Embed Size (px)
Citation preview


Sleep and dreams are taken for granted by those not affected by
obstructive sleep apnea. Unfortunately for tens of millions of
Americans and untold numbers worldwide, sleep is a nightly battle which leaves it’s victims and their
bed partners fatigued, stressed and much less healthy. Untreated sleep
apnea is one of the major public health issues we face as a nation. The emergence of dental sleep medicine as a safe and effective
treatment brings hope for the millions of patients looking for
alternatives to CPAP treatment. ThomasBisharaDMD.com © 2016
AASM•AADSM Clinical Guideline Update 2015 http://www.aasmnet.org/Resources/clinicalguidelines/Oral_appliance-OSA.pdf (2015)
ThomasBisharaDMD.com © 2016
AASM•AADSM Clinical Guideline Update 2015 http://www.aasmnet.org/Resources/clinicalguidelines/Oral_appliance-OSA.pdf (2015)
http://www.aasmnet.org/resources/practiceparameters/pp_update_oralapplicance.pdf (2005)
Clinical Practice Guideline for the Treatment of Obstructive Sleep Apnea and Snoring
with Oral Appliance Therapy
The purpose of this new guideline is to replace the previous and update recommendations for the use of OAs in the treatment of obstructive sleep
apnea (OSA) and snoring.
ThomasBisharaDMD.com © 2016
AASM•AADSM Clinical Guideline Update 2015 http://www.aasmnet.org/Resources/clinicalguidelines/Oral_appliance-OSA.pdf
1. We recommend that sleep physicians prescribe oralappliances, rather than no therapy, for adult patients who request treatment of primary snoring (without
OSA). (STANDARD)
ThomasBisharaDMD.com © 2016
AASM•AADSM Clinical Guideline Update 2015 Guideline Interpretation
1. We recommend that sleep physicians prescribe oralappliances, rather than no therapy, for adult patients who request treatment of Primary Snoring (without
OSA). (STANDARD)
ThomasBisharaDMD.com © 2016
Update 1 InterpretationPrimary Snoring is chronic, loud snoring WITHOUT the presence of Sleep Apnea. The diagnosis of Primary Snoring requires a sleep study. Once diagnosed the Sleep physician should write a prescription for a Custom Oral Appliance for adult patients seeking treatment. The Sleep Dentist will then evaluate the patient to determine if they are a candidate for an oral appliance.
AASM•AADSM Clinical Guideline Update 2015 http://www.aasmnet.org/Resources/clinicalguidelines/Oral_appliance-OSA.pdf
2. When oral appliance therapy is prescribed by a
sleep physician for an adult patient with obstructive sleep
apnea, we suggest that a qualified dentist use a
custom, titratable appliance over non-custom oral devices. (GUIDELINE)
ThomasBisharaDMD.com © 2016
AASM•AADSM Clinical Guideline Update 2015 Guideline Interpretation
ThomasBisharaDMD.com © 2016
Update 2 InterpretationWhen Oral Appliance Therapy (OAT) is indicated, the sleep dentist should fabricate a mandibular advancement device (MAD) that is customized for the patients unique occlusion, periodontal health and parafunctional habits such as bruxism and TMJ status. The ability to titrate the oral appliance is essential for proper airway management. OTC “Boil and Bite” solutions are contraindicated.
2. When oral appliance therapy is prescribed by a
sleep physician for an adult patient with obstructive sleep
apnea, we suggest that a qualified dentist use a
custom, titratable appliance over non-custom oral devices. (GUIDELINE)
AASM•AADSM Clinical Guideline Update 2015 http://www.aasmnet.org/Resources/clinicalguidelines/Oral_appliance-OSA.pdf
3. We recommend that sleep physicians consider
prescription of oral appliances, rather than no treatment, for
adult patients with OSA who are intolerant of CPAP therapy or
prefer alternate therapy. (STANDARD)
ThomasBisharaDMD.com © 2016
AASM•AADSM Clinical Guideline Update 2015 Guideline Interpretation
ThomasBisharaDMD.com © 2016
Update 3 Interpretation3. We recommend that sleep
physicians consider prescription of oral appliances,
rather than no treatment, for adult patients with OSA who are
intolerant of CPAP therapy or prefer alternate therapy.
(STANDARD)
Approximately 50% of patients using CPAP ultimately fail. Unless these CPAP failure patients seek treatment with Oral Appliance Therapy they will likely develop the common comorbidities and risk factors of untreated OSA. The sleep physician should refer the CPAP patient to a sleep dentist with a prescription for a custom oral appliance, letter of medical necessity, and CPAP Intolerance affidavit.
AASM•AADSM Clinical Guideline Update 2015 http://www.aasmnet.org/Resources/clinicalguidelines/Oral_appliance-OSA.pdf
4. We suggest that qualified dentists provide oversight —rather than no follow-up—of
oral appliance therapy in adultpatients with OSA, to survey for
dental related side effects or occlusal changes and reduce their incidence. (GUIDELINE)
ThomasBisharaDMD.com © 2016
AASM•AADSM Clinical Guideline Update 2015 Guideline Interpretation
ThomasBisharaDMD.com © 2016
Update 4 InterpretationThe sleep dentist should provide followup observation of their patients using oral appliances. The most common side effects of OAT are TMJ and myofascial discomfort, changes in occlusion and tooth mobility. Patient compliance should also be noted.
4. We suggest that qualified dentists provide oversight —rather than no follow-up—of
oral appliance therapy in adultpatients with OSA, to survey for
dental related side effects or occlusal changes and reduce their incidence. (GUIDELINE)
AASM•AADSM Clinical Guideline Update 2015 http://www.aasmnet.org/Resources/clinicalguidelines/Oral_appliance-OSA.pdf
5. We suggest that sleep physicians conduct follow-up
sleep testing to improve or confirm treatment efficacy,
rather than conduct follow-up without sleep testing, for patients fitted with oral
appliances. (GUIDELINE)
ThomasBisharaDMD.com © 2016
AASM•AADSM Clinical Guideline Update 2015 Guideline Interpretation
ThomasBisharaDMD.com © 2016
Update 5 InterpretationOnce the oral appliance has beeninserted and fully titrated to maximize the airway, the patient should be referred back to sleep physician. The sleep physician should conduct a followup sleep study to confirm the efficacy of the oral appliance.
5. We suggest that sleep physicians conduct follow-up
sleep testing to improve or confirm treatment efficacy,
rather than conduct follow-up without sleep testing, for patients fitted with oral
appliances. (GUIDELINE)
AASM•AADSM Clinical Guideline Update 2015 http://www.aasmnet.org/Resources/clinicalguidelines/Oral_appliance-OSA.pdf
6. We suggest that sleep physicians and qualified
dentists instruct adult patients treated with oral appliances forOSA to return for periodic office
visits— as opposed to no follow-up—with a qualified
dentist and a sleep physician. (GUIDELINE)
ThomasBisharaDMD.com © 2016
AASM•AADSM Clinical Guideline Update 2015 Guideline Interpretation
ThomasBisharaDMD.com © 2016
Update 6 InterpretationPatients using oral appliance therapy (OAT) to manage their OSA should be instructed to have their oral appliance checked on a regular basis. This will confirm patient compliance, appliance integrity and monitor common side effects of OAT including TMJ, Occlusal changes and tooth mobility.
6. We suggest that sleep physicians and qualified
dentists instruct adult patients treated with oral appliances forOSA to return for periodic office
visits— as opposed to no follow-up—with a qualified
dentist and a sleep physician. (GUIDELINE)
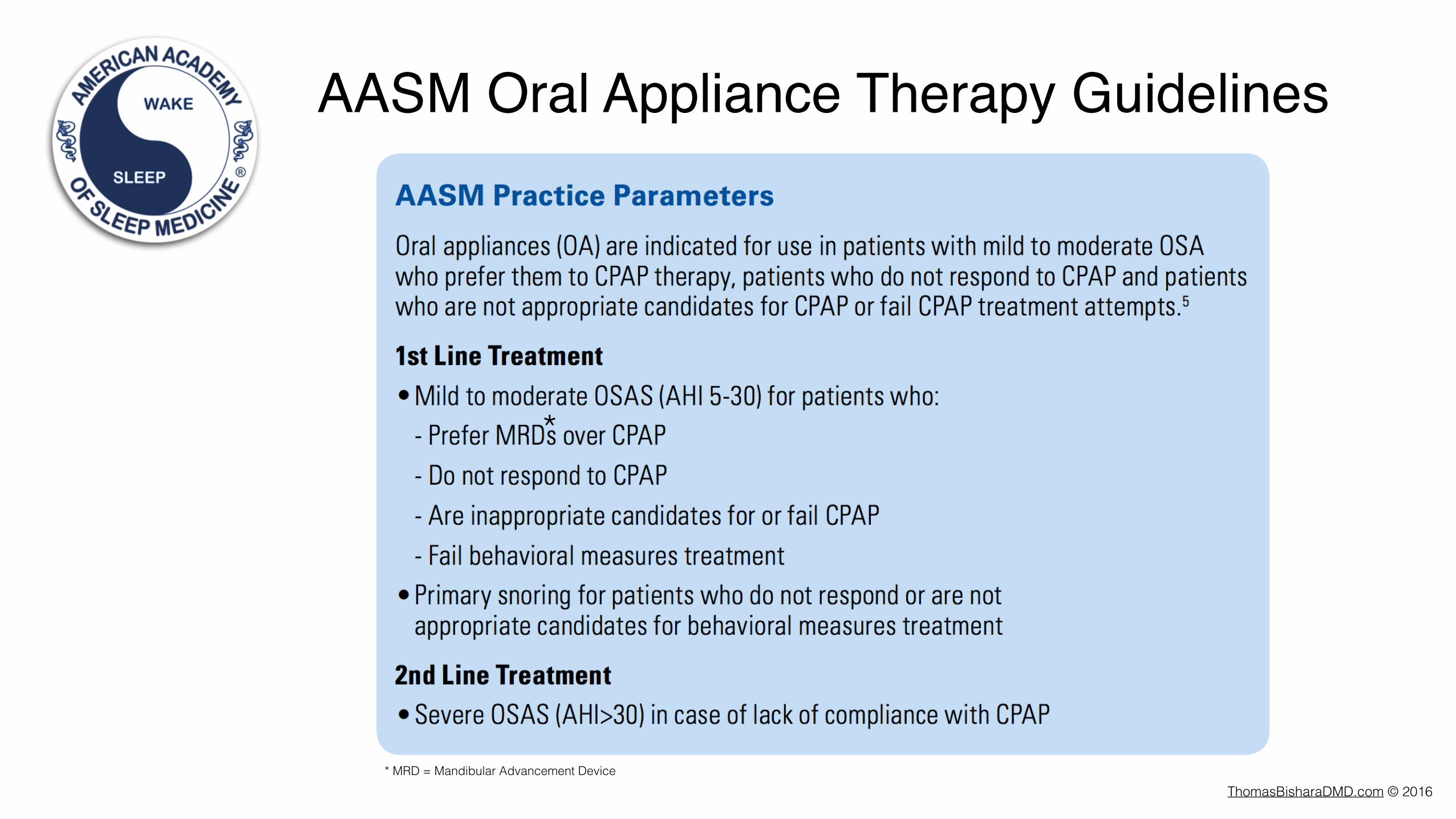
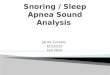
AASM Oral Appliance Therapy Guidelines
ThomasBisharaDMD.com © 2016* MRD = Mandibular Advancement Device
*
ThomasBisharaDMD.com © 2015
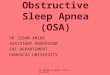
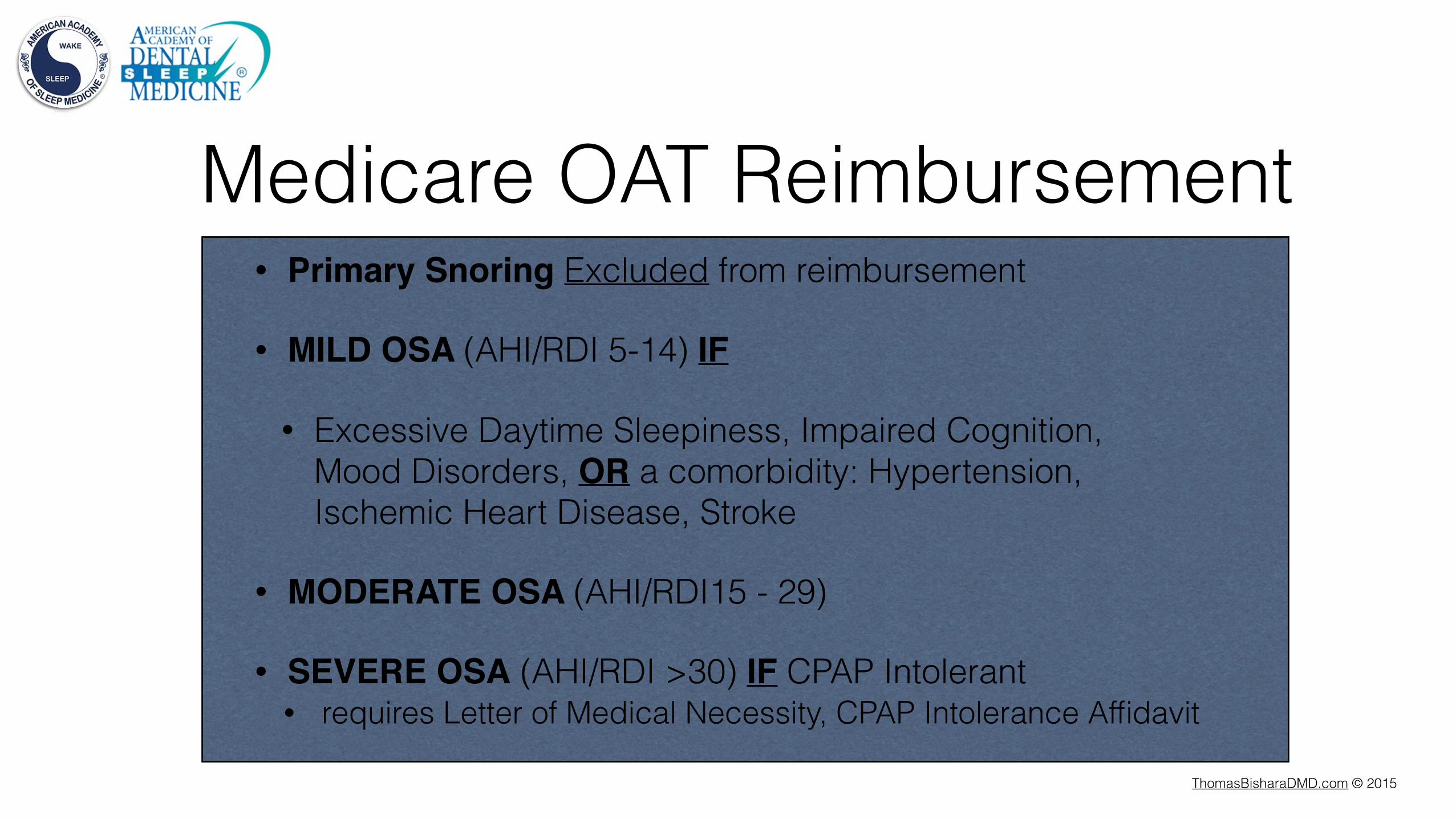
Medicare OAT Reimbursement• Primary Snoring Excluded from reimbursement
• MILD OSA (AHI/RDI 5-14) IF
• Excessive Daytime Sleepiness, Impaired Cognition, Mood Disorders, OR a comorbidity: Hypertension, Ischemic Heart Disease, Stroke
• MODERATE OSA (AHI/RDI15 - 29)
• SEVERE OSA (AHI/RDI >30) IF CPAP Intolerant• requires Letter of Medical Necessity, CPAP Intolerance Affidavit
ThomasBisharaDMD.com
ThomasBisharaDMD.com © 2016