or 30Gy


References
Fowler. Br J Radiol, 2010; 83:554-568
Jones et al. Clin Oncol, 2001;13:71-81
Brady et al. Cancer J 2013;19: 71-78
Cremonesi et al. J Nucl Med, 2007;48:1871-1879
Rajendran et al. J Nucl Med, 2008;49:837-844
van der Veldt et al. Eur J Nucl Med Mol Imaging, 2010;37:1950-1958
Rolleman et al. Eur J Nucl Med, 2003;30:9-15
Cremonesi et al. Front Oncol, 2014;4:210
Forrer et al. Eur J Nucl Med Mol Imaging, 2009;36:1138-1146
Baroneet al. J NuclMed. 2005;46:99s-106s
Bodeiet al. EurJ NuclMed Mol Imaging. 2008;35:1847-1856
Otte et al. Eur J Nucl Med,1999;26: 1439-1447
Fisher et al. J Nucl Med, 2009;50:644-652
Zevalin prescribing information; http://www.zevalin.com/v3/pdf/
Bexxar prescribing information; http://us.gsk.com/products/assets/ us_bexxar.pdf.
O’Donoghue et al. Cancer Biother Radiopharm, 2002;17:435-443
Boucek et al. Eur J Nucl Med Mol Imaging, 2005;32:458-469