Embed Size (px)
Citation preview

C.H.B.
Hepatitis C in Liver Transplantation
Patterns of Recurrence and Therapy
Professor Didier Samuel
Centre Hépatobiliaire, Inserm Unit 785, Paris XI University
Hopital Paul Brousse, Villejuif, France

C.H.B.
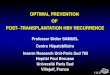
With HCCWithout HCC
0
100
200
300
400
500
600
700
800
1986 1987 1988 1989 1990 1991 1992 1993 1994 1995 1996 1997 1998 1999 2000 2001 2002 2003 2004 2005 2006 2007 2008 2009
Virus Delta Virus B Virus C
0
100
200
300
400
500
600
700
800
1986 1987 1988 1989 1990 1991 1992 1993 1994 1995 1996 1997 1998 1999 2000 2001 2002 2003 2004 2005 2006 2007 2008 2009
Virus Delta Virus B Virus C
www.eltr.org
HCV
HBV
HDV
INDICATIONS
SURVIVALHDV
HBV
HCV
Current Situation of LT for Viral Hepatitis in Europe

C.H.B.
LT
Asymptomatic hepatitis
AcuteHepatitis
FCH
Chronic Hepatitis
Chronic hepatitis
DeathRelT
Cirrhosis
Chronic Hepatitis
PatientHCV RNA+
Adapted from Mc Caughan
20%
70%
10%
HCV Recurrence: a Main issue
• HCV recurrenceo Poor outcome, accounting for 2/3 of graft losto Five years post-LT, 30% of LT patients have a cirrhosis on the graft o First cause of mortality

McCaughanJ Hepatol 2011
CHOLESTATIC HEPATITIS C

C.H.B.
Impact of Fibrosing Cholestatic Hepatitis on Survival
No FCH
FCH 19%
P=0.004
Antonini Am J Transplant 2011

Immunosuppression
ProliferationApoptosisFibrosis
HCV load Inflammation + IFN- related genes IFN-
response
-
Acute Rejection
InflammationStress Response
The immune response
-
+
Pathobiology of Chronic HCV Post LT
McCaughan and Zekry J.Hepatol 2004, Samuel Easl Hepatol 2006
Stimulation of the IMMUNE RESPONSE by more HCV WINS

C.H.B.
• Liver BiopsyGold Standard, Bring additional information than fibrosis stage
. HPVG Invasive, can be done with liver biopsyNot routine for many Centres
. Non invasive testsBiochemical
Elastometry (fibroscan). Time post-LT as an adding variable
EVALUATION OF THE SEVERITY OF HCV RECURRENCE

Blasco Hepatology 2006; 43: 492-499
HPVG, Fibrosis at 1 Year Post-Transplant and Outcome

Gallegos-Orozco Liver Transplant 2009
Fibrosis Stage at 12 months at Liver Biopsy and Survival

Carrion Hepatology 2010
Liver Stiffness and Severity of HCV Recurrence

Piciotto J Hepatol 2007
Impact of SVR on Survival in Transplant HCV +ve Patients
Berenguer M AJT 2008

C.H.B. Feray J Hepatol 2011
HCV Recurrence: a Main Issue

Roche, Samuel Liver Int 2012
Antiviral Treatment Before Transplantation

C.H.B.
PegIFN + RBV Before LT
• Treatment PegIFN+RBV until LT– 47 G1/4/6 patients
» 30 treated» 17 not treated
• 32 G2/3 patients treated» 29 treated» 3 not treated
Everson Hepatology 2012

C.H.B.
PegIFN + RBV Treatment Before LT
Everson Hepatology 2012
Meld score: 12, CTP score : 7Serious Infection rate: 7/59 (12) pts vs 0% controlDeath pre-LT: 5/59 vs 2/20 (NS)

Antiviral Treatment in Patients Waiting for Liver Transplantation, Risk of Sepsis Related to CPT
Carrión JA et al. J Hepatol. 2009;50:719-28.

C.H.B.Hezode J Hepatol 2013
Risk Factors of Death and Severe infections in cirrhotics on Triple therapy with Boceprevir or Telaprevir
The Cupic Study

Curry Gastro 2015
Sofosbuvir + Riba in Patients with HCC on the waiting List

Curry Gastro 2015
Sofosbuvir + Riba in Patients with HCC on the Waiting ListPost-Transplant SVR in those HCV RNA Negative at LT

Curry Gastro 2015
Sofosbuvir + Riba in Patients on the Waiting ListRecurrence Related to the Duration of HCV Indetectability Pre-LT

• 108 patients randomised 1:1 to 12 or 24 weeks of treatment • GT 1 or 4 treatment-naïve or -experienced patients with decompensated
cirrhosis (CTP class B [7–9] or C [score 10–12]*) • Broad inclusion criteria
– No history of major organ transplant, including liver – No hepatocellular carcinoma (HCC) – Total bilirubin ≤10 mg/dL, Hb ≥10 g/dL – CrCl ≥40 mL/min, platelets >30,000/mm3
Flamm S, et al. AASLD 2014; Oral #239.
LDV/SOF + RBV for 12 weeks is not an EMA-recommended treatment regimen;*Patients with CTP scores 13–15 excluded; CrCl: creatinine clearance;
EMA: European Medicines Agency
SOLAR-1: LDV/SOF + RBV in Decompensated Cirrhosis
Wk 0 Wk 12 Wk 36Wk 24
SVR12N=53
SVR12N=55 LDV/SOF + RBV
LDV/SOF + RBV

Flamm S, et al. AASLD 2014; Oral #239.
LDV/SOF + RBV for 12 weeks is not an EMA-recommended treatment regimen; Error bars represent 90% confidence intervals;
TE: treatment-experienced; TN: treatment-naïve
SOLAR-1: LDV/SOF + RBV in Decompensated Cirrhosis
0
20
40
60
80
100 87 8689 90
CTP B CTP C
SV
R12
(%)
26/30 19/22 18/2024/27
LDV/SOF + RBV 12 weeks LDV/SOF + RBV 24 weeks
SVR rates were similar with 12 or 24 weeks of LDV/SOF + RBVVirological response was associated with improvements in bilirubin, albumin, MELD and CTP
scores in both CTP class B and C patients
Prospective, multicentre study of 12 or 24 weeks of LDV/SOF + RBV in TN and TE HCV GT 1 and 4 patients with CTP B (N=59) or CTP C (N=49) clinically decompensated cirrhosis

Flamm S, et al. AASLD 2014; Oral #239.
LDV/SOF + RBV for 12 weeks is not an EMA-recommended treatment regimen *Missing FU-4: n=2 CTP B 12 wk; n=4 CTP B 24 wk; n=2 CTP C 12 wk;
n=7 CTP C 24 wk; BL: baseline; FU: follow-up
SOLAR-1: LDV/SOF + RBV in decompensated cirrhosis: Change in MELD from BL to Week 4
(-8)-6
-4
-2
0
2
4
-6
-4
-2
0
2
4
n=5 n=5 n=2 n=3
(+10)
CTP B CTP C12 wk (n=30)* 24 wk (n=29)* 12 wk (n=23)* 24 wk (n=26)*

Efficacy before LT Excellent results in compensated cirrhotic patients Lower efficacy in decompensated ones
Approved regimens
RBV RBVALLYRBV RBV Δ
SOF+LDV (1) SOF+DCV (2) 3D (3) SOF+SIM (4)
88%82%
94%
72%
Compensated
Child<11
(1) Charlton M. Gastroenterology 2015; (2) Poordad F, Etats-Unis, EASL 2015, Abs. L08; (3) Poordad F, Etats-Unis, EASL 2014, Oral late breaker LB O163 (4) Reddy R, Etats-Unis, EASL 2015, Abs. O007

Efficacy before LT SVR12 depends on severity of cirrhosis
o Using SOF+LDV or 3D, low platelets count and low albumin level are risk factors of relapse
RBV RBVALLYRBV RBV Δ
SOF+LDV (1) SOF+DCV (2) 3D (3) SOF+SIM (4)
88%82%
94%
72%
Compensated
(1) Charlton M. Gastroenterology 2015; (2) Poordad F, Etats-Unis, EASL 2015, Abs. L08; (3) Poordad F, Etats-Unis, EASL 2014, Oral late breaker LB O163 (4) Reddy R, Etats-Unis, EASL 2015, Abs. O007

Efficacy before LT
SVR12 depends also on genotype
RBV RBVALLYRBV RBV Δ
0
20
40
60
80
100
8086
59
89
71
81
43
0
7482
70
85
73
60
71
100
SVR1
2 %
(ITT
)
252 28 172 15 164 21 45 5 61 7 114 7 27 13 3
SOF + LDV + RBV SOF + LDV SOF + DCV + RBV SOF + DCV
Overall Genotype 1 Genotype 3 Others
p < 0,05
Foster G, UK, EASL 2015, Abs. O002
Combinaison SOF and NS5A inhibitor + RBV during 12 weeks 467 cirrhotic patients Child ≥ B7

Next Generation: Is this going to change?Astral 4: Sofobuvir + Velpatasvir
Ribavirin still required in most cirrhotic patients
Curry NEJM 2016

Safety before LT Good safety profile SAE rate of 20% (mainly due to RBV) Hepatic function is one issue
1. Ouwerkerk-Mahadeva S, et al. AASLD 2013. Oral #65; 2. Gilead Sciences Europe. SOVALDI (sofosbuvir), Summary of Product Characteristics, January 2014; 3. German P, et al. AASLD. 2013. Oral #52; 4. Khatri A, et al. AASLD. 2012. Oral #66; 5. Bifano M, et al. AASLD. 2011. Oral #78.
Pharmacokinetic changes according to liver function
Hepatic function impairment AvoidMild Moderate Severe
Simeprevir1 + 2.44 + 5.22 Child CSofosbuvir2 + 1.26 + 1.43Ledipasvir3 No adjustementParitaprevir/r4 - 0.71 + 1.62 + 10.23 Child COmbitasvir4 + 0.92 + 0.70 + 0.45Dasabuvir4 + 1.17 + 0.84 + 4.19 Child C?Asunaprevir5 - 0.79 + 9.8 + 32 Child B/CDaclatasvir5 - 0.57 - 0.62 - 0.64

Decompensated CirrhosisIs Delisting Possible?
BaselineMELD < 15(n = 199)
Patie
nts (
%)
0
10
20
-16
0
-11 -9 -8 -7 -6 -5 -4 -3 -2 -1 0 1 2 3 4 7 8 9 12 13
Deterioration : 26 %
0 0
Improvement: 56 %
<1 2 3 3
8 8
1517 18
13
7
2 1 <1 1<1 <1<1
BaselineMELD ≥ 15
(n = 72)
Patie
nts (
%)
0
10
20
-16 -11 -9 -8 -7 -6 -5 -4 -3 -2 -1 0 1 2 3 4 7 8 9 12 13
Deterioration : 11 %Improvement : 76 %
52
3
1110
16
8
1413
5
03 3
0 00 00
522
Gane EJ, New Zealand, AASLD 2015, Abs. 1049
Variations of MELD score Baseline/EOT in SOLAR I and II studies among Child>B cirrhotics

Association Between Improvement and SVR
Munoz J, USA, AASLD 2015, Abs. 202
Only 28% had an improvement in the MELD score ≥ 3 points
Delta
MEL
D
+10
+15
56 %+50
-5-10-15-20
20 % 23 %
020
All MELDimprovement
No change MELD
deterioration
406080
100
SVR1
2 (%
) Some patients improve without achieving SVR Although achieving SVR, some patients worsen
(comorbidities?)
Meta-analyses of 5 studies

Is there a Point of no Return?
National cohort study in patients waiting for LT in France
SVR12 = 88 %
183 patients
ESLD without HCC
N=77
LT31%
Delisting for improvement
16%
HCCN=106
LT54%
Drop-out6%
Coilly A, France, AASLD 2015, Abs. 95

7.5
AUC: 0.814
Child-Pugh score
MELD score
CHC, n=70Complete improvement
No response
Partial improvement
Is there a Point of no return?
National cohort study in patients waiting for LT in France: SVR12 = 88 %
Coilly A, France, AASLD 2015, Abs. 95
36%
28%
36%
Cirrhosis, n=53
21% Child B
25% Child C
72% Child A
MELD score could not be the good marker

Taking into account the System of Organs
AllocationDeaceased donor
Male 61 yo, G1bESLD without HCCMELD 23 after SBPListed for LT
National allocation system

Taking into account the system of organs allocationDeaceased donor
Male 61 yo, G1bESLD without HCCMELD 23 after SBPListed for LT
AscitesCovert HE
LT still indicates but no more access…
National allocation system
HCV treatment

C.H.B.
o Antiviral treatment with Peg-IFN+RBV
Treatment done at the stage of chronic hepatitis
Peg-IFN +RBV = standard of care:
Overall SVR: 30%;
SVR G1: 25- 30%, SVR G3: 50% (Berenguer J Hepatol 2008, Calmus J Hepatol 2012)
EPO in 40% of patients
Poor tolerance of treatment when F3-F4 (Carrion Gastro
2007, Roche LT 2008): 30% of premature discontinuation
HCV Treatment after LTStandard of Care Until 2012

C.H.B.
Coilly AAC 2012
Coilly J Hepatol 2014
First Generation Protease inhibitors in HCV RecurrenceBoceprevir and Telaprevir

C.H.B.Coilly Plos One 2015
First Generation Protease inhibitors in HCV RecurrenceBoceprevir and Telaprevir

C.H.B.Coilly Plos One 2015
First Generation Protease inhibitors in HCV RecurrenceBoceprevir and Telaprevir

C.H.B.
Triple Therapy with Telaprevir or BoceprevirThe Crush Study
Burton J Hepatol 2014
ToleranceAnemia < 10 : 78%Blood Transfusion: 57%EPO: 81%GCSF: 41%Creat 0.5 mg/l : 38%Rash: 11%Hospitalizations for infection: 11%Discontinuation: 15%Deaths : 9%

C.H.B.
Triple Antiviral Therapy with Telaprevir in HIV-HCV Liver Transplant Recipients
Antonini et al. AIDS 2013

C.H.B.
The Advent of Second Generation DAAs After Liver Transplantation

C.H.B.
PegIFN +RBV+Daclatasvir for FCH after LT
Fontana Liver Transpant 2012

C.H.B.
Sofosbuvir+Daclatasvir for FCH after LT
Fontana Am J Transplant 2013

C.H.B.
Sofosbuvir + Ribavirin After Transplantation
Charlton Gastro 2015
SOF 400 mg + RBV 400‒1200 mg (N=40) SVR12
• Patients with recurrent HCV post-liver transplant
– Liver transplant ≥6 and ≤150 months prior to enrollment
– Any HCV genotype
– Naïve or treatment-experienced
– CTP ≤7 and MELD ≤17
• Low, ascending-dose RBV regimen starting at 400 mg/day, escalated based on hemoglobin levels

C.H.B.
Sofosbuvir + Ribavirin After Transplantation
Charlton AASLD 2013
SOF + RBV (N=40)
Male, n (%) 31 (78) Median age, y (range) 59 (49-75) White, n (%) 34 (85) BMI <30 kg/m2, n (%) 30 (75) Mean HCV RNA log10 IU/mL (range) 6.55 (4.49-7.59)
Genotype, n (%)1a1b234
22 (55)11( 28)
06 (15)1 (3)
IL28B, n (%)CCCTTT
13 (33)16 (40)11 (28)
Metavir-equivalent fibrosis stage, n (%)None or minimal (F0)Portal Fibrosis (F1-F2) Bridging Fibrosis (F3)Cirrhosis (F4)
1 (3)14 (35)9 (23)16 (40)
Prior HCV Treatment, n (%) Yes 35 (88)Median years since liver transplantation (range) 4.3 (1.02-10.6)

C.H.B.
Sofosbuvir + Ribavirin After Transplantation
Charlton Gastro 2015

C.H.B.
Sofosbuvir + Ribavirin After TransplantationTolerance
Charlton AASLD 2013 and Gastro 2015
0 1 2 3 4 8 12 16 20 24 FU-2 FU-410
11
12
13
14
15
0.8
0.9
1.0
1.1
1.2
Hb Creatinin
SAE: 15%, SAE leading to discontinuation: 5%, fatique 30%, Hb< 10g:/dl: 33%; Hb< 8g: 3%, 20% Received EPO

C.H.B.
Compassionate Use Sofosbuvir + Ribavirin ± PegIFN in Liver Transplant Patients
X Forns Hepatology 2015

C.H.B.
Compassionate Use Sofosbuvir + Ribavirin ± PegIFN in Liver Transplant Patients
X Forns Hepatology
in press 2015

C.H.B.
Compassionate Use Sofosbuvir + Ribavirin ± PegIFN in Transplant Patients: Virologic Response
X Forns Hepatology In Press 2015

C.H.B.
Compassionate Use Sofosbuvir + Ribavirin ± PegIFN in Transplant Patients: Virologic Response: Clinical Outcome
X Forns Hepatology 2015

ABT450/Ritonavir/Ombitasvir + Dasabuvir + RBV in LT Recipients with Recurrent HCV GT 1
• Phase II Study on efficacy and tolerance of ABT-450/r/ombitasvir 150 mg/100m g/25 mg/d + dasabuvir 250 mg x 2/d in patients with HCV reinfection post-LT
• Patients G1, fibrosis ≤ F2 at Liver biopsy, no prior PEG/RBV after LT• Dosing RBV free for the investigator• CNI adaptation
– Tacrolimus 0.5 mg/week or 0.2 mg/3 days– Ciclosporine 1/5 of initial daily dosing once a day
3D + RBV(n = 34)
SVR12
D0 W24 W72
Kwo P, Etats-Unis, EASL 2014, Abs. O114 actualisé

C.H.B.
ABT450/Ritonavir/Ombitasvir + Dasabuvir + RBV in LT Recipients with Recurrent HCV GT 1
P Kwo NEJM 2015

12 or 24 weeks LDV/SOF + RBV after LT: Solar 1 studyExcellent results in F0-F3 Patients
F0–F3
SV
R12
(%)
53/55 22/26 15/18
CTP B
55/56 25/26 24/25 2/3
CTP A
LDV/SOF + RBV 12 weeks LDV/SOF + RBV 24 weeks
3/5
CTP C
SVR rates were similar with 12 or 24 weeks of LDV/SOF + RBV Charlton et al, Gastroenterology 2015

Sofosbuvir + Daclatasvir After LT-The Cupilt Study
• Decision of investigator
Week 0 Week 12 Week 24 Week FU12
SOF=400mg/day; DCV=60mg/day; RBV=decision of physician according to renal function
SOF+DCV
SOF+DCV+RBV
SOF+DCV+RBV
SOF+DCV
n=11
n=3
n=52*
n=64*
Coilly et al, EASL 2015

Sofosbuvir + Daclatasvir After LT-The Cupilt StudyVirological Kinetics
Coilly et al, EASL 2015 Mean time to achieve undetectability: 5.7±3.3 weeks [1-20]
0 4 8 12 16 20 2401234567
SOF+DCV (n=75)SOF+DCV+RBV (n=55)
Week
HCV
RN
A (
log
IU/m
L)
p=ns

Sofosbuvir + Daclatasvir After LT-The Cupilt StudySVR according to Treatment Duration
Coilly et al, EASL 2015
SOF+DCV (n=11) SOF+DCV+RBV (n=3) SOF+DCV (n=64) SOF+DCV+RBV (n=52)Week 12 Week 24
100%
67%
100% 98%100%
67%
97% 96%
EOT SVR12
Virological breakthrough n=1
Lost of FU n=1Relapse n=1
Death n=2Wk1 & FU Wk6
p=ns

Sofosbuvir + Daclatasvir After LT-The Cupilt StudyOverall Tolerability
Coilly et al, EASL 2015
• One death at week 1: hyperosmolar coma in a patients with a previous history of diabetes mellitus
• One death at week 6 post-treatment: HCC recurrence (HCV RNA negative)• 4 cardiac disorders: 2 High Blood Pressure, 2 cardiac decompensations in patients
with past history of cardiomyopathy
Overall (n=130) SOF+DCV (n=75) SOF+DCV+RBV (n=55) p
Serious adverse events 30 (23.1) 15 (20.0) 15 (27.3) ns
Death 2 (1.5) 0 (0) 2 (3.6) ns
Cardiac disorders 4 (3.0) 1 (1.3) 3 (5.5) ns
Biopsy proven acute rejection 2 (1.5) 1 (1.3) 1 (1.8) ns
Infections (G3/4) 9 (6.9) 3 (4) 6 (10.9) ns

Sofosbuvir + Daclatasvir After LT-The Cupilt StudyHematological Adverse Events
Coilly et al, EASL 2015
Overall (n=130) SOF+DCV (n=75) SOF+DCV+RBV (n=55)
Anaemia 49 (37.7) 17 (22.6) 32 (58.2) Grade 0 (but EPO) 7 (5.3) 1 (1.3) 6 (11.0) Grade 3/4 (<8 g/dL) 18 (13.8) 6 (8.0) 12 (21.8) Erythropoietin use 30 (23.1) 9 (12.0) 21 (38.2) Blood transfusion 13 (10.0) 5 (6.7) 8 (6.2) RBV reduction for AE 25 (19.2) - 25 (45.5) Neutropenia 35 (27) 13 (17.3) 22 (40) Grade 3/4 (<0.75G/L) 8 (6.2) 1 (1.3) 7 (12.8) G-CSF use 2 (1.6) 1 (1.3) 1 (1.8) Thrombocytopenia 37 (28.5) 20 (26.7) 17 (30.1) Grade 3/4 (<50G/L) 7 (5.4) 3 (4.0) 4 (7.3)

Efficacy after LT Most regimens allow to achieve a SVR12 rate of >90%
Approved regimens
SOF+RBV (1) SOF+LDV (2) SOF+DCV (3,4) 3D (5) SOF+SIM (6,7)
70%
95% 94% 95%90%
RBV RBVALLYRBV RBV Δ
(1) Charlton M, Gastroenterology, 2015; (2) Charlton M, Gastroenterology, 2015; (3) Coilly A, EASL G15, 2015; (4) Poordad F, Etats-Unis, EASL 2015, Abs. L08; (5) Kwo py, NEJM, 2014; (6) Pungpapong S, Hepatology 2015. (7) Reddy R, Etats-Unis, EASL 2015, Abs. O007

Leroy et al, Clin Gastroenterol Hepatol 2015
Impressive Efficacy in FCH Transplant Patients
Sofosbuvir + Daclatasvir or Sofosbuvir + Ribavirine in 23 Patients with FCH-The Cupilt Cohort

Leroy et al, Clin Gastroenterol Hepatol 2015
Sofosbuvir + Daclatasvir or Sofosbuvir + Ribavirine in 23 Patients with FCH-The Cupilt Cohort
Impressive Efficacy in FCH Transplant Patients

Compassionate use of Sofosbuvir + Ribavirine +- Peg IFN After LT- Clinical outcome
Forns et al, Hepatology 2015
Efficacy Lower in Transplant Patients with Advanced Cirrhosis

Ciclosporine Tacrolimus
Sofosbuvir
Sofosbuvir/Ledipasvir
Ciclosporine AUC - 2% Tacrolimus AUC + 13%
Daclastavir
Simeprevir
Ciclosporine AUC +4.74 Tacrolimus AUC +79%
Ombitasvir, paritaprevir, ritonavir, dasabuvir
Ciclosporine AUC +5.82Dosage ÷5
Tacrolimus AUC +57.10.5mg/wk ou 0.2mg/2days
Safety after LT Good safety profile SAE rate of 20% (mainly due to RBV) Issue: drug-drug interactions
Coilly, A. Liver Int. 2015

Safety after LT Good safety profile SAE rate of 20% (mainly due to RBV) Issue: drug-drug interactions
Coilly, A. France, G15, EASL 2015.
ANRS C023 CUPILT cohort: SOF+DCV
Tacrolimus Ciclosporine Everolimus MMF
Number of patients 78 37 13 71
Number who changed dosage –
n (%)44 (56 %) 18 (49 %) 5 (38 %) 9 (13 %)
Most changes occurred after 4 weeks of treatment, reflecting improvement in liver function more than clinically relevant drug-drug interactions
To monitor immunosuppressive drugs is still mandatory

C.H.B.
SVR with DAA in LT Patients
Gamballi J Hepatol 2014

C.H.B.
CONCLUSION
• The Field of Liver Transplantation In HCV Patients is moving dramatically with IFN-free regimen
• Some questions are open:– Treat before or after Transplantation?– Remove patients from the waiting list?– Which combination?– Duration of treatment ? Use of RBV?– How to avoid relapse? Risk of liver failure in case of relapse?
• The survival after transplantation for HCV infection will improve

Conclusion 3: Management ProposalTreatment with DAA Before or After LT
Patients on waiting list
HCC
Child A/B
Treat before LT
Child C
Consider benefits
To control HCC: Treat
Reduced access to LT:
Delay
ESLD – No HCC
Child B
Consider MELD score
Low: Treat High: Delay
Child C
Treat after LT

Take Home Messages
Treat hepatitis C using DAA before or after LT? Both strategies are feasible with excellent efficacy results and good safety profiles
Regarding efficacy, better results are achieved after LT than before in decompensated cirrhotic patients
Regarding safety, drug-drug interactions and degree of hepatic impairment are still issues, and favor the use of NS5A inhibitors
Withdraw patients of waiting list is feasible and should concern about 30% of patients.

Centre Hépato-BiliaireA Coilly
E De MartinF Chiappini
B RocheR Sobesky
F SalibaT Antonini
JC Duclos-ValléeAnd all the Team at The CHB