Embed Size (px)
Citation preview
Inhalation Injury and Carbonmonoxide poisoning
EMEL ERYÜKSEL
Assoc. Prof.
Marmara University Medical School
Pulmonary and Critical Care, İstanbul


Inhalation Injury

lnhalation injury
• Upper airway injury (heat)
• Lower airway injury (local chemi cal)
• CO /cyanide poisoning (systemic toxicity)
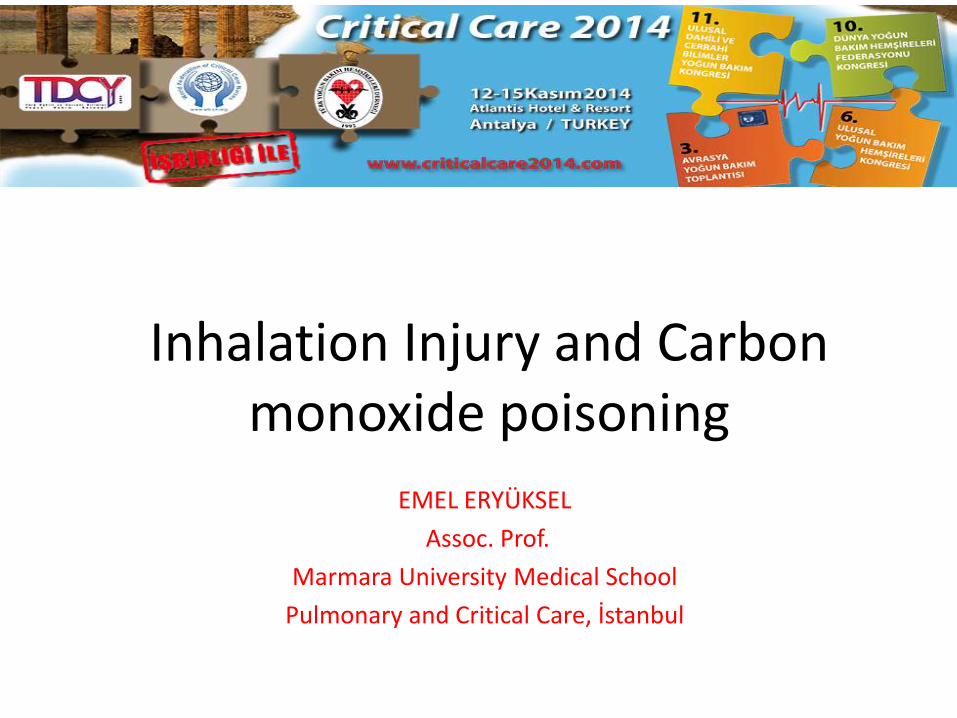
Heat injury to the upper airway
• may cause massiveswelling of the tongue, epiglottis, and aryeepiglottic folds with obstruction.
• as fluid resuscitation is ongoing it can exacerbateobstruction
• Initial evaluation is not a good indicator of the severity of obstructionthat may occur later
with permission from Dr. Yorgancı
Therefore, intubation should not be delayed ifsevere inhalation injury is present.

Diagnosis of inhalation injury
• ıs a subjective decision based on a history of smoke exposure in a closed space.
• Physical findings (facial injury, singed nasal hairs, soot in theproximalairways,changes in voice ) support the diag

Airway management
• Common signs of thepotential need forintubation include:
• Persistent cough, stridor, or wheezing
• Hoarseness
• Deep facial orcircumferential neckburns
• Nares with inflammationor singed hair
with permission from Dr. Yorgancı

Airway management
• Intubation is justified ifany of the following signsare present:
• Blistering or edema of theoropharynx
• Depressed mental status
• Respiratory distress
• Hypoxia or hypercapnia
• Elevated carbonmonoxide and/or cyanidelevels
with permission from Dr. Yorgancı

INDICATIONS FOR INTUBATION
• “When in doubt, intubate”
• altered mental status, refractory hypoxemia, and signs of airway obstruction and progressive facial swelling.
laryngoscopic exam

• Patients who do not require intubation
should receive supplemental oxygen at a
fraction of inspired oxygen (FiO2) of 100
percent.
• The tissue hypoxia is multifactorial, including
the inspiration of air with an FiO2 of less than
0.15 during the fire and the impaired
delivery and utilization of oxygen by the
tissues due to carbon monoxide and cyanide
poisoning
• Tissue hypoxia can quickly lead to death.

Lung Injury

• Inhalation injury leads todesuqamation of tracheaand bronchial tree followedby atelectasis.
• Atelectasis causes ven/permismatch.
• Ventilator associated lunginjury occurs related tocytokine release in overventilated regions.
As a result, ARDS follows VALI

INHALATION INJURY
• lnhalation injury is in part a mechanical processcharacterized by secretions, can occlude the airway leading to atelectasis andpneumonia.
• Aggressive use of bronchoscopy is highly effective in removing foreign particles and accumulated secretions
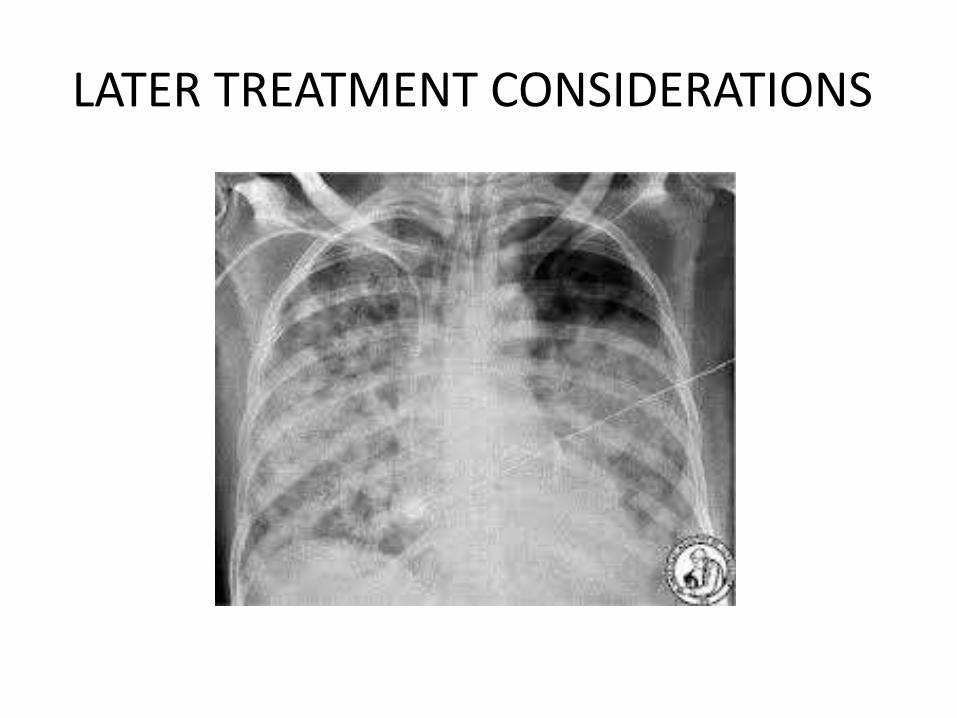
LATER TREATMENT CONSIDERATIONS
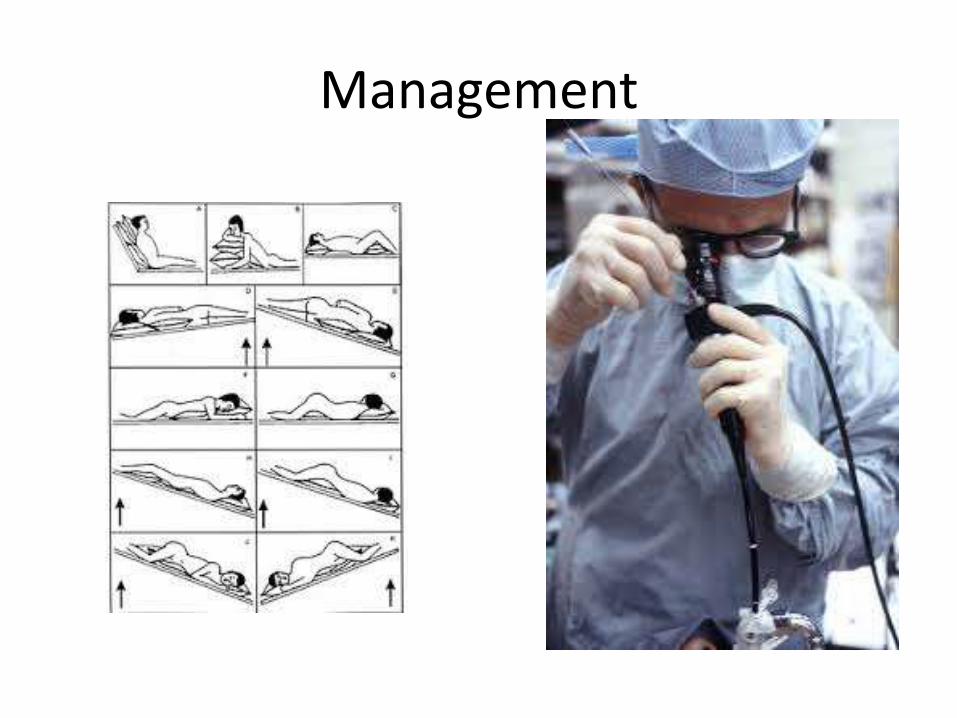
Management

ARDS

Carbon monoxide poisoning

CARBON MONOXIDE POISONING
• Competes with oxygen for hemoglobin binding which shifts the oxyhemoglobin dissociation curve to the left
• Oxygen delivery is compromised because of reduced oxygen carrying capacity
• competitively inhibits intracellular cytochrome P-450 resulting in inability of cellular systems to utilize oxygen
• can also precipitate an inflammatory cascade that resultsin CNS lipid peroxidation anddelayed neurologic sequelae
Carbon monoxide and cyanide
• Standard pulse oximetryis NOT reliable with significant CO toxicity(The absorbent spectrum of Cohb and Ohb are very similar)
• COhb level be obtained in all patients with moderate or severe burns.

CO- Symptoms
Weaver LK. N Engl J Med 2009;360:1217-25.

Carboxyhemoglobin levels
• an elevated carboxyhemoglobin levelmeasured by cooximetry of an arterial bloodgas sample.
• Nonsmokers may have up to 3 percentcarboxyhemoglobin at baseline; smokers mayhave levels of 10 to 15 percent.
• Levels above these respective values areconsistent with CO poisoning.

MANAGEMENT
• the most importantinterventions in themanagement of a CO-poisoned patient areprompt removal from thesource of CO and institutionof high-flow oxygen by facemask.
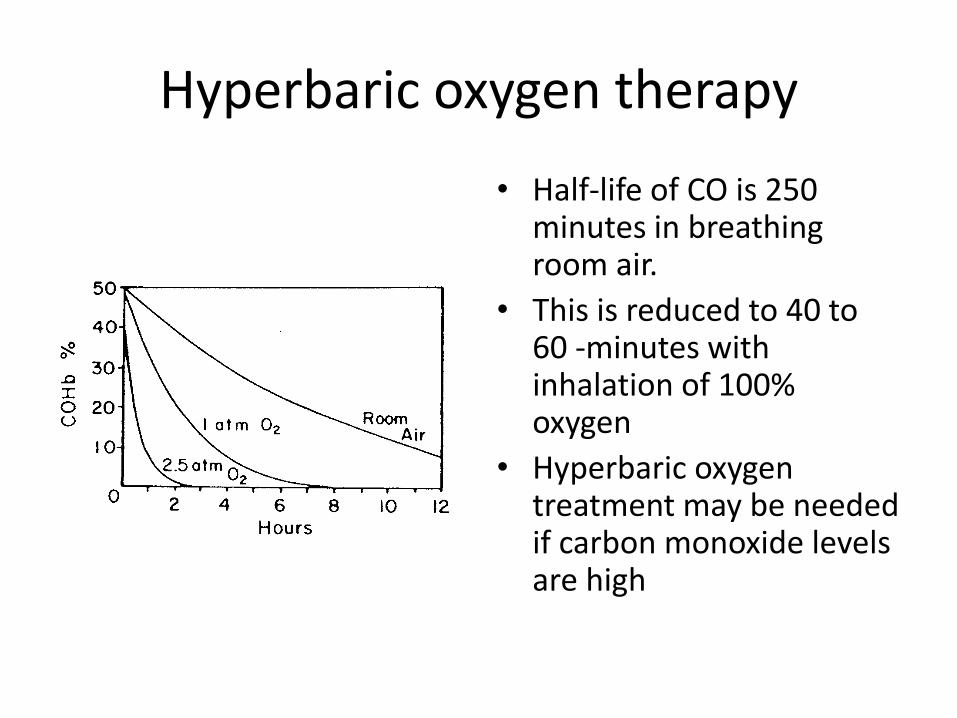
Hyperbaric oxygen therapy
• Half-life of CO is 250 minutes in breathing room air.
• This is reduced to 40 to 60 -minutes with inhalation of 100% oxygen
• Hyperbaric oxygentreatment may be neededif carbon monoxide levelsare high


• the more rapidly treatment is provided.
• Ideally, HBO should be initiated within sixhours.
• Benefit for patients treated more than 12 hours after their CO exposure is unproven

Cyanide
• produced during combustion of multiple household materials
• Cytochrome oxidase
• Lactic acidosis

Cyanide Intox-Symp
• Elevated lactat levels(>10mmol/L)
• Methabolic acidosis

Mechanical ventilation
• no ideal ventilator strategy has emerged
• limit plateau pressures to < 30 cm H2O
• allow Pco2 to increase if needed to minimize plateau pressures
• use the appropriate level of positive end-expiratory pressure

Noninvasive ventilation
• Without an ET tube, patients communicate more effectively, require less sedationand are morecomfortable

NIV : Keys of Success

NIV: Failure Rate
• %5-40
Brochard L, et al. N Engl J Med 1995;333(13):817–822.
Bott J, et al. Lancet 1993;341(8860):1555–1557..
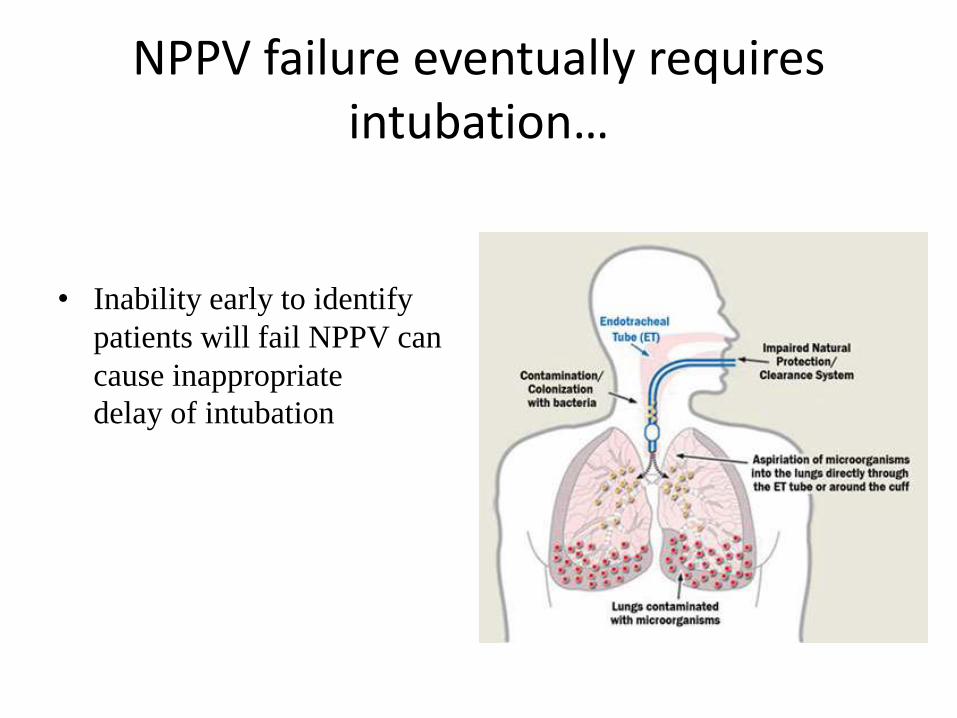
NPPV failure eventually requires intubation…
• Inability early to identify
patients will fail NPPV can
cause inappropriate
delay of intubation

Basic rules…….

NIMV – Noneligiable Patients
• Non-cooperable, agitated patients
• Hemodynamically unstable patients withmultiple organ failure
• Face/ Upper Airway Trauma
• Recent history of upper GI surgery
• Intestinal Obstruction
• Increased Secretion
• Presence of undrained pneumothorax

Noninvasive ventilation
• High secretions load areoften seen with II…
The most serious complication is failure torecognize when should we stop?Delayed entubation may cause continueddeterioration