Embed Size (px)
Citation preview



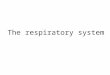
Aeromedical evacuation

Hoist Rescue

Sling single?

Double sling?

Stretcher?

Rescue basket?

Respiratory Function in Hoist Rescue: Comparing
Slings, Stretcher, and Rescue Basket
From CareFlight NSW, Northmead, NSW, Australia.
David Murphy , Alan Garner , and Rod Bishop
Aviation, Space, and Environmental Medicine x Vol. 82, No. 2 x February 2011
CareFlight NSW, Northmead, NSW, Australia

INTRODUCTION

A) single sling B) double sling
INTRODUCTION

C) stretcher
D) rescue basket
INTRODUCTION

INTRODUCTION

INTRODUCTION

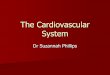
So what happens?
General feelings of unease Dizzy, sweaty and other signs of shock Increased pulse and breathing rates
Then a sudden drop in pulse & BP Instant loss of consciousness If not rescued, death is certain
From suffocation due to a closed airway, or from lack of blood flow and oxygen to the brain.
Suspention trauma and harness-hang syndrome
INTRODUCTION

Suspention trauma and harness-hang syndrome
INTRODUCTION

INTRODUCTION

INTRODUCTION

INTRODUCTION

INTRODUCTION

When is a severe acute episodehappening?• Limited ability to speak• Pulsus paradoxus > 25mmHg• Pulse >110/min• RR >25-30/min• Flow rates <50% predicted• O2 saturation <91-92%• Some consider flow rates < 35% predictedto be life-threatening
INTRODUCTION
Sever Asthma





Stepwise approach ( children)
classificaticlassificationon
mild mild IntermitteIntermittentnt
Mild Mild persistentpersistent
Moderate Moderate persistentpersistent
Severe Severe persistentpersistent
Minor Minor symptomssymptoms
< 1/week< 1/week 1-3 /week1-3 /week 4-5/week4-5/week ContinuouContinuouss
exacerbatiexacerbation/ on/ nocturnalnocturnal
< 1/month< 1/month 1 /month1 /month 2-3/month2-3/month > 4 > 4 /month/month
PEF PEF between between attacksattacks
>80%>80% >80%>80% 60-80%60-80% < 60%< 60%
Step 1Step 1 Step 2Step 2 Step 3Step 3 Step 4Step 4

Stepwise approach ( adult)
classificaticlassificationon
mild mild IntermitteIntermittentnt
Mild Mild persistentpersistent
Moderate Moderate persistentpersistent
Severe Severe persistentpersistent
Minor Minor symptomssymptoms
< 2 /week < 2 /week 2-3 /week2-3 /week 4-5 /week4-5 /week ContinuouContinuouss
exacerbatiexacerbation/ on/ nocturnalnocturnal
< 2 < 2 /month/month
2-3 /month2-3 /month 4-5 /month4-5 /month > 5 > 5 /month/month
PEF PEF between between attacksattacks
>80%>80% >80%>80% 60-80%60-80% < 60%< 60%
Step 1Step 1 Step 2Step 2 Step 3Step 3 Step 4Step 4

Asthma classification

INTRODUCTION

Rescue Basket
(RB)>Stretcher
INTRODUCTION

H0 & H1 thesis
H1:Use of the RB would not be associated with impairment of spirometry in healthy volunteers
H0:Use of the Stretcher would not be associated with impairment of spirometry in healthy volunteers
INTRODUCTION

METHODS

Winch simulator

Randomized ,Controlled cross-over study
METHODS

Hypothesis Testing: Case-Crossover Studies
Study of “triggers” within an individual ”Case" and "control" component, but
information of both components will come from the same individual
”Case component" = hazard period which is the time period right before the disease or event onset
”Control component" = control period which is a specified time interval other than the hazard period
Randomized ,Controlled cross-over study

Randomized ,Controlled cross-over study
METHODS

METHODS

542-04-#38
Table of Random NumbersSequence - randomization

METHODS

METHODS

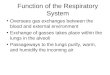
EasyOne Diagnostic Spirometer
METHODS

Pulmonary Function Testing

Perform test

Types of Spirometers
Bellows spirometers: Measure volume; mainly in lung function units
Electronic desk top spirometers: Measure flow and volume with real time display
Small hand-held spirometers: Inexpensive and quick to use but no print out

Volume Measuring Spirometer

Flow Measuring Spirometer

Desktop Electronic Spirometers

Small Hand-held Spirometers

Actual PFT Performance Technique
Prepare the equipment – find a nurse who knows (or is that nose?) what to do.
Patient should be seated with nose clip in place.
The patient needs to practice the exercise before actually performing the test. Have the patient breath in and out deeply several times.
Ask the patient to breath in as deeply as they can.

Actual PFT Performance Technique
The patient should place their mouth completely over the mouthpiece, not inside it.
Ask the patient to blow out as fast and as quick as they can for at least six seconds. Enthusiatically coach the patient – jump, shout, get down, hoot and holler…
“Blow, blow, come on, blow more, you can do it!”

Actual PFT Performance Technique
Once the patient has blown out as much as they can, ask them to then inhale as deeply as they can.
Repeat the whole test three times. The goal is to get a reproducible result that is consistent.
You may need to repeat the test more than three times in order to obtain an internally valid test.

Difinitions &Considerations

Lung Volumes and Capacities
There are four basic lung volumes: Inspiratory reserve volume (IRV) Tidal volume (TV) Expiratory reserve volume (ERV) Residual volume (RV)
In various combinations, these lung volumes then form lung capacities.
E.g., Vital capacity = IRV + TV + ERV


Lung Volumes

Normal Spirometry

Obstructive Pattern
■ Decreased FEV1
■ Decreased FVC
■ Decreased FEV1/FVC
- <70% predicted
■ FEV1 used to follow severity in COPD

Obstructive Lung Disease — Differential Diagnosis
Asthma
COPD - chronic bronchitis
- emphysema
Bronchiectasis
Bronchiolitis
Upper airway obstruction

Restrictive Pattern
Decreased FEV1
Decreased FVC
FEV1/FVC normal or increased

Restrictive Lung Disease —Differential Diagnosis
Pleural
Parenchymal
Chest wall
Neuromuscular

Spirometry Patterns

Indications for Pulmonary Function Testing
Patients 45 years old and older who have ever smoked.
Patients with prolonged or excessive cough or sputum production.
Patients with a history of exposure to lung irritants.

Indications for Pulmonary Function Testing
Detecting pulmonary disease Pulmonary symptoms – chest pain, orthopnea,
cough, phlegm production, dyspnea, wheezing
Physical findings – Chest wall problems, cyanosis, clubbing, decreased breath sounds
Abnormal labs/x-rays – ABG, Chest X-Ray

Indications for Pulmonary Function Testing
Assessing disease severity and progression Pulmonary disease – COPD, Cystic fibrosis, Interstitial
lung disease, Sarcoidosis
Cardiac disease – CHF, Congenital heart disease, Pulmonary hypertension
Neuromuscular disease – Amyotrophic lateral sclerosis, Guillain-Barre syndrome, Multiple sclerosis, Myasthenia gravis

Indications for Pulmonary Function Testing
Pre-operative risk stratification Thoracic surgery
Cardiac surgery
Organ transplantation
General surgical procedures
Evaluating disability and impairment

Contraindications for PFT
Relative contraindications for spirometry include hemoptysis of
unknown origin, pneumothorax, unstable angina pectoris,
recent myocardial infarction, thoracic aneurysms, abdominal
aneurysms, cerebral aneurysms, recent eye surgery (increased
intraocular pressure during forced expiration), recent abdominal
or thoracic surgical procedures, and patients with a history of
syncope associated with forced exhalation.

Normal Values
FVC is the total amount of air a person can exhale, usually measured in six seconds. 80 – 120% of predicted is a normal value 70 – 80% demonstrates mild
reduction/restriction 50 – 70% demonstrates moderate reduction <50% demonstrates severe reduction
FEV1 is the amount of air a person can exhale in one second. 80 – 120% of predicted is a normal value

Normal Values
FEV1/FVC ratio is the percentage of FVC that can be expired in one second. 75 – 80% is normal
60 – 80% demonstrates mild obstruction
50 – 60% demonstrates moderate obstruction
<50% demonstrates severe obstruction

Normal Values
FEF25-75 reflects small airway function >80% is normal
60 – 80% reflects mild obstruction in the small airways
40 – 60% reflects moderate obstruction
<40% reflects severe obstruction

Spirometry Interpretation: So what constitutes normal?
Normal values vary and depend on:
Height Age Gender Ethnicity

PFT Interpretation

PFT Interpretation
Three steps in interpretation
Is the test valid?
Interpret the test
Classify severity of disease if present

Validity
The test is valid is you have good patient effort and the three tests performed are internally consistent.
You may notice a learning curve in that the latter tests are better performed than the former.
Make sure that the tests are maximal effort. You need to be really aggressive in coaching your patient.

1 - good start of test : sharp take off 2- Meet end-of-test criteria
3- free from artifacts:
-Cough or glottis closure during the first second of exhalation
-Variable effort , submaximal effort
-Leak
-Obstructed mouthpiece
-Have a satisfactory exhalation 6 s of exhalation
Acceptability Criteria

After 3 acceptable spirograms been obtained
Are the two largest FVC within 150ml of each other?
Are the two largest FEV1 within 150ml of each other? If both of these criteria are met, the test session may
be concluded. If both of these criteria are not met, continue testing
until Both of the criteria are met with analysis of additional acceptable spirograms; OR a total of eight tests have been performed
Reproducibility Criteria

Interpretation of Spirometry
Step 1. Look at the Flow-Volume loop
Step 2. Look at the FEV1 (Nl ≥ 80% predicted).
Step 3. Look at FVC (Nl ≥ 80%).
Step 4. Look at FEV1/FVC ratio (Nl≥ 75%).
Step 5. Look at FEF25-75% (wide normal range)

Normal Values
FVC is the total amount of air a person can exhale, usually measured in six seconds. 80 – 120% of predicted is a normal value 70 – 80% demonstrates mild
reduction/restriction 50 – 70% demonstrates moderate reduction <50% demonstrates severe reduction
FEV1 is the amount of air a person can exhale in one second. 80 – 120% of predicted is a normal value

Normal Values
FEV1/FVC ratio is the percentage of FVC that can be expired in one second. 75 – 80% is normal
60 – 80% demonstrates mild obstruction
50 – 60% demonstrates moderate obstruction
<50% demonstrates severe obstruction

Normal Values
FEF25-75 reflects small airway function >80% is normal
60 – 80% reflects mild obstruction in the small airways
40 – 60% reflects moderate obstruction
<40% reflects severe obstruction

PFT Interpretation
Assess FVC, FEV1, and FEV1/FVC ratio.FVC and FEV1 normal, with a normal FEV1/FVC ratio:
Normal Test
FVC low, FEV1 low or normal, and a normal to high FEV1/FVC ratio:--Restrictive lung disease
FVC low or normal, FEV1 low, and a low FEV1/FVC ratio: Obstructive lung disease

Measurements Obtained from the FVC Curve
FEV1---the volume exhaled during the first second of the FVC maneuver
FEF 25-75%---the mean expiratory flow during the middle half of the FVC maneuver; reflects flow through the small (<2 mm in diameter) airways
FEV1/FVC---the ratio of FEV1 to FVC X 100 (expressed as a percent); an important value because a reduction of this ratio from expected values is specific for obstructive rather than restrictive diseases

Spirometry Interpretation: Obstructive vs. Restrictive Defect
Obstructive Disorders FVC nl or↓ FEV1 ↓ FEF25-75% ↓ FEV1/FVC ↓ TLC nl or ↑
Restrictive Disorders FVC ↓ FEV1 ↓ FEF 25-75% nl to ↓ FEV1/FVC nl to ↑ TLC ↓

Spirometry Interpretation: What do the numbers mean?
FVC Interpretation of %
predicted:
80-120% Normal 70-79% Mild reduction 50%-69% Moderate
reduction <50% Severe reduction
FEV1Interpretation of %
predicted:
>75% Normal 60%-75% Mild
obstruction 50-59% Moderate
obstruction <49% Severe obstruction
<25 y.o. add 5% and >60 y.o. subtract 5

Actual Predicted % PredictedFVC 4.0 4.5 88FEV1 3.4 4.2 89FEV1/FVC 85 82 112FEF25-75
Normal

Actual Predicted % PredictedFVC 2.0 4.0 50FEV1 1.8 3.7 47FEV1/FVC 90 82 112FEF25-75
Restrictive Pattern

Actual Predicted% PredictedFVC 4.0 4.5 88FEV1 2.4 4.2 58FEV1/FVC 60 82 76FEF25-75 2.2 4.450 Obstructive Pattern

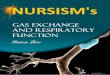
Acceptable and Unacceptable Spirograms (from ATS, 1994)

PFTsPFTs

Normal vs. Obstructive vs. Restrictive

Variable Effort

Early Glottic Closure

Cough

Flow-Volume Loops

Flow-Volume Loops

Special Techniques
Beta Agonist Challenge Methacholine Challenge DLCO

Beta Agonist Challenge
Perform this when there is a suspicion that the obstructive defect may be reversible –> asthma.
Give the patient a beta agonist treatment (two puffs of an albuterol MDI or an albuterol nebulizer) and repeat the PFTs several minutes later. If you notice a 12% or more increase in FEV1, then you have diagnosed reversible airway disease/asthma.

Methacholine Challenge
If you have a suspicion that the patient might have Exercise-induced bronchospasm (EIB), then refer them to a pulmonary lab where they can do provocative testing with methacholine.
If the patient has a decrease in their FEV1/FVC ratio with the inhalation of methacholine, then you have diagnosed EIB.
Pretreat before exercise with albuterol or cromolyn.

Diffuse capacity of carbon monoxide in the lung DLCO
After performing the standard PFTs, the patient then inhales trace amounts of carbon monoxide.
CO traverses the alveolar capillary beds much more readily than CO2 or O2.
As such, most of the CO inhaled should be absorbed.
When it is not, this suggests pulmonary scarring consistent with pulmonary fibrosis. Search for a cause.

Diffusing Capacity
Decreased DLCO (<80% predicted)
Obstructive lung disease
Parenchymal disease
Pulmonary vascular disease
Anemia
Increased DLCO (>120-140% predicted)
Asthma (or normal)
Pulmonary hemorrhage
Polycythemia
Left to right shunt


paired T test
The paired t-test will show whether the
differences observed in the 2 measures will be
found reliably in repeated samples.

ANOVA:One way
If we have data measured at the interval level, we
can compare two or more population groups in
terms of their population means using a
technique called analysis of variance, or ANOVA.

Honestly significant difference test (HSD)
When you do multiple significance tests, the chance of finding a "significant" difference just by chance increases. Tukey´s HSD test is one of several methods of ensuring that the chance of finding a significant difference in any comparison (under a null model) is maintained at the alpha level of the test.

RESULTS







DISCUSSION

DISCUSSION

DISCUSSION

DISCUSSION

DISCUSSION

DISCUSSION

DISCUSSION

DISCUSSION

Air Turbulance
DISCUSSION

Major sources of noise generated by a helicopter
DISCUSSION

DISCUSSION

Static Spirometry
DISCUSSION

Dynamic Spirometry
DISCUSSION

DISCUSSION

Body Plethysmography
DISCUSSION

Body Plethysmography
DISCUSSION

helium dilution
DISCUSSION

DISCUSSION


DISCUSSION

DISCUSSION



134
THANKS FOR YOUR ATTENTION