Embed Size (px)
DESCRIPTION
Citation preview

J. Clin. Endocrinol. Metab. 2003 88: 4440-4445, doi: 10.1210/jc.2002-021690
Catharina Larsson and Jan Zedenius Trisha Dwight, Srinivasan R. Thoppe, Theodoros Foukakis, Weng O. Lui, Göran Wallin, Anders Höög, Tony Frisk,
Rearrangement in Follicular Thyroid Tumors
Involvement of the PAX8/Peroxisome Proliferator-Activated Receptor {gamma}
Society please go to: http://jcem.endojournals.org//subscriptions/ or any of the other journals published by The EndocrineJournal of Clinical Endocrinology & Metabolism To subscribe to
Copyright © The Endocrine Society. All rights reserved. Print ISSN: 0021-972X. Online

Involvement of the PAX8/Peroxisome Proliferator-Activated Receptor � Rearrangement in FollicularThyroid Tumors
TRISHA DWIGHT, SRINIVASAN R. THOPPE, THEODOROS FOUKAKIS, WENG O. LUI,GORAN WALLIN, ANDERS HOOG, TONY FRISK, CATHARINA LARSSON, AND JAN ZEDENIUS
Endocrine Tumor Unit (T.D., S.R.T., T.Fo., W.O.L., T.Fr., C.L.), Department of Molecular Medicine, Karolinska HospitalCMM L8:01, Stockholm, SE-171 76 Sweden; Centre for Metabolism and Endocrinology (T.D., T.Fo., T.Fr., J.Z.), Departmentof Surgery, Karolinska Institutet at Huddinge University Hospital, Stockholm, SE-141 86 Sweden; Department of Surgery(T.Fo., G.W., T.Fr.), Karolinska Hospital P9:03, Stockholm, SE-171 76 Sweden; and Department of Oncology and Pathology(A.H.), Karolinska Hospital P1:02, Stockholm, SE-171 76 Sweden
Recently, a translocation t(2; 3)(q13;p25), involving the fusionof PAX8 and peroxisome proliferator-activated receptor �(PPAR�) was suggested to arise only in follicular thyroid car-cinomas. In this study, a group of 87 thyroid tumors wereanalyzed to determine the involvement of the PAX8/PPAR�fusion gene in these tumors, and also to determine whetherthis rearrangement can be used as a diagnostic marker for thedifferentiation between follicular thyroid carcinoma and ad-enoma. The PAX8/PPAR� rearrangement was detected by RT-PCR, fluorescence in situ hybridization, and/or Western anal-ysis in 10 of 34 (29%) follicular thyroid carcinomas and in oneof 20 (5%) atypical follicular thyroid adenomas, but not in anyof the 20 follicular thyroid adenomas or 13 anaplastic thyroid
carcinomas studied. In addition, seven of the 87 thyroid tu-mors exhibited involvement of PPAR� alone. Our findingssuggest that PAX8/PPAR� occurs frequently in follicular thy-roid carcinomas, and the presence of this rearrangement islikely to prove highly suggestive of a malignant tumor. Lackof the PAX8/PPAR� rearrangement in the anaplastic thyroidcarcinoma group suggests that the tumorigenic pathway inthese tumors is likely to be independent of this fusion. Fur-thermore, the results suggest that other rearrangements, in-volving PPAR� and other unidentified genes, may be involvedin follicular thyroid tumorigenesis. (J Clin Endocrinol Metab88: 4440–4445, 2003)
FOLLICULAR THYROID CARCINOMA (FTC) accountsfor 10–20% of all thyroid malignancies and normally
arises sporadically in the fifth to sixth decades of life (1).Although the use of fine needle aspiration biopsies has beenof great benefit in the preoperative diagnosis of other thyroidmalignancies, such as papillary and medullary thyroid car-cinoma, it has proved to be of limited use for the differen-tiation of FTC and follicular thyroid adenoma (FTA) (2).Diagnosis of follicular thyroid malignancy is based on thepresence of capsular or vascular invasion (3), which can onlybe assessed by histopathological examination of the surgi-cally removed specimen. Hence, although FTA arises muchmore frequently than FTC (2), most individuals diagnosedwith follicular thyroid neoplasia undergo surgery. The pre-operative differentiation between FTA and FTC is thereforeof great importance in the clinical setting.
Translocations or inversions can give rise to the activationof an oncogene through its positioning near a strong pro-moter or its fusion with another gene, endowing the fusedtranscript with tumorigenic properties (4). Recently, a trans-location between chromosomes 2 and 3, t(2;3)(q13;p25), wasreported to be specific to FTC (5). Cloning of the translocationbreakpoint revealed a fusion between the DNA binding do-main of the thyroid-specific transcription factor paired box
gene (PAX8) and the peroxisome proliferator-activated re-ceptor � (PPAR�). This fusion gene was present in the ma-jority of FTC but was not seen in any of the papillary thyroidcarcinoma, FTA, or multinodular goiters (5), suggesting thatit may be a useful marker for the preoperative differentiationbetween FTC and FTA. The occurrence of PAX8/PPAR� re-arrangements in a significant proportion of FTC cases wasrecently confirmed by three studies, which also reported thePAX8/PPAR� fusion in a few cases of FTA (6–8).
In the present study, we have determined the involvementof the PAX8/PPAR� rearrangement in a series of 34 regularFTC and 20 FTA, as well as in 20 FTA diagnosed as atypical(AFTA). In addition, 13 anaplastic thyroid carcinomas (ATC)were similarly analyzed, because this most aggressive formof thyroid cancer has been proposed to originate from dif-ferentiated papillary or follicular forms. These analyses wereperformed using RT-PCR followed by sequencing, fluores-cence in situ hybridization (FISH), and Western analysis.
Patients and MethodsPatients and tumor samples
Seventy-four follicular tumors, 13 anaplastic carcinomas, and twonormal thyroid samples were obtained from 89 patients who underwentthyroidectomy at the Karolinska Hospital (Stockholm, Sweden). Thetumors were classified by routine histopathological examination, ac-cording to the criteria of the World Health Organization committee (9),as follows: 1) FTA, a benign encapsulated tumor showing evidence offollicular cell differentiation; 2) AFTA, an encapsulated tumor withfollicular cell differentiation. The tumor has an irregular architecture and
Abbreviations: AFTA, Atypical FTA; ATC, anaplastic thyroid carci-nomas; FISH, fluorescence in situ hybridization; FTA, follicular thyroidadenoma; FTC, follicular thyroid carcinoma; PPAR�, peroxisome pro-liferator-activated receptor �.
0021-972X/03/$15.00/0 The Journal of Clinical Endocrinology & Metabolism 88(9):4440–4445Printed in U.S.A. Copyright © 2003 by The Endocrine Society
doi: 10.1210/jc.2002-021690
4440

cellular pattern, with signs of considerable proliferation and pleomor-phism. Frequent mitoses are often seen. Invasion into the capsule, orvascular invasion must be carefully excluded; 3) FTC, minimally inva-sive (MI) type, a malignant tumor with follicular cell differentiation butlacking the diagnostic features of papillary carcinoma. Unequivocalvascular invasion in few vessels occur and/or invasion through the fullthickness of the capsule; 4) FTC, widely invasive (WI) type, as per MItype but with widespread infiltration of several blood vessels and/orbroad invasion of surrounding tissues; 5) ATC, a highly malignanttumor composed in part or wholly of undifferentiated cells. The tumoris typically composed of varying proportions of spindle, polygonal, andgiant cells.
Using the above-mentioned criteria, the 87 thyroid tumors were clas-sified as follows: 28 FTC-MI, six FTC-WI, 20 FTA, 20 AFTA, and 13 ATC.All AFTA samples were reevaluated by further sectioning, at differentdepths through the tumor sample, to exclude capsular or vascular in-vasion. In no case was the original diagnosis changed. All tissue fromthe thyroid tumors was frozen in liquid nitrogen immediately aftersurgical removal and stored at �70 C until required. For each frozensample used, a representative section was cut, embedded in paraffin,and subjected to histopathological evaluation to confirm the high purityof tumor cells (�70%) in the tumor samples and the lack of neoplasticcells in the normal controls. None of the patients had previously beenexposed to irradiation, with the exception of the 13 ATC patients whounderwent intensive irradiation therapy 3–6 wk before surgery. Allpatients gave informed consent according to a protocol approved by theethical committee at the Karolinska Hospital.
RT-PCR and cDNA sequencing
Total RNA was isolated from the 87 tumor samples and two normalthyroid samples using either the BIOTECX Ultraspec-II (Biotecx Labo-ratories, Houston, TX) or TRIzol (Invitrogen AB, Lidingo, Sweden) RNAisolation system and was used for RT-PCR-based detection of the PAX8/PPAR� fusion transcript. Briefly, cDNA was synthesized from 3 �g oftotal RNA using oligo (dT) primers and Superscript II reverse tran-scriptase (Invitrogen AB, Lidingo, Sweden), according to the manufac-turer’s instructions. The PCR amplifications were performed using theAdvantage 2 PCR Enzyme System (Clontech, Palo Alto, CA) accordingto the manufacturer’s instructions and with the following primers: 5�-GCATTGACTCACAGAGCAGCA-3� (PAX8, c.786–806, accession no.X69699) or 5�-GCCACCAAGTCCCTGAGTCC-3� (PAX8, c.605–624, ac-cession no. X69699) and 5�-CATTACGGAGAGATCCACGG-3� (PPAR�,c.158–177, accession no. X90563). In short, 2 �l of each cDNA wasamplified in 20-�l reactions containing 0.4 �l of 50� dNTP Mix, 0.4 �lof 50� Advantage 2 Polymerase Mix, 2.0 �l of 10� Advantage 2 PCRBuffer, and 0.4 �m of each primer. The amplifications were performedusing the following thermocycling conditions: an initial denaturation at95 C for 1 min, was followed by 35 step cycles of denaturing at 95 C for10 sec, annealing at 60 C for 10 sec, and extension at 72 C for 15 sec, witha final extension at 72 C for 1 min. RNA integrity and efficiency of cDNAsynthesis were assessed by parallel amplification with the housekeepinggene �-actin (ACTB, accession no. XM037239), as previously described(10). PCR products were directly sequenced and analyzed on a 377XLautomated DNA sequencer (Applied Biosystems, Perkin-Elmer Corp.,Foster City, CA), as previously described (11).
FISH
Probes. The genomic clones used for FISH analyses originate from thehuman male BAC library RPCI-11 (http://www.chori.org/bacpac). Afusion assay was applied to detect the presence of the PAX8/PPAR�fusion gene, whereby one clone from the PAX8 locus in 2q13 wascohybridized with a second clone from the PPAR� locus in 3p25. Spe-cifically, RP11–434I13 centromeric of PAX8 was combined with RP11–402P11 telomeric to PPAR�, or RP11–368K23 telomeric of PAX8 wascombined with RP11–57D6 centromeric of PPAR� (see Fig. 2). DNA wasisolated from the BAC clones using the Qiagen Plasmid Midi Kit (VWRInternational AB, Stockholm, Sweden), according to the manufacturer’sinstructions, and labeled by nick translation with fluorescein-12-dUTPor Texas Red-5-dUTP (NEN, Life Science Products, Boston, MA). Incontrol experiments, the accuracy and specificity of all four BAC clones
were confirmed by hybridization onto normal male human metaphasechromosomes (Vysis, Inc., Downers Grove, IL).
Interphase FISH analysis. Interphase nuclei were prepared as previouslydescribed (12). Briefly, a small piece of each tumor or normal tissue wascut and gently touched onto a glass slide, fixed in methanol-acetic acid(3:1), air dried, and stored at �20 C. Dual-color FISH was performedusing standard methods. Interphase nuclei were denatured in 70% for-mamide/2� saline sodium citrate (SSC) (pH 7.0) at 75 C for 3 min,followed by dehydration in 70, 85, and 100% ethanol for 2 min each. Thehybridization mixture, containing 10 ng/�l of each of the labeled probes(either 57D6 and 368K23, or 402P11 and 434I13), was denatured for 7 minat 80 C followed by preannealing at 37 C for 60 min. Ten microliters ofthe hybridization mixture were then applied to the interphase nuclei.After hybridization at 37 C for 48 h, the slides were washed in 0.4�SSC/0.3% Tween 20 at 74 C for 2 min, 2� SSC/0.1% Tween 20 at roomtemperature for 2 min, followed by water at room temperature for 2 min,before being air dried. After counterstaining with 4,6-diamino-2-phenylindole and mounting in antifade, hybridization signals wereanalyzed by use of a Zeiss Axioplan 2 (Carl Zeiss Jena GmbH, Jena,Germany) epifluorescence microscope and documented using theMetasystems Isis imaging system (Metasystems, Altlussheim, Ger-many). Nuclei in which the two probes were fused, touched, or wereclose to each other (distance � 1 probe signal) were scored as positivefor gene fusions. From each case, 100 nonoverlapping nuclei were in-cluded in the scoring without other selection criteria. All discrete hy-bridization signals were counted, and manual adjustment was appliedto detect signals in slightly different focal planes. The specificity of thefusion assay was confirmed by hybridization to the interphase nuclei oftwo normal thyroids, which showed falsely positive signals in less than10% of the nuclei.
Western analysis
Protein was extracted from the tumor and normal thyroid tissuesaccording to standard procedures using RIPA buffer. A total of 100 �gof protein in 1� sodium dodecyl sulfate buffer containing 50 mm di-thiothreitol was heated to 85 C for 5 min and then electrophoresed, with5 �l of kaleidoscope protein size standard (Bio-Rad Laboratories, Her-cules, CA), on 7.5% SDS-PAGE gels in a mini-Protean 2 electrophoresissystem (Bio-Rad). Proteins were blotted onto 0.45-�m nitrocellulosemembranes (Protran; Schleicher & Schuell, Dassel, Germany), stainedwith Ponceau S, and scanned into the computer to use as a loadingcontrol. After blocking in 4% nonfat milk, the membranes were incu-bated with anti-PPAR� (sc-7273; 1:500 dilution) (Santa Cruz Biotech-nology, Santa Cruz, CA) or anti-Pax-8 (kindly provided by Prof. RobertoDi Lauro, Stazione Zoologica A. Dohrn, Napoli, Italy; 1:2000 dilution) at4 C overnight. The membranes were then incubated with secondaryhorseradish peroxidase-conjugated antibodies (1:2000 dilution; SantaCruz Biotechnology). Detection was carried out by enhanced chemilu-minescence (Amersham Pharmacia Biotech, Uppsala, Sweden) for 1 h,and the proteins were visualized by a charge coupled device camerausing the luminescent image analyzer LAS-1000plus (Fujifilm, Tokyo,Japan) and analyzed using the Image Gauge V3.3 program (Fujifilm). Toconfirm that approximately equal amounts of protein were blotted ineach sample, the filters were reversibly stained with a 3% Ponceau Ssolution (Sigma-Aldrich, St. Louis, MO) in 3% trichloroacetic acid, beforeincubating with the primary antibody, as described by Wautot et al. (13).Specific blocking peptides for PPAR� (Sc7752p) and PAX8 (Sc7273p)(Santa Cruz Biotechnology) were used to confirm the identity of bandsfor fusion transcripts. Peptide neutralization was done according to theprotocol recommended by the manufacturer. The blocking peptideswere incubated with the primary antibody at room temperature for 2 hand then used for filter hybridization. In all cases, the Western signal(enhanced chemiluminescence) was blocked, thus confirming the iden-tity and specificity of the PPAR� and PAX8 signals. A positive controlwith a known PAX8-PPAR� fusion was also used.
Results
The involvement of the PAX8/PPAR� fusion oncogene wasevaluated on the genomic, RNA, and protein levels in a panel
Dwight et al. • PAX8/PPAR� in Follicular Thyroid Tumors J Clin Endocrinol Metab, September 2003, 88(9):4440–4445 4441
of 87 thyroid tumors. The results for the different histopatho-logical subtypes are summarized in Table 1.
RT-PCR and cDNA sequencing
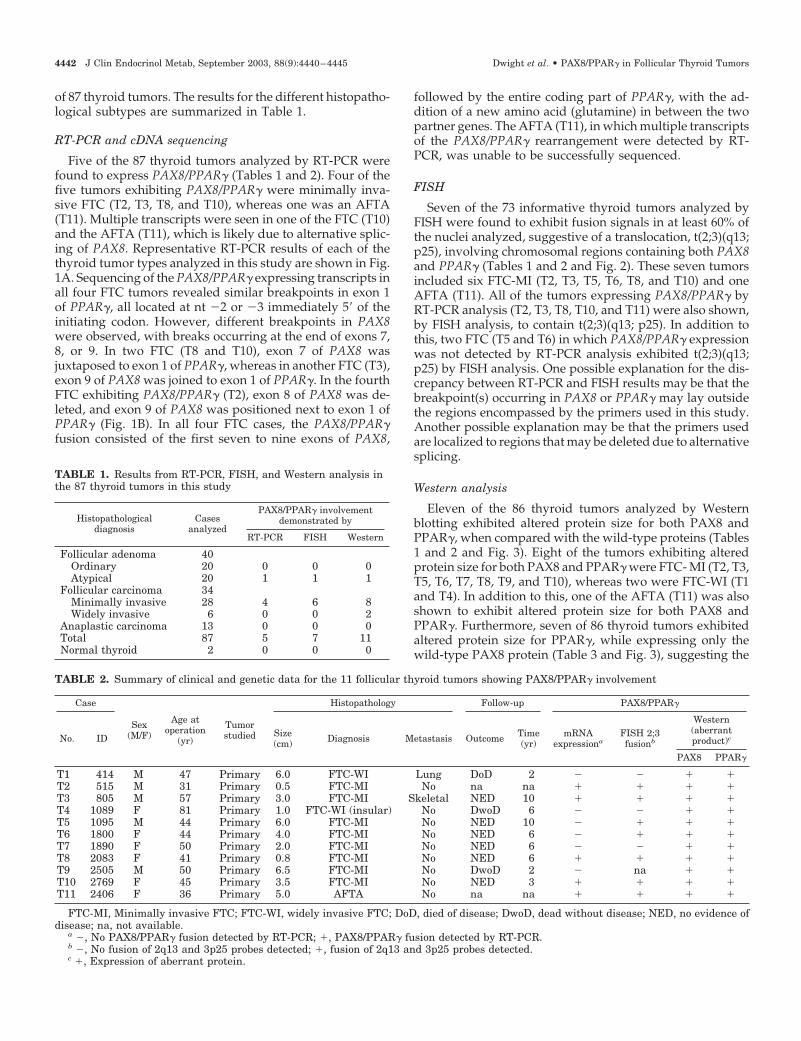
Five of the 87 thyroid tumors analyzed by RT-PCR werefound to express PAX8/PPAR� (Tables 1 and 2). Four of thefive tumors exhibiting PAX8/PPAR� were minimally inva-sive FTC (T2, T3, T8, and T10), whereas one was an AFTA(T11). Multiple transcripts were seen in one of the FTC (T10)and the AFTA (T11), which is likely due to alternative splic-ing of PAX8. Representative RT-PCR results of each of thethyroid tumor types analyzed in this study are shown in Fig.1A. Sequencing of the PAX8/PPAR� expressing transcripts inall four FTC tumors revealed similar breakpoints in exon 1of PPAR�, all located at nt �2 or �3 immediately 5� of theinitiating codon. However, different breakpoints in PAX8were observed, with breaks occurring at the end of exons 7,8, or 9. In two FTC (T8 and T10), exon 7 of PAX8 wasjuxtaposed to exon 1 of PPAR�, whereas in another FTC (T3),exon 9 of PAX8 was joined to exon 1 of PPAR�. In the fourthFTC exhibiting PAX8/PPAR� (T2), exon 8 of PAX8 was de-leted, and exon 9 of PAX8 was positioned next to exon 1 ofPPAR� (Fig. 1B). In all four FTC cases, the PAX8/PPAR�fusion consisted of the first seven to nine exons of PAX8,
followed by the entire coding part of PPAR�, with the ad-dition of a new amino acid (glutamine) in between the twopartner genes. The AFTA (T11), in which multiple transcriptsof the PAX8/PPAR� rearrangement were detected by RT-PCR, was unable to be successfully sequenced.
FISH
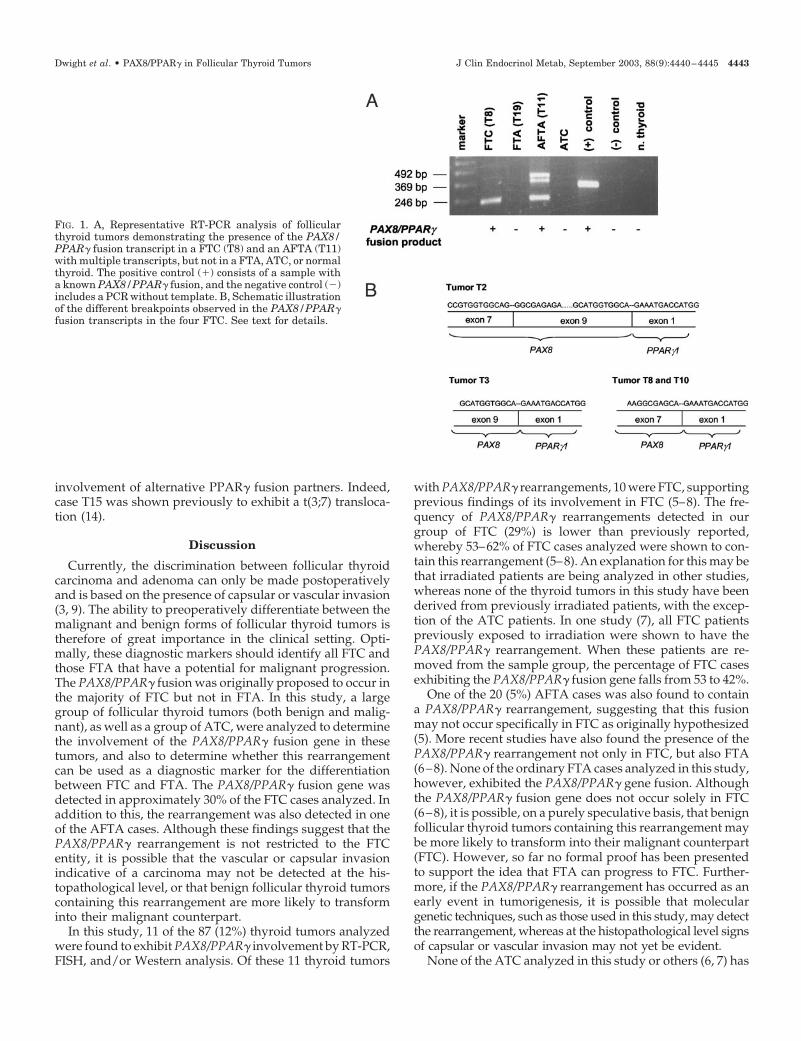
Seven of the 73 informative thyroid tumors analyzed byFISH were found to exhibit fusion signals in at least 60% ofthe nuclei analyzed, suggestive of a translocation, t(2;3)(q13;p25), involving chromosomal regions containing both PAX8and PPAR� (Tables 1 and 2 and Fig. 2). These seven tumorsincluded six FTC-MI (T2, T3, T5, T6, T8, and T10) and oneAFTA (T11). All of the tumors expressing PAX8/PPAR� byRT-PCR analysis (T2, T3, T8, T10, and T11) were also shown,by FISH analysis, to contain t(2;3)(q13; p25). In addition tothis, two FTC (T5 and T6) in which PAX8/PPAR� expressionwas not detected by RT-PCR analysis exhibited t(2;3)(q13;p25) by FISH analysis. One possible explanation for the dis-crepancy between RT-PCR and FISH results may be that thebreakpoint(s) occurring in PAX8 or PPAR� may lay outsidethe regions encompassed by the primers used in this study.Another possible explanation may be that the primers usedare localized to regions that may be deleted due to alternativesplicing.
Western analysis
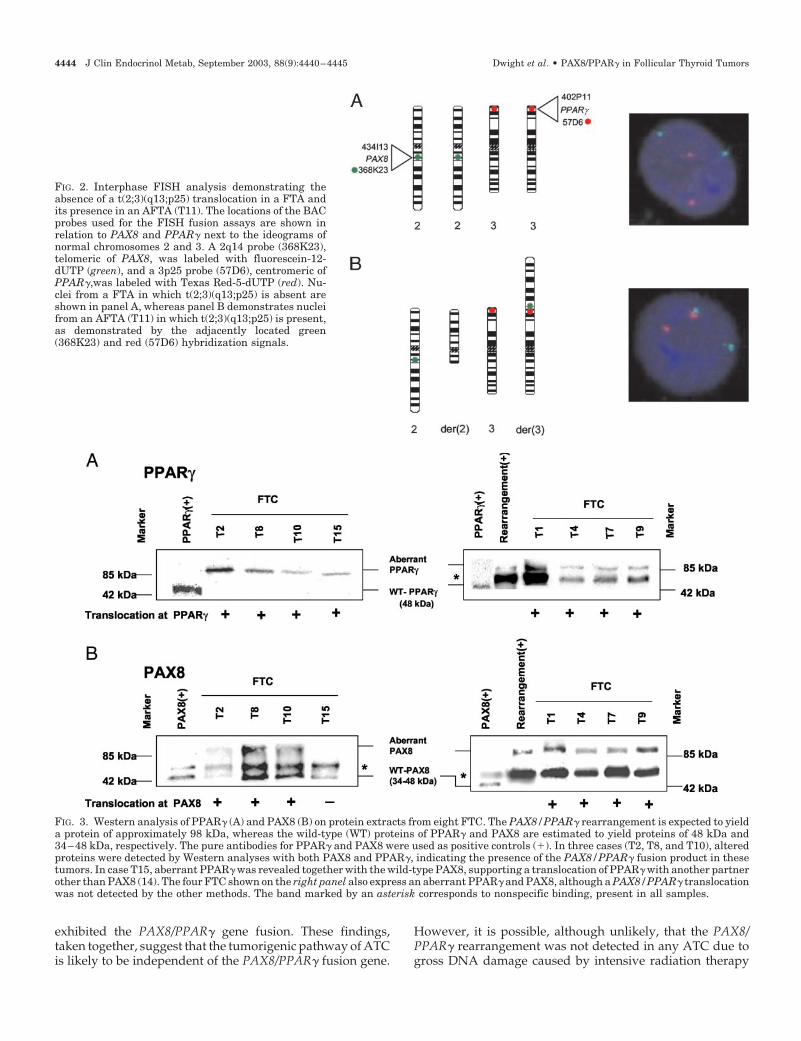
Eleven of the 86 thyroid tumors analyzed by Westernblotting exhibited altered protein size for both PAX8 andPPAR�, when compared with the wild-type proteins (Tables1 and 2 and Fig. 3). Eight of the tumors exhibiting alteredprotein size for both PAX8 and PPAR� were FTC- MI (T2, T3,T5, T6, T7, T8, T9, and T10), whereas two were FTC-WI (T1and T4). In addition to this, one of the AFTA (T11) was alsoshown to exhibit altered protein size for both PAX8 andPPAR�. Furthermore, seven of 86 thyroid tumors exhibitedaltered protein size for PPAR�, while expressing only thewild-type PAX8 protein (Table 3 and Fig. 3), suggesting the
TABLE 1. Results from RT-PCR, FISH, and Western analysis inthe 87 thyroid tumors in this study
Histopathologicaldiagnosis
Casesanalyzed
PAX8/PPAR� involvementdemonstrated by
RT-PCR FISH Western
Follicular adenoma 40Ordinary 20 0 0 0Atypical 20 1 1 1
Follicular carcinoma 34Minimally invasive 28 4 6 8Widely invasive 6 0 0 2
Anaplastic carcinoma 13 0 0 0Total 87 5 7 11Normal thyroid 2 0 0 0
TABLE 2. Summary of clinical and genetic data for the 11 follicular thyroid tumors showing PAX8/PPAR� involvement
Case
Sex(M/F)
Age atoperation
(yr)
Tumorstudied
Histopathology Follow-up PAX8/PPAR�
No. ID Size(cm) Diagnosis Metastasis Outcome Time
(yr)mRNA
expressionaFISH 2;3fusionb
Western(aberrantproduct)c
PAX8 PPAR�
T1 414 M 47 Primary 6.0 FTC-WI Lung DoD 2 � � � �T2 515 M 31 Primary 0.5 FTC-MI No na na � � � �T3 805 M 57 Primary 3.0 FTC-MI Skeletal NED 10 � � � �T4 1089 F 81 Primary 1.0 FTC-WI (insular) No DwoD 6 � � � �T5 1095 M 44 Primary 6.0 FTC-MI No NED 10 � � � �T6 1800 F 44 Primary 4.0 FTC-MI No NED 6 � � � �T7 1890 F 50 Primary 2.0 FTC-MI No NED 6 � � � �T8 2083 F 41 Primary 0.8 FTC-MI No NED 6 � � � �T9 2505 M 50 Primary 6.5 FTC-MI No DwoD 2 � na � �T10 2769 F 45 Primary 3.5 FTC-MI No NED 3 � � � �T11 2406 F 36 Primary 5.0 AFTA No na na � � � �
FTC-MI, Minimally invasive FTC; FTC-WI, widely invasive FTC; DoD, died of disease; DwoD, dead without disease; NED, no evidence ofdisease; na, not available.
a �, No PAX8/PPAR� fusion detected by RT-PCR; �, PAX8/PPAR� fusion detected by RT-PCR.b �, No fusion of 2q13 and 3p25 probes detected; �, fusion of 2q13 and 3p25 probes detected.c �, Expression of aberrant protein.
4442 J Clin Endocrinol Metab, September 2003, 88(9):4440–4445 Dwight et al. • PAX8/PPAR� in Follicular Thyroid Tumors
involvement of alternative PPAR� fusion partners. Indeed,case T15 was shown previously to exhibit a t(3;7) transloca-tion (14).
Discussion
Currently, the discrimination between follicular thyroidcarcinoma and adenoma can only be made postoperativelyand is based on the presence of capsular or vascular invasion(3, 9). The ability to preoperatively differentiate between themalignant and benign forms of follicular thyroid tumors istherefore of great importance in the clinical setting. Opti-mally, these diagnostic markers should identify all FTC andthose FTA that have a potential for malignant progression.The PAX8/PPAR� fusion was originally proposed to occur inthe majority of FTC but not in FTA. In this study, a largegroup of follicular thyroid tumors (both benign and malig-nant), as well as a group of ATC, were analyzed to determinethe involvement of the PAX8/PPAR� fusion gene in thesetumors, and also to determine whether this rearrangementcan be used as a diagnostic marker for the differentiationbetween FTC and FTA. The PAX8/PPAR� fusion gene wasdetected in approximately 30% of the FTC cases analyzed. Inaddition to this, the rearrangement was also detected in oneof the AFTA cases. Although these findings suggest that thePAX8/PPAR� rearrangement is not restricted to the FTCentity, it is possible that the vascular or capsular invasionindicative of a carcinoma may not be detected at the his-topathological level, or that benign follicular thyroid tumorscontaining this rearrangement are more likely to transforminto their malignant counterpart.
In this study, 11 of the 87 (12%) thyroid tumors analyzedwere found to exhibit PAX8/PPAR� involvement by RT-PCR,FISH, and/or Western analysis. Of these 11 thyroid tumors
with PAX8/PPAR� rearrangements, 10 were FTC, supportingprevious findings of its involvement in FTC (5–8). The fre-quency of PAX8/PPAR� rearrangements detected in ourgroup of FTC (29%) is lower than previously reported,whereby 53–62% of FTC cases analyzed were shown to con-tain this rearrangement (5–8). An explanation for this may bethat irradiated patients are being analyzed in other studies,whereas none of the thyroid tumors in this study have beenderived from previously irradiated patients, with the excep-tion of the ATC patients. In one study (7), all FTC patientspreviously exposed to irradiation were shown to have thePAX8/PPAR� rearrangement. When these patients are re-moved from the sample group, the percentage of FTC casesexhibiting the PAX8/PPAR� fusion gene falls from 53 to 42%.
One of the 20 (5%) AFTA cases was also found to containa PAX8/PPAR� rearrangement, suggesting that this fusionmay not occur specifically in FTC as originally hypothesized(5). More recent studies have also found the presence of thePAX8/PPAR� rearrangement not only in FTC, but also FTA(6–8). None of the ordinary FTA cases analyzed in this study,however, exhibited the PAX8/PPAR� gene fusion. Althoughthe PAX8/PPAR� fusion gene does not occur solely in FTC(6–8), it is possible, on a purely speculative basis, that benignfollicular thyroid tumors containing this rearrangement maybe more likely to transform into their malignant counterpart(FTC). However, so far no formal proof has been presentedto support the idea that FTA can progress to FTC. Further-more, if the PAX8/PPAR� rearrangement has occurred as anearly event in tumorigenesis, it is possible that moleculargenetic techniques, such as those used in this study, may detectthe rearrangement, whereas at the histopathological level signsof capsular or vascular invasion may not yet be evident.
None of the ATC analyzed in this study or others (6, 7) has
FIG. 1. A, Representative RT-PCR analysis of follicularthyroid tumors demonstrating the presence of the PAX8/PPAR� fusion transcript in a FTC (T8) and an AFTA (T11)with multiple transcripts, but not in a FTA, ATC, or normalthyroid. The positive control (�) consists of a sample witha known PAX8/PPAR� fusion, and the negative control (�)includes a PCR without template. B, Schematic illustrationof the different breakpoints observed in the PAX8/PPAR�fusion transcripts in the four FTC. See text for details.
Dwight et al. • PAX8/PPAR� in Follicular Thyroid Tumors J Clin Endocrinol Metab, September 2003, 88(9):4440–4445 4443
exhibited the PAX8/PPAR� gene fusion. These findings,taken together, suggest that the tumorigenic pathway of ATCis likely to be independent of the PAX8/PPAR� fusion gene.
However, it is possible, although unlikely, that the PAX8/PPAR� rearrangement was not detected in any ATC due togross DNA damage caused by intensive radiation therapy
FIG. 2. Interphase FISH analysis demonstrating theabsence of a t(2;3)(q13;p25) translocation in a FTA andits presence in an AFTA (T11). The locations of the BACprobes used for the FISH fusion assays are shown inrelation to PAX8 and PPAR� next to the ideograms ofnormal chromosomes 2 and 3. A 2q14 probe (368K23),telomeric of PAX8, was labeled with fluorescein-12-dUTP (green), and a 3p25 probe (57D6), centromeric ofPPAR�,was labeled with Texas Red-5-dUTP (red). Nu-clei from a FTA in which t(2;3)(q13;p25) is absent areshown in panel A, whereas panel B demonstrates nucleifrom an AFTA (T11) in which t(2;3)(q13;p25) is present,as demonstrated by the adjacently located green(368K23) and red (57D6) hybridization signals.
FIG. 3. Western analysis of PPAR� (A) and PAX8 (B) on protein extracts from eight FTC. The PAX8/PPAR� rearrangement is expected to yielda protein of approximately 98 kDa, whereas the wild-type (WT) proteins of PPAR� and PAX8 are estimated to yield proteins of 48 kDa and34–48 kDa, respectively. The pure antibodies for PPAR� and PAX8 were used as positive controls (�). In three cases (T2, T8, and T10), alteredproteins were detected by Western analyses with both PAX8 and PPAR�, indicating the presence of the PAX8/PPAR� fusion product in thesetumors. In case T15, aberrant PPAR� was revealed together with the wild-type PAX8, supporting a translocation of PPAR� with another partnerother than PAX8 (14). The four FTC shown on the right panel also express an aberrant PPAR� and PAX8, although a PAX8/PPAR� translocationwas not detected by the other methods. The band marked by an asterisk corresponds to nonspecific binding, present in all samples.
4444 J Clin Endocrinol Metab, September 2003, 88(9):4440–4445 Dwight et al. • PAX8/PPAR� in Follicular Thyroid Tumors

administered to these patients before surgery. It is also un-clear as to whether ATC develops from papillary or follicularcancers, respectively, or if they occur by dedifferentiationwithout an intermediate stage as a differentiated carcinoma.Furthermore, it is possible that the PAX8/PPAR� rearrange-ment arrests tumors in a differentiated state. Other geneticevents may then accumulate, driving progression and aclonal loss of the PAX8/PPAR� fusion gene, which subse-quently may lead to dedifferentiation. There is some geneticevidence for such a process (10), but whether or not thePAX8/PPAR� fusion gene, or its loss, is involved in ATCtumorigenesis requires further study.
It is of interest to note that PPAR� involvement alone wasshown by Western analysis in seven follicular thyroid tumors(four minimally invasive FTC, one AFTA, one ATC, and oneFTA), suggesting that, in some cases, PPAR� may be fusingwith a non-PAX8 partner. Further analysis in one of thesetumors (T15), revealed a translocation involving chromo-somes 3 and 7 [t(3;7)(p25;q34)] (Ref. 14). Identification of thetranslocation partners has revealed a new fusion oncogene(Lui, W. O., I. Leibiger, B. Leibiger, S. Thoppe, U. Enberg, J.Liden, A. Hoog, L. O. Farnebo, J. A. Fletcher, C. Larsson,submitted for publication).
In conclusion, our findings suggest that PAX8/PPAR�shows a high specificity to FTC, and although it was detectedin one AFTA, the presence of this rearrangement is highlysuggestive of a malignant form of follicular thyroid tumor.We therefore postulate that detecting the presence of thePAX8/PPAR� rearrangement is of considerable importancein the clinical setting.
Acknowledgments
We thank Lisa Ånfalk for excellent technical assistance and Dr. ToddKroll for valuable comments on the manuscript.
Received October 29, 2002. Accepted May 28, 2003.Address all correspondence and requests for reprints to: Trisha
Dwight, Ph.D., or Catharina Larsson, Department of Molecular Medi-
cine Endocrine Tumor Unit, CMM L8:01 Karolinska Hospital, SE-171 76,Stockholm, Sweden. E-mail: [email protected] or [email protected].
This work was supported by the Swedish Cancer Foundation, theGustav V Jubilee Foundation, the Milton Foundation, the Cancer Societyin Stockholm, the Emil and Vera Cornell Foundation, the Wenner-GrenFoundation, and the Torsten and Ragnar Soderberg Foundations.
References
1. Gimm O 2001 Thyroid cancer. Cancer Lett 163:143–1562. Lawrence Jr W, Kaplan BJ 2002 Diagnosis and management of patients with
thyroid nodules. J Surg Oncol 80:157–1703. Vini L, Harmer C 2002 Management of thyroid cancer. Lancet Oncol 3:407–4144. Lengauer C, Kinzler KW, Vogelstein B 1998 Genetic instabilities in human
cancers. Nature 396:643–6495. Kroll TG, Sarraf P, Pecciarini L, Chen CJ, Mueller E, Spiegelman BM,
Fletcher JA 2000 PAX8-PPAR�1 fusion oncogene in human thyroid carcinoma.Science 289:1357–1360
6. Marques AR, Espadinha C, Catarino AL, Moniz S, Pereira T, Sobrinho LG,Leite V 2002 Expression of PAX8-PPAR�1 rearrangements in both follicularthyroid carcinomas and adenomas. J Clin Endocrinol Metab 87:3947–3952
7. Nikiforova MN, Biddinger PW, Caudill CM, Kroll TG, Nikiforov YE 2002PAX8-PPAR� rearrangement in thyroid tumors: RT-PCR and immunohisto-chemical analyses. Am J Surg Pathol 26:1016–1023
8. Cheung L, Messina M, Gill A, Clarkson A, Learoyd D, Delbridge L, Went-worth J, Philips J, Clifton-Bligh R, Robinson BG 2003 Detection of thePAX8-PPAR� fusion oncogene in both follicular thyroid carcinomas and ad-enomas. J Clin Endocrinol Metab 88:354–357
9. Hedinger CE, Williams ED, Sobin LH 1988 The WHO international classi-fication of tumors. 2nd ed. Berlin: Springer-Verlag
10. Frisk T, Foukakis T, Dwight T, Lundberg J, Hoog A, Wallin G, Eng C,Zedenius J, Larsson C 2002 Silencing of the PTEN tumor-suppressor gene inanaplastic thyroid cancer. Genes Chromosomes Cancer 35:74–80
11. Dwight T, Twigg S, Delbridge L, Wong FK, Farnebo F, Richardson AL,Nelson A, Zedenius J, Philips J, Larsson C, Teh BT, Robinson BG 2000 Lossof heterozygosity in sporadic parathyroid tumours: involvement of chromo-some 1 and the MEN1 gene locus in 11q13. Clin Endocrinol (Oxf) 53:85–92
12. Yang K, Lui WO, Xie Y, Zhang A, Skytting B, Mandahl N, Larsson C, LarssonO 2002 Co-existence of SYT-SSX1 and SYT-SSX2 fusions in synovial sarcomas.Oncogene 21:4181–4190
13. Wautot V, Khodaei S, Frappart L, Buisson N, Baro E, Lenoir GM, CalenderA, Zhang CX, Weber G 2000 Expression analysis of endogenous menin, theproduct of the multiple endocrine neoplasia type 1 gene, in cell lines andhuman tissues. Int J Cancer 851:877–881
14. Lui WO, Kytola S, Ånfalk L, Larsson C, Farnebo LO 2000 Balanced trans-location (3;7)(p25;q34): another mechanism of tumorigenesis in follicular thy-roid carcinoma? Cancer Genet Cytogenet 119:109–112
TABLE 3. Summary of clinical and genetic data for the thyroid tumors showing only PPAR� involvement
Case
Sex(M/F)
Age atoperation
(yr)
Tumorstudied
Histopathology Follow-up PAX8/PPAR�
No. ID Size(cm) Diagnosis Metastasis Outcome Time
(yr)mRNA
expressionaFISH 2;3fusionb
Western(aberrantproduct)c
PAX8 PPAR�
T12 1129 F 83 Primary 3.0 FTC-MI No NED 8 � � � �T13 2311 F 31 Primary 2.0 FTC-MI No NED 5 � � � �T14 2384 F 70 Primary 6.0 FTC-MI No NED 4 � � � �T15 2723 M 72 Primary 7.0 FTC-MI No NED 3 � � � �T16 2507 F 49 Primary 2.0 AFTA No NED 4 � � � �T17 2288 M 71 Primary 6.5 ATC No na na � na � �T18 222 F 55 Primary 2.0 FTA No NED 14 � na � �
FTC-MI, Minimally invasive FTC; NED, no evidence of disease; na, not available.a �, No PAX8/PPAR� fusion detected by RT-PCR; �, PAX8/PPAR� fusion detected by RT-PCR.b �, No fusion of 2q13 and 3p25 probes detected; �, fusion of 2q13 and 3p25 probes detected.c �, Expression of aberrant protein.
Dwight et al. • PAX8/PPAR� in Follicular Thyroid Tumors J Clin Endocrinol Metab, September 2003, 88(9):4440–4445 4445














![Clinical impact of follicular oncocytic (Hürthle cell ... · oxyphilic or oncocytic cell follicular thyroid carcinoma, rep-resents about 3–5% of thyroid carcinomas [5–8]. Traditionally,](https://img.pdfslide.net/doc/110x75/5f96415ab1c35b1da41c4408/clinical-impact-of-follicular-oncocytic-hrthle-cell-oxyphilic-or-oncocytic.jpg)













