Embed Size (px)
Citation preview

Interventional Radiology
Aaron Shiloh MD FSIRSection Chief
Interventional Radiology
A Primer on Minimally Invasive
Image Guided Therapies

Overview• Paracentesis• Thoracentisis• PICC Line• Can this be biopsied?

Overview• Basics of liver directed
therapy• Embolization• PE lysis• Arterial disease and CVI

Liver Directed Therapy
Local
• RFA
• Microwave
• Cryoablation
Regional
• Chemoembolization
• Drug-Eluting Bead embolization
• Y90 (Glass and Resin) Beads

Interventional Oncology
Local Treatment Options Microwave Ablation

Microwave Ablation (MWA)
MWA – “the application of high frequency electric currents to heat and coagulate
target tissue”

MWA – A Variety of Applications
Liver Kidney Bone Lung

MWA Pathology
Hyperemic Rim
Coagulation zone(= MWA lesion)

MWA AblationNSC Lung Cancer
3 cm MWA 3 mo S/P MWA/XRT
18 mo S/P MWA/XRT

Post MWAPre MWA
MWA Images Pre & Post CT

65 year old male with recurrent liver mets from CRC
after multiple cycles of chemo

Colorectal Metastatic Disease
Two PET positive lesions
Immediate post microwave ablation
6 month follow-up

84 yo malewith
multipleMedical
problems And a
growing RCC

Summary of MWA Advantages
Preserves liver function in cirrhotic patients Minimally invasive
Local effect Potential for improved quality of life when
combined with radiotherapy and chemotherapy Repeatable for recurring disease

Interventional Oncology
Regional Therapeutic Options

Interventional Oncology
Chemoembolization&
Bland Embolization

Chemoembolization & Bland Embolization
HCC Metastases
Neuroendocrine Colorectal Breast Melanoma RCC

TheraSphere®
HCC one of most common forms of cancer worldwide (est. 1 million new cases annually) In US, NCI estimate 19,160 new cases and 16,780
deaths in 20071
Incidence increasing with rise in hepatitis C-induced cirrhosis
5-10% of HCC patients are resectable2 1 National Cancer Institute www.cancer.gov (accessed December 1, 2008)2 Llovet, JM. Current Treatment Options for Gastroenterology. 2004;7:431-441
HCC Epidemiology

HCC: Difficult to Treat, Few Effective Treatment Options
Tenuous liver functions (cirrhosis, hepatitis)
Spontaneous decompensation Resistant to standard chemotherapy and
low dose radiation Responsive to high dose radiation
TheraSphere®
HCC Epidemiology

Limited Treatment Options for HCC
Therapeutic Options: Resection or transplantation
Unresectable HCC treatment options: Radiofrequency ablation Transarterial chemoembolization (TACE or Drug
Eluting Beads) Transarterial TheraSphere, Y90 Glass Microspheres External Beam radiation Systemic therapy (ie. Sorafenib) No treatment
TheraSphere®

What is TheraSphere®
20-30 µm glass microspheres Y-90 is an integral constituent of the glass
matrix Innovative treatment to deliver powerful, targeted
radiation inside the liver
Y-90 glass microspheres comparison to human hairTheraSphere dose vial

Administered via hepatic artery catheter
Targeted internal radiation due to tumor hypervascularity
Microspheres are trapped in the tumor arterioles and are minimally-embolic (microembolization)
Pure beta-emitter Average beta emission energy is
0.9367 MeV Average penetration range in
tissue is 2.5 mm Physical half-life is 64.2 hours and
decays to stable zirconium-90
TheraSphere®
Mechanism of Action


• 52 year old male with alcoholic hepatitis with ascites and pleural effusions.
• Cirrhosis lead to CT and MRI
• PMH: Ascites, Pleural effusions, right nephrectomy
• ECOG 0, CP A
• 3 cm Tumor seen in right lobe, segment 7
• AFP not elevated

June 2010

July 2010

Mapping August 2010

Therasphere administration

Sept 2010 – One month post treatment

Jan 2014

2010-2014

Embolization Tools
• Coils• Gelfoam• Alcohol• Particles• Glue

• 42 y/o obese female with Right 3 cm AML treated 8 yrs prior with
embolization at another institution when the AML was alledgedly 7 cm
and spontaneously bled.






Bronchial Artery
The patient presented with hemoptysis and a known right
perihilar lung cancer. The patient had been previously brought to the
operating room where an endotracheal tube was placed as
well as a bronchial blocker





GDA• Duodenal ulcer oversewn 10 days prior• Repeat severe upper gi bleeding• At endoscopy found to have a large visible
vessel that was bleeding and three clips were placed.



Embolization
Uterine Fibroid Embolization

Procedure Small incision
in skin
Uterine Fibroid Embolization
– Catheter inserted into femoral artery
Femoral Artery

Procedure
Uterine Fibroid Embolization
– Dye is injected
– Blood no longer reaches fibroids
UterineArtery
– Catheter is steered to uterine artery
– Small inert particles “emboli” are injected– Branches of uterine
artery are blocked
– Fibroids shrink over time

Procedure








PE and DVT lysis
• Basics of PE and DVT lysis

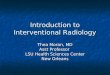
Massive PE Submassive PE Minor/Nonmassive PEHigh risk Moderate/intermediate risk Low risk
•Sustained hypotension (systolic BP <90 mmHg for ≥15 min)
• Inotropic support•Pulseless•Persistent profound bradycardia (HR <40 bpm with signs or symptoms of shock)
•Systemically normotensive (systolic BP ≥90 mmHg)
•RV dysfunction•Myocardial necrosis
•Systemically normotensive (systolic BP ≥90 mmHg)
•No RV dysfunction•No myocardial necrosis
RV dysfunction• RV/LV ratio > 0.9 or RV systolic dysfunction on echo• RV/LV ratio > 0.9 on CT• Elevation of BNP (>90 pg/mL)• Elevation of NTpro-BNP (>500 pg/mL)• ECG changes: • new complete or incomplete RBBB• anteroseptal ST elevation or depression• anteroseptal T-wave inversion
Jaff et al. Circulation 2011;123(16):1788-1830.
LVRV
Jaff et al. Circulation 2011;123(16):1788-1830.
Background and Definitions

− Registry of 1,416 patients
− Mortality rate: 1.9% if RV/LV ratio < 0.96.6% if RV/LV ratio ≥ 0.9
Fremont et al. CHEST 2008;133:358-362
How to Determine Risk

Degree of PE Treatment* Bleeding Risk
Non-Massive Heparin (I) Less
Sub-Massive Lytics (IIb)
Massive Lytics (IIa) More
20% risk of major bleeding3% risk of intracranial hemorrhage
*ACC/AHA Guidelines 2011 Circulation 2006;113:577-82
Treatment of High Risk Patients



The ULTIMA Trial
A Prospective, Randomized, Controlled Study of Ultrasound Accelerated Thrombolysis for the Treatment of Acute Pulmonary Embolism
Annual Meeting of the American College of Cardiology, March 9, 2013
Treatment of High Risk Patients

Systemic Lytics v Heparin
EKOS v Heparin
Total Lytics Dose 100mg 20.7mg (12.2mg)
Mortality 5.9% -> 4.3% 1/29 -> 0/30
RV Size Improved Improved
RV Function Improved Improved
Major Bleeding 20% 0/30
ICH 3% 0/30


Arterial DiseaseOne patient, many techniques













Chronic Venous Insufficiency


Epidemiology: Prevalence
Of the over 30 million Americansaffected:• Only 1.9 million seek treatment
annually1,2
• While the vast majority remain undiagnosed and untreated
CVI Prevalence*,1,2
30,000,000+
Seek Treatment *2 1,900,000
Treated447,0002 (Table 30)
*Statistics based on individuals over the age of 40
More than 30 million Americans suffer from varicose veins or a more seriousform of venous disease called Chronic Venous Insufficiency (CVI).1
1. Gloviczki P, et al. The care of patients with varicose veins and associated chronic diseases: clinical practice guidelines of the Society for Vascular Surgery and the American Venous Forum. JVS; May 2011.2. Lee, A. US markets for varicose vein treatment devices 2011. Millennium Research Group, Inc. (A Decision Resource, Inc. Company), www.mrg.net, May 2011.

Epidemiology: Risk FactorsMany factors contribute to the presence of venousdisease and CVI including1,2,3,4,5:
• Gender
• Age
• Family history
• Multiple pregnancy
• Standing occupation
• Obesity
• Prior injury or surgery
1. "Chronic Venous Insufficiency." Vascular Web. Society For Vascular Surgery, Jan. 2011. Web. 17 Aug. 2011. http://www.vascularweb.org/vascularhealth/Pages/chronic-venous-insufficiency.aspx. 2. Maurins U, Hoffmann BH, Lösch C, Jöckel KH, Rabe E, Pannier F. Distribution and prevalence of reflux in the superficial and deep venous system—results from the Bonn vein study, Germany. J Vasc Surg.2008;48:680-87.3. Criqui MH et al. Epidemiology of chronic peripheral venous disease; JJ Bergan Editor, The Vein Book, Elsevier Academic Press .(2007):30.4. Chiesa R, Marone EM, Limoni C, Volonte M, Schaefer E, Petrini O. Chronic venous insufficiency in Italy: the 24-cities cohort study. Eur J Vasc Endovasc Surg. 2005;30:422-429.5. Rabe E, Pannier F. Epidemiology of chronic venous disorders; P. Glovicki, Editor, Handbook of venous disorders (3rd edition), Hodder Arnold.(2009);109.

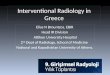
Anatomy: Venous System
• Venous blood flows from the capillaries to the heart
• Flow occurs against gravity– Muscular compression of the
veins – Negative intrathoracic pressure– Calf muscle pump
• Low flow, low pressure system

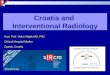
Etiology & Pathophysiology
Healthy veins, with competent vein valves, keep blood moving in one direction back to the heart
Diseased veins, with damaged vein valves, cause blood to move in both directions, elevating venous pressure

Single puncture percutaneous access under ultrasound guidance
Temperature controlled 85°C heating at or below deep fascia
Endovenous ablation specifically indicated to treat incompetent perforator veins
The Venefit™ Procedure with the ClosureRFS™Stylet

The Venefit™ Procedure with the ClosureRFS™Stylet
• Ultrasound exam to diagnose vein reflux
• Outpatient or hospital procedure
• Local or general anesthetic
• Quick return to normal activities – often within a few days1
Click graphic to play video
1. Roth S, Endovenous radiofrequency ablation of superficial and perforator veins, Surg Clin N Am 87:1267-1284(2007)
*Indications, contraindications, warnings, and instructions for use can be found in the product labeling supplied with each device.CAUTION: Federal (USA) restricts this device to sale by or on order of a physician.




So I was working on this grand rounds talk. I was reviewing old presentations and I came upon this case presentation from 2013.

Case Presentation• 84 year old female with chronic autoimmune
hepatitis
• LFTs elevation lead to CT
• PMH: Atrial Fibrillation, Hypertension, hypothyroidism
• ECOG 0, CP A
• T. Bili 0.8, cr 0.8, AFP 3320




2016


Thank you!