Embed Size (px)
Citation preview

Sensory Adaptation to Strabismus
Summary
• it should now be apparent that binocular vision is not inborn.
• A series of conditioned reflexes develop in the first three years of life to produce binocular input to the cortical cells leading to the development of binocularly driven cells in the cortex.
• These reflexes become firmly established by about 5 to 6 years (the plastic period) and hence become unconditioned reflexes.

However:
• if strabismus develops before three years
– adaptation to normal development occurs to prevent symptoms
– leads to abnormal unconditioned reflexes developing by age 6 years.
– Usually NO SYMPTOMS
• if strabismus acquired from 6 years to adult:
– binocular vision is well established,
– symptoms very likely to occur
• if strabismus is acquired at 3-6 years:
– symptoms will occur
– but the system is unstable and readily breaks down
– adaptations will develop (plastic period)
– AND AGAIN SYMPTOMS ARE UNLIKELY TO OCCUR

Binocular Vision is embarrassed in two ways:
• Diplopia
• Confusion

X
F lF r
O
P
In visual cortex Fl = X and Fr = O, Therefore results in confusion Fl and P both see the X but In Fl, X = Central In P, X = In Temporal field, Therefore results in diplopia

X
F lF r
O
P
In visual cortex Fl = X and Fr = O, Therefore results in confusion Fl and P both see the X but In Fl, X = Central In P, X = In Temporal field, Therefore results in diplopia

How does the visual system cope?
• In young patients sensory adaptations overcome diplopia and confusion.
• These sensory adaptations are:
– suppression
– abnormal (anomalous) retinal correspondence (ARC).

Anomalous Retinal Correspondence (ARC)
• describes a condition in which originally non-corresponding retinal areas of the two eyes co-operate to produce a form of binocular single vision.
• A shift in the spatial localisation of the deviating eye occurs to counteract the effect of the ocular deviation.

ARC can be defined in two ways:
• the two foveas have different visual directions
• the fovea of the fixating eye has acquired an anomalous common visual direction with a peripheral element in the deviating eye

3 types of ARC
• HARMONIOUS (HARC) – if the angle of anomaly = angle of strabismus
• UNHARMONIOUS (UN-HARC) – if angle of anomaly is greater than zero but less than the angle of deviation
• PARADOXICAL (PARC) – if angle of anomaly is in the opposite direction

• present in the retinal area receiving the peripheral image in the strabismic eye
• convergence of nerve fibres from here means there is no longer point to point correspondence ie LOSS OF RESOLUTION
• may occur at various levels eg retinal horizontal cells, LGN, Cortex
• in effect produces enlarged ‘pseudo-Panums’ area centred on the point receiving the image, which corresponds with the fovea of the other eye: HARMONIOUS ARC (90% of strabismus)
• hence in ARC the images of the object of regard are given the same visual direction despite the strabismus.
• Therefore there is no diplopia and some very low grade BV may be present

• 1. Strabismus before 4 years old (especially before 30 months)
2. Delay in treatment3. Small constant strabismus angle4. Esotropia>exotropia5 Unilateral > alternating
Conditions for development of ARC

Theories of ARC
• The Innate Theory
• The Adaptive Theory
• Travers’ Theory• Motor Theories
The Innate Theory
• This theory considers the retinal correspondence innate and immutable reflecting a congenital anomaly, which is untreatable.
• The ARC has been put forward as the cause of the strabismus.

The Adaptive Theory
• Retinal correspondence changes as a sensory adaptation to the strabismus. The “local sign” of anatomically corresponding points is learned early in life and can adapt during this period.
• Burian (1947) was a supporter of this view
• which is central to current understanding of ARC.

Travers’ Theory
• a theory to explain the more frequent detection of UN-HARC than HARC.
• suggested that the confusion and diplopia associated with strabismus in a subject with NRC could be relieved by a suppression scotoma at the fovea of the deviating eye.
• A retinal point adjacent to this scotoma was now used as a corresponding point to the fovea of the straight eye but confusion and diplopia were not relieved by this UNHARC.
• This area of the retina was in turn suppressed and the process continued until HARC resulted.
• This process was thought to be very slow and may not actually be completed, which accounts for the high incidence of UNHARC.
• During this period the assessment of retinal correspondence was restricted to a synoptophore for its evaluation.
• now believed that the type of equipment used to measure ARC is influential in its detection. The more deeply ingrained the ARC the more tests will detect it.
• The main problem with this theory is that HARC is present continuously despite the angle of strabismus changing from distance to near.
Problems
If an adaptive process is present there should be a temporary aftereffect when the adapting process is removed. Though such aftereffects can be observed in ARC (eg monocular diplopia) the findings are often different. HARC is present continuously despite the angle of strabismus changing from distance to near; or with or without spectacle. The instrument used to measure ARC does not indicate the depth of the ARC but represents the influence of the technique on the binocular status.

These unsatisfactory aspects of ARC as an adaptive process led Morgan (1961) to propose an alternate motor theory. The theory places emphasis on ego-centric localisation. Oculo-centric localisation refers to the visual direction associated with a particular retinal and cortical point. This direction is not absolute but relative to the ego-centric localisation attributed to the fovea of the eye at that time.

Motor Theories
the innervation pattern of the extra-ocular muscles gives the potential for change in correspondence by influencing the correction from oculo-centric to ego-centric localisation. Morgan (1961) states “thus anomalous correspondence might depend not on sensory adaptations to a strabismus but rather on whether the basic underlying innervational pattern to the extra-ocular muscles was one which registered itself to consciousness as altering ego-centric direction”.
The attraction of this theory is that it has none of the restrictions of the adaptive theories when applied to small angle strabismus and offers the possibility of an instant change in ARC with changed conditions.
However the prediction that accommodative esotropia would not have ARC has not been substantiated.

• The innate theory of ARC is not compatible with clinical observations. • The adaptive theory is convincing for a small proportion of small angled
strabismus of constant angle and long duration.• However the motor theory offers the promise of an ARC which varies with
the sensed positions of the strabismic eye.
Summary

• Many of the procedures used to assess ARC give varying results depending upon the status of fixation.
• Therefore prior to testing ARC it is essential to determine whether central or eccentric fixation is present.
• It is often necessary to use more than one test to measure retinal correspondence.
• Different tests introduce varying degrees of sensory dissociation and as a result can have different findings.
Clinical evaluation of ARC

• a plano trial lens with fine grating of lines.
• You can see through the lens with very little disturbance of normal vision
• except when you look at a spotlight where it produces a faint streak crossing the light.
• Two Bagolini lenses are placed in the trial frame to produce streaks at 45 and 135 degrees
• In unilateral strabismus if the lens before the deviated eye produces a streak that appears to go through the spot of light = harmonious ARC.
• If there is a gap in the streak = suppression.
• If the lens before the deviated eye produces a streak that does not go through the spot of light then NRC or UNHARC is present.
• Different Bagolini lenses are available.
• The fainter the streak the more likely the ARC will occur as there is less disturbance to normal vision.
Bagolini Striate Lens Method



• Using two lenses = X in ARC
• introduce the filter before the strabismic eye and increase the depth of the filter until ARC is not seen (ie removed from everyday conditions)
• When illumination is reduced in the strabismic eye – NRC is favoured as there is not so much need for adaptation as the weak image is less bothersome.
Filter Bar with Bagolini Lenses

• Regard the spotlight with both eyes open.
• Place a red filter before the strabismic eye and a vertical prism (6-15∆) before one eye to move the image out of the suppression area.
• The patient should see one red and one white light.
• If vertically aligned but a strabismus is present = HARC
• If separated, either NRC or UNHARC
• if you introduce a prism of the angle of strabismus : the two lights should be aligned if NRC is present
Red Filter/Diplopia Method

• During alternating cover test the patient subjectively will see an apparent jump of the fixation point when the cover changes eyes
• only occurs in NRC if Px has a deviation
• There will be no jump if: – there is no deviation
– the deviation is relieved with prism– HARC
It is useful to cover the eye for the shortest time possible as ARC is a feature of binocularity
Phi Phenomenon Method

• Another similar method is to first correct the angle of strabismus using prism CT and then ask the patient if they still see Phi movement. If yes then the patient has ARC
• To do this:• Detect habitual angle of deviation• Total angle of strabismus (alternating CT)• Correct total angle with prism• There should then bifoveal fixation and no Phi movement• If Phi movement present = ARC• Then reduce prism until no movement seen• If no prism required =HARC• Prism often habitual angle of strabismus in UNHARC
Phi Phenomenon Method
• Same as for Phi Movement
• Move the tubes until they are neutralised when switched on and off
Synoptophore Method

• This is described in greater detail in the suppression section of the notes
Worths Four Dot Test

• Produces a central foveal image in each eye in turn (produces a cross)
• In NRC the after images will coincide
• In ARC the after images will be separated
• The best way to do this is to first let the patient detect the two images by closing his eyes.
• Then open eyes and look at a plain surface and see if lines cross.
• Then provide a fixation point for the dominant eye and see if lines cross – this is more like the patients habitual position
• NB must take EF into account and measure its angle first.
After-Image method



• If the deviation is present but the eyes are aligned with the X = HARCNB it is better to use the bigger OXO on the near unit or the distance unit at 2m.
Mallett Unit

Evaluation of Tests
• The visual conditions of the various tests for evaluating retinal correspondence are variable and subsequently produce quite differing results.
• Tests that most readily duplicate the prevailing visual conditions are most likely to provide evidence of sensory adaptation.
• Tests interfering with the patient’s visual status are less likely to be successful.
• Pickwell identifies 5 factors that are influential in determining the sensory adaptation.
– Degree of dissociation– Retinal area stimulated – Eye used for fixation– Constancy of deviations– Relative illuminance of retinal images

Test NRC ARC Suppression DiplopiaBagolini Lenses 3.8% 83.4% HARC 9.7% 2.9%Worth 4 - dot 0 33.9% HARC 56.3% 9.7%Synoptophore 34.9% 12.6% HARC
52% UNHARC0 0
After-imagetest
63% 35%
Table : provides a comparison of results on the determination of the status of sensory response of strabismic patients using various methods.

The hierarchy of tests in which NRC is least likely to occur
• Bagolini lenses
• Synoptophore
• Red filter
• Worths 4 – dot
• Negative after image
• Positive after image

• General Rule : the continued presence of ARC under increasingly more dissociative conditions indicates a more deeply embedded condition and subsequently a more difficult adaptation to eliminate.
• Stereopsis
• Microtropia - term generally used for small angle strabismus which shows no movement on the cover test because the ARC and eccentric positions coincide.
• Using a titmus stereotest, stereoacuities of 100 seconds have been reported.
• Using random dot stereograms, Cooper and Feldman (1978) could find no stereopsis in their patients.
• In large angle strabismus no stereopsis is possible but course peripheral depth perception has been found.
• The clinical stability of microtropia does suggest an adaptive basis for ARC.
Clinical Characteristics of ARC

Depth of ARC
• It is possible to grade ARC in terms of the nature of the stimulus conditions under which it persists.
• Alternatively the nature of the stimulus conditions under which ARC can be retained can indicate how ingrained the ARC has become.
• Mallett (1975) suggested a classification to optimise treatment based on filter density. Three types of ARC have been suggested:– A plastic superficial adaptation found in medium to large angle strabismus. This
type readily breaks down in synoptophores. A filter of 0-7 will break this down. Represent 80% of all strabismics.
– More deeply ingrained and commonly found in small angle stable strabismus. Filter >8 required to break it down. ARC needs treatment before orthoptic exercises are attempted.
– Very intense and rare form of ARC. Not treatable and subjects often present with stereopsis on the Titmus test

• The presence of a horopter has been demonstrated in ARC.
• The locus of the horopter is less precise and the anomalous fusional space is larger than that of normal binocular vision.
• This is evidence of sensory fusion and raises the possibility of motor fusion.
• There is differing opinion on the form that this anomalous fusional activity takes.
Sensory and Motor Fusion in ARC

• In the majority of strabismus cases, ARC is considered beneficial, and is therefore encouraged and not treated.
• The exception is if surgery is to be carried out with a chance of obtaining BSV. However, great care should be taken so as not to produce diplopia.
• In general the cases considered for treatment will be of mixed correspondence. Predominantly normal correspondence will recover anyway and predominantly abnormal has too poor a prognosis.
Management of ARC

• Accurate refractive correction• Amblyopia treated by occlusion• Orthoptics: with regard to the 5 factors previously stated
Start with maximum dissociation• Aim for bifoveal stimulation• Encourage fixation with the strabismic eye• Identify conditions where BSV is achieved and start here• Start with more reduced illumination before the strabismic eye• Teach physiological diplopia (eg bead and string, needles)• Improvement should be shown within 6-8 weeks• Prism Methods : to remove the angle of the strabismus
vertical, to encourage NRC• NB Treatment of ARC also helps in overcoming suppression. Therefore in strabismus cases
where treatment is undertaken, it is better to concentrate on the management of the ARC rather than the suppression alone.
The general pattern for treatment is as follows:

• After treatment of sensory adaptations and only once NRC is fully established – you can then carry out vergence exercises to attend to the motor deviation by vergence exercises.
Vergence Exercises

• Suppression and ARC are interrelated adaptations to strabismus occurring before 6 years.
• is a binocular sensory adaptation that occurs when the patient is using both eyes in the presence of a strabismus to avoid confusion and diplopia.
• is a cortical adaptive phenomena which prevents images in the strabismic eye from reaching a conscious level.
• also represents an obstacle in trying to restore normal sensorimotor function.
• In small strabismus < 25∆: both suppression and ARC usually occur
• In larger strabismus > 25∆: suppression dominates• Suppression is an extension of normal visual processing.
SUPPRESSION
• When differing images are presented to normally corresponding points the strongest image or dominant eye predominates or alternating rhythm of change between two eyes if equal
eg F L - E
• In strabismus corresponding points are constantly receiving a different image and there is a loss of retinal rivalry over area from fovea to point receiving image (nasal in convergent strabismus).
• This loss of form in the deviated eye prevents confusion.
• Suppression is an anomaly of BV although it also occurs without strabismus in amblyopia.
Retinal Rivalry

F L


• DEPTH
• EXTENT OF RETINAL AREA
Investigation of Suppression is mainly concerned with determining:

Filter Bar Method
• In strabismus the patient fixates a spot of light.
• A filter bar (palest filter) is placed before the non-suppressing eye and the density of the filter is increased until two lights are seen.
• This filter is a measure of depth.
• Occasionally when the end point is reached fixation swaps to the other eye and suppression swaps over, resulting in no diplopia.
• If there is no strabismus use red filters or red/green diplopia goggles.
• grade cards in same way as synoptophore slides
• Present larger picture before the suppressing eye (simultaneous vision)gross suppression
• Fusion cards eg interrupted passages = more shallow suppression
• May need to use a variable prism stereoscope in strabismus – set to the angle of the strabismus.
Stereoscope :

• useful in anisometropia, heterophoria and some small angle strabismus
• if suppresses, may be overcome by momentary occlusion of better eye – shallow suppression
• if worse VA<6/12 then use larger letters
Infinity Balance or Septum Test

• Place lenses before both eyes to produce two streaks at 90 degrees to each other.
• Ask the patient if both streaks are seen and if there is any central gap between them.
• If one streak is missing (or there is a central gap) then add a filter bar to the good eye to test the depth of the suppression.
Bagolini Striate Lenses

• ask if spot and streak are both seen or only one (streak is easier to suppress)
Maddox Rod

• polarised lines
• suppression test
Mallett Unit
• Consists of distance and near units with two white, one red and one green aperture, that is viewed through red and green goggles.
• It is popular in orthoptic departments but is only a check for gross suppression and can produce many false positive/negative results.
• For example, the eyes are easily dissociated with the red-green spectacles and therefore a patient with unstable but functionally useful binocular vision may exhibit a suppression response.
• Also a suppression area may fall within the centre of the test and miss all the apertures and retinal rivalry can occur which may cause false positive results.
Worths Four Dot Test

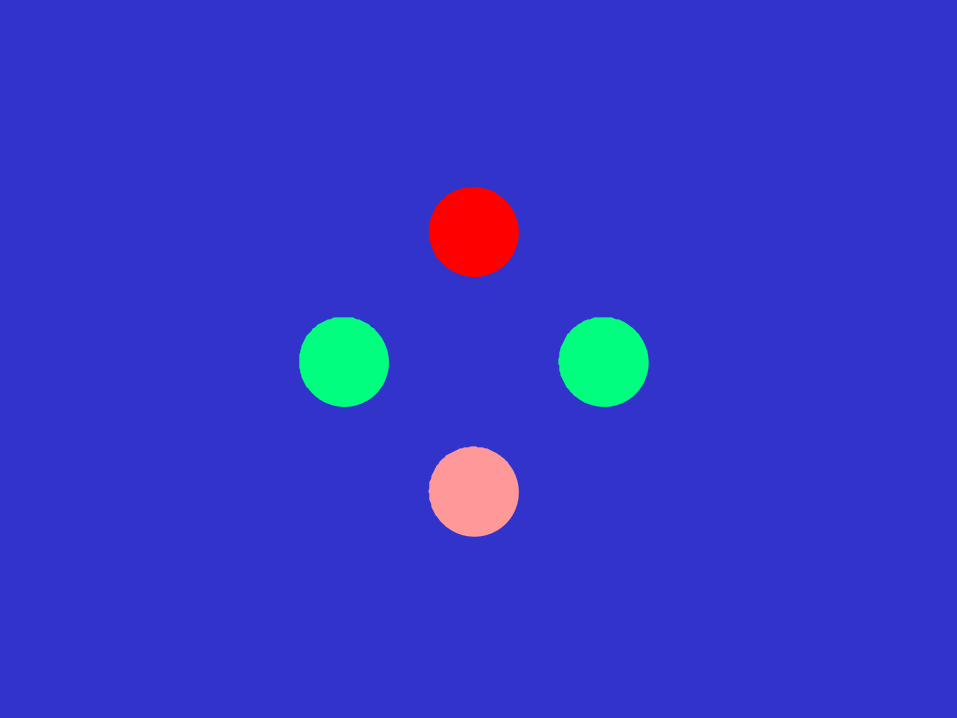
• Red filter on right eye, green filter on left
• Patient sees all 4 lights = normal fusion
• 4 lights in presence of strabismus = ARC
• If Px sees 2 red lights = left suppression
• If Px sees 3 green lights = right supression
• If Px sees 2 red lights and 3 green lights = diplopia
• Green and red lights alternating = alternating supression
Worths Four Dot Test

• This is usually due to suppression
• can be tested with the suppression plate in the TNO test.
Loss of stereopsis in heterophoria

• This is a binocular field loss scotoma onlyMust be investigated under binocular conditions Either get 2 suppression scotoma, one at the fovea and one at the point receiving image
• or
• a joining of these into one area (longstanding or large angle strabismus),
• and when investigating with smaller targets
EXTENT OF SUPPRESSION SCOTOMA

• The patient sits in front of Bjerrum screen, which is in the corner of the room. • A small mirror is mounted at ~45degrees (may be compensated to angle of the
strabismus) before the FIXING eye, which occludes the screen from this eye but can fix a small marker at the side of PX, at the same distance as screen.
• Both eyes are open throughout• Plot ‘scotoma’, non-seeing to seeing with Bjerrum targets of different sizes
(size varies with target size)SOT – suppression of nasal retinaXOT – suppression of temporal retina
• This test is difficult to set up and time consuming and as a result not often measured clinically.
Suppression scotometry

Prism Bar Method
• this is used more clinically
• The patient fixates the spotlight with the dominant eye and prism bar is moved before the suppressing eye.
• When the image of the spot has moved off the suppression scotoma the patient reports diplopia.
• The difference between the angle of strabismus (from CT) and the prism which moves spot out of scotoma = angular extent of the scotoma.
• This can be used to measure vertically as well.

• The deeper the suppression and greater the extent across the retina – the more difficult it will be to treat.
• Factors such as patient’s age, duration of strabismus, co-operation etc must be taken into account.
• Only treat suppression if the deviation can also be eliminated and if there is a strong chance of BSV occurring ie only young children where strabismus can be corrected/has been corrected and binocular driven cells can still develop.
• OTHERWISE INTRACTABLE DIPLOPIA MAY OCCUR (NB suppression is an adaptation to prevent diplopia and confusion).
• Suppression can also be treated in anisometropic amblyopia in conjunction with Rx and amblyopia treatment.
Evaluation

• If it has been decided to treat the suppression, this involves training the patient to be aware of the suppressed image.
• Correct integration of the two images ie using normally corresponding points so that you do not enforce ARC.
• Stimulating normally corresponding points must be carried out where the visual axis cross or by first correcting the angle of the strabismus.
• Treat ARC at the same time.
• First carry out accurate refraction to minimise the angle of strabismus and maximise clarity (supp less strong).
• One or more of the following methods of treatment:
Management of Suppression

• Problems: not easy to enforce bifoveal stimulation
• Can use variable prism stereoscope to correct angles of >10 degrees and adjust card distance in smaller angles on the Holmes stereoscope
• If appropriate, use fusion cards eg Bradford F series (The ship) – especially in anisometropic suppression
• Choose type at limit of acuity in the amblyopic eyeOr G series (black box with binocular lock, red and black lettering inside – can use with a red filter)
L series – also black box but with a pictorial design inside
• In strabismic Px it is often better to use simultaneous vision cards as this encourages NRC
Stereoscopes

• Again must be done when eyes are not strabismic
• In most people with strabismus from an early age both ARC and suppression are presenteg in convergent strabismus- form vision suppressed at macula and to nasal retinal point receiving image-localisation of object in space is modified across more extensive peripheral area of strabismic eye to avoid diplopia
Wire Reading/Bar Reading
• Red filter before the dominant eye, trace a picture with red pen/computer game.
• The drawing is seen by the poor eye but the paper by both eyes
• Or sort coloured beads (must use suppressing eye as red filter distorts the colour).
• Again must take care not to reinforce ARC - make sure the angle of strabismus is corrected
• also make sure that monocular acuity is good enough for the task.
Red-filter method

• string and nut or needles
• find the point of intersection of visual axes and encourage seeing points further and nearer in physiological diplopia
• check for NRC by CT
• inhibitions of images from central area of retina of one eye during binocular conditions - “suppression scotoma”
• suppressed area may extend to cover area of retina usually receiving object of regard ie into nasal retina for convergent strabismus
temporal retina for divergent strabismus
or may get total retinal suppression
• abnormal protraction of a normal mechanism of inhibiting passage of a signal for visual processing
Physiological Diplopia
• suppression can transfer from one eye to the other eg in ACS• probably initiated cortically but may have a retinal component• eliminates confusion and, if area extends, diplopia
In most people with strabismus from an early age both ARC and suppression are presenteg in convergent strabismus- form vision suppressed at macula and to nasal retinal point receiving image-localisation of object in space is modified across more extensive peripheral area of strabismic eye to avoid diplopia
• ARC and Suppression are binocular adaptations• Normal correspondence returns and there is no suppression when the fixing
eye is occluded and the strabismic eye takes up fixation.
Summary





























