Embed Size (px)
Citation preview

Dr. Rahi kiran.B
SR Neurology
GMC Kota

Parkinson’s disease (PD) is the second most common neurodegenerative disease, affecting 1% of the population over 55 years of age.
Disease is characterized by the loss of ~50–70% of the dopaminergic neurons in the substantia nigra, a profound loss of dopamine (DA) in the striatum, and the presence of intracytoplasmic inclusions called Lewy bodies (LB).
2

Four cardinal symptoms:
resting tremor
bradykinesia
muscle rigidity
postural insatability
3

4
Step 1. Diagnosis of a parkinsonian syndrome
Bradykinesia and at least one of the following:• muscular rigidity
• rest tremor (4–6 Hz)
• postural instability unrelated to primary visual,cerebellar, vestibular or proprioceptive dysfunction.

Step 2. Exclusion criteria for Parkinson's disease
History of :
repeated strokes with stepwise progression
repeated head injury
antipsychotic or dopamine-depleting drugs
definite encephalitis on no drug treatment
more than one affected relative
sustained remission

Step 2. Exclusion criteria for Parkinson's disease
Strictly unilateral features after 3 yr
Supranuclear gaze palsy
Cerebellar signs
Early severe autonomic involvement
Early severe dementia
Presence of cerebral tumour
Negative response to large doses of L-dopa

Step 3. Supportive criteria for PD
Three or more required for diagnosis of definite PD:
unilateral onsetexcellent response to levodopa rest tremor present severe levodopa-induced chorea
progressive disorder
levodopa response for over 5 yearspersistent asymmetry affecting the side of onset most clinical course of over 10 years.

Section 1. Communication
Section 2. Diagnosis and Progression
Section 3. Treatment
A. Pharmacological therapy for motor symptoms in early PD
B. Pharmacological therapy for motor symptoms in later PD
C. Surgery
D. Other treatment Options
Section 4. Non-motor Features and Their Treatment
A. Mental Health
B. Sleep disorders
C. . Autonomic dysfunction

AAN - American Academy of Neurology
NICE - National Institute for Health and Clinical Excellence
EFNS - European Federation of Neurological Societies

Because people with PD may develop impaired cognitive ability, a communication deficit and/or depression, they should be provided with both oral and written communication throughout the course of the disease. NICE Level D (GPP) [2006]
Offer people with Parkinson's disease an accessible point of contact with specialist services. This could be provided by a Parkinson's disease nurse specialist. [2006]

Suspect Parkinson's disease in people presenting with tremor, stiffness, slowness, balance problems and/or gait disorders. [NICE 2006]
If Parkinson's disease is suspected, refer people quickly and untreated to a specialist with expertise in the differential diagnosis of this condition. [NICE 2006, amended 2017]
Diagnose Parkinson's disease clinically, based on the UK Parkinson's Disease Society Brain Bank Clinical Diagnostic Criteria. [NICE 2006]

Determining the presence of the following clinical features in early stages of disease should be considered to distinguish PD from other parkinsoniansyndromes:
1) falls at presentation and early in the disease course;
2) poor response to levodopa;
3) symmetry atonset;
4) rapid progression
5) lack of tremor; and
6) early dysautonomia AAN Level B D (GPP)

People diagnosed with Parkinson's disease should be seen at regular intervals of 6–12 months to review their diagnosis and reconsidered if atypical clinical features develop.[NICE 2006]
In patients with newly diagnosed PD, older age at onset and rigidity/hypokinesia as an initial symptom should be used to predict more rapid rate of motor progression. AAN Level B
The presence of associated comorbidities (stroke, auditory deficits, and visual impairments), Postural Instability/Gait difficulty (PIGD), and male sex may be used to predict faster rate of motor progression. AAN Level C

Consider SPECT for people with tremor if essential tremor cannot be clinically differentiated from parkinsonism. [NICE 2006, amended 2017]
Do not use positron emission tomography (PET) in the differential diagnosis of parkinsonian syndromes, except in the context of clinical trials. [NICE 2006, amended 2017]

Do not use structural MRI to diagnose Parkinson's disease. It may be considered in the differential diagnosis of other parkinsonian syndromes. [NICE 2006, amended 2017]
Do not use acute levodopa and apomorphine challenge tests and objective smell testing in the differential diagnosis of parkinsonian syndromes. [NICE 2006, amended 2017]

initiation of pharmacologic therapy – goal :
▪ reducing motor symptoms
▪ improving quality of life without causing side effects.
Factors that influence this decision include:
▪ symptom severity,
▪ whether the symptoms affect the dominant hand,
▪ ability to continue working and/or participate in activities such as hobbies,
▪ cost,
▪ patient preference.

Levodopa remains the most effective medication for the treatment of motor symptoms.
Levodopa used as a symptomatic treatment for people with early PD. NICE Level A
The dose of levodopa should be kept as low as possible to maintain good function in order to reduce the development of motor complications. NICE Level A
Modified-release levodopa preparations should not be used to delay the onset of motor complications in people with early PD. NICE Level A

Dopamine agonists are the second most potent class of medication (after levodopa) for control of motor symptoms in PD with good evidence that they can be used in early PD with success.
Dopamine agonists have less likelihood of producing fluctuations in early disease, but are less effective and associated with high side effects and more expensive than levodopa.
18

Dopamine agonists may be used as a symptomatic treatment for people with early PD. NICE Level A
A dopamine agonist should be titrated to a clinically efficacious dose. If side effectsprevent this, another agonist or a drug from another class should be used in itsplace. NICE Level D (GPP)

MAO-B inhibitors may be used as a symptomatic treatment for people with early PD. NICE Level A 2006
Amantadine may be used as a treatment for people with early PD but should not be a drug of first choice. NICE Level D (GPP) 2006

Anticholinergics may be used as a symptomatic treatment typically in young people with early PD and severe tremor, but should not be drugs of first choice due to limited efficacy and the propensity to cause neuropsychiatric side effects. NICE Level B 2006
Beta-adrenergic antagonists may be used in the symptomatic treatment of selected people with postural tremor in PD, but should not be drugs of first choice.
NICE Level D (GPP) 2006

Up to 50% of patients on LD for 5 years - motor fluctuations and dyskinesia.
common if onset before 50 years of age.
unique to LD, and are not produced by the other anti-Parkinson drugs.
Wearing off is the most common type of MF. It refers to the predictable return of parkinsonian symptoms in the hours before the next dose as the plasma level of the drug falls below the critical level.
22

On/off is the unpredictable reappearance of parkinsonian symptoms at a time when central levels of anti-parkinsonian drugs are expected to be within the target of therapeutic range.
Delayed on is delay in the onset of symptom relief after a dose.
Dose failure is a complete failure to develop a favorable response to an incremental dopaminergic dose.
Protein-related offs occur when the transport of LD across the intestinal wall is impeded by competition for facilitated transport by large amounts of neutral amino acids.

Manipulation of the dose or frequency of levodopa can be a first strategy but eventually the emergence of dyskinesias will preclude this.
For patients with PD with motor fluctuations the available evidence suggests: Entacapone and rasagiline should be offered to reduce off time. AAN Level A
Pramipexole and ropinirole should be considered to reduce off time.AAN Level B

Entacapone, a COMT inhibitor and rasagiline, a MAO-B inhibitor, have both been shown in clinical trials to reduce off time by approximately 1.5 waking hours perday
Dopamine agonists such as pramipexole, ropinirole and bromocriptine have beenshown in clinical trials to reduce off time by approximately 15%.

Modified-release levodopa preparations may be used to reduce motor fluctuations in people with later PD but should not be drugs of first choice. NICE Level B
Modified release levodopa remains most useful in addressing overnight wearing off.

Antiparkinsonian medicines should not be withdrawn abruptly or allowed to fail suddenly due to poor absorption to avoid the potential for acute akinesia. [NICE 2006]
The practice of withdrawing people from their antiparkinsonian drugs (so called 'drug holidays') to reduce motor complications should not be undertaken because of the risk of neuroleptic malignant syndrome. [NICE 2006]

If symptoms are very mild, the patient may be choosen not to begin therapy.
Offer levodopa to people in the early stages of Parkinson's disease whose motor symptoms impact on their quality of life. [NICE 2017]
Consider a choice of dopamine agonists, levodopa or monoamine oxidase B (MAO-B) inhibitors for people in the early stages of Parkinson's disease whose motor symptoms do not impact on their quality of life. . [NICE 2017]

Offer a choice of dopamine agonists, MAO-B inhibitors or COMT inhibitors as an adjunct to levodopa for people with Parkinson's disease who have developed dyskinesia or motor fluctuations despite optimal levodopa therapy [NICE 2017]
If dyskinesia is not adequately managed by modifying existing therapy, consider amantadine [NICE 2017] AAN Level C
Do not offer anticholinergics to people with Parkinson's disease who have developed dyskinesia and/or motor fluctuations [NICE 2017]

Do not offer ergot-derived dopamine agonists as first-line treatment for Parkinson's disease . [NICE 2017]
Only consider an ergot-derived dopamine agonist as an adjunct to levodopa for :
who have developed dyskinesia or motor fluctuations despite optimal levodopatherapy
whose symptoms are not adequately controlled with a non-ergot-derived dopamine agonist.

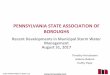
Levodopa Dopamine agonists
MAO-B inhibitors
COMTinhibitors
Amantadine
Motorsymptoms
More improvement
Improvement Improvement Improvement No evidence
Activities ofdaily living
More improvement
Improvement Improvement Improvement No evidence
Motorcomplications
More Fewer Fewer
Off time More reduction reduction reduction No evidence
Adverseevents
Fewer Intermediate Fewer More No evidence
Hallucinations More risk Lower risk Lower risk No evidence

The different types of impulse control disorders –
▪ compulsive gambling,
▪ hypersexuality,
▪ binge eating
▪ obsessive shopping
Recognise that impulse control disorders can develop in a person with Parkinson's disease who is on any dopaminergic therapy at any stage in the disease course. [NICE 2017]

Impulse control disorders can also develop while taking dopaminergic therapies other than dopamine agonists. [NICE 2017]
Recognise that the following are associated with an increased risk of developing impulse control disorders:
Dopamine agonist therapy.
A history of previous impulsive behaviours.
A history of alcohol consumption and/or smoking. [NICE 2017]
Discuss potential impulse control disorders at review appointments, particularly when modifying therapy, and record that the discussion has taken place. [NICE 2017]

first gradually reduce any dopamine agonist and monitor [NICE 2017]
Offer cognitive behavioural therapy targeted at impulse control disorders if modifying dopaminergic therapy is not effective [NICE 2017]
Discuss the following with the person and their family members

Good sleep hygiene should be advised in people with PD with any sleep disturbance NICE Level D (GPP)
Consider modafinil if a detailed sleep history has excluded reversible pharmacological and physical causes. [NICE 2017] Level D(GPP), (AAN 2010)
Care should be taken to identify and manage RLS and RBD in people with PD and sleep disturbance. NICE Level D (GPP)
Consider clonazepam or melatonin to treat RBD if a medicines review has addressed possible pharmacological causes [NICE 2017]
Methylphenidate may be considered for fatigue (AAN 2010)

Consider levodopa or oral dopamine agonists to treat nocturnal akinesia in people with Parkinson's disease. [NICE 2017]
Consider rotigotine if levodopa and/or oral dopamine agonists are not effective in treating nocturnal akinesia. [NICE 2017]

NON- PHARMACOLOGICAL
↑ fluid intake
↑ dietary salt
avoid alcohol / large meals / excessive
warmth,
elevate head of bed.
advised to rise slowly after
sitting/lying for a period of time
PHARMACOLOGICAL
Discontinue unnecessary
medications, e.g., antihypertensives
Fludrocortisone
Domperidone
Midodrin
pyridostigmine

Review the person's existing medicines to address possible pharmacological causes:
▪ antihypertensives (including diuretics)
▪ Dopaminergics
▪ Anticholinergics
▪ Antidepressants [NICE 2017]
Consider midodrine for people with Parkinson's disease and orthostatic Hypotension[NICE 2017]
If midodrine is contraindicated, not tolerated or not effective, consider fludrocortisone [NICE 2017]

Consider emotional fluctuations associated with “OFF” periods → Reduce “OFF”time
When depression is accompanied by symptoms of anxiety, the first priority should usually be to treat the depression. [NICE 2017]
For patients with persistent subthreshold depressive symptoms or mild to moderate depression, consider CBT

TCAs, SSRIs (Amitriptyline may be considered.) AAN Level C
Especially if motor control is suboptimal, consider dopamine agonists such as Ropinirole or Pramipexole, may have antidepressant effect
ECT in severe refractorycases

Do not treat hallucinations and delusions if they are well tolerated by the person with Parkinson's disease and their family members [NICE 2017]
Consider quetiapine to treat hallucinations and delusions in people with Parkinson's disease who have no cognitive impairment, if not effective, offer clozapine
[NICE 2017]
Be aware that lower doses of quetiapine and clozapine are needed for people with Parkinson's disease than in other indications
Do not offer olanzapine to treat hallucinations and delusions, other antipsychotic medicines (such as phenothiazines and butyrophenones) can worsen the motor features[NICE 2017]

Look for triggers
Taper or discontinue sedative medications
Taper antiparkinson drugs in roughly the following order
i. Anticholinergics
ii. Amantadine
iii. Dopamine agonists
iv. MAO-B inhibitors
v. Levodopa

Donepezil should be considered for the treatment of dementia in PD. AAN Level B
Consider memantine for people with Parkinson's disease dementia, only if cholinesterase inhibitors are not tolerated or are contraindicated. [NICE 2017]

Eating chewing gum or a hard candy often decreases drooling by triggering increased spontaneous swallowing movements.
Only consider pharmacological management for drooling of saliva in people with Parkinson's disease if non-pharmacological management is ineffective.
Consider glycopyrronium bromide or topical atropine, if not effective consider botulinum toxin A [NICE 2017]

Vitamin E should not be used as a neuroprotective therapy for people with PD. [NICE Level A 2006 amended 2017]
Co-enzyme Q10, dopamine agonists, monoamine oxidase B (MAO-B) inhibitors should not be used as a neuroprotective therapy for people with PD, except in the context of clinical trials. [NICE Level B 2006 amended 2017]
45

Consider the Alexander Technique for people with Parkinson's disease who are experiencing balance or motor function problems [NICE 2017]
no evidence that one type of physiotherapy was superior to others

Considered in advanced patients when the optimized medical treatment has failed in treating motor symptoms (such as motor fluctuations and/or dyskinesia).
DBS is currently the surgical treatment of choice in advanced PD patients
The most used current targets for PD are:
▪ thalamus (Vim nucleus)
▪ the subthalamic nucleus (STN)
▪ globus pallidus internus (GPi).

may be considered as an option in people with PD who predominantly have severe disabling tremor and where STN stimulation cannot be performed. NICE Level D 2006
Eliminate contralateral rest tremors in 75% to 85% of patients , but there is less effect on rigidity and no effect on bradykinesia.

May be considered to improve motor function and to reduce motor fluctuations, dyskinesia, and medication usage.
Patients need to be counselled regarding the risks and benefits of this procedure. AAN Level C
The overall improvement of ADLs and motor UPDRS scores in the off medication/on stimulation condition has been reported to be on average 50% when compared to the off medications condition before surgery.
Levodopa-induced dyskinesia has also been reduced by 69% on average aftersurgery.

Procedure related
infections (6.1%)
migration or misplacement of the
leads (5.1%)
lead fractures (5%)
intracranial hemorrhage (3%)
skin erosion (1.3%)
Stimulation related
eyelid opening apraxia (1.8-30%)
dysarthria/hypophonia (4-17%)
gait disturbances (14%)
postural instability (12.5%)
weight gain (8.4%)
verbal fluency decline.

Age and duration of PD may be considered as factors predictive of outcome after DBS of the STN. Younger patients with shorter disease durations may possibly have improvement greater than that of older patients with longer disease durations. AAN Level C

may be used in people who:
have motor complications that are refractory to best medical treatment
Are biologically fit with no clinically significant active comorbidity
Are levodopa responsive
Have no clinically significant active mental health problems, for example
depression or dementia. NICE Level D 2006

GPi DBS may be particularly useful for patients who may have troublesome
dyskinesia as well as mild cognitive or behavioral impairment, whereas bilateral
STN DBS may be a choice for patients who are cognitively intact but in whom
reduction in levodopa dosage is primary goal.

Offer people with advanced Parkinson's disease best medical therapy, which may include intermittent apomorphine injection and/or continuous subcutaneous apomorphine infusion. [NICE 2017]
Apomorphine (subcutaneous infusion or injections)-Apomorphine is the most potent dopamine receptor agonist and it can provide symptom relief similar to that of L-dopa. Apomorphine is rapidly absorbed, with onset of effect within 5-15 minutes of subcutaneous injection.

Levodopa–carbidopa intestinal gel is currently available through an NHS England clinical commissioning policy. It is recommended that this policy is reviewed in light of this guidance. [NICE 2017]
Adv - faster absorp-tion, and maintenance of more constant levels of levodopa.
L-Dopa emulsion can be applied by an external pump via a percutaneous tubing into the jejunal cavity in order to provide a nearly constant continuous supply of L-Dopato the blood and thus to the CNS.


Safinamide –Approved, Motor wearing-off, MAO-B-inhibitor, Glutamate modulator, add-on to L-Dopa, 50 or 100 mg/day present in Europe
piribedil, only registered in Europe non-ergot dopamine agonists
Remacemide

Phase III
Istradefylline , Tozadenant- adenosine-2A-receptor antagonists, approved in Japan,
glutamate-receptor-4-antagonists
Pimavanserin- 5HT2A inverse agonist,for dopamimetic-induced psychosis, FDA approved in the USA
Droxidopa- precursor of noradrenaline- approved for the treatment of neurogenicorthostatic hypotension - in PD and MSA

deacetylase inhibitors -target the transport system and reverse the defects caused by the faulty LRRK2 within nerve cells.
Nicotine- Intake of nicotine has shown to slow the degeneration of neurons.Actssimilar to levodopa.
Melatonin-Serotonin derivative that helps insomnia. Also shown to cause a reduction in production of neurodegenerative radicals

packaging GDNF and neurturin within an "encapsulated cell" which will secrete GDNF into the brain of people with PD, with the goal of protecting dopamine neurons.
A gene therapy in development comprises an adeno-associated virus (AAV) vector that delivers the gene for aromatic L-amino acid decarboxylase (AADC) to cells in a part of the brain that controls movement.

Caffeine- Adenosine-receptor antagonist
Inosine- Precursor of urate, antioxidant
Isradipine- Dihydropyridine calcium channel blocker
Nilotinib-small pilot study planned, not started, reduce alpha-synuclein levels

Treatment
summary

Treatmentsummary

prevention (that is, slowing or stopping PD in a prodromal stage) is still a dream
No studies in Pd with comorbidities
trial (for example, against the intrajejunal L-Dopainfusion or DBS) is under way or in planning in PD patients with motor complications.

NICE guideline. nice.org.uk/guidance/ng71. 19 July 2017
American Family Physician :Volume 74(12);2006, 15 Dec
SAMJ October 2009, Vol. 99, No. 10
Parkinson’s disease: The non-motor issues. K R Chaudhuri et al. Parkinsonism and Related Disorders17 2011; 717-723.
emedicine@medscape