Embed Size (px)
DESCRIPTION
Paraganglioma ie both 1) Adrenal- Pheochromocytoma 2) Extra-adrenal paragangliomas.
Citation preview

PARAGANGLIOMA
1
By:Dr. Nishit Gupta
Moderator:Dr. Anil K. Suri

2
INTRODUCTION• It is also known as glomus tumor, chemodectoma,
perithelioma, fibroangioma, and sympathetic nevi.• Paragangliomas are categorised as
neuroendocrine tumors in the WHO classification.• Paragangliomas originate from paraganglia in
chromaffin-negative glomus cells derived from the embryonic neural crest.
• Paragangliomas are closely related to pheochromocytomas, which however are chromaffin-positive.

3

PARAGANGLION SYSTEM
• Paraganglia are the collections of neuroepithelial (Chief) cells scattered throughout the body, associated with sympathetic and parasympathetic nervous system.
• Adrenal medullary chief cells along with extra-adrenal paraganglia constitute the paraganglion system.
4

5

EXTRA-ADRENAL PARAGANGLIA
6
RELATED TO PARASYMPATHETIC
SYSTEM
RELATED TO ORTHOSYMPATHETIC
SYSTEM
Majority Few. (Extra Adrenal Pheochromocytomas)
Non chromaffin Chromaffin
Located in head and neck, mediastinum
Located in retroperitoneal, thoracolumbar, para-aortic region
Secrete little or no catecholamines.
Secrete catecholamines, principally norepinephrine.

7

8
• Microscopically, all paraganglia have a similar morphology characterized by chief cells (chromaffin) arranged in well defined nests (Zellballen-”Cell Balls“ in German) encircled by a thin layer of supporting sustentacular cells.

9
• Chief cells of adrenal medulla are also called as Chromaffin Cells (Pheochromocytes)
• The word 'Chromaffin' comes from chromium and affinity because they can be visualized by staining with chromium salts which oxidize and polymerize catecholamines to form a brown colour.
• Microscopically, cells have finely granular abundant basophilic-amphophilic-eosinophilic cytoplasm. Nuclei are round to oval with stippled(salt and pepper) chromatin and prominent nucleoli.

10
• Ultrastructurally, consist of “dense core” neurosecretory granules that store catecholamines.

PHEOCHROMOCYTOMA
• “ Paraganglioma of the adrenal medulla”• Greek “Phaios- dark, Chroma- color,
Cytos- cell, Oma- tumor") • Composed of chromaffin cells.• Surgically correctable cause of
hypertension.• Age group 40-60 years.• Usually sporadic.
11

12
“10% Tumor”1. 10% extra-adrenal
2. 10% sporadic, bilateral
3. 10% malignant
4. 10% not associated with hypertension
5. 10% (25%) familial

Clinical features
Usually paragangliomas are asymptomatic. Those that secrete catecholamines behave as pheochromocytomas:
• Symptom triad of palpitations, headache sweating.• Hypertension paroxysmal or sustained. (Precipated
by emotional stress, exercise, palpation of tumor)• Orthostatic hypotension ( Fall SBP>20mmHg,
DBP>10mmHg on standing.• Associated nausea, vomiting, abdominal pain• Catacholamine cardiomyopathy, ventricular
arrhythmia.13

14
HISTOPATHOLOGY
GROSS:• Few grams upto 2000grams.• Encapsulated, soft, on section yellowish brown to
reddish brown, with areas of necrosis, hemorrhage, cyst formation.
• Remnants of the adrenal gland attached to one pole.
• Incubation of fresh tissue in potassium dichromate solution turns the tumor to a dark brown color due to oxidation of stored catecholamines.

MICROSCOPY:• Tumor cells (Chief cells) clustered with
sustentacular cells in well defined nests or alveoli (ZELLBALLEN) bound by a delicate fibrovascular stroma.
• Histological patterns :-
1. An anastomosing cell cord or trabecular
pattern
2. Alveolar pattern and
3. A diffuse or solid arrangement of cells
• Intracytoplasmic hyaline globules.15

16
CYTOLOGY OF PHEOCHROMOCYTOMA
• Many dispersed and loosely clustered neoplastic cells.
• Prominent anisokaryosis, uniformly bland nuclear chromatin.
• Abundant fragile cytoplasm ; indistinct cell borders.• Fine red cytoplasmic granulation in a proportion of
cells.• Distinct nucleoli• Contraindicated in view of the risk of precipitating
a hypertensive crisis.

17

Important points• Cellular and nuclear pleomorphism, giant cells, mitotic
figures and even capsular and vascular invasion are
not an expression of malignancy.
• The definitive diagnosis of malignancy is based
exclusively on the presence of metastases.
• Metastasize to skeletal system (ribs & spine), regional
lymph nodes, lungs.
• Malignant tumors are usually larger, have more
necrosis and are composed of smaller cells than their
benign counterparts.18

19
EM & IHC
Ultrastructurally, the hallmark of pheochromocytoma is
the presence of dense-core neurosecretory granules and
abundant large mitochondria.
IHC –
• Chief cells reactive for catecholamines, catecholamine-
synthesizing enzymes, NSE, chromogranin,
synaptophysin, galanin, neurofilaments, serotonin and
synaptophysin and opioid peptides. Keratin negative
(differentiating with other neuroendocrine carcinomas)
• Sustentacular cells are strongly positive for S-100.
CG
S-100

20
Extra-adrenal Paragangliomas
1. CAROTID BODY TUMOR• Located at the bifurcation of common
carotid artery.• Chemodectoma- because it has
chemoreceptor function. • 10 times more frequent in the people living
at higher altitudes.• Larger lesions cause cranial nerve palsy
(X & XII)

21
2. JUGULOTYMPANIC PARAGANGLIOMAS
• Also called GLOMUS TUMOR.• Female preponderance.
A. Glomus juglare: arise from the dome of juglar bulb.
B. Glomus Tympanicum: arise from the promontary of the middle ear.
• Spread to inner ear, juglar foramen causing cranial nerve palsy, eustachian tube, nasopharynx and intracranial.

• Present as a middle ear mass resulting in tinnitus (in 80%) and hearing loss (in 60%).
• On otoscopy, through intact tympanic membrane “Rising sun” appearance, when it originates from floor of middle ear.
• Pulsation sign (Brown’s Sign) is positive when ear canal pressure is raised with Siegle’s speculum, tumor pulsates vigorously and then blanches.
22

23
3. VAGAL PARAGANGLIOMA
• Least common of paragangliomas.• Located in the anterolateral portion of the
neck• Presents as painless neck mass or with
dysphagia and hoarsness of voice.• Can also occur along the peripheral
distribution of the vagus nerve.

24
4. MEDIASTINAL PARAGAGLIOMA
• Originate in supra-aortic/aorticopulmonary bodies (Chemodactomas)
• Found in the anteriosuperior portion of the mediastinum, in the area of aortic arch.
• Higher incidence of aggressive tumor growth.

25
5. RETROPERITONEAL PARAGANGLIOMA
• Anywhere along paravertebral chain.

26
6. ZUCKERKANDL BODY PARAGANGLIOMA
• Found close to angle formed by the anterior wall of aorta and the origin of the inferior mesenteric artery
• Orthosympathetic, chromaffin, catacholamine secreting.
• May secondarily involve inferior vena cava.

27
7. Other sites
• Cavernous sinus • Orbit• Nose• Paranasal cavities• Larynx • Trachea• Thyroid• Heart• Salivary glands
• Gall bladder• Urinary bladder• Uterus• Spinal chord (Lumbar
region, cauda equina, exceptionally keratin positive)
• Lung • Pineal gland

28
Familial Pheochromocytoma/ Paraganglioma
• Younger age at presentation• More often bilateral• Associations:
1. MEN-2A, MEN-2B (RET gene)
2. Neurofibromatosis (NF1 gene)
3. Von Hippel Lindau (VHL gene)
4. Familial paragangliomas (SDH gene related.)

29
SDH gene
• Four distinct syndromes – PGL 1 to 4 are related to mutations in the succinate dehydrogenase gene – mitochondrial complex involved in electron transfer and Krebs cycle.
• Although different SDH mutations occur in single multi-unit enzyme, they express significant phenotype heterogeneity. Their prevalence is estimated to lie between 10–30% of PGLs.

30
SDH A SDH B SDH C SDH D SDH 5
PGL Syndrome
Leigh PGL 4 PGL 3 PGL 1 PGL2
Inheritance AR AD AD Maternal AD
Malignancy risk
None high Low Low Low
Multifocal Disease
Frequent Frequent

31

32
Diagnosis
1. Clinical presentation
2. Histopathological, IHC, EM, histochemical techniques.
3. For chatecholamine secreting tumors• Biochemical testing • Localization of tumor by imaging

33
Biochemical testing
• Elevated plasma & urine levels of catecholamines and methylated metabolites, (metanephrines and vinyl mandelic acid)
• Can be measured using HPLC, ELISA, other immunoassays.
• A value more than two-three times the upper limit of normal, pheochromocytoma highly likely.
• Plasma tests are more sensitive and convenient compared to urine tests (with 24 hour urine sample) but latter are more commonly done.

34
• Pattern of catecholamines is helpful in localizing tumor as epinephrine is never increased in extra-adrenal pheochromocytoma.
• CLONIDINE SUPPRESSION TEST: Diagnostic test used in the past for a pheochromocytoma. Administer clonidine, a centrally-acting alpha-2 agonist used to treat high blood pressure. Clonidine mimics catecholamines in the brain, causing it to reduce the activity of the sympathetic nerves controlling the adrenal medulla. A healthy adrenal medulla will respond to the by reducing catecholamine production; the lack of a response is evidence of pheochromocytoma.

35
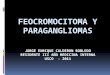
Diagnostic imaging
• CECT scan and MRI with gadolinium enhancement have equal sensitivity.
• I-123 metiodobenzylguanidine (MIBG) and F-dopa PET scan help localize, as these agents exhibit selective uptake in paragangliomas
Right (1) and left (2) glomus jugulare tumors; a left glomus vagale tumor (3); and left (4) and right (5) carotid body tumors.

36
Treatment
• The main treatment modalities are surgery (laparotomy or laparoscopy), tumor embolization and radiotherapy.
• Pre-surgical alpha receptor antagonist (Phenoxybenzamine) either alone or combined with a beta blocker administered to overcome the severe hypertension caused to massive release of catecholamines during manipulation of tumor.

PHEOCHROMOCYTOMA PARAGANGLIOMAS.
Originate from Adrenal medullary sympathetic
ganglia.
Originate usually from parasympathetic ganglia.
Chromaffin-positive. Chromaffin- negative.
Majority symptomatic. Majority asymptomatic. All have neurosecretory
granules, but only 1-3% secrete catecholamines.
10% malignant. 3% malignant.37

38
CASE- 3012/13(Reported by Dr. M.S. Bal)
• 53/ M, swelling right infra-auricular region- 8 years, painless, no other aural complaints, no hoarseness of voice, no loss of weight, no loss of appetite.
• Grossly, a circumscribed, grayish white are identified in the grayish brown STP measuring 6 X2.5 X1.5

39

40
CASE – 1616/13(Reported by Dr. Anil K. Suri)
• 50 year old female with complaints of pain abdomen since one month.
• On surgical exploration, a well circumscribed mass, found attached to the root of mesocolon, just above the superior mesenteric vessels.
• Grossly, a circumscribed globular STP measuring 9 cm.

41

42

43
References
• Rosai & Ackerman’s- Surgical Pathology (10Th ed.)
• Robbins and cotran- Pathological basis of disease. (8th ed.)
• P.L Dhingra ENT textbook.• Pubmed central (NCBI)

44
ACKNOWLEDGEMENT
Dr. Manjit Singh BalDr. Anil Suri

45