Embed Size (px)
Citation preview

White Paper
Indranil Ganguly, CHCIO, FHIMSS, FCHIME, MBAVice President and Chief Information Officer, CentraState Healthcare System Carl Ausfahl, MS, RN, CPHQAssistant Vice President, Quality and Performance Improvement, CentraState Healthcare System Jack H. Dworkin, MD, MBA, FACCVice President and Chief Medical Officer, CentraState Healthcare System Raj Lakhanpal, MD, FRCS, FACEPChief Executive Officer, SpectraMD USA, Inc.
Executive Summary............................................................................................................................................................. 2
The Preventable Readmissions Challenge..................................................................................................................... 2
Strategies for Reducing Readmissions......................................................................................................................... 6
The Need for a Clinical Analytics Solution.................................................................................................................... 8
How a Clinical Analytics Solution Helped CentraState Healthcare System Reduce CHF Readmissions... 9
Conclusion..................................................................................................................................................................................11
Solving Preventable Readmissions Challenges, Strategies and the Need for a Clinical Analytics Solution

Executive Summary Federal regulatory bodies continue to advance initiatives that tie financial incentives to the quality and efficiency of health care delivered by hospitals and other providers. One of the most prominent of these initiatives is the Centers for Medicare and Medicaid Services’ (CMS) Readmissions Reduction Program. In the program, 2,213 hospitals were penalized a percentage of their total Medicare payments for fiscal year 2013, and this percentage has the potential to double and triple in 2013 and 2014.
Hospitals experiencing high readmission rates have started to implement strategies to reduce these rates. That said, managing readmissions poses considerable difficulties for many hospitals. The manual processes for tracking admissions, discharges and readmissions commonly used are a strain on resources and not conducive to effective readmissions management.
A real-time & predictive clinical analytics solution that integrates with hospital workflows can assist in solving these challenges for hospitals by enabling them to:
» Identify potential high-risk patients in real-time for immediate intervention
» Assess in real-time which patients are most likely to be readmitted to properly allocate
limited resources while patients are being treated
» Ensure appropriate transitions in care are provided to patients pre- and post-discharge
» Monitor performance and provide a real-time feedback loop for continuous quality improvement
In December 2013, CentraState Healthcare System deployed a solution to manage and reduce preventable readmissions for patients with congestive heart failure (CHF). During the first six months of installation, CentraState's CHF readmission rate was reduced 25.3%. The deployment process also provided CentraState with an in-depth understanding of the challenges inherent with implementing a clinical analytics solution and the resources required.
The Preventable Readmissions ChallengeHealthcare payers, led by Medicare, are concerned with the cost of preventable hospital readmissions. The PricewaterhouseCoopers’ Health Research Institute estimates the total cost of preventable hospital readmissions at $25 billion annually.i Medicare alone currently spends $15 billion a year on re-hospitalizationsii and almost one in five Medicare patients discharged from a hospital is readmitted within 30 days.iii
For those responsible for health care quality, the cost of readmissions is secondary. CMS 30–day readmission rates have become a broadly accepted measure of overall hospital care effectiveness.iv Preventable readmissions are an enormous burden on hospital staff and resources. Providers and quality officials view reducing preventable readmissions as a way to improve outcomes and provide patients with the best possible care.
Solving Preventable Readmissions: Challenges, Strategies and the Need for a Clinical Analytics Solution 2

The responsibility for reducing readmissions does not lie solely within the four walls of the hospital. There are many factors outside of a hospital’s control that can contribute to a patient being readmitted, including:
» Not adhering to discharge instructions
» Not refilling medications
» Not scheduling Primary Care Provider
(PCP) appointments
» Lack of transportation
» Quality of the patient’s home care
» Advanced age of the patient
There are many community factors as well which are often outside the hospital’s direct control such as patient demographics and socioeconomic status. Hospitals that serve underprivileged populations have challenges that their counterparts serving wealthier communities do not have. Rural hospitals face different challenges than urban hospitals. Additionally, hospitals often have patient populations that pull significantly from outside their immediate service areas. Therefore, managing health care across the continuum of care to link hospital, patient, PCP and community factors is a central goal of health care reform. As care delivery becomes a team effort, coordination across hospital departments and outpatient settings sites is essential.
The Readmissions Reduction ProgramTo counter rising readmissions, CMS has enacted the Hospital Readmissions Reduction Program. The program reduces total Medicare payments to hospitals with excessive 30-day readmission rates, effective for discharges beginning on October 1, 2012 (fiscal year 2013). The schedule for payment reductions is a 1% maximum reduction in 2013, 2% in 2014, and 3% in 2015 and onward. The financial impact to hospitals from these penalties is significant. A hospital with an average annual Medicare payment of $100 million could lose up to $1 million in 2013, $2 million in 2014 and $3 million in 2015. As mentioned, 2,213 hospitals have been penalized, which is roughly two-thirds of the hospitals whose readmission rates were reviewed.
Readmissions by the Numbers
$25 Billion Estimated total annual cost of preventable
readmissions
20% Approximate percentage of Medicare patients
who are readmitted to the hospital within 30
days of being discharged
2,200+ Hospitals penalized by first round of CMS
readmissions penalties
276 Hospitals that received maximum 1.00%
reduction in Medicare payments
$3 Million Amount a hospital with $100 million in
Medicare payments could be penalized in
2015
30% Percentage of Medicare readmissions
spending accounted for by top seven
conditions with highest number of
readmissions
76% Percentage of readmissions estimated to be
preventable
Solving Preventable Readmissions: Challenges, Strategies and the Need for a Clinical Analytics Solution 3

CMS is tasking hospitals only with reducing readmissions in areas where they can be prevented. The Readmission Reduction Program currently focuses on three conditions that cause the highest number of readmissions:
» Congestive heart failure (CHF)
» Pneumonia (PN)
» Acute myocardial infarction (AMI)
These conditions were identified by the Medicare Payment Advisory Commission (MedPAC) to have accounted for 30% of Medicare readmission spending in 2008, along with four others:
» Chronic obstructive pulmonary disease (COPD)
» Coronary artery bypass graft surgery (CABG)
» Percutaneous transluminal coronary angioplasty
(PTCA)
» Other vascular procedures
By 2015, CMS will most likely extend its penalties to all seven conditions.xi
In addition to Medicare, many health plans and other risk-bearing organizations are targeting readmissions in their payment incentive programs. As a result, many hospitals either have, or will soon have, multiple programs from Medicaid and private payers that link reimbursements to readmissions performance.
Finally, the Readmission Reduction Program can have a negative impact on a hospital’s public profile. CMS uses publicly-reported readmissions data to calculate penalties. Since the first round of penalties have already been administered and publicly announced, hospitals are becoming aware that high readmission rates have the potential to negatively impact their reputation for quality and safety.
It is important for hospitals to be aware of confounding factors that can increase the likelihood of a patient with CHF, AMI or PN being readmitted:
CHF » Age 65 or older at the time of initial
hospitalization v
» High pre-discharge B-type natriuretic
peptide (BNP) that has not decreased by
more than 50% of the admission valuevi
» Stable heart failure patients who have
undergone elective major, non-cardiac
surgeryvii
AMI » Co-morbid diabetes or chronic
obstructive pulmonary disease (COPD)viii
» Initial AMI inpatient stay was longer
than five days or required blood product
transfusionsix
Pneumonia » Low systolic blood pressure
» Elevated respiratory or heart rate and/or
an oxygen saturation of less than 90%
» In-hospital treatment failure including
hemodynamic instability, respiratory failure,
required mechanical ventilation or the
appearance of new infectious foci15x
These clinical factors also increase
readmission risk for CHF, AMI or PN
patients:
» Major depression
» COPD
» Childhood diseases
» Born prematurely
Solving Preventable Readmissions: Challenges, Strategies and the Need for a Clinical Analytics Solution 4

Risk Factors and CausesAccording to a 2007 MedPAC report, 76% of readmissions are preventable.xii Patients may be readmitted because of errors or omissions in care during the initial hospitalization, or inadequate post-discharge care. A readmission is considered to be clinically related to a prior admission and preventable if there was a reasonable expectation that it could have been prevented by one or more of the following:
1. The provision of quality care in the initial hospitalization
2. Adequate discharge planning
3. Adequate post discharge follow-up
4. Improved coordination between inpatient and outpatient health care teamsxiii
For hospitals, reducing preventable readmissions starts with identifying their highest-risk subset of patients. To identify these patients, hospitals must first understand the many factors that can increase a patient’s risk of being readmitted.
First and foremost, having any of the three conditions targeted by CMS or the additional four identified by MedPAC puts a patient at a higher risk for readmission. In addition to these conditions (and in conjunction with them), poor transitions in care planning - failing to quickly identify the patient in the hospital and provide support in transition from hospital to home to community physicians - is a primary contributor to preventable readmissions. From there, a broad range of other factors can contribute to hospital readmissions, including:
» Patient non-adherence to
treatment plans
» Confusion about dosing of
medications
» Patients with advanced
disease states
» Patients with multiple
co-morbidities, especially
diabetes
» Cognitive, mental or
behavioral health issues
» Living alone
» Age (specifically 65 or older)
» Low health literacy
» Language barriers
» Socio-economic factors Finally, there are stresses related to hospitalization in general, such lack of sleep, poor nutrition, pain and discomfort, being overwhelmed by the hospital experience, and negative reactions to medications that can contribute to a patient being readmitted.
Solving Preventable Readmissions: Challenges, Strategies and the Need for a Clinical Analytics Solution 5

It should be noted that multiple studies have concluded that over 50% of readmissions occur for reasons other than the condition at discharge. For example, 63% and 71% of readmitted patients with CHF and PN, respectively, are readmitted for factors unrelated to those discharge conditions.
Because the reasons for readmission are varied and complex, identifying at-risk patients - which should be a core component of every hospital’s readmissions reductions strategy - typically requires harnessing data from a range of different sources. With so many risk factors to manage, caring for at-risk patients is a comprehensive task that requires effort and coordination across the continuum of care: in the hospital, the community physician’s office, the emergency room, and the patient’s home.
Strategies for Reducing ReadmissionsAs outcomes-based payment reform initiatives gain traction, providers will be increasingly incentivized to improve patient health across the continuum of care. Appropriate discharge and transitions of care planning are integral to reducing readmissions and meeting overall health care quality improvement objectives. A successful readmissions reduction strategy should be centered on a transitional care workflow that ensures high-risk patients are quickly identified, receive appropriate care while admitted, receive sufficient education and instruction at discharge, and continue to receive follow-up care across all appropriate settings.
An effective strategy for reducing readmissions should entail four main components:
» Identify at-risk patients upon arrival at the ED. Hospitals should harness all available patient data to quickly and accurately identify patients upon arrival that are potentially at risk for readmissions. The quality and timeliness of available data plays an important role in this. Ideally, data from electronic health record (EHR) systems and other in-house sources can be used to achieve a complete and real-time (or near-real-time) picture of admitted patients, their diagnoses on admission and their current disease states. Having real-time data, and the software to effectively leverage it, empowers care coordination teams to take immediate action to avoid gaps in care for these patients.
» Assess which patients are most likely to be readmitted by running real-time patient data through risk modeling software. The software should score patients by level of risk, enabling staff to quickly allocate resources and attention appropriately and ultimately maximize positive patient outcomes and keep at-risk patients out of the hospital.
» Continually track at-risk patients, from the hospital to the PCP and home care settings. Hospitals must engage in proactive communication with at-risk patients, PCPs and health care professionals to help reduce the risk of future hospitalizations. Work lists integrating case management, discharge planning, and follow-up/monitoring procedures can help reduce readmissions by ensuring each patient receives the proper care while in the hospital and while transitioning to a home or outpatient setting. Each care settings has an important, specialized role in keeping patients out of the hospital. Since one or more of these care settings will likely contribute to the patient’s continued recovery, hosptals should have a mechanism in place for sharing post-discharge plans and other vital patient information with outpatient personnel.
Solving Preventable Readmissions: Challenges, Strategies and the Need for a Clinical Analytics Solution 6

» As part of a mandatory pre-discharge procedure, clinical staff should educate patients about their disease, their risks, and what they can do to self-monitor their condition. Post-discharge plans that give patients the best chances of recovering without needing to be readmitted must be created, shared with patients and outpatient staff, and monitored by care coordinators. Patient follow-up visits should be scheduled within 5-7 days of discharge with physicians or at outpatient clinics. Care coordination personnel must have a way to follow up and keep tabs on patients after they’re discharged to ensure their condition is being appropriately managed.
» Monitor performance improvement and provide a real-time feedback loop through dashboards customized to the user’s role. Efforts to reduce readmissions must be closely monitored and analyzed in order to determine the precise financial and quality of care improvements realized as a result. Stakeholders across the chain-of-care should be able to view real-time data and analyses in a way that’s customized based on their responsibilities.
Potential Obstacles to ImplementationThe implementation of a strategy to reduce preventable readmissions will inevitably present challenges. These usually concern data access and governance or the installation and application of new workflows.
Most hospitals are utilizing retrospective clinical and claims data to drive their clinical quality management efforts. This data is useful for illuminating patient care history and improving utilization management, but its value is limited for identifying at-risk patients upon admission/readmission. Hospitals require real-time data to effectively identify and manage at-risk patients but generally lack the tools and expertise to collect this data and the processes in place to leverage it.
Solving Preventable Readmissions: Challenges, Strategies and the Need for a Clinical Analytics Solution 7

Common obstacles to implementing a readmission reduction strategy include:
1. The inability to access real-time data. Real-time data collection requires the ability to connect with and access data from disparate locations (within the same facility or multiple facilities) and vendor systems which do not necessarily interface with one another. Hospitals must also be able to ensure all necessary data elements are collected and prevent future gaps in data.
2. Lack of an admitting and/or working diagnosis. The ability to capture admitting and working diagnoses as discrete data elements in the hospital system while the patient is still in the hospital is extremely beneficial in identifying at-risk patients. This functionality is unavailable in many hospitals.
3. Lack of “ownership” of a patient. It often is not clear who has the overall responsibility for the patient. For example, specialists are not always employed by hospitals, attending physicians keep rotating and multiple specialists end up working on one case.
4. No clear plan for readmissions workflow. Everyone from senior management down to the physicians and nurses on the floor must be engaged and invested in the process of redesigning, implementing and following a workflow suited to preventing readmissions.
5. Poor data governance. Hospitals require a well-defined data governance that supports and aligns operational workflow, clinical and business requirements, and communication across the enterprise.
Additionally, many hospitals lack procedures or infrastructure to perform appropriate care coordination, follow-up, and post-discharge monitoring. All parties involved with post hospital care, whether they be PCPs, home care providers or families, must have received the proper instructions and care guidelines to manage the patient’s care. Penalties for excessive readmissions should help motivate hospitals to invest in the personnel and technology needed to stay connected with discharged patients and support outpatient and in-home care providers.
The Need for a Clinical Analytics SolutionHospitals need access to real-time and predictive data, but they also need a mechanism to leverage this data to identify at-risk patients, segment them based on risk and align hospital resources appropriately. Clinical analytics solutions help hospitals unlock the value of their data and perform these functions.
Clinical analytics solutions enable hospitals to achieve their readmissions objectives with:
» Advanced algorithms that integrate real-time data and allow hospitals to identify upon arrival at the ED potential HF, AMI and PN patients and patients with other conditions that put them at risk for readmission. This allows care coordination teams to take immediate action to avoid gaps in care for these patients.
Solving Preventable Readmissions: Challenges, Strategies and the Need for a Clinical Analytics Solution 8

» Predictive algorithms and risk models continually updated with real-time information, enabling hospitals to calculate readmission risk scores of identified cases for the above conditions. Hospitals can then segment populations based on risk and focus resources appropriately to ensure these patients get the appropriate amount of care and post-discharge treatment.
» Software as a Service (SaaS) care coordination systems - which incorporate sophisticated predictive algorithms and targeted intervention tracking – that allow hospitals to track at-risk patients from the hospital to the PCP and home settings, greatly improving transitions in care. Clinical analytics platforms provide a number of case management tools to help hospitals more effectively manage discharged patients across the continuum of care. These tools include patient lists to monitor and track identified inpatient cases; work lists to facilitate case management, discharge planning, and post-discharge follow-up; and watch lists to notify ER staff and Case Managers of patients discharged with CHF, PN and AMI within the 30-day readmission penalty timeframe. Clinical analytics tools also allow care coordination personnel to share key patient data with clinicians at various outpatient care settings so they can make more informed care decisions.
» Custom role-based portals and similar presentation tools enable each stakeholder to focus on the data and analyses most closely aligned with their responsibilities. These portals enable real-time feedback loops that can help drive process improvements throughout hospital workflows. Clinical analytics solutions also allow hospital executives to forecast the financial impact of improvements in quality and patient care based on readmission rates.
How a Clinical Analytics Solution Helped CentraState Healthcare System Reduce CHF ReadmissionsCentraState Healthcare System is a 282-bed community medical center located in New Jersey which experiences nearly 15,000 inpatient admissions (excluding newborns) and more than 150,000 outpatient visits on average per year. Before implementing a clinical analytics solution, CentraState had received its first readmissions penalty from CMS - a 1.00% reduction in Medicare funds for fiscal year 2013.
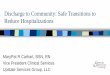
Successful Readmission Rate Reduction With FOCUS Actionable AnalyticsCentraState implemented the Readmission Module of the FOCUS Actionable Analytics platform from SpectraMD in December 2012 to support their strategy to reduce preventable readmissions. For the initial installation, CentraState elected to concentrate on reducing readmissions for CHF patients. Over the six months that FOCUS has been implemented at CentraState, the platform’s real-time data aggregation capabilities and predictive models have assisted CentraState in lowering its CHF readmission rate 25.3%.
Next, CentraState will focus on reducing readmissions for AMI, PN and additional chronic diseases including COPD and diabetes. CentraState is applying FOCUS solutions to manage conditions across the continuum of care as well, including a post-discharge work list to support transitions in care for patients receiving home health services or long-term care, and improving Value-based Purchasing and Core Measures scores.
Solving Preventable Readmissions: Challenges, Strategies and the Need for a Clinical Analytics Solution 9

FOCUS Actionable Analytics is a real-time and predictive clinical analytics solution that empowers hospitals and ambulatory care settings to identify patients at risk of readmission, enabling clinical quality administrators, care coordinators and providers to immediately intervene and align appropriate resources. FOCUS is an integrated system featuring the following key components:
1. An enterprise data model that includes real-time clinical and batch data integration from multiple data sources, including various HL-7 feeds
2. Proprietary algorithms for real-time identification of CHF, AMI and PN patients and sending alerts
3. Predictive algorithms for risk-scoring that enable resources to be allocated effectively to at-risk patients
4. Workflow tools including patient lists, work lists and watch lists to ensure appropriate care coordination, discharge and post-discharge care
5. Role-based dashboards for leadership at all organizational levels which present a range of performance metrics and the ability to drill down into details of specific patient/client level information
Additionally, the clinical analytics solutions of FOCUS assist providers and health care professionals to improve Core Measures and Value-based Purchasing scores, participate in ACOs and Health Homes, improve care coordination and monitor return on investment (ROI) of quality improvement initiatives.
(Same hospital readmission rates)
Figure 3: CentraState Healthcare System CHF Readmission Rates, December 2012 through May 2013
Solving Preventable Readmissions: Challenges, Strategies and the Need for a Clinical Analytics Solution 10

Installation and ImplementationIn the initial Needs Assessment, Data Collection and Analysis stage, SpectraMD gathered and analyzed information on CentraState’s current analytics capabilities, data sources and workflow. By identifying ahead of time CentraState’s current capabilities and what processes would be impacted, SpectraMD was able to plan a customized installation and workflow that ensured FOCUS operated with optimal efficiency. Prior to implementation, SpectraMD also met with CentraState executives to analyze CentraState’s business objectives, which allowed SpectraMD to map the FOCUS system’s functionality onto its organizational goals.
“SpectraMD provided quality analysts that helped us quickly mine the data needed from our data warehouse and other data sources to power their predictive models,” said Brian Dusheck, Manager of Financial Applications at CentraState Healthcare System. “This has helped us transform our data into actionable opportunities for our Quality & Care Management teams to reduce preventable readmissions.”
ConclusionHospital readmissions are a critical issue. Substantial financial penalties, quality of care, and reputations are at stake for hospitals based on their ability to keep readmissions at an acceptable level. Creating and implementing a readmissions reduction strategy should be a top priority for any hospital that isn’t measuring up in this area.
A successful strategy for reducing readmissions should include identifying at-risk patients, assessing which patients are most likely to be readmitted, tracking at-risk patients across the continuum of care and monitoring performance improvements as a result of these efforts. Such a strategy is challenging to implement without a clinical intelligence solution. The right clinical analytics application can help hospitals harvest the right data, make the right care decisions, transform their care workflows, bridge the continuum of care, and measure the precise quality and financial benefits of all of these activities.
i.) PriceWaterhouse Coopers’ Health Research Institute. (2008). The Price of Excess: Identifying Waste in Healthcare [White paper]. Retrieved from www.pwc.com/us/en/healthcare/publications/the-price-of-excess.jhtml
ii.) Krames Patient Education. (2010). Reducing Hospital Readmissions With Enhanced Patient Education [White paper]. Retrieved from http://www.bu.edu/fammed/projectred/publications/news/krames_dec_final.pdfhttp://www.bu.edu/fammed/projectred/publications/ne ws/krames_dec_final.pdf
iii.) Jencks, S.F., Williams M.V., & Coleman E.A. (2009). Rehospitalizations among patients in the Medicare fee-for-service program. New Engl J Med, 360(14),1418–1428.
iv.) Foster, Dave & Young, Janet. (2011). Lower Readmissions For Heart Patients Tied to Core Measure Compliance and Shorter Lengths of Stay [White paper]. Retrieved from http://healthcare.thomsonreuters.com/thought- leadership/assets/Readmissions_Core_Measures_and_LOS.pdf
v.) Aranda, J.M., et al. (2009). Current trends in heart failure readmission rates: analysis of medicare data. Clin Cardiol, 32(1), 47-52. vi.) Cournot, M., et al. (2008). Optimization of the use of B-type natriuretic peptide levels for risk stratification at discharge in elderly patients with decompensated heart failure. Am Heart J, 155(6), 986-991; Logeart, D., et al. (2004). Predischarge B-type natriuretic peptide assay for identifying patients at high risk of re-admission after decompensated heart failure. J Am Coll Cardiol, 43(4), 635- 641.
vii.) Hammill, B.G., et al. (2008). Impact of heart failure on patients undergoing major noncardiac surgery. Anesthesiology, 108(4), 559-567; Xu-Cai, Y.O., et al. (2008). Outcomes of patients with stable heart failure undergoing elective noncardiac surgery. Mayo Clin Proc, 83(3), 280-288.
viii.) Salisbury, A.C., et al. (2007). Impact of chronic obstructive pulmonary disease on post-myocardial infarction outcomes. Am J Cardiol, 99(5), 636-641.
ix.) Sun, X., et al. (2008). Early readmission of low-risk patients after coronary surgery. Heart Surg Forum, 11(6): E327-332
x.) Capelastegui, A, et al. (2009). Predictors of Short-term Rehospitalization Following Discharge of Patients Hospitalized With Community-Acquired Pneumonia. Chest 136(4), 1079-1085.
xi.) H.R. 4872, the Health Care and Education Affordability Reconciliation Act of 2010 (the Reconciliation Act, or HCERA; P.L. 111- 152).xii.) Medicare Payment Advisory Commission. (2007). Report to the Congress: Promoting Greater Efficiency in Medicare. Washington, DC: MedPAC.
xii.) Medicare Payment Advisory Commission. (2007). Report to the Congress: Promoting Greater Efficiency in Medicare. Washington, DC: MedPAC.
xiii.) Goldfield, N.I., et al. (2008). Identifying Potentially Preventable Readmissions. Healthcare Financing Review, 30(1), 75.
Solving Preventable Readmissions: Challenges, Strategies and the Need for a Clinical Analytics Solution 11