Embed Size (px)
DESCRIPTION
describes the pathophysiology and epidemiology of TBI based on Indian scenario...
Citation preview
Epidemiology &
Pathophysiology of
Head injuriesDr
Unnikrishnan P
1 EPIDEMIOLOGY OF TBI BASED ON INDIAN SCENARIO
PATHOPHYSIOLOGY OF TBI
CEREBRAL VASCULAR PHYSIOLOGY IN TBI
2
3
We will go through…
Definition
Traumatic brain injury is a non degenerative,
non congenital insult to the brain from an
external mechanical force ,possibly leading
to permanent or temporary impairment of
cognitive, physical and psychosocial
functions, with an associated diminished or
altered state of consciousness
Severity based on GCS
severe= 3-8
Moderate = 9-12
Mild = 13-15
We know all about others ;nothing about ourselves….!
At the global level, the annual incidence and mortality from Traumatic Brain Injuries (TBIs) is 200 and 20 per 1,00,000 per year, respectively
National level data in India is not available for traumatic brain injuries as in many developed countries.
• The only epidemiological study was undertaken in Bangalore by Dr Gururaj et al at NIMHANS during the period March 2000 to March 2003, over a period of three years
What it revealed about TBI IN INDIA….
the incidence, mortality and case fatality rates were 150/100000, 20/100000 and 10%, respectively
At the national level, nearly two million people sustain brain injuries, 0.2 million loose their lives and nearly one million need rehabilitation services every year.
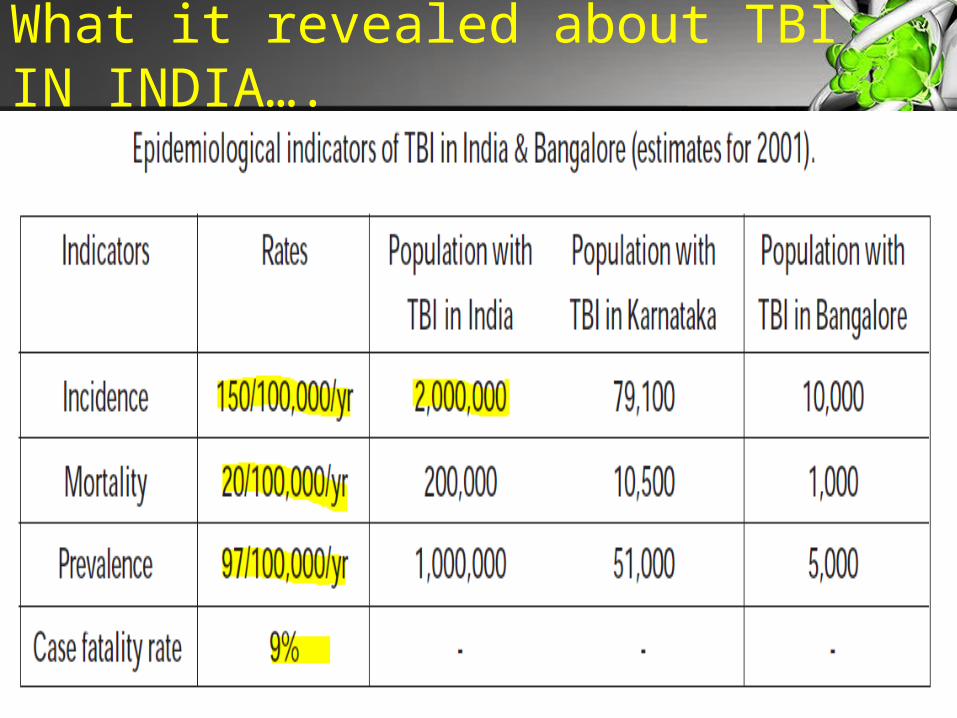
What it revealed about TBI IN INDIA….
.
What it revealed about TBI IN INDIA….
Nearly 10,000 people sustain brain injury every year in the city of Bangalore with more than 1,000 deaths.
20 - 25 patients are registered every day with a head injury at NIMHANS and TBIs constituted 39% of total registration during 2000
How they worked it out?
7,164 persons were enrolled into a Neurotrauma Registry during the year 2000 at NIMHANS.
While Phase–1 study focused on identifying and measuring all epidemiological correlates in a hospital setting,
phases–II and III focused on identifying disability patterns, extent of socio-economic burden & measuring quality of life
The scenario is likely to be similar for other Indian cities and in some of the other developing countries.
1
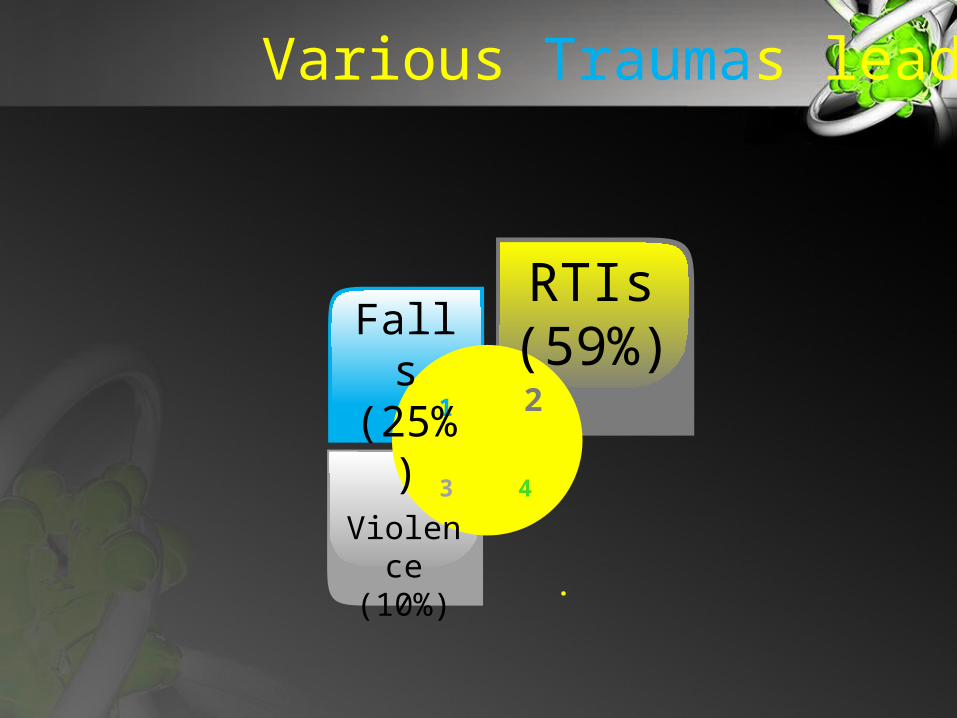
Falls (25%
)2
RTIs (59%)
3
Violence
(10%)
4
.
Various Traumas leading to Brain Injury
The social picture
• majority of these individuals are males, in their early years (5 - 44 years) [male to female ratio of 4:1]
Individuals in the age group of 21 - 35 years were represented to the extent of 40%
The majority of those injured were with less than collegiate levels of education
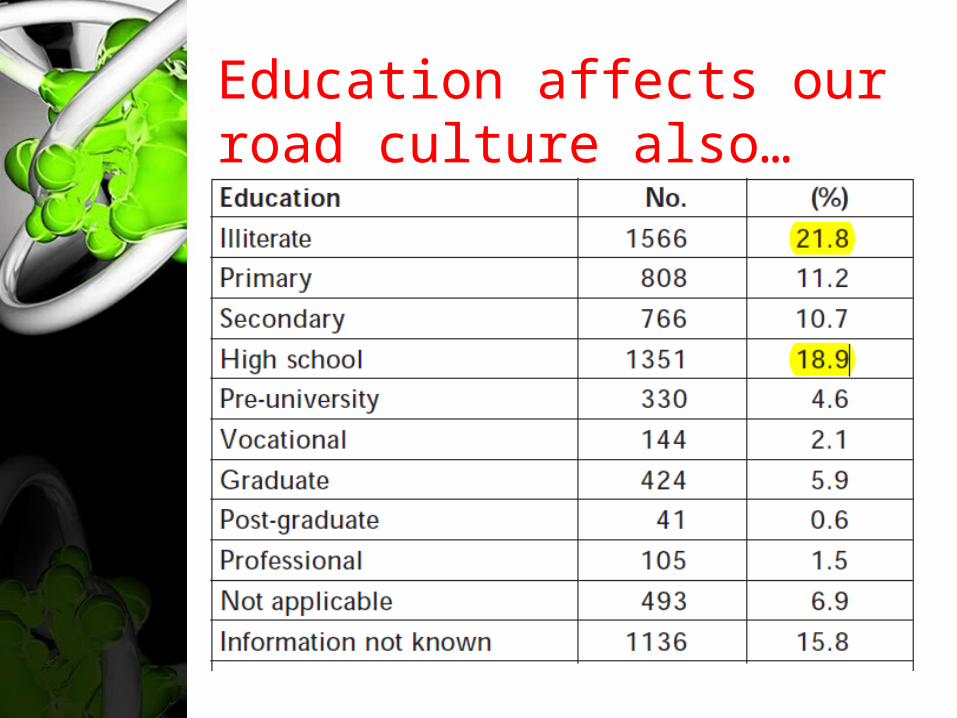
Education affects our road culture also…• ,
Road Traffic Injuries
RTIs occurred predominantly in the age group of 15 - 40 years, among men and during evenings and nights (66%).
Pedestrians (26%), two-wheeler riders (31%) and pillions (12%) and bicyclists (8%) were represented in higher numbers
The majority of the RTIs took place in midblocks of roads (70%).
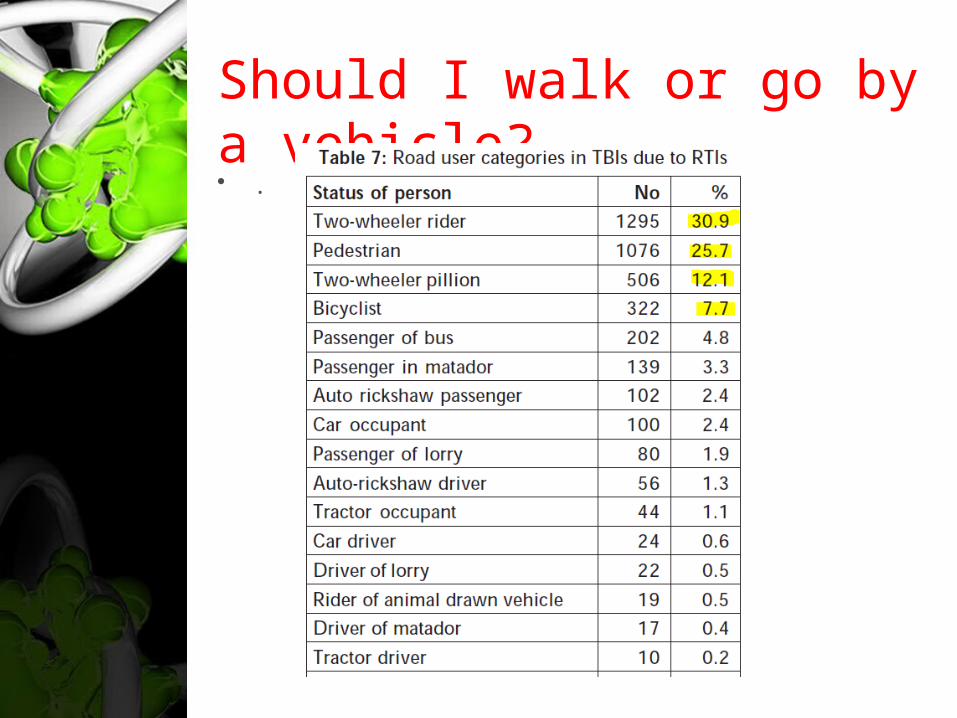
Should I walk or go by a vehicle?• .
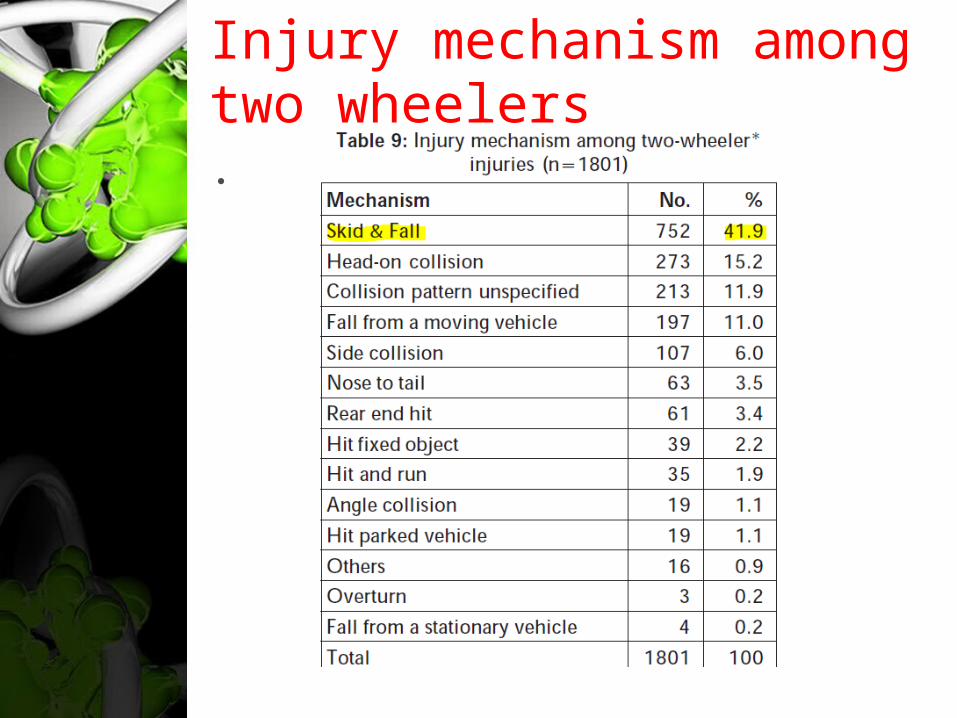
Injury mechanism among two wheelers• .
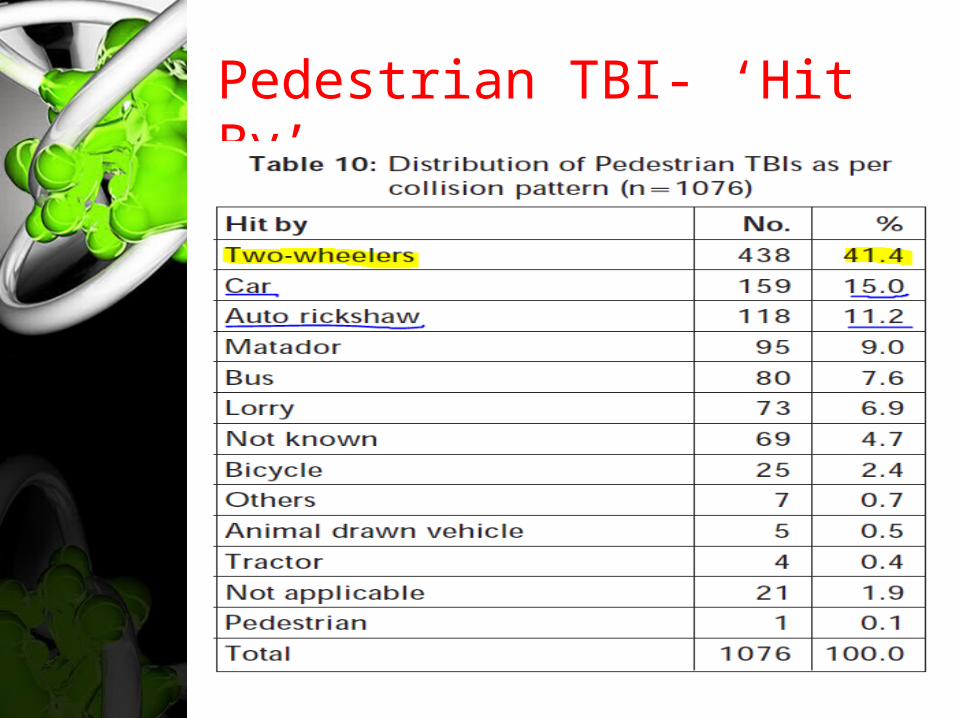
Pedestrian TBI- ‘Hit By’• .
Our genome always shows perfect inheritance of disobedience!
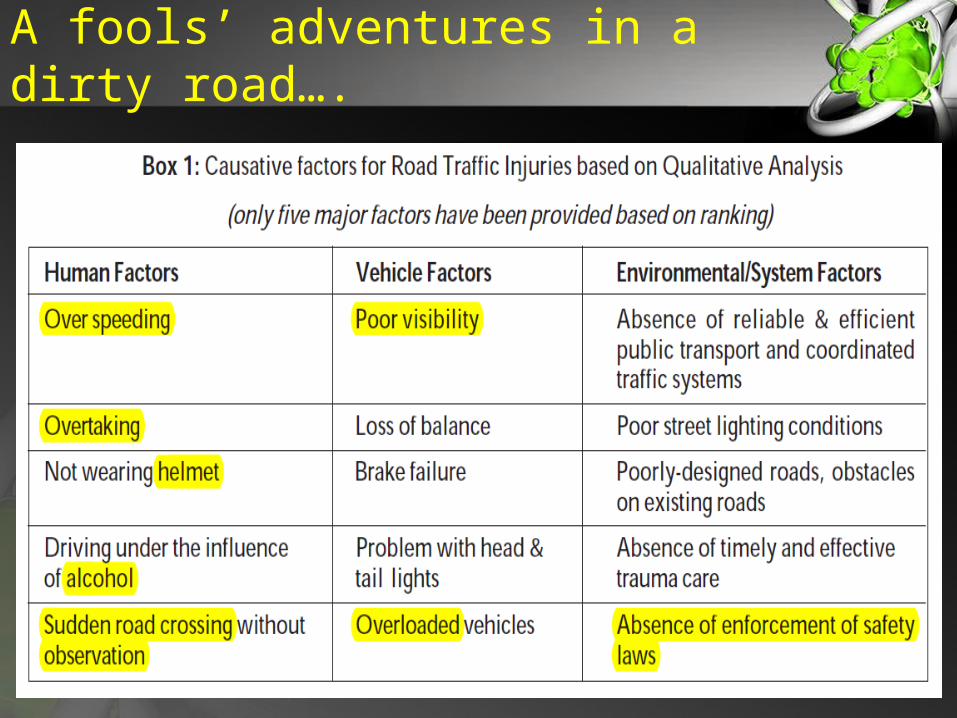
Not wearing helmets
driving under influence of alcohol
over speeding and overtaking
crossing in the middle of the road ……………………
were the major behavioural factors.
Remain indoor for a prosperous life!
Poor visibility of vehicles and or roads
mechanical problems of vehicles ……………….……
were responsible for one-third of injuries
Road design and structural issues ……………………..
were responsible for another 30% of TBIs.
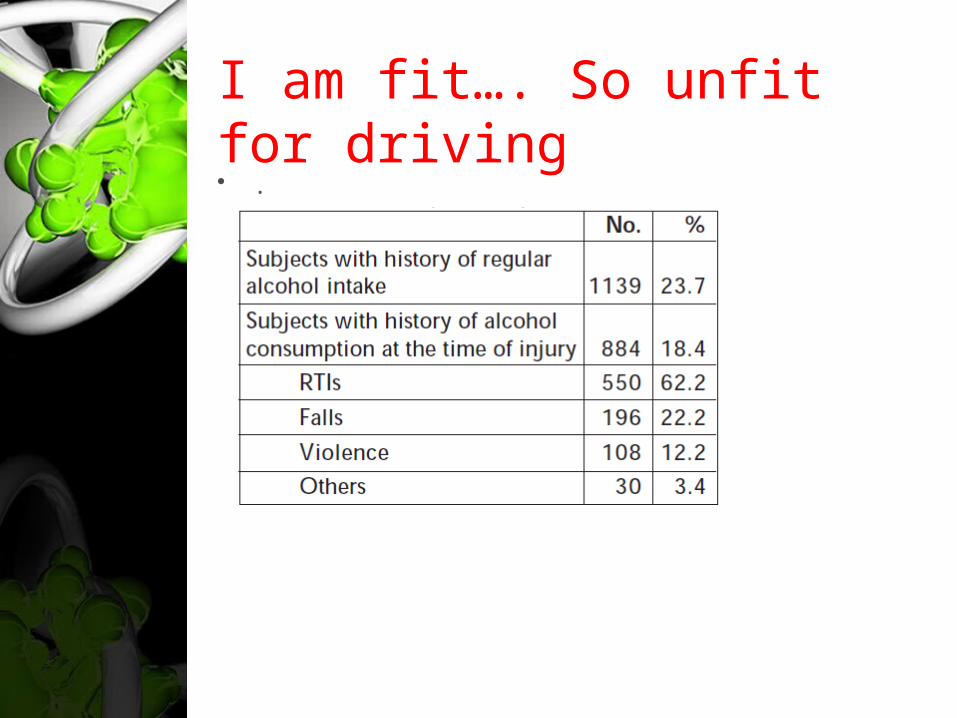
I am fit…. So unfit for driving• .
A fools’ adventures in a dirty road….
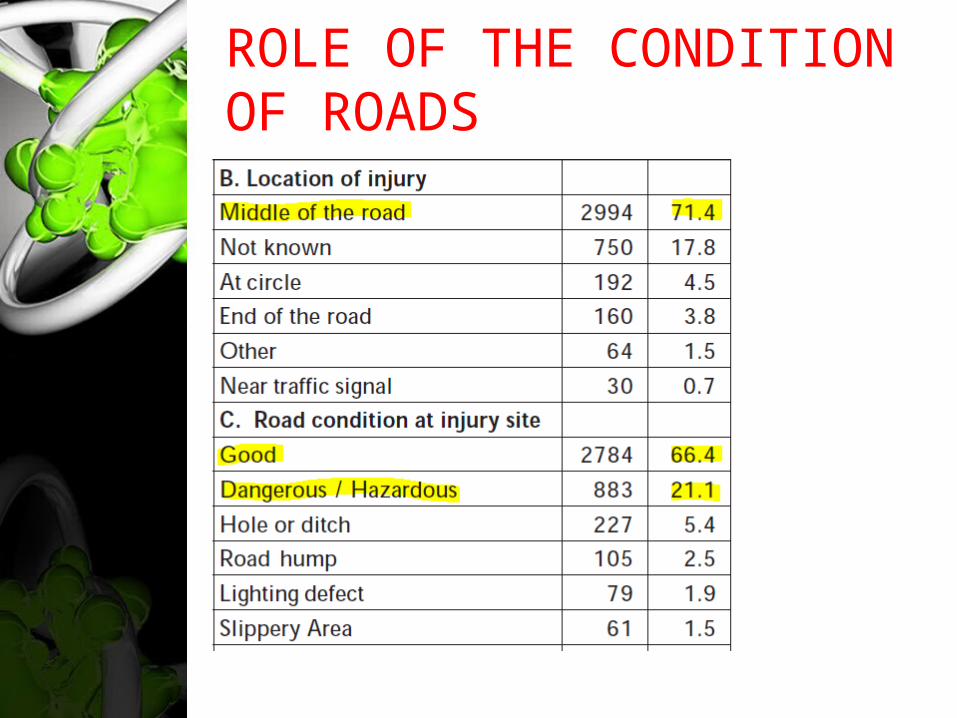
ROLE OF THE CONDITION OF ROADS• ,
Other causesFalls were the second-leading cause (25%), with the majority occurring in children and elderly.
Amongst them domestic falls (57%) were the leading cause followed by falls in public places (15%).
Violence/assault (10%) were the third-leading cause, more frequent among men and associated with use of blunt physical objects.
Prehospital and emergency care was poor in these areas:
availability of First Aid Services
high referrals from local hospitals
safer transportation
longer interval between injury and reaching definitive hospital (only 13% within one hour and 40% in one to three hours)
Severity and patterns
In total, 71% of TBIs were mild, 15% moderate and 13% severe in nature based on Glasgow Coma Scale.
Concussions (36%), contusion (32%), skull fractures (12%) and brain haemorrhages (13%) were the injury patterns.

Hospital stay
• .
We are just observers in many situations…
Severe polytrauma was noticed in 22% of total injuries.
5.5% died in hospital and 4% were discharged in a persistent vegetative state.
Severe and moderate disabilities were observed in 15% and 37%, respectively.
Various types of disabilities affecting activities of daily living, memory, communication, social interaction and ability to work were seen in 52% of the patients at hospital discharge time.
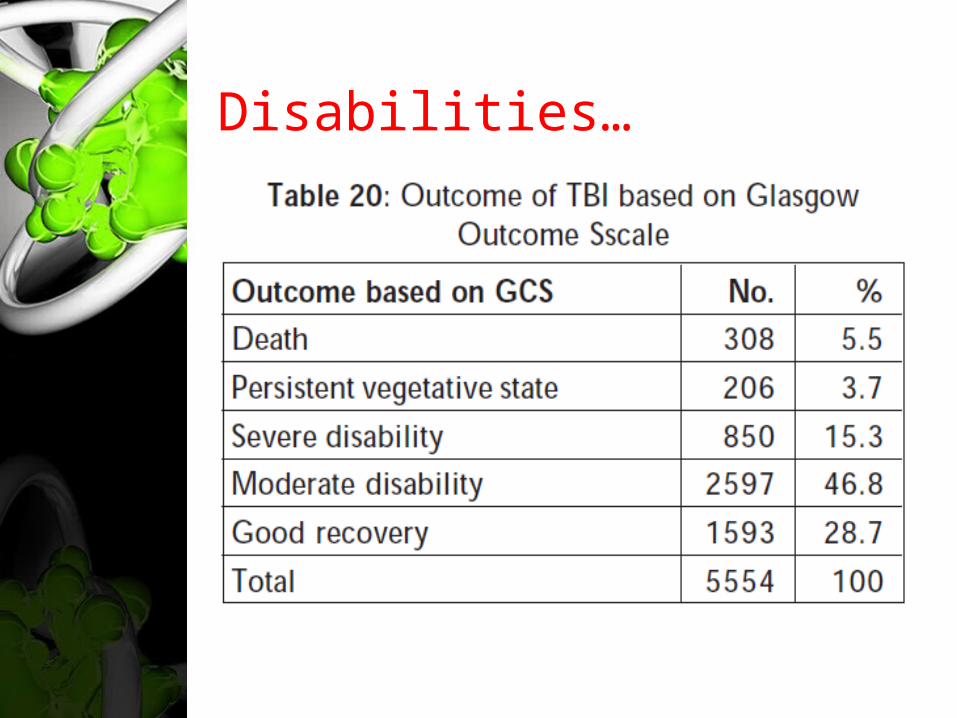
Disabilities…• .
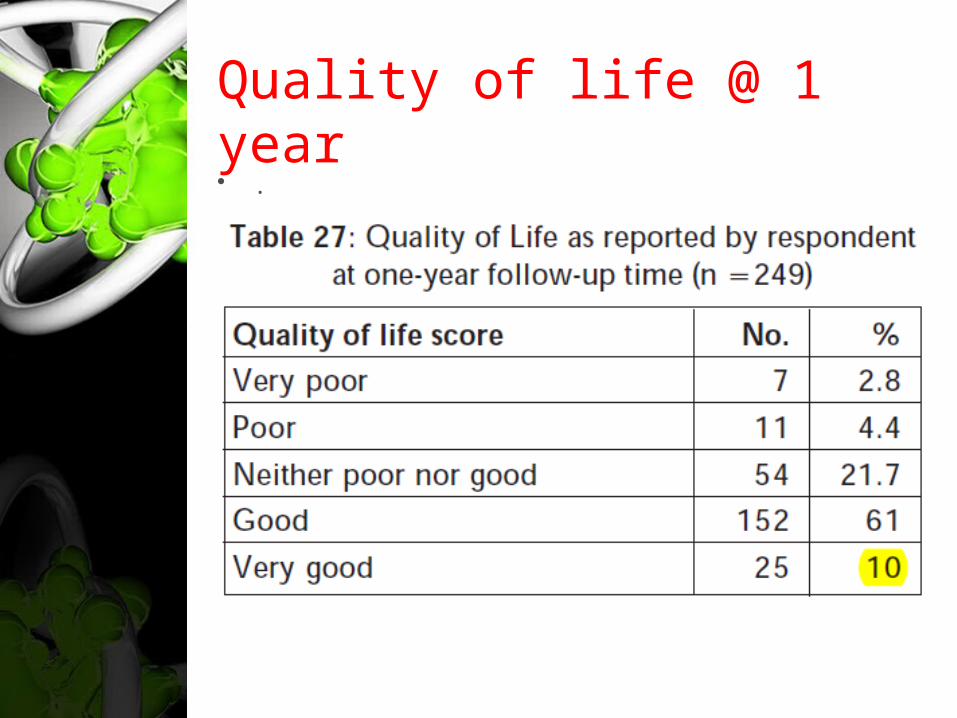
Quality of life @ 1 year• .
In 1 sec, life is turned upside down…
35% had problems in health, social, economic dimensions of life at 1-year follow-up
more than 50% of them continued to have problems in similar areas at second year follow up
The quality of life was poor in nearly 30% of brain-injured persons at two years post discharge.
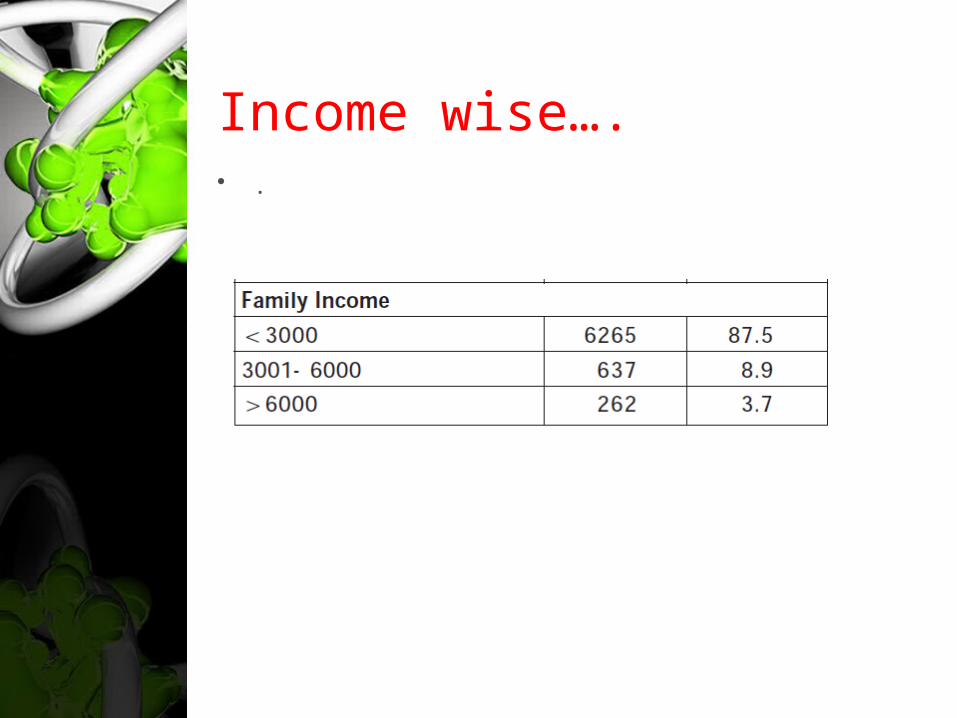
Income wise….• .
When we treat him/her for umpty no: of days, we should be aware of….
major economic burden on individuals and families to meet costs of hospitalization and rehabilitation
affected families had to spend resources [ their own or borrowed ] to reach definitive hospitals, to take care of injured person during hospital stay and after discharge.
The indirect costs due to loss of work and income are substantial
Foundation for gathering all these data is a……
a neurotrauma register
provides
detailed description of all individuals
sustaining a TBI
during a given period (beginning with a date)
in a defined population,
the major demographic features of which are
known and representative of the selected
population.
CRITERIA
• .The criteria of a neurotrauma registry are:-
1) Uniform definition
2) Inclusion of all subjects with a TBI in a defined area
3) Case identification from multiple sources
4) Case evaluation by a trained team
5) Consistency in diagnosis
6) Established classification methods.
HOW IT IS VITAL IN EPIDEMIOLOGY OF TBI
The registry can identify major causes, pattern and mode of injury occurrence in subcategories of injured persons, thus identifying "Population at risk”
It improves diagnostic accuracy as all subjects are weighed in comparison with gold standard.
Registry helps in in establishing cause-effect associations over a period of time (e.g.: Epilepsy and TBI's).
HOW IT IS VITAL IN EPIDEMIOLOGY OF TBI
The registry reveal vital data on morbidity, mortality and disability rates (Incidence,fatality and disability rates)
will reveal temporal changes in occurrence and pattern of neurotrauma
it can serve as a basic ground tool for clinical and intervention trials. It would highlight how much change has been brought about by an intervention
HOW IT IS VITAL IN EPIDEMIOLOGY OF TBI
helps in developing and understanding prognosis in neurotrauma management and in anticipating future risks.
reveal the socioeconomic burden and health needs of a community
this will help in creating awareness among policy makers and public to place neurotrauma prevention high on the public health agenda
brings out problems in diagnostic classification

.
PATHOPHYSIOLO
GY PRIMARY
INJURY
TBI
Traumatic brain injury (TBI) is the result of
an external mechanical force applied to the
cranium and the intracranial contents,
leading to temporary or permanent
impairments, functional disability, or
psychosocial maladjustment
Injuries are divided into 2 subcategories
(1) primary injury, which occurs at the
moment of trauma, and
(2) secondary injury, which occurs
immediately after trauma and produces
effects that may continue for a long time.
Primary injury- Physical mechanisms
Impact loading - Collision of the head with a solid object at a tangible speed [through a combination of contact forces and inertial forces]
Impulsive loading - Sudden motion without significant physical contact
Static or quasistatic loading :occurs when a slowly moving object traps the head against a fixed rigid structure and gradually squeezes the skull, causing many comminuted fractures and deforms the brain
3 basic types of tissue deformation
Compressive - Tissue compression
Tensile - Tissue stretching
Shear - Tissue distortion produced when
tissue slides over other tissue
Types of Primary Injuries
focal injuries (eg, skull fractures, intracranial
hematomas, lacerations, contusions,
penetrating wounds)
diffuse (as in diffuse axonal injury).
Skull fractures
vault fractures or basilar fractures.
stellate, closed, or open fractures
depressed or nondepressed
simple fracture and compound fracture
Vault fractures may extend into the sinuses
Basal skull fractures may be associated with
injuries to the cranial nerves and discharges
from the ear, nose, and throat.
Auditory/vestibular
dysfunctionconductive or sensorineural hearing loss.
Benign paroxysmal positional vertigo
Intracranial hemorrhages
Epidural hematoma
Subdural hematoma
Intracerebral hemorrhages
Intraventricular hemorrhage
Subarachnoid hemorrhage
Intracranial hemorrhages
Epidural hematoma
Subdural hematoma
Intracerebral hemorrhages
Intraventricular hemorrhage
Subarachnoid hemorrhage
Epidural hematoma
laceration of the dural arteries or veins, or by
diploic veins in the skull's marrow
a tear in the middle meningeal artery
when hematoma occurs from laceration of an
artery, blood collection can cause rapid
neurologic deterioration.
Intracerebral hemorrhages
Due to injury to larger, deeper cerebral
vessels occurring with extensive cortical
contusion.
Intraventricular hemorrhage tends to occur in
the presence of very severe TBI and is,
therefore, associated with an unfavorable
prognosis.
Subarachnoid hemorrhage
by lacerations of the superficial microvessels in
the subarachnoid space.
If not associated with another brain pathology,
this type of hemorrhage could be benign.
may lead to a communicating /
noncommunicating hydrocephalus if blood
products obstruct the arachnoid villi / the third
or fourth ventricle.
Coup and contrecoup
contusionsCoup contusions occur at the area of direct
impact to the skull
and occur because of the creation of negative
pressure
when the skull, distorted at the site of impact,
returns to its normal shape.
Coup and contrecoup
contusionsContrecoup contusions are are located
opposite the site of direct impact.
Cavitation in the brain, from negative pressure
due to translational acceleration impacts
as the skull and dura matter start to accelerate
before the brain on initial impact.
contusion is coup or contrecoup type?
impact from a small, hard object tends to
dissipate at the impact site, leading to a coup
contusion.
In contrast, impact from a larger object causes
less injury at the impact site, because energy
is dissipated at the beginning or end of the
head motion, leading to a contrecoup
contusion
Concussions
caused by deformity of the deep structures of
the brain
leading to widespread neurologic dysfunction
that can result in impaired consciousness or
coma
Concussion is considered a mild form of diffuse
axonal injury.
Diffuse axonal injury
characterized by extensive, generalized
damage to the white matter of the brain.
Strains of the tentorium and falx during high-
speed acceleration/deceleration produced by
lateral motions of the head may cause the
injuries.
also could occur as a result of ischemia
Neuropathologic findings in patients with diffuse axonal injury
Grade 1 - Axonal injury mainly in parasagittal
white matter of the cerebral hemispheres
Grade 2 - As in Grade 1, plus lesions in the
corpus callosum
Grade 3 - As in Grade 2, plus a focal lesion in
the cerebral peduncle
...........Gennarelli and colleagues
.
PATHOPHYSIOLO
GY
SECONDARY INJURY
Secondary injuries
Due to further cellular damage from the effects
of primary injuries.
develop over a period of hours or days
following the initial traumatic assault.
mediated through the following neurochemical
mediators..
Excitatory amino acids
glutamate and aspartate
influx of Cl,Na and Ca, leading to acute
neuronal swelling., vacuolization, and neuronal
death
↓high-energy phosphate stores or ↑ free radical
production...
cause astrocytic swellings via volume-
activated anion channels (VRACs). Tamoxifen is
a potent inhibitor of VRACs and potentially
could be of therapeutic value.
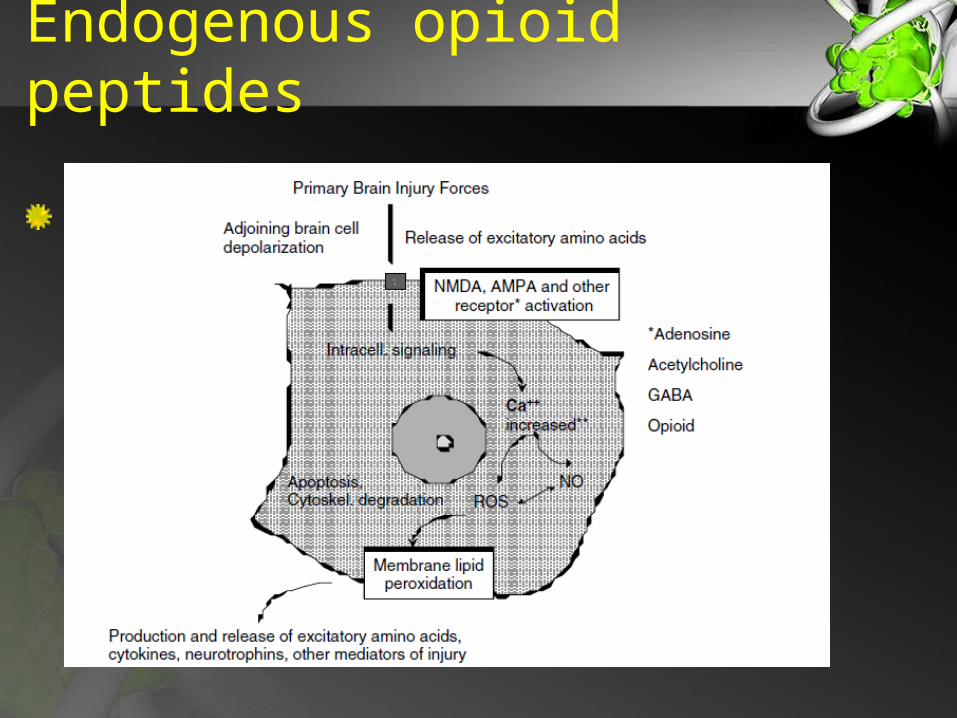
Endogenous opioid peptides
modulating the presynaptic release of EAA
neurotransmitters.
Heightened metabolism in the injured brain is
stimulated by
an increase in the circulating levels of
catecholamines
from TBI-induced stimulation of the
sympathoadrenomedullary axis and
serotonergic system
with associated depression in glucose
utilization, contributing to further brain injury.
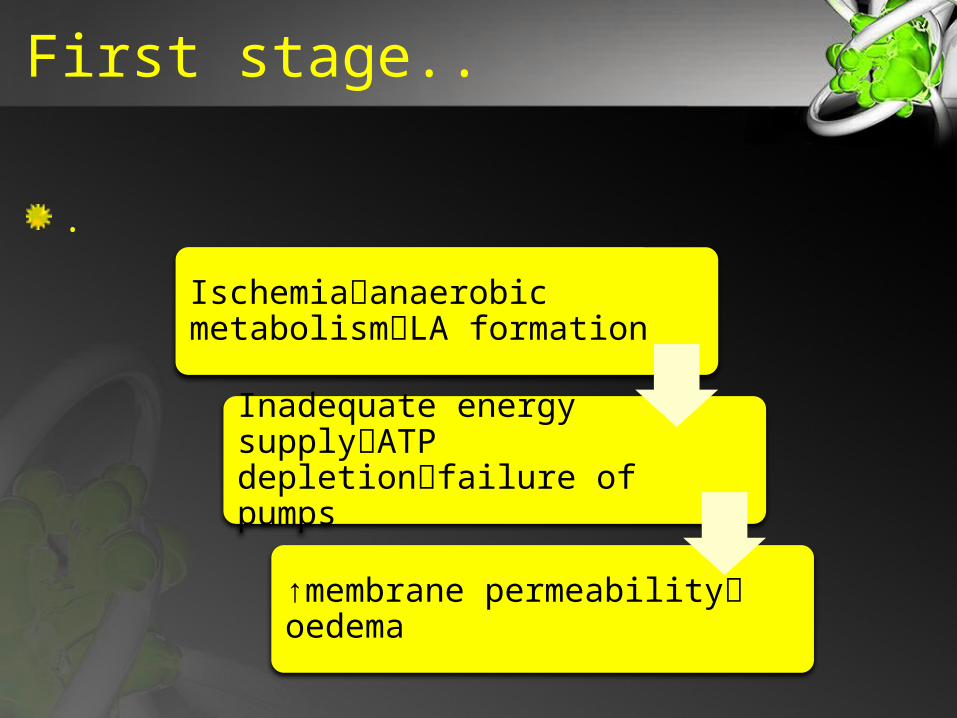
First stage..
.Ischemiaanaerobic metabolismLA formation
Inadequate energy supplyATP depletionfailure of pumps
↑membrane permeability oedema
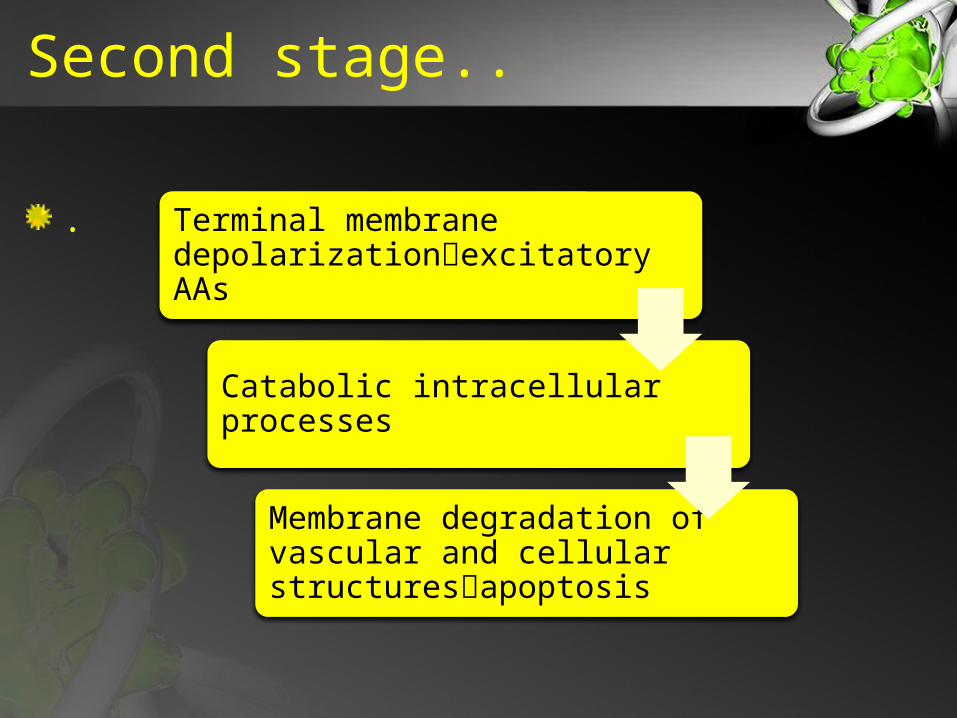
Second stage..
. Terminal membrane depolarizationexcitatory AAs
Catabolic intracellular processes
Membrane degradation of vascular and cellular structuresapoptosis
Oxidative stress
excessive production of reactive oxygen
species due to excitotoxicity and exhaustion of
the endogenous antioxidant system induces
peroxidation of cellular and vascular
structures.These mechanisms can cause....
immediate cell death
inflammatory processes and
induction of early or late apoptotic
programmes
Endogenous opioid peptides
.
Increased intracranial pressure
The severity increase due to heightened ICP
[esp if the pressure exceeds 40 mm Hg.]
also can lead to cerebral hypoxia, cerebral
ischemia, cerebral edema, hydrocephalus, and
brain herniation
Hydrocephalus
communicating type of hydrocephalus is more
common
The noncommunicating type of hydrocephalus
is often caused by blood clot obstruction of
blood flow at the interventricular foramen,
third ventricle, cerebral aqueduct, or fourth
ventricle.
Cerebral edema-contributors
neurochemical transmitters
increased ICP.
Disruption of the blood-brain barrier
impairment of vasomotor autoregulation
leading to dilatation of cerebral blood vessels
Brain herniation
Supratentorial herniation is attributable to
direct mechanical compression by an
accumulating mass or to increased intracranial
pressure.
Types :
Subfalcine herniation
The cingulate gyrus of the frontal lobe is
pushed beneath the falx cerebri when an
expanding mass lesion causes a medial shift of
the ipsilateral hemisphere.
This is the most common type of herniation.
Central transtentorial herniation
characterized by the displacement of the basal
nuclei and cerebral hemispheres downward
while the diencephalon and adjacent midbrain
are pushed through the tentorial notch.
Cerebellar herniation
involves the displacement of the medial edge
of the uncus and the hippocampal gyrus
medially and over the ipsilateral edge of the
tentorium cerebelli foramen, causing
compression of the midbrain; the ipsilateral or
contralateral third nerve may be stretched or
compressed.
Cerebellar herniation
This injury is marked by an infratentorial
herniation in which the tonsil of the cerebellum
is pushed through the foramen magnum and
compresses the medulla, leading to
bradycardia and respiratory arrest.
Cerebellar herniation
.
.
CEREBROVASCULAR
PHYSIOLOGY AFTER
TBI
Altered Cerebral Blood Flow and Metabolism
can cause flow-metabolism uncoupling,
resulting in cerebral ischemia or cerebral
hyperemia;
Hyperemia is as bad as ischemia
[vasoparalysis↑CBV ↑ICP]show 3 phases
FIRST[6-12 HRS]: brain may suffer poor perfusion and cerebral ischemia
SECOND phase of hyperemia[CBF>55ml/100g/min]: With luxury perfusion & ↑ ICP
THIRD: vasospasm and poor perfusion
Altered Cerebral Blood Flow and Metabolism
Focal/global ischemia occurs frequently & is a
a major causative factor for poor outcome
the critical threshold of CBF for the
development of irreversible tissue damage is
15 ml 100 g21 min21 in patients with TBI
How TBI causes ischemia?
Morphological injury (e.g. vessel distortion)
hypotension in the presence of autoregulatory
failure
inadequate availability of nitric oxide or
cholinergic neurotransmitters
potentiation of prostaglandin-induced
vasoconstriction
Altered CO2 Vasoreactivity
During the early period, CO2 vasoreactivity
can be transiently impaired, but generally
recovers after 4 to 7 days
may be associated with cerebral hyperemia,
cerebral ischemia, or intracranial hypertension
CO2 vasoreactivity is less in patients with
lower baseline CBF
Altered CO2 Vasoreactivity
Cerebrovascular CO2-reactivity seems to be a
more robust phenomenon.
It is in patients with severe brain injury and
poor outcome, where CO2-reactivity is found to
be impaired in the early stages ; it was intact
in most other patients with lesser insults
Altered CO2 Vasoreactivity
hyperventilation to induce cerebral
vasoconstriction and reduce CBF, ICP and
cerebral blood volume may unintentionally
lead to secondary ischemic damage after TBI
hyperventilation may not be effective in TBI if
CO2 vasoreactivity is decreased.
Altered CO2 Vasoreactivity
hyperventilation to induce cerebral
vasoconstriction and reduce CBF, ICP and
cerebral blood volume may unintentionally
lead to secondary ischemic damage after TBI
hyperventilation may not be effective in TBI if
CO2 vasoreactivity is decreased.
Impaired Cerebral Pressure Autoregulation
incidence is 28% after moderate and 67%
after severe TBI
a recent study of severe pediatric TBI reported
that cerebral autoregulation often changed
and worsened during the first 9 days after
injury
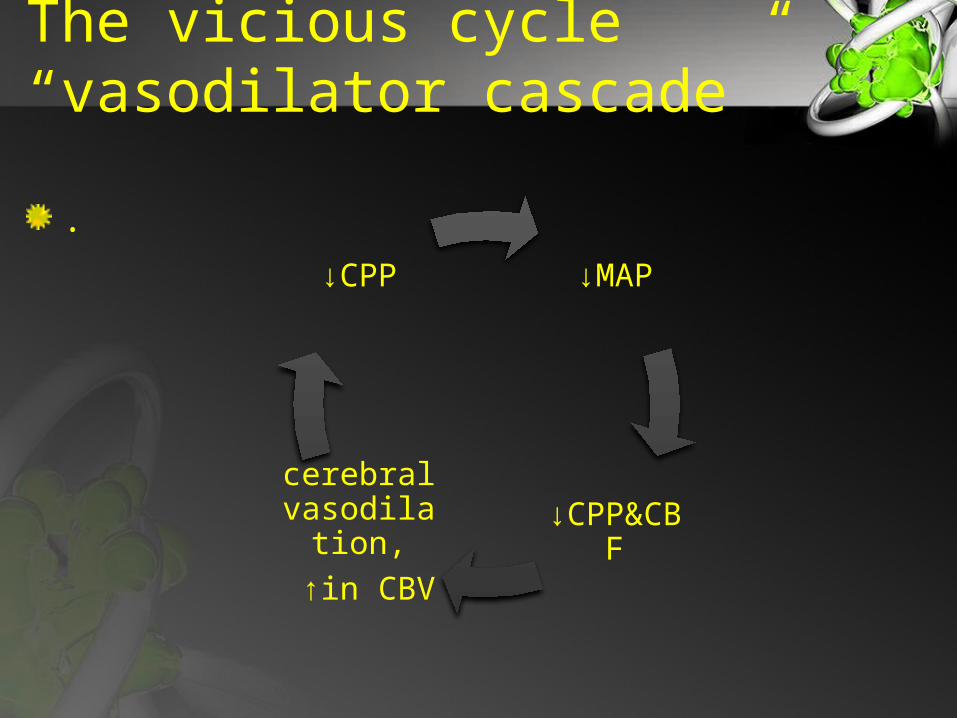
The vicious cycle “vasodilator cascade”
.
↓MAP
↓CPP&CBF
cerebral vasodilati
on, ↑in CBV
↓CPP
Impaired Cerebral Pressure Autoregulation
autoregulatory vasoconstriction seems to be
more resistant compared with autoregulatory
vasodilation
indicates that patients are more sensitive to
damage from low rather than high CPPs.16
Secondary Insults and Injuries
Secondary insults, include systemic causes
such as hypotension, hypocarbia, hypercarbia,
hypoxia, hyperthermia, and hyperglycemia
result in secondary injuries
Cerebral vasospasm
occurs in more than one-third of patients with
TBI and indicates severe damage to the brain.• onset varies from post-traumatic day 2 to 15
and hypoperfusion• (haemodynamically significant vasospasm)
occurs• in 50% of all patients developing vasospasm
The mechanisms behindCerebral vasospasm
chronic depolarization of vascular smooth
muscle due to reduced potassium channel
activity
release of endothelin along with reduced
availability of nitric oxide
cyclic GMP depletion of vascular smooth
muscle potentiation of prostaglandin-induced
vasoconstriction
free radical formation.
Cerebral metabolic dysfunction
Cerebral metabolism and cerebral energy state
are frequently reduced after TBI
outcome is worse in patients with lower metabolic rates compared with those with minor or no metabolic dysfunction.
Mechanisms-metabolic dysfunction
mitochondrial dysfunction with
reduced respiratory rates and ATP-production
a reduced availability of the nicotinic co-
enzyme pool
intramitochondrial Ca2-overload ……
may not be associated with matching
decreases in CBF.
reflects uncoupling of CBF and metabolism,
probably due to increased adenosine availability
Cerebral oxygenation
imbalance between cerebral oxygen delivery
and cerebral oxygen consumption leading to
brain tissue hypoxia.
have identified the critical threshold of brain
tissue oxygen pressure in patients suffering
from TBI 15–10 mm Hg PtO2 below which
infarction of neuronal tissue occurs.
oxygen deprivation of the brain with
consecutive secondary brain damage may
occur even in the presence of normal CPP or
ICP
Oedema - vasogenic
caused by breakdown of the endothelial cell
layer of brain vessels
allows for uncontrolled ion and protein transfer
from the intravascular to the extracellular
(interstitial) brain compartments
Anatomically, this pathology increases the
volume of the extracellular space
Oedema - vasogenic
caused by breakdown of the endothelial cell
layer of brain vessels
allows for uncontrolled ion and protein transfer
from the intravascular to the extracellular
(interstitial) brain compartments
Anatomically, this pathology increases the
volume of the extracellular space
Oedema - Cytotoxic
• Caused by intracellular water accumulation
due to an increased cell membrane
permeability for ions, ionic pump failure due to
energy depletion, and cellular reabsorption of
osmotically active solutes
• irrespective of the integrity of the vascular
endothelial wall.
• more frequent than vasogenic oedema in TBI
Inflammation
Both primary and secondary insults activate
the release of cellular mediators including
proinflammatory cytokines, prostaglandins,
free radicals, and complement induce
chemokines and adhesion molecules and in
turn mobilize immune and glial cells
injured and adjacent tissue is replaced
astrocytes produce microfilaments and
neutropines ultimately to synthesize scar
tissue
Inflammation
The additional release of vasoconstrictors
(prostaglandins and leucotrienes)• the obliteration of microvasculature through
adhesion of leucocytes and platelets, • the blood–brain barrier lesion, • and the oedema formation • further reduce tissue perfusion and
consequently aggravate secondary brain damage
Necrosis vs apoptosis
Two different types of cell death may occur
after TBI
Necrosis occurs in response to severe
mechanical or ischaemic/hypoxic tissue
damage
neurons undergoing apoptosis are
morphologically intact
The clinical relevance of apoptosis relates to
the delayed onset of cellular deterioration,
potentially offering a more realistic window of
opportunity for therapeutic (anti-apoptotic)
interventions
Outcome of the last hour should be…..
Understanding the multidimensional cascade of
injury offers therapeutic options including the
management
of CPP, mechanical (hyper-) ventilation, kinetic
therapy to improve oxygenation and to reduce
ICP, and pharmacological intervention to
reduce excitotoxicity and ICP

THANK YOU