Embed Size (px)
DESCRIPTION
Physical Activity
Citation preview

Physical activity and cardio-vascular prevention
Graziano OnderCentro Medicina dell’InvecchiamentoUniversità Cattolica del Sacro Cuore
Rome - Italy

Factors for successful aging Male and female aging
Social factorsEducation, social support, prevention, abuse
Personal factorsBiology, genetic factors
Social and Health servicesPromotion of health, primary and secondary prevention, long-term care
Environmental factors Metropolitan/rural area, personal environmental, injuries
Economical factorsType of work.
Life style Physical activity, nutrition, smoke, alcohol, drugs abuse
Successful aging
0NU 2002

EXERCISE IN THE ELDERLY
THE ROLE OF EXERCISE IN THE ELDERLY
a) In the young-old, exercise has much the same function as in the young:
- prevention of disease - maintenance of aerobic capacity
- maintenance of muscle strength - psychological well-being

b) In the old-old, exercise is still used for its preventive effects, but more often for:
- secondary or tertiary prevention - rehabilitation from pre-existing chronic conditions
c) Some of the most important goals of exercise in the frail elderly are:
- the improvement of muscle strength and endurance capacity to allow increased functional independence


Characteristics of study poplulation according to physical activity

Risk of disability according to physical activity

- the prevention of falls and fall- related injuries
- maintenance of fat-free mass
- cardiovascular reconditioning, treatment of peripheral vascular
- adjunctive treatment of depression, anxiety, isolation, insomnia, dementia
- rehabilitation from neurologic diseases
- increased survival


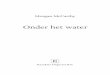
Crude and adjusted relative risk of mortality
Adjusted for gender and for all other possible risk factors for death (gender, physical and cognitive disability, cardiovascular diseases, pneumonia, cancer, stroke, diabetes, chronic obstructive pulmonary disease, renal failure, Parkinson’s disease, depression, delirium, and arthritis).

Preventive Medicine 47 (2008) 422–426

Crude and adjusted relative risks (RRs) of mortality in the Italian cohorts of the ilSIRENTE study, examined at baseline between 2003
and 2004 and after 24 months
Sedentary: subjects walking less than 1 h per day; Active: subjects walking 1 h or more per day.Adjusted for age, gender and for other possible risk factors for death (functional and cognitive disability, congestive heart failure, hypertension, osteoarthritis, depression, number of medications, body mass index, cholesterol and C reactive protein).

Incidence of Coronary Heart DiseaseHonolulu Heart Program
2678 active menAge: 71-93 yearsFU: 2 to 4 years
Hakim et al. Circulation 1999

Vigorous Moderate Vigorous Moderate0
102030405060
75-79 years 80-84 years >=85 years
AMI r
ate
per 1
mill
ion
pers
on-h
ours
Estimated rates of AMI
Mittleman et al. NEJM 1993
Men WomenMen Women

Sacco et al. Stroke 1998
Association between physical activity and stroke
Case control study1047 men and womenAge: 70 years

Mediators ?

Physical activity - Lipids
Total Cholesterol LDL HDL Triglycerides-20
-10
0
10
20
30
40
Active Sedentary
% c
hang
e
Petrella et al. Diabetes Care 2005
Observational study380 men and womenAge: 68 yearsFU: 10 years

Irwin et al. JAMA 2003
Physical activity – Body composition
173 women Age: 55-70 years

Physical activity – Diabetes
Knowler et al. NEJM 2003
3234 non-diabetic Age: 50 years FU 2.8 years

Physical activity – Glucose intolerance
Van Dam et al. Med Sci Sports Exerc 2002
424 men Age: 74 years FU 5 years

Physical activity and inflammation
Gaffken et al. Am J Epidemiol. 2001

Physical activity – Hypertension
Whelton et al. Ann Intern Med 2002

Mediators
1. Antiatherogenic effects2. Antithrombotic effects
↓plasma fibrinogen levels↑ plasminogen activator↑ active tissue plasminogen activator↓ plasminogen activator inhibitor
3. Endothelial function alterationrelease of endothelium-derived relaxing (NO)
Fletcher et al. Circulation 2002

Mediators
4. Autonomic functional changes↑ parasympathetic activity
5. Anti-ischemic effects↓ myocardial work (↓ BP and HR)
6. Antiarrhythmic effectsimproved myocardial oxygen supply-demand balance↓ in sympathetic tone and catecholamine release↑ ventricular fibrillation during strenuous exercise
Fletcher et al. Circulation 2002

Which type of intervention?
1. Dynamic aerobic (endurance) exercise – running or walking
2. Dynamic resistance anaerobic (strength) exercise – weight lifting

Endurance

Endurance

Resistance

Resistance

Endurance training
Cornelissen et al. Hypertension 2005
Blood pressure
Cardiac output
Heart rate
Stroke volume
Vascular resistance

Resistance training
Cornelissen et al. J Hypert 2005

Williams et al. Circulation 2007
Resistance and endurance trainingEndurance Resistance
Body fat ↓↓ ↓
Lean mass 0 ↑↑
Strength 0↑ ↑↑↑
Insulin sensitivity ↑↑ ↑↑
HDL 0↑ 0↑
LDL 0↓ 0↓
HR ↓↓ 0
Stroke volume ↑↑ 0
Cardiac output (maximal) ↑↑ 0
SBP ↓ 0↓
Basal metabolic rate 0↑ ↑
Quality of life 0↑ 0↑

For persons at moderate to high risk of cardiac events, RT can be safely undertaken with
proper preparation, guidance, and surveillance … given the extensive evidence of the benefits of aerobic exercise training on the modulation of cardiovascular risk factors, RT should be viewed as a complement to rather than a replacement for aerobic exercise.
Resistance training
Williams et al. Circulation 2007

Training - Guidelines
Fletcher et al. Circulation 2002
Frequency Intensity Duration ModalityEndurance training3–5 days/week 50%–70% max HR 20–60 min Lower extremity: walking,
jogging/running,stairclimberUpper extremity: arm ergometryCombined: rowing, cross-country ski machines, combined arm/leg cycling,swimming, aerobics
Resistance training2–3 days/week 1–3 sets of 8–15 RM Lower extremity: leg
for each muscle group extensions, leg curls, leg press, adductor/abductorUpper extremity: biceps curl, triceps extension, bench/overhead press.

Age-Associated Alterations in Physiological Response to Aerobic
Exercise• Reduced aerobic capacity: decline in V˙ O2
max of 8% to 10% per decade in nontrained populations
• Reduced maximal heart rate of 1 beat/min per year
• More rapid increase in systolic blood pressure with exercise
• Attenuated rise in ejection fractionFletcher et al. Circulation 2002

Classification of Physical Activity Intensity
Fletcher et al. Circulation 2002
MET=metabolic equivalents
1 MET = resting metabolic rate of 3.5 mL O2 * kg-1 * min-1

If exercise could be packed into a pill, it would be the
single most widelyprescribed, and beneficial,
medicine
Robert N. Butler, M.D. Director, National Institute on Aging
Bottleexercise
PHYSICAL ACTIVITY = MEDICINE

Potential risks
General
• Muscle soreness
• Soft tissue injury
• Falls
• Fractures
Resistance training
• Detached retina
• Hernia
• Hemorrhage
• Lumbar disk hernia

Potential risks Vigorous exercise
• Sudden death
• Acute myocardial infarction
• Hypoglycemia in persons with diabetes
• Orthostatic hypotension
• Arrhythmia

8,58,7
7,57,98,0
6
7
8
9
10
0 6 12
Sco
re
Physical activitySuccessful aging
P<0.001
mo mo
LIFE-P SPPB score
Pahor et al J Gerontol A Biol Sci Med Sci 2006
mo

LIFE-P – Side effects
Pahor et al J Gerontol A Biol Sci Med Sci 2006

Exercise in the Elderly- Screening
• History• Physical• Cardiovascular reserve: get up and down
from the examination table, walking 15 m, climbing 1 flight of stairs, cycling in the air for 1 min while lying down
• ECG
Gill et al JAMA 2000

It is not necessary that all individuals beginning a moderate-intensity and moderately progressive exercise program undergo an exercise stress test, although this issue remains controversial.
Gill et al JAMA 2000
Exercise in the Elderly- Screening

Exercise in the Elderly
Pre-exercise period of stretching and light activity involving the large muscle groups for 5-10 minutes
Extended cool-down period after physical activity
Importance of range of motion and flexibility exercises
Evaluation of participant’s footwear
Evaluation of thermoregulatory capacity of participant
Gill et al JAMA 2000

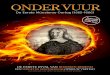
Majority of Americansdo not follow healthy lifestyle
0
20
80
1002000 Behavioral Risk Factor Surveillance System, N = 153,805
Respondents(%)
Smokers
Reeves et al. Arch Intern Med. 2005
BMI≥25 kg/m2
Consumesfruits/vegetables
<5x/day
Infrequentexercise
(<5x/week)
60
40
24.0
59.9
76.7 77.8

Conclusions
1. People of all ages, both male and female, benefit from regular physical activity
2. Significant health benefits can be obtained by including a moderate amount of physical activity on most, if not all, days of the week
3. Additional health benefits can be gained through greater amounts of physical activity

Conclusions
4. Physical activity reduces the risk of premature mortality in general, and of coronary heart disease, hypertension, stroke, and diabetes mellitus in particular
5. Both aerobic (endurance) and resistence training may influence health outcomes
6. Potential risks related to physical activity should be always considered

Søren Kierkegaard in 1847 in a letter to his sister in law who had just been ill.
”Do not give up your wish to walk. I walk every day and feel well and walk away from any illness. I have had my best thoughts while walking and I do not know of any thoughts so dark that I can not walk away from them…”